
Abstract
Objective
Prolactin elevation has been proposed as a risk factor for low bone density and potentially osteoporosis in patients on long-term treatment with prolactin-elevating antipsychotics. Our objective was to study the acute effects of prolactin elevation on serum markers of bone formation and resorption in patients treated with risperidone.
Methods
Thirty participants meeting Diagnostic and Statistical Manual of Mental Disorders fourth edition criteria for schizophrenia, major depressive disorder with psychotic features, or bipolar disorder with psychosis were enrolled. At baseline, subjects were antipsychotic free. Subjects were evaluated before and after 4 weeks of risperidone treatment. Assessments included symptom ratings along with testosterone, estradiol, prolactin, osteocalcin (marker of bone formation), and n-telopeptide crosslinks (NTx marker of bone resorption). Primary analysis examined the impact of risperidone treatment on change in the bone markers and hormone levels from pre to post treatment.
Results
Prolactin levels significantly increased from 12.1 ± 1.9 ng/ml to 65.7 ± 12.2 ng/ml after treatment (p < 0.001). NTx markers of bone resorption significantly decreased from 18.31 ± 1.49 nM bone collagen equivalent (BCE) before treatment to 15.50 ± 1.22 nM BCE after treatment in the study sample as a whole (p < 0.05). A trend was observed indicating that NTx may increase in individuals who have the greatest increases in prolactin after treatment r = 0.33, p = 0.07).
Conclusions
These findings suggest that prolactin elevation is associated with changes in bone physiology very early in the course of treatment with risperidone. Bone resorption decreased in many subjects but higher levels of bone resorption occurred in patients with the greatest increases in prolactin. This may have important implications for prolactin monitoring or the periodic assessment of osteoporosis-related outcomes in patients requiring extended treatment.
Introduction
A growing body of literature suggests that there may be an increased risk for low bone density and osteoporosis in patients receiving chronic therapy with antipsychotics associated with significant prolactin elevation [O’Keane, 2008]. This phenomenon was initially observed in patients with schizophrenia, where bone mineral density (BMD) values measured by dual-emission X-ray absorptiometry (DXA) scans were 14% lower than matched controls [Baastrup et al. 1980] with further research indicating that up to 44% of women treated with first-generation antipsychotics had BMD values at least 1 SD below age- and sex-matched controls [Halbreich et al. 1995]. To date the relationships between antipsychotics and changes in BMD or bone metabolism have predominantly been investigated in cross-sectional studies of chronically treated patients compared with healthy controls, cross-sectional studies comparing BMD in chronically treated patients prescribed either ‘prolactin-elevating’ agents (e.g. risperidone or first-generation antipsychotics) to ‘prolactin-sparing’ agents (e.g. other second- generation antipsychotics with lower risks of prolactin elevation), or in smaller prospective studies examining change in bone density over the course of year in chronically treated patients [Baastrup et al. 1980; Halbreich et al. 1995; Abraham et al. 2003a; Abraham et al. 2003b; Meaney et al. 2004; Howes et al. 2005]. These data indicate that antipsychotic effects on BMD are often, but not always, [Howes et al. 2005] likely to be observed after chronic treatment. Furthermore, there is some preliminary indication that changes in bone metabolism may occur as early as 6 months after the initiation of therapy [Abraham et al. 2003b; Meaney and O’Keane, 2007]. No investigations to date have studied acute changes (<3 months) in bone turnover in patients with minimal prior antipsychotic exposure. Identifying and characterizing whether changes in bone metabolism occur early in treatment may help us better understand how and if antipsychotics acutely influence bone physiology. The potential relationship between antipsychotic treatments and osteoporosis-related outcomes is difficult to assess in patients with chronic psychosis due to known confounding prior medication treatments. Therefore, the investigation of this relationship in relatively healthy patients, early in the course of illness, with minimal prior exposure to antipsychotic agents would be informative.
In this study we assessed hormone and selected bone metabolism measures during the first 4 weeks of risperidone treatment in patients who were antipsychotic free before the study, the majority of whom had little or no prior lifetime antipsychotic exposure and were receiving their first treatment for psychosis. We tested the hypothesis that markers of bone resorption and bone formation are associated with risperidone-associated prolactin elevation. We also examined the changes of other important hormones such as estradiol and testosterone, and assessed the relationships between changes in these markers and bone physiology outcomes. These data provide important information on the acute effects of risperidone treatment on bone homeostasis and the relationship between bone turnover and changes in serum hormones seen early in treatment.
