
Abstract
Ontario, the most populous province and the main driver of economic growth in Canada, has been plagued by rising healthcare costs and declining health quality. Firmly believing that care integration is integral to health quality and efficiency of the healthcare system, the Ontario government has embarked on its journey of healthcare system transformation. The case, by taking a snapshot of its transition from the Local Health Integration Network (LHIN) model to the Ontario Health Team model, offers insights into the governance of the LHIN model as well as the initiative of integrating a myriad of healthcare information systems to support care integration. After 12 years’ controversial operation of LHINs, the government dissolved the organization and announced its plan to switch to the Ontario Health Team model. Under the new model, Ontario Health Teams would be responsible for providing a full and coordinated spectrum of care for patients, especially those with complex care needs. Would this round of transformation and emphatic focus on digital health lead Ontario one step closer to integrated care that Ontarians have been chasing for so long?
Keywords
Introduction
On 13 November 2019, Ontario government made a formal announcement that on 2 December 2019, the 14 Local Health Integration Networks (LHINs), the crown agency that had been overseeing community health service delivery for the last 15 years, would be dissolved and replaced by Ontario Health Teams (OHTs), a new mega government agency, Ontario Health.
Their exuberance toward this healthcare system overhaul was evident when the government officials made the announcement. Christine Elliott, Deputy Premier and Minister of Health, remarked, “This transfer will combine the knowledge, strength and expertise of many talented professionals under one roof as part of our plan to better coordinate and connect Ontario’s health care system to end hallway health care.” 1 Doug Ford, Premier of Ontario, pointedly stated, “In order to bring our world-class health care system into the 21st century, we need to get rid of the inefficiencies and back-office duplication. This is how we are continuing to put patients first and ensure sustainability for future generations.” 2
To support the integrated and patient-centered care, the government put forth the Digital First for Health Strategy (DFFH) with the aim to enable system integration and information sharing within OHTs. A variety of information systems were proposed to support patients, caregivers, providers, and healthcare organizations including digital access for patients, online appointment booking, virtual care, better and more connected tools for frontline providers, and data integration and predictive analytics.
Rod Black, Digital Health Program Manager, Ontario Health Central (formerly with the Mississauga Halton Local Health Integration Network), viewed the announcement with mixed feelings. An IT veteran, Black accrued under his belt 11 years of defining annual work plans for provincial, regional, and local digital health priorities and managing overall local digital health budget. He worked closely with local Health Service Providers (HSPs) and provincial delivery partners to ensure on-time project completion. Through his role in coordinating regional and local digital health initiatives for different healthcare providers, Black acutely felt pain points of integrated care attempted by the Ontario government, particularly those of the now legacy, Local Health Integration Networks. After hearing the announcement of OHTs and DFFH, Black wondered, “Would this round of restructuring and emphatic focus on digital health enable integrated care?”
