
Abstract
Humanoid service robots made swift progress in extending a helping hand to the strained global healthcare during the COVID-19 pandemic. This case provides an overview of the robots’ inclusion in healthcare regarding pre- and intra-pandemic contexts. Specific focus is devoted to humanoid service robots as their shape, size, and mobility make them advantageous in using the physical spaces designed for humans. A collection of examples from hospitals worldwide is presented in illustrating the humanoid service robots’ deployment in healthcare during the COVID-19 pandemic. The pointed future directions aim to facilitate better decision- and policy-making that may ease human anxiety and promote greater acceptance.
Keywords
Introduction
In October 2019, only a few months before the COVID-19 pandemic outbreak, Diligent Robotics managed to raise US$3 million seed funding to launch an autonomous robot assistant to deliver medical supplies and lab samples across the hospital (Muoio, 2019). A few months into the pandemic, robots for hospitals received even further interest, where US$10 million in Series A funding followed (Demaitre, 2020). As of mid-2020, humanoid robots started to serve in hospitals worldwide to collect patient information from those with possible exposure to the SARS-Cov-2 virus, thereby reducing human contact (Chandrayan, 2020). Similarly, human-size robots are used in Rwandan COVID-19 clinics to take patients’ temperatures and deliver supplies (Beaubien, 2020).
Robots not only helped in healthcare during the pandemic, but they also assisted in spraying disinfectants, walking dogs, showing properties for real estate agents (Hayasaki, 2020), cleaning floors in grocery stores, sorting at recycling centers (Howard and Borenstein, 2020), and helping in contactless check-in and supporting security in airports (Hornyak, 2020; Lo, 2018). A recent examination of the reported uses of robots around the globe indicates that they play crucial roles in various aspects of managing the crisis (Figure 1) (Murphy et al., 2020).
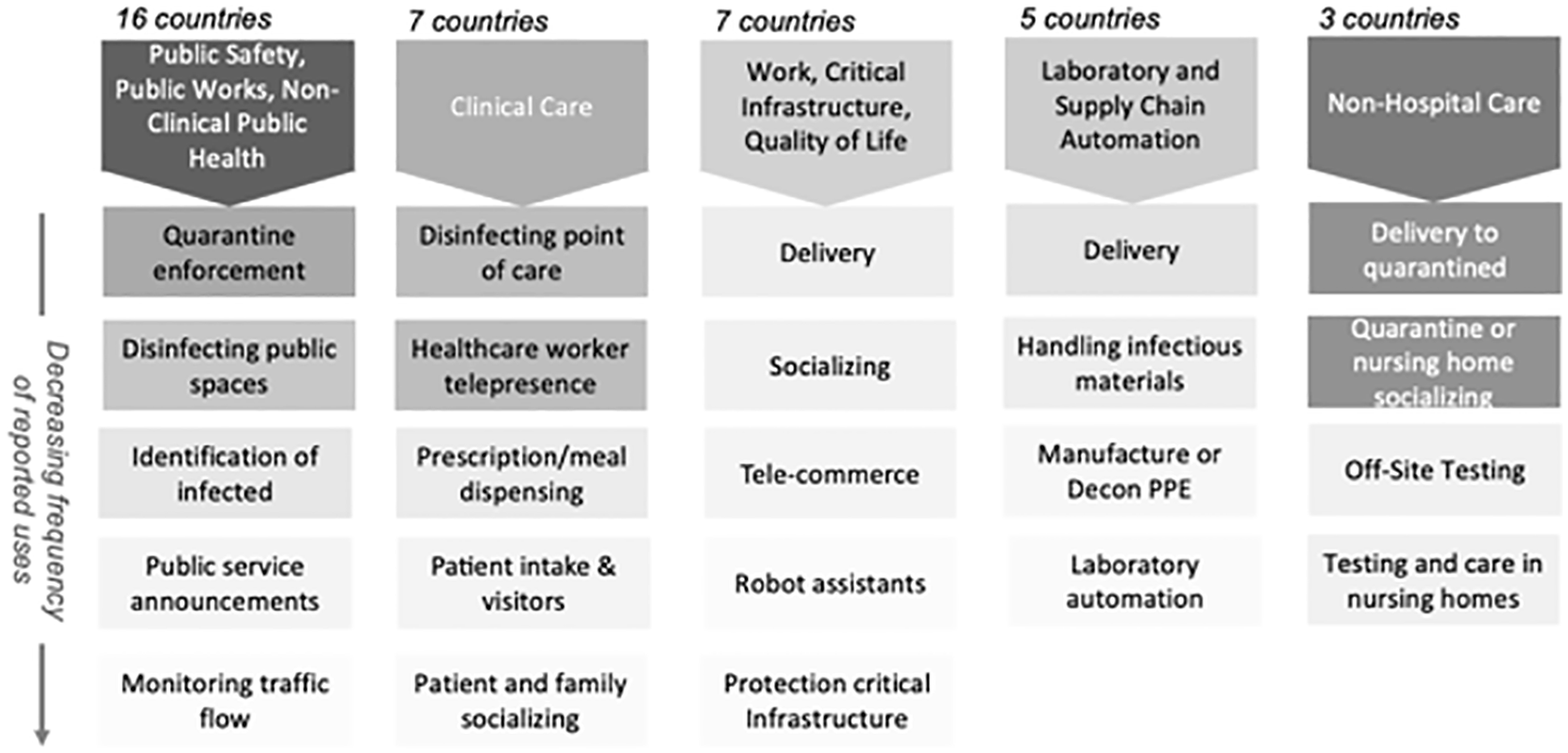
Reported use of robots (ground and aerial) worldwide for COVID-19 as of 20 April 2020.