Methods
Participants
Participants were recruited, consented, and assessed through the University of Illinois at Chicago (UIC) inpatient and outpatient services. Study procedures and consent forms were approved by the UIC Institutional Review Board. Participants were between 18 and 45 years of age, scheduled to begin treatment with the antipsychotic risperidone for the treatment of psychosis, and had no known systemic, endocrine, or neurological disease. The appropriateness of risperidone treatment for patients was made in conjunction with treating clinicians. The study sample included 30 participants (19 men, 11 women). Nineteen (63%) participants had no prior lifetime exposure to antipsychotic medications and all participants were antipsychotic free for 4 half lives or 5 days of any prior oral treatment at the time of the initial study assessments. The timeframe of any previous antipsychotic exposure was determined through current or previous treating clinicians, patient medication history interviews, family or caregiver interviews, and medical record reviews. Seventeen participants were recruited as outpatients and 13 were inpatients at the initiation of study procedures. Baseline assessments were completed prior to the initiation of risperidone and follow-up assessments were completed after four weeks of treatment. Diagnoses were assigned according to Diagnostic and Statistical Manual of Mental Disorders fourth edition (DSM-IV) criteria by trained raters administering the Structured Clinical Interview [First et al. 1995], along with collateral clinical data which were reviewed at consensus diagnosis meetings. Demographical data and clinical ratings were assessed by trained clinicians and raters, and included the Brief Psychiatric Rating Scale (BPRS) [Overall and Gorham, 1962] to assess clinical symptoms over the course of treatment. Blood draws before and after 4 weeks of treatment were completed by trained nursing or phlebotomy staff between 6:00 am and 12:00 pm. Risperidone was dosed in a flexible manner as indicated by treating clinician prescribers (median dosage 3 mg/day; range 0.5–6 mg/day).
Laboratory assessments
Blood (10 ml) was collected for the assessment of N-telopeptide crosslinks (NTx), osteocalcin, prolactin, estradiol, and free testosterone. These measures were selected based on prior established relationships with bone metabolism or antipsychotic-associated hypogonadism. Samples were drawn in red top BD Vacutainer (Franklin Lakes, NJ, USA) blood collection tubes with silicon clot activator. Serum was separated via centrifugation at 1800g for 15 min in a 4°C centrifuge. Serum samples were aliquoted and stored at −80°C until analysis. Laboratory assessments were completed in the UIC Pharmacogenomics Laboratory. Commercially available enzyme-linked immunosorbent assay (ELISA) procedures were used to determine serum concentrations for hormones and peptides using a BioTek Synergy HT Multidetection Microplate Reader (Winooski, VT, USA; www.biotek.com) according to manufacturer specifications. All samples were batched by assay and were completed in duplicate. Prolactin ELISA (ALPCO Diagnostics, Salem, NH, USA) has a sensitivity of 2 ng/ml, range 0–210 ng/ml, intra-assay coefficient of variation (CV) of 2.1–4.6%, and inter-assay CV of 3.1–7.4%. Estradiol ELISA (ALPCO Diagnostics) has a sensitivity of 10 pg/ml, range 0–3200 pg/ml, intra-assay CV of 4.6–9.3%, and inter-assay CV of 6.2–10.1%. Testosterone (free) ELISA (ALPCO Diagnostics) has a sensitivity 0.17 pg/ml, range 0–125 pg/ml, intra-assay CV of 4.7–17%, and inter-assay CV of 5.3–12.4%. Osteocalcin (Intact) ELISA (ALPCO Diagnostics) has a sensitivity of 0.08 ng/ml, range 0–75 ng/ml, intra-assay CV of 3.1–4.7%, and inter-assay CV of 3.5–5.6%. NTx ELISA (Wampole Laboratories, Princeton, NJ, USA) has a sensitivity of 1.3 nM bone collagen equivalents (BCEs), range of 0–40 nM BCEs, intra-assay CV of 4.6%, and inter-assay CV of 6.9%.