Ontario healthcare crisis and need for integrated care
Ontario, the most populous province in Canada, contributed to 38.6% of Canada GDP (amounts to $851 billion in 2020), the highest among all provinces. 3 Despite being the driver of the Canadian economy, Ontario was facing a healthcare crisis. Over years, although healthcare expenditures steadily increased from $2.8 billion (1974–1975) to $75 billion (202–2022), 4 Ontarians were suffering from prolonged healthcare problems, notably “hallway medicine” and long wait times for care. Every day, roughly 3000 hospital beds (16% of the total) in Ontario were occupied by patients who were waiting to be discharged (hence hallway medicine). 5 Health Quality Ontario reported that in 2017/2018, people spent an average of nearly 16 h in the emergency department, 2 h longer than in 2015/2016, the longest in 6 years. 6 In 2016/2017, people waited 92 days from hospital to move into a long-term care home, 3 weeks longer than in 2015/2016. 7 Dr. David Walker, Provincial Alternate Level of Care (ALC), commented, “… the challenge is not limited to those who are occupying acute care beds when their needs could be better served in other care settings, but our health care system needs to undergo a broader transformation in order to meet the care needs of an aging population” (p. 6). 8
With 156 hospitals, 631 long-term care homes, 14 Community Care Access Centres, 400 Mental Health and Addiction Agencies, and 76 Community Health Centres, Ontario health system was complex, 9 and health services provided by the Ontario health system were inadequately coordinated, overlapping, conflicting. 10 The importance of care integration was relentlessly stressed by the provincial government. For example, in the report Ontario’s Action Plan for Health Care, the Ministry emphasized “patient-centred integration” the right thing to do for both patients and Ontario healthcare system. 11 In Patients First: Action Plan for Health Care, 2015, Dr. Eric Hoskins, the Minister of Health and Long-term Care, stated that care coordination and integration was crucial in improving patients and people’s healthcare experience. 12
What was integrated care? According to the Local Health Integration Act, 2006, integrated care was defined as (1) coordination of services and interactions between different persons and entities; (2) partnering with another person or entity in providing services or in operating; (3) transferring, merging, or amalgamating services, operations, persons, or entities; and (4) starting or ceasing care provision, and ceasing the operations of a person or entity. 13
The Ontario government created Local Health Integration Networks to achieve such integration. LHINs represented a regional health model which was heralded as “a critical part of the evolution of health care in Ontario from a collection of services to a true system that is patient-focused, results-driven, integrated, and sustainable” (p. 1). 14 The vision of LHINs was to improve health planning and integration at the local level.
LHINs: First attempt at integrated care
Fourteen LHINs, non-for-profit agencies, commenced in 2007 its management of health services in their designated geographical area. In accordance with stipulation of the Local Health System Integration Act, 2006, each LHIN was governed by its board of directors. 15 The chair of a LHIN board was accountable to the goals, objectives, and performance of the local health system set by the provincial government. Each LHIN board consisted of no more than 12 members appointed by the Lieutenant Governor. Each board member could serve for a term up to 3 years and no more than 6 years in total.
Each LHIN differed significantly in population they served (see Appendix A). In 2011, of over 12 million people served by all LHINs, over 1.7 million resided in Central LHIN, the most populous region, and 219,188 in North West LHIN, the least inhabited area. In addition, despite the overall increase in Ontario population from 2006 to 2011, the increase varied from LHIN to LHIN (from 0.7% in North East LHIN to 13.6% in Central West LHIN from 2006 to 2011), and some LHINs (Erie St. Clair and North West) even suffered a loss (−1.2% and −5%, respectively).
Moreover, demographic composition was diverse across LHINs. For example, in 2011, the population of those 20 years old or above (20+) in the North West LHIN was the lowest (167,968) and the Central LHIN highest (1, 286,701), an almost tenfold difference. In 2015, the 20+ population of Central LHIN rose to 1,486,871 and that of North West remained the lowest (193,236). 3 LHINs also varied in the number of elderlies. For example, the South West LHIN had the highest percentage of people aged 65 and over (19%), while Central West LHIN lowest (10.7%). In addition, LHINs also differed in the number of ethnic populations. Central LHIN had the highest percentage of population who had no knowledge of official language (4.9%) and North East lowest (0.2%). Furthermore, the percentage of people with chronic diseases varied from LHIN to LHIN. Take diabetes as an example, Toronto Central had the lowest percentage of people with diabetes (9.3%), and North East highest (13.9%) (see Appendix B for chronic diseases distribution across all LHINs).
In 2014–2015, LHINs managed $25 billion expenditures in total, of which hospitals were allocated $16.9 billion, long-term care homes $3.5 billion, and Community Care Access Centres $2.5 billion. 16 As the largest LHIN in terms of population, Toronto Central reported in 2020 over five billion in expenses, seven times of that of North West LHIN (see Appendix A). As of March 2015, the LHINs collectively employed approximately 600 full-time staff with the total operational expenditures amounting to $90 million. 17
Care integration
After its formation, LHINs played its crucial role in planning and integrating local health services. Health Links and bundled care were two notable care integration initiatives.