Robots are believed to help the world resuming “normal” life faster, despite their potential contribution to already high unemployment levels (Glow, 2020). There is a heated debate on whether COVID-19 is speeding up the robots’ use to replace human workers (Thomas, 2020).
Service robots
Robots are considered effective and efficient in providing personalized, on-demand care (Kalb, 2020). Some service robots (SRs) are already being used in elderly care (Kalogianni, 2015; Ochiai, 2019; Toyota, 2018), as well as café and restaurant services (Frey and Osborne, 2017). Mende et al. (2017) mention that SRs’ rise is a double-edged sword with increased user buzz and engagement, on the one hand, but uncomfortable feelings, on the other. There were times when the marketplace emotions toward robots turned from excitement and empathy toward anger and fear due to several entrepreneurs’ warnings against uncontrolled artificial intelligence (AI) and increased use of robots for the defense industries (Mattel, 2015; Ozturkcan and Merdin-Uygur, 2018). In coincidence with these findings, people were exposed to videos depicting crash-tests with dummies or defense robots tested against human violence (Darrow, 2016). All-in-all, socio-technical and contextual influences on SR deployment are stimulating research areas, especially in healthcare (Garmann-Johnsen et al., 2014).
SRs in healthcare
Researchers started to investigate about healthcare robots a decade ago (Broadbent et al., 2009; Hansen et al., 2010). Since then, robots and their uses advanced to many areas that range from complex assignments involved in surgery and prosthetics (Bogue, 2011) to the simple tasks of checking blood pressures (Broadbent et al., 2010) as well as continuous assignments involved in the medication management services (Datta et al., 2013) or assisted living at home for the elderly and disabled (Harmo et al., 2005).
A classical theory of technology acceptance (Davis, 1989) seeks to explain and predict human behavior based on perceived usefulness and perceived ease of use. Relatedly, humanoid robots’ perceived usefulness and perceived ease of use by the doctors and nurses are likely to play a critical role in their acceptance as a new technology in their working life.
Acceptance toward SR is also highly related to certain demographics such as age, gender, personality, and culture. Blood pressure monitoring proved to be one of the prevalent situations that attracted researchers’ attention, where findings indicate differences in age and gender in acceptance toward the robots (Kuo et al., 2009). In healthcare activities, for example, extroverted female robots were preferred, and introverted male robots were preferred in protection positions (Tay et al., 2014). Culture Aware Robots and Environmental Sensor Systems for Elderly Support (CARESSES 1 ) is a European Union (EU)-funded project that seeks to create the first culturally knowledgeable robots to care for older adults (Riva and Riva, 2019).
Previous experiences with robots in different domains (i.e. entertainment) tend to impact the perceptions of encounters with robots in healthcare settings, too. Negative attitudes by the healthcare professionals with limited exposure to robots were reported in a recent study conducted in Finland, where robots were only welcomed for assisting with specific tasks such as heavy lifting and logistics (Turja et al., 2018). Japanese healthcare professionals’ more welcoming attitudes toward the care robots in comparison with that of the Finnish healthcare professionals (Coco et al., 2018) might also be attributed to their past experiences with robots in different fields. Along similar lines, “tech-resistance” within the nursing profession (Salzmann-Erikson and Eriksson, 2016) and negative attitudes toward inclusion of robots in healthcare (Göransson et al., 2008) are reported in studies with samples of Swedish healthcare professionals. On the other hand, it is estimated that robots can do at least 20% of nurses’ work in hospitals and long-term elderly care (Ministry of Social Affairs and Health, 2018). The inclusion of robots can help curb the rising social welfare and healthcare costs and improve healthcare professionals’ work content.