Statistical analyses
Our primary hypothesis was that prolactin elevation observed early in treatment with risperidone would be associated with changes in markers of bone turnover. Given the prior relationships between high prolactin and lower BMD values in patients receiving antipsychotics and in patients with prolactinomas, we hypothesized that higher prolactin levels would be associated with increases in bone resorption and decreases in bone formation. We also examined other hormones that are part of the pituitary–gonadal axis (i.e. testosterone and estradiol). To meet the assumptions for parametric analysis, non-normal distributions were normalized using natural log transformations. To examine the degree to which bone and hormone markers changed with treatment, we used mixed effects regressions in which the two measurement time points (i.e. baseline and 4 weeks) were nested within individuals. For these analyses, we examined the effect of treatment (baseline and 4 weeks; level 1 in model) on bone markers and hormone levels adjusting for age, sex, dose, and baseline body mass index (BMI). Next, Pearson correlations were calculated to evaluate whether bone markers impacted by treatment (e.g. NTx) were related to changes in hormone levels that were affected by treatment (e.g. prolactin). Finally, exploratory correlational analyses were conducted to examine how risperidone dose related to endpoint bone markers and hormone levels that were impacted by treatment. This was done to assess whether dose as a non-laboratory variable is an informative clinical parameter for the outcomes assessed herein. Owing to our small sample size, we analyzed all subjects together controlling for sex for our primary analyses. Recognizing the importance of differences between men and women for some of the biomarkers assessed, we also conducted post hoc exploratory analyses stratified by sex. While not powered to detect treatment effects or differences between men and women, this information was intended to identify potential trends for hypothesis generation and future exploration. Within group effect sizes generated from paired comparisons (pre and post treatment) were calculated to generate Cohen’s d values for these relationships. All p values are two sided, and the statistical significance level was set at p = 0.05. Analyses were performed using SAS (version 9.2, SAS Institute Inc., Cary, NC, USA).
Results