Health Links represented an “integrated patient-centered approach to care” that focused on patients with multiple chronic conditions and complex needs. 18 Health Links were designed to target the 5% of the patient population responsible for consuming 65% of healthcare resources. Examples of targeted patients included those whose Length of Stay, Acuity, Co-morbidities, ED visits (LACE) score was 8 or higher, who had 5 or more ED visits in last 12 months, and patients who had 2 or more co-morbidities. 19
Health links rested upon coordinated care provided by a cross-professional team of providers (e.g., primary care, hospital, and community care) in a same geographic area. 20 Coordinated care was provided by following seven steps: identifying patient, inviting and engaging patient, gathering information and initiating care plan, sharing information and conducting care conference, updating care plan, and reassessing patient, and patient transitions.
To coordinate cross-professional care, the Ministry put forward the Coordinated Care Plan (CCP), a written or electronic plan “created and maintained by the patient or his or her family, the health care team including physician consultants where appropriate, and when necessary, community services. […] It outlined the patient’s short and long-term needs, recovery goals, and coordination requirements, and it identifies who is responsible for each part of the plan.” 21 The process to create the plan started right after patient hospital admission, when the hospital notified community providers. 22 After the patient was taken over by a local community center, the CCP was used by the care coordinator to monitor services provided and shared by service providers to arrange/update care services needed by the patient.
Bundled care model provided “a single payment to a team of health care providers to cover care for patients both in the hospital and at home.” 23 The intention of the model was to meet patients’ needs in transitioning them back to home, to reduce emergency department visits, and to decrease hospital readmission. The bundled care approach started since 2011 and was first piloted in St. Joseph’s Health System in Hamilton and expanded to six cross-sector healthcare teams in 2015. 24
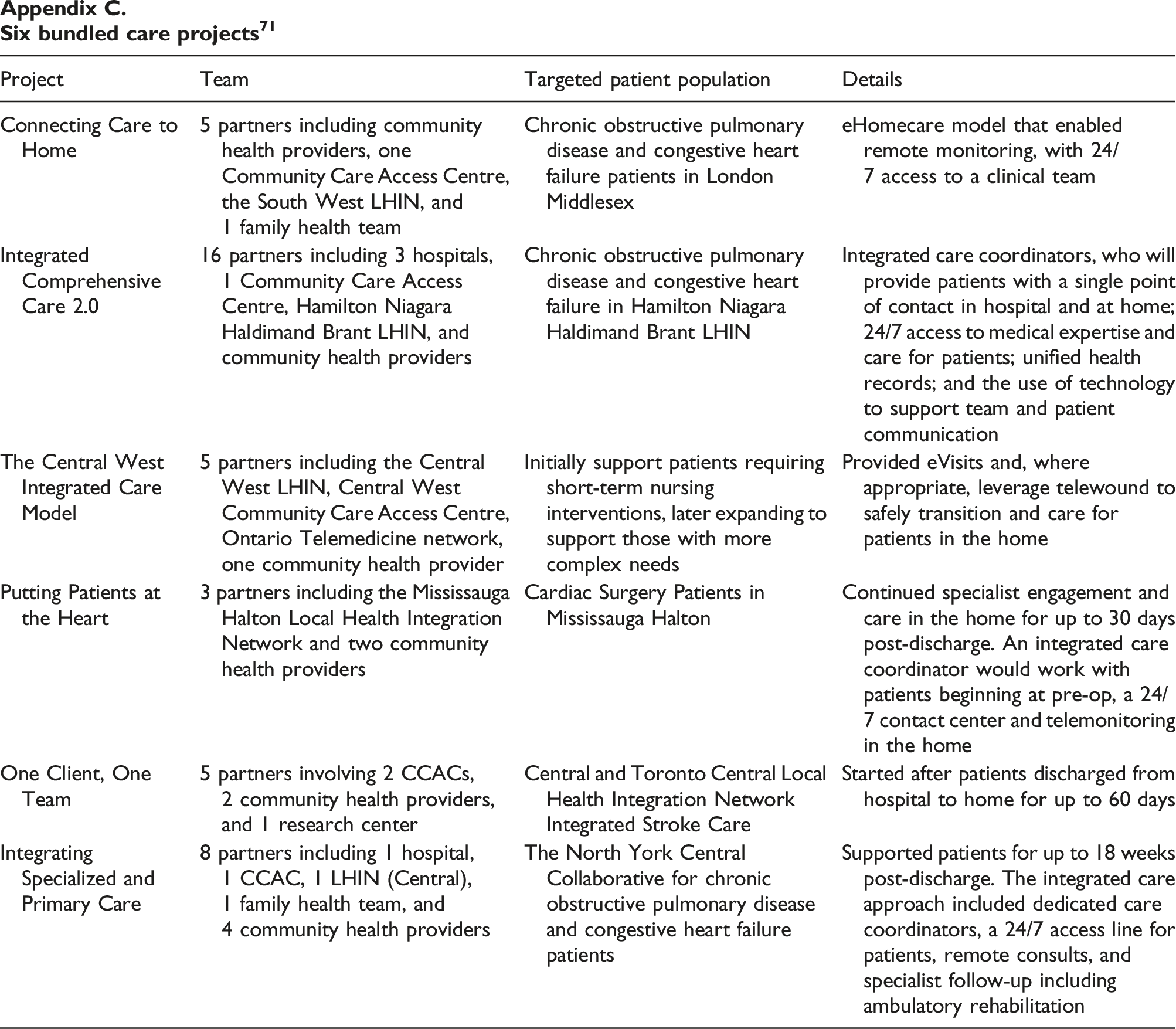
The six teams (see Appendix C for details) were funded for six projects targeting at different populations and diseases, all of which aimed to provide integrated care, reduce duplication and barriers, and create seamless care experience. For example, the program Telehomecare was created to improve the management of chronic conditions (e.g., obstructive pulmonary disease and heart failure), which accounted for significant healthcare costs in Ontario. 25 The program provided patients with 6 months of health status monitoring and self-management education at no cost.