On the other hand, several concerns have been raised regarding robotic healthcare’s negative outcomes on the patients’ side. Especially among the elderly, several considerations are presented regarding dehumanization, increased social isolation and neglect by physical caregivers, emotional attachment toward robotic caregivers, anger, frustration, and even rejection (Veruggio et al., 2016).
Humanoid SR
The humanoid, also referred to as anthropomorphic, is defined as imbuing the imagined or real behavior of nonhuman agents with human-like characteristics, motivations, intentions, and emotions (Epley et al., 2007). Past research indicates that the level of anthropomorphism, the kind and type of interaction with the humanoid SR, and the level of personal characteristics such as power and status influence how individuals form and report attitudes toward robots (Ozturkcan, 2018; Ozturkcan and Merdin-Uygur, 2018). Also seen as the humanization of robots, humanoid SR raise some concerns (Robert, 2017) in terms of their impacts on individuals’ emotions as well as expectations and interactions (Gallagher et al., 2016; Giger et al., 2019; Kemenade et al., 2015a, 2015b). According to the uncanny valley theory (Mori, 1970; Mori et al., 2012), human-like SR evokes discomfort (Moosa and Ud Dean, 2010) and eeriness in human beings (Appel et al., 2020; Cameron et al., 2021; Van Pinxteren et al., 2019). These feelings are most of the time accompanied by feelings of being threatened (Gray and Wegner, 2012), mortality salience (MacDorman, 2005), fear of job loss (Savela et al., 2021), and dystopic robot-domination ruminations (Ray et al., 2008). However, some experts point out that digital interactions with humanoid SR could be better off than the automated faceless kiosks (Goertzel, 2019). This argument can be extended in comparing humanoid robots with wheeled, legged, or flying mobile robots or wearable robots (Tavakoli et al., 2020). All in all, humanoid SR seems advantageous in comparison with other forms of SR by adapting to physical spaces built for humans with their human-like shapes, sizes, and motions. However, humanoid SR’s inclusion in services remains unexplored despite promising opportunities (Berry et al., 2020). Little is known about the possible social-technological acceptance of the humanoid SR apart from recent research looking into the robotic service failure attributions (Leo and Huh, 2020).
Humanoid SR in healthcare
“Will we have robot colleagues at work?”
Robotics technology providers mention that the healthcare culture can be seen both as a driving factor and a limiting one (Lanne et al., 2020) toward the inclusion of humanoid SR in healthcare services. Among many reservations, the discussion surrounding robots’ presence in the work-life (Van der Zande et al., 2018) can be further amplified with the humanoid SR.
Humanoid SR functions in healthcare involve advanced mentoring roles such as physiotherapists’ (Bhuvaneswari et al., 2013) or contributing to human–robot health teams in performing complex cognitive/analytical and complex emotional/social tasks (Wirtz et al., 2018). While AI-supported SR may function as rare disease detecting algorithms, teaming up AI with a physical nurse or doctor with soft skills like displaying empathy and communicating to decrease psychological discomfort is advised (Roongruangsee et al., 2016).
Accelerated inclusion of humanoid SR in healthcare during the COVID-19 pandemic
The COVID-19 pandemic accelerated the inclusion of humanoid SR in healthcare. The suddenly increasing demand in healthcare nurtured an atmosphere where any possible help was embraced. Moreover, the possibility to minimize or eliminate contact with patients promoted an opportunity to protect the precious healthcare workforce from contracting the virus. The scarcity observed in personal protective equipment (PPE) was also minimized. By eliminating the need for donning and doffing PPE, which also included a time-consuming protocol to wear and take off, doctors and nurses were provided with more time to dedicate to their patients, too. When hospital visits were no longer a possibility, humanoid SR helped with connecting patients with their families for morale and support.
In India, humanoid SR, named Mitra, assists the COVID-19 patients in the hospital beds to connect with their loved ones through a tablet installed in its chest (SCMP, 2020). Mitra’s human colleagues stress the prolonged recovery period together with bans on hospital visits as problematic, especially with the COVID-19. Patients also reflect that the hospital’s loneliness was depressing before Mitra helped them and indicate feeling much better afterward. They can talk to their families and friends during a period when they need their support the most. Besides, Mitra can check temperatures and even facilitate a patient to consult with a psychiatrist upon need. Mitra includes a facial recognition technology that recognizes the people it has met before; therefore, it can identify the patients independently. Furthermore, Mitra also assists in remote consultation, mostly when it can protect the at-risk specialists from possible infection. Another humanoid SR was also used to deliver vital supplies such as food and medicine to patients in different parts of the hospitals (AlJazeera, 2020).