Global symptoms of psychosis were of moderate severity (mean BPRS total scores of 44.6 ± 6.2) at baseline and significantly improved (p < 0.001) after treatment. Table 1 summarizes clinical and demographical data.
Baseline demographic and clinical characteristics of overall sample (N = 30).
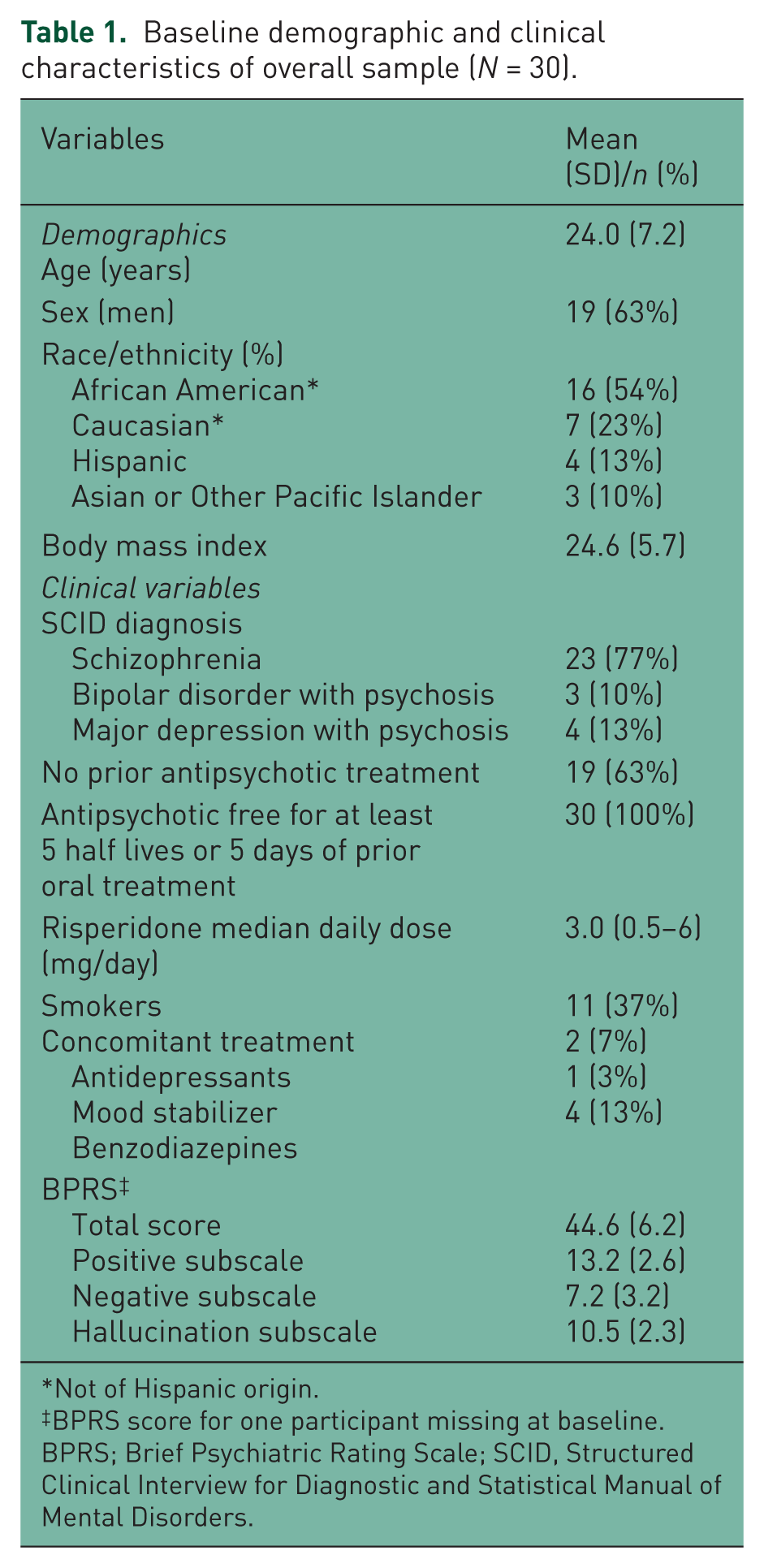
Not of Hispanic origin.
BPRS score for one participant missing at baseline.
BPRS; Brief Psychiatric Rating Scale; SCID, Structured Clinical Interview for Diagnostic and Statistical Manual of Mental Disorders.
Participants were all treated with the antipsychotic risperidone (median daily dose 3 mg/day, range 0.5–6 mg/day).Table 2 summarizes changes in serum hormone and bone marker concentrations after treatment adjusting for sex, age, BMI, and risperidone dose. Mean NTx values decreased from 18.31 ± 1.49 nM BCE before treatment to 15.50 ±1.22 nM BCE after treatment (p < 0.05), representing a moderate absolute effect size (ES, d) of 0.4. Of the sample, 63% showed this decrease (post–pre treatment <0 nM BCE) in NTx after treatment, while 37% had values which increased (post–pre treatment >0 nM BCE). Prolactin levels significantly increased from 12.1 ± 1.9 to 65.7 ± 12.2 ng/ml after treatment (p < 0.001). All participants had post-treatment prolactin levels that were greater than baseline. Osteocalcin, NTx:osteocalcin ratios, estradiol, and testosterone did not significantly change after treatment (all p > 0.05, ES 0.14–0.3). When looking at changes in hormones and bone turnover markers separately in men and women, the directions and magnitudes of change were similar to those observed in the whole group.
Mean (SE) and change scores across time for bone markers and serum hormone levels for all patients.

Analyses in the overall sample adjusted for sex, age, body mass index, and risperidone dose.
BCE, bone collagen equivalent; NTx, n-telopeptide crosslinks.
We then examined the correlations between changes in NTx after treatment with changes in other markers impacted by treatment (prolactin) and dose. Notably, a trend was observed when assessing the correlation between the magnitude of change in prolactin to the change in NTx after treatment (r = 0.33, p = 0.07; see Figure 1). Important to the interpretation of this correlation is that a sample size of 70 would be needed to obtain p < 0.05 for a relationship at this magnitude. There were no significant associations between risperidone dose and prolactin (r = 0.06, p = 0.77), or NTx (r = 0.27, p > 0.05).

Relationship between changes in prolactin with treatment with changes in NTx with treatment.