The six teams differed in their composition of care delivery partners (e.g., primary care, acute care, and community care), length of the care (e.g., 30 days, 60 days, and 18 weeks), and care coordination. For example, the Connecting Care to Home project specified that patients would be supported by a clinical team accessible 24/7 and a navigator, a clinical care coordinator, and a dedicated homecare provider. In contrast, the Central West Integrated Care Model project offered no specification of coordinating roles. In addition, these projects varied in supporting technologies including remote monitoring (e.g., Connecting Care to Home, Putting Patients at the Heart), virtual visits (e.g., The Central West Integrated Care Model, Integrating Specialized and Primary Care), and electronic medical records (e.g., Integrated Comprehensive Care 2.0).
Governance of integrated care within LHINs
Unlike the regional model adopted by other provinces in Canada, LHINs did not directly provide health services. Rather, under the Local Health Services Integration Act, 2006, LHINs promoted care integration by negotiating with local health service providers. To guide care integration effort, each LHIN produced an Integrated health Services Plan (IHSP) and service accountability agreements. 26
An IHSP, developed for a 3-year horizon, not only supported the vision and goal of the Ministry but also set priorities that reflected unique needs of its local region. 27 For example, the North West stated its vision statement in its 2016–2019 IHSP: “Healthier people, a strong health system – our future” (p. 10). 28 In contrast, Central East LHIN defined its vision “Living healthier at home” (p. 24). 29
Guided by the IHSP, each LHIN entered into service accountability agreements with local health service providers. These agreements outlined responsibilities, set activity and financial targets, detailed expectations for ongoing development and service delivery, and provided benchmarks to measure performance year over year. 30 The provincial targets set in a Ministry-LHIN Accountability Agreement (MLAA) informed the target levels that needed to be met by local service providers. In the year ending 31 March 2015, all LHINs managed 1700 agreements with 1300 health service providers. 31 Subject to Ministry approval, LHINs could allocate funds between health service providers and health sectors.