Mitra was also employed in Bangalore (Fortis, 2020) to screen each entering individual to a hospital in the following suit. Through its facial and speech recognition, Mitra screens the doctors, nurses, medical, and non-medical staff for COVID-19 symptoms such as fever or cough. Through Mitra’s support in identification and referral, the human healthcare workers can maintain their safe distance from the symptomatic patients.
As a donation from the United Nations Development Program, humanoid SR was also used in Rwanda for up to 50% of technical work, such as taking vitals (i.e. checking temperature, monitoring patients) and recording messages to give feedback in clinical judgments to the human healthcare staff (Reuters, 2020). The deployed humanoid SR minimizes contact between patients and human healthcare workers, thus decreasing the transmission.
Another humanoid SR, nurse Tommy, helped Italy’s frontline staff (AlJazeera, 2020; YahooNews, 2020). Tommy facilitated the connection between the doctors and patients without direct contact. As a consequence, less PPE was consumed, which saved both time and money. Perhaps more importantly, fewer doctors and nurses contracted the virus from their patients. The continuous relay of information on the patient’s immediate situation also helped with the needed medical decisions’ timeliness.
Similarly, the risk of exposure from patients in isolation was minimized by using humanoid SR in Singapore (CNA, 2020). The humanoid SR assigned to making rounds between several isolation wards allowed healthcare professionals to reduce touchpoints that may lead to contracting the virus as they could inspect their patients remotely. Also, conversing more regularly with patients was even possible since the protocol to wear and take off PPE was eliminated in this novel communication method.
In Belgium, a polyglot humanoid SR was assigned to screening patients for coronavirus symptoms and making sure that they wore facemasks during their visit to the hospital (Euronews, 2020). It spoke 34 different languages. The humanoid SR scanned the QR code that the patients are given during the entry, warned those patients who did not wear their facemasks properly, checked their temperatures, and approved their direction toward the relevant department. Through the humanoid SRs inclusion, the needed high level of temperature control was established without leading to long queues in the hospital. In a way, humanoid SR replaced the human actor required to monitor the incoming data from temperature checks.
Sophia, who has been around since the year 2016 as a pioneer humanoid, has also been tasked with a new role amid the COVID-19 pandemic (Reuters, 2021; SCMP, 2021). With her highly developed facial gestures, Sophia is believed to be able to promote human-to-machine communication, empathy, and compassion. Her role as a frontliner involved taking patients’ temperatures, leading morning exercises of the elderly, and fighting against loneliness during social distancing both as a telepresence device and autonomous extension of human expertise.
SR, not necessarily in the form of humanoids, was also used in China for delivering between different parts of a hospital (CGTN, 2020). Thus, they helped reduce the pressure on frontline healthcare and prevented infection transmission between various hospital departments. Humanoid SR nurses were also used in isolation wards in other Chinese hospitals for food, water, and medicine delivery (NewChina, 2020). A year into the pandemic, China built an entire hospital ran by humanoid SR healthcare (Reuters, 2021).
SR robots, also referred to as Ninjas, were used in Thailand to take patient temperature and contact patients through video chat (NowThis, 2020). They helped to minimize infection risk since patients communicated through the SR that stood outside the room.
An SR named James helped the socially distancing elderly keep in touch with their families in Belgium (NowThis, 2020). James fought against loneliness during the COVID-19 restrictions to care-home visits. It connected to the Facebook Messenger service for elderly residents to call their loved ones. James helped both the elderly and their families feel more at ease, even with the lack of physical contact during the trying times.
Implications and future directions
Global healthcare is facing short- and long-term challenges such as demographic changes, demands for increased quality, limited resources, and cost requirements. Robots, especially humanoid SR, offer opportunities for tackling some of these challenges. In the not so far future, the healthcare system needs to be reinvented to possibly include more humanoid SR in different roles to provide improved assistance and service. A better understanding of the drivers, effects, and impact of humanoid SR in healthcare can facilitate better decision- and policy-making that ease human anxiety and facilitate greater acceptance. Moreover, the future regulations encouraging and safeguarding the human–humanoid interaction will possibly influence the degree to which different actors will be open-minded to shared collaborative environments. In other words, the goal should involve creating guidelines that ethically explore the potential of humanoid SR for a positive impact on society. The next generation of humanoid SR could then benefit from proactive policy-making and informed ethical human–humanoid interaction.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Notes
Author biography
![]() .
.