Discussion
This study describes changes in serum hormones and markers of bone turnover observed early in treatment with the antipsychotic risperidone in individuals with psychosis who had little or no prior antipsychotic exposure. To our knowledge, this is the first study to examine the acute effects of risperidone exposure on markers of bone turnover and relationships with prolactin, testosterone, and estradiol. Our results identify potentially important drug-related effects that may help to better elucidate the mechanisms of antipsychotic influences on bone homeostasis. Our a priori hypothesis was that risperidone-associated prolactin elevation would be related to changes in bone turnover as measured by osteocalcin or NTx. We anticipated identifying increases in NTx markers of bone resorption or decreases in osteocalcin markers of bone formation. In this study sample, NTx markers of bone resorption, but not osteocalcin markers of bone formation, changed during the acute phase of risperidone treatment. Increases in prolactin were observed as expected. Estradiol and testosterone did not change over the course of treatment. In this study sample, NTx markers of resorption on average decreased after treatment, and these decreases appear to occur in those with less robust increases in prolactin. Interestingly there was a trend indicative of a positive correlation between increases in prolactin and increases in NTx, suggesting that greater increases in prolactin were correlated with potentially deleterious increases in bone resorption. We did not observe a statistically significant relationship between risperidone dose and the outcomes described herein.
Exposure to antipsychotics results in a number of physiometabolic changes. As a result, it has been difficult to determine exactly what pharmacological consequences of drug administration cause or influence changes in bone metabolism. In the absence of antipsychotic treatment or other causes of prolactin elevation, dopamine signaling through dopamine D2 receptors on the anterior pituitary modulates prolactin release. D2 antagonism from antipsychotic medications like risperidone disinhibits this negative feedback, resulting in prolactin elevation [Fitzgerald and Dinan, 2008]. Extended periods of elevated prolactin suppress gonadotropin-releasing hormone, luteinizing hormone, follicle-stimulating hormone, and subsequently testosterone and estrogen [Tresguerres et al. 1981; Bhasin and Serdloff, 1985; Bartke et al. 1987]. Data from hyperprolactinema studies in nonpsychiatric patient populations, largely in the context of prolactinomas, implicate related gonadal dysfunction as an underlying mechanism for bone loss in women and men [Shibli-Rahhal and Schlechte, 2009]. In this context, the clinical relationship between prolactin elevation and changes in bone density appears to correlate with menstrual dysregulation in women. In studies of patients with prolactin elevation during chronic antipsychotic treatment, hypogonadism has also been observed [Smith et al. 2002; Kinon et al. 2003; Huber et al. 2005; O’Keane and Meaney, 2005; Kishimoto et al. 2008]. Studies in rodents and nonhuman primates also illustrate that chronic treatment with risperidone lowers BMD by increasing bone resorption [Kunimatsu et al. 2010; Sackett et al. 2010], and that this increase in resorption is related to prolactin elevation and reductions in estrogen.
In addition to these indirect effects of hyperprolactinemia on bone physiology, accumulating evidence also suggests that prolactin may have direct effects on bone. Osteoblasts express prolactin receptors and in rodent models, the effects of increases in prolactin appear to be related to age [Krishnamra and Seemoung, 1996; Seriwatanachai et al. 2009]. Elevating prolactin may reduce osteoblasts by slowing proliferation [Seriwatanachai et al. 2009]. Furthermore, prolactin elevation in mature rats increases the rate of calcium release, resulting in bone loss [Krishnamra and Seemoung, 1996]. Cell culture studies further clarify that exposing MG-63 osteoblast-like cells to prolactin decreases alkaline phosphatase and increases the ratios of receptor activator of nuclear factor κB ligand (RANKL) and osteoprotegerin (OPG) proteins [Coss et al. 2000; Seriwatanachai et al. 2008]. Increasing the ratio of RANKL (which increases osteoclast differentiation) to OPG (which inhibits osteoclast differentiation) [Manolagas, 2000] results in an overall increase in bone resorption.
Taken together these findings indicate that the effects of hyperprolactinemia on bone homeostasis involve a complex interplay of direct and indirect effects. In the context of our short-term study, we observed decreases in bone resorption in patients with less robust increases in prolactin in the absence of any observable changes in estradiol or testosterone. Additionally we observed a trend suggesting that greater increases in prolactin may be associated with increases in bone resorption. It is likely that the extent and timeframe of prolactin elevation observed in our study was not sufficient to result in any indirect effects on bone metabolism from prolactin-associated hypogonadism, as evidenced by minimal changes in estrogen and testosterone after treatment. As previously indicated, longer-term exposure to antipsychotics may be required to suppress this axis, further influencing bone physiology [O’Keane, 2008]. Perhaps increases in bone resorption observed in those with greater prolactin increases were the result of alterations in bone remodeling associated with the direct effects on osteoblasts or osteoclasts. However, we do not have information on other bone physiology markers to help us clarify these relationships. The reasons for the reduction in NTx at lower levels of prolactin change are unclear. We did not collect information on diet before or during the study period that would have been informative in assessing whether changes in nutrient intake influenced this measure.