Performance indicators
LHIN performance was evaluated quarterly based on the Ministry/LHIN Performance Agreement. The initial set of indicators contained 15 items, which later were expanded to 23 (see Appendix D for the list of indicators), which could be grouped into four categories: access to health services, coordinated healthcare, high-quality health services, and non-hospital. The three indicators for coordinated healthcare included % of Alternate Level of Care (ALC) days, alternate Level of Care rate, and 90th percentile wait time from community for CCAC in-home services. 32 The 2019–2020 provincial target for the indicators of the coordinated healthcare was 9.46%, 12.70%, and 21 days, respectively. 27
In the quarterly report, also called Stocktake Reports, 33 each LHIN’s performance was assessed based on how close its performance was to the provincial target. Each LHIN’s performance was color coded: green for achieved target, yellow for within 10% of target, and red for over 10% from target. For each indicator, an explanation was provided on the LHIN’s performance in the area. For indicators that were below the provincial target, specific action plans were included on how the LHIN planned to improve the performance in the measured areas.
Digital health for integrated care
To support integrated care, patient data should flow seamlessly across service providers. However, Ontario health IT systems were composed of disparate systems residing in with various health service providers. As a result, healthcare data (e.g., patient records, medical examinations, test results, and drugs) were stored and maintained locally, making it difficult to obtain timely and accurate medical information. Quality care was affected as a result.
Developing a province-wide electronic health record (EHR) system, proposed in 2000 by Canada’s federal government, 34 was first tasked to the Smart Systems for Health Agency (SSHA) and later taken over by eHealth Ontario, which was officially enacted in 2008 and funded by the government with the mission to digitize Ontario health systems. In its first strategy report, eHealth Ontario stated its plan to complete the EHR implementation by 2015. 35
To address the disconnected IT landscape, eHealth Ontario intentionally adopted the strategy of connecting existing IT systems (called legacy systems), rather than building a centralized IT system and scraping the legacy systems along the way. 36 Greg Reek, then CEO remarked, “It’s not about reinventing the wheel, but rather providing the highway to ensure they are all spinning in the right direction” (p. 4). 37 In particular, eHealth led/funded many provincial digital health initiatives such as the creation and implementation of Ontario Lab Information Systems (OLIS) and ConnectingOntario. The selected initiatives shall align with specified priorities set by the Ministry. In addition, eHealth identified local digital health needs/opportunities that could benefit from digital health funding. Moreover, eHealth played a critical role of coordinating planning and adoption of information systems at a multi-LHIN scope (e.g., ConnectingOntario and ClinicalConnect).
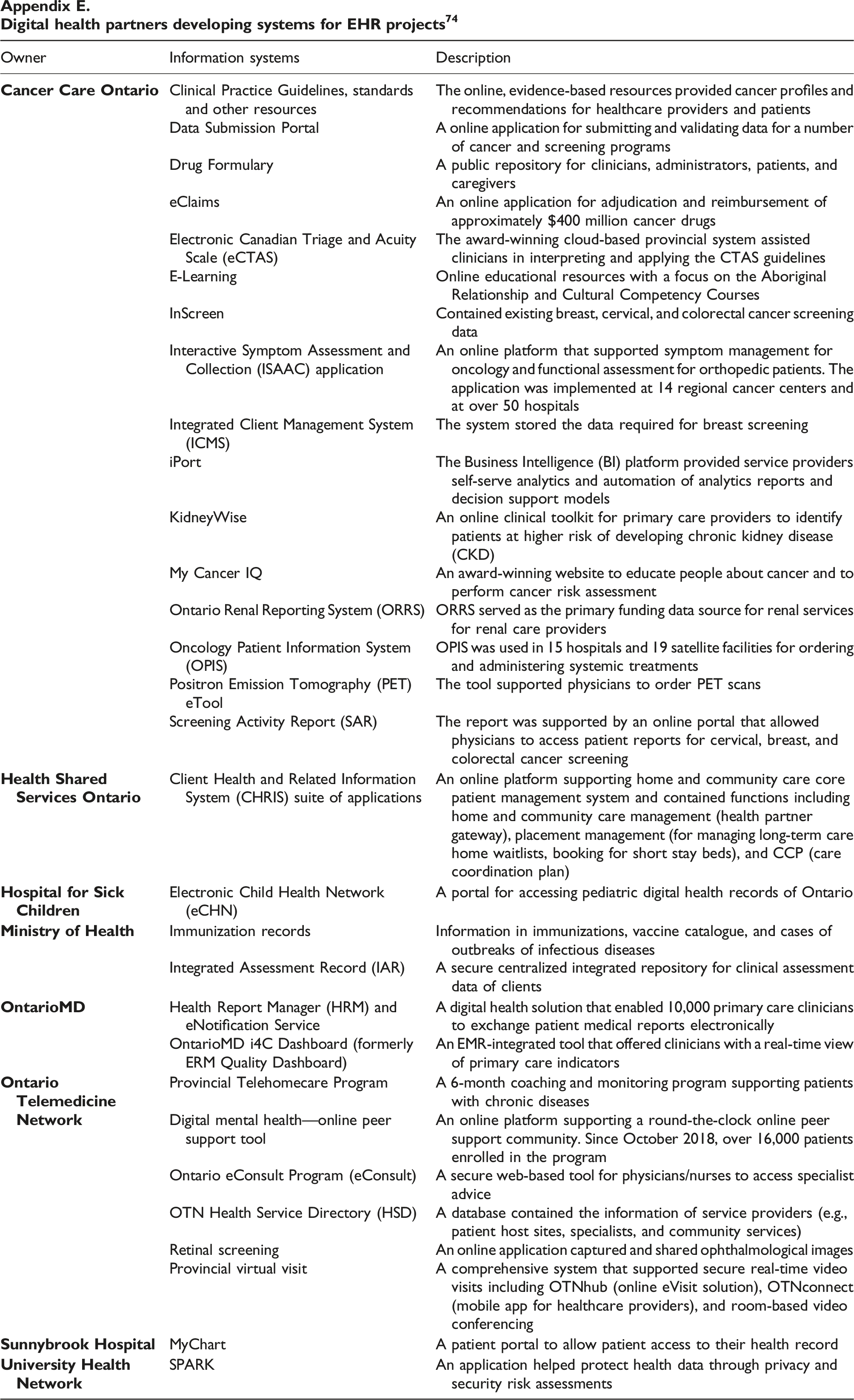
It should be noted that although mandated to connect EHR systems throughout the province, eHealth Ontario had no control over other EHR projects undertaken by digital health delivery partners (see Appendix E on these partners and systems they developed). Each LHIN had its IT resources (e.g., Project Manager, Program Manager, and Director of eHealth) to identify digital health priorities (which were then incorporated in IHSPs) and plan and implement its digital health initiatives.
The Ministry tracked only EHR projects managed directly by eHealth Ontario. Of $ 8 billion invested in EHR-related projects in the period of 2002/03–2015/2016, $3.2 billion was allocated to eHealth Ontario (and its predecessor agency) and the rest to digital health delivery partners including Ontario Telemedicine Network and Cancer Care Ontario ($1.5 billion) and LHINs ($3.7 billion). 38 In 2018, the Ministry put in place a digital health governance organization, the Digital Health Board, to advise on how digital health could be improved and how to best allocate funding. Sitting on the board were the eHealth Ontario CEO, CEOs of selected LHINs, Associate Deputy Ministers from the Ministry, and representatives from healthcare providers. 39
Over years, eHealth Ontario spearheaded the development of EHR projects which could be broadly grouped into three categories (see details in Appendix F) 40 : (1) Provincial clinical applications (e.g., acute care clinical data repository, Ontario Lab Information System (OLIS), Diagnostic images, and eReferral); (2) public-facing services and programs including Immunization, Connect Ontario, ONEMail, and ONE ID; and (3) IT and network infrastructure services (e.g., ConnectingOntario and ClinicalConnect).