Until now, the early time course and dose relationships of antipsychotics with bone turnover have not been extensively studied and to our knowledge this is the first investigation to study the acute effects of risperidone on bone turnover in a group of first-episode patients with little prior antipsychotic exposure. In other longitudinal studies, Abraham and colleagues did not find a relationship between prolactin elevation and BMD in women over the course of 1 year of treatment with risperidone or olanzapine [Abraham et al. 2003b]. However, those with prolactin elevation did have higher rates of bone resorption over the course of the study, indicating that a longer timeframe was likely needed to observe the resulting effects on BMD. More recently, evidence was observed that in premenopausal women, treatment for 1 year with prolactin-raising antipsychotics such as risperidone, sulpride, amisulpride, or depot first-generation antipsychotics reduced lumbar BMD compared with patients treated with the prolactin-sparing agent olanzapine [Meaney and O’Keane, 2007].
The findings presented herein need to be interpreted in the context of certain limitations of the study. The study sample examined here is too small to clearly delineate sex differences in relationships between hormone markers and bone turnover. Additionally, our lack of controls and small sample size increases the risk for type 1 and type 2 errors. The flexible dosing strategy employed, while representative of typical clinical practice, likely increased the variability observed in some of the outcomes, but similarly allowed us to gain insight into potentially important effects to examine in future studies. It is unknown whether any of the antipsychotic-associated changes observed here differ based on diagnosis. We were not powered to detect effects by diagnostic category. However, an exploratory post hoc analysis did not identify evidence for differences across diagnostic groups. Other modifying factors may also influence bone homeostasis in patients requiring treatment with antipsychotic agents. These include biological and environmental variables such as diet, smoking, and exercise [Halbreich and Palter, 1996]. We did not examine diet or exercise in these participants but an examination of smoking status (data not shown) did not reveal evidence for associations with bone markers before or after treatment. Finally, this was an acute study examining short-term drug exposure on selected blood-based biomarkers related to bone homeostasis. There are also other biomarkers beyond NTx and osteocalcin not assessed in this study that may be informative for identifying drug-related effects on bone metabolism. It is unclear how these short-term effects translated into longer-term outcomes. In longer-term studies researchers often use DEXA scans as a gold standard for assessing bone density changes over extended periods of time and it will be informative to conduct subsequent studies examining the relationships between blood biomarkers of bone metabolism and bone density from imaging studies.
Risperidone-associated prolactin elevation is common and is observed in most patients treated with this medication [Haddad and Wieck, 2004]. All participants in our study showed an increase in prolactin after treatment. However, there is accumulating evidence that the extent of elevation is important. Our findings indicate that changes in bone metabolism are observed after 4 weeks of treatment and may be related to the extent of prolactin elevation experienced. In light of previous studies identifying relationships between long-term exposure to prolactin-elevating antipsychotics and bone density, this information provides a platform for subsequent investigations. Maximizing the likelihood of clinical response while minimizing side effects is an ongoing struggle, but increasing our knowledge about the mechanisms underlying insidious effects such as the disruption of bone homeostasis and other antipsychotic-associated side effects is an important part of refining and improving the ways we approach drug selection and dosing in patients with psychotic disorders.
Footnotes
This work was supported by the National Institute of Mental Health (grant numbers K08MH083888 to Bishop and R01MH062134 to Sweeney), the American College of Clinical Pharmacy (to Bishop), the University of Illinois Campus Research Board (to Bishop), National Institute of Child Health and Human Development (grant number K12HD055892), and the National Institutes of Health Office of Research on Women’s Health (to Rubin).
Dr Bishop has received research grant support from Ortho-McNeil Janssen. Dr Sweeney has received research grant support from Ortho-McNeil Janssen. Dr Pavuluri is on the Speaker’s Bureau for Bristol-Meyers Squibb. The other authors have nothing to disclose.