Some of the systems were developed to support coordination among care service providers. Client Health and Related Information System (CHRIS), an online platform, supported access and sharing of care coordination plans which was essential to the health links initiative. eConsult, a secure web-based tool, allowed physicians to get advice from specialists. eReferral enabled fast transfer of referrals (e.g., specialist and lab tests) from one service provider to another. MyChart offered integrated patient health records across care providers.
These systems, however, were not without limitations. Care coordination plans, for example, was in the image format, so the information contained in the plans was static. With varying level of IT maturity, not all service providers (e.g., homecare) had the access to the care plan. eConsult was available only to family physicians and nurse practitioners. To use an eReferral system, care providers must use either a shared/linked EMR or an eReferral platform to share patient health information. MyChart was adopted by hospitals, which could grant family caregivers, physicians, and care teams access to patient records.
Mixed views on LHINs
Since their inception, LHINs received mixed reviews. On one hand, LHINs stated that they had succeeded in their community-based, organic, and engaging local approach to healthcare. Statistics over the years indicated positive outcomes achieved through Health Links. For example, since 2013, 89,342 CCPS were developed, 5392 unattached patients found a new primary care physician, 64% of newly identified patients waited 7 days or less to initiate the CCP, and 77% of patients surveyed indicated timely access to a primary care physician. 41
On the other hand, however, the number of patients in Ontario with chronic diseases and conditions continued to increase. 42 There were complaints about insufficient funding. In 2015, physicians in South West Ontario complained the LHINs would not allocate sufficient funds for knee surgeries, resulting in unreasonable wait times for clients. 43 Patient demand for joint replacements in the South West LHIN exceeded the allotted number allowed by the Ministry of Health. 44 There were also critiques that the IHSPS lacked detail and included few specific operational or functional details. This ambiguity left too much room for hospitals and long-term care facilities to shape planning and action while working with the LHINs. 45
Furthermore, it was pointed out that the healthcare system functioned largely in silos throughout the duration of the LHINs. 46 Hospitals, for example, did not know whether discharged patients were getting any homecare. 47 The Auditor General, while recognizing that the formation of LHINs allowed for service providers to “work together to find solutions to common health system issues” (p. 314), 48 concluded that the ministry had not successfully defined what constitutes a “fully integrated health system.” 49 This might contribute to LHINs lackluster performance: while some performance indicators (e.g., the length of stay in emergency rooms) showed improvement, some key performance indicators (e.g., cardiac bypass wait times) showed little performance, and some indicators (e.g., readmissions, repeat visits, and some wait times) even deteriorated. 50
In addition, there existed large variations among LHINs in their performance. For example, the highest-performing LHINs were able to achieve a target set for 10 out of 15 indicators, while lowest-performing LHINs met only 4. The North East LHIN ranked poorly as it met only 4 of the 15 targets set by the government. The Auditor General recommended “to fully realize the value of LHINs, both the Ministry of Health and Long-Term Care and the LHINs themselves need to better ensure the LHINs are meeting their mandate” (p. 314).
Fragmented digital health
The clinical systems developed under the leadership of eHealth Ontario supported a variety of users including service providers, care coordinators, patients, the public, IT systems administrators, and IT developers. According to eHealth Ontario, in 2019, the agency stored over 7 billion records (e.g., patients, test orders, and clinical records) and processed an average of 30 million requests for patient information every month. There were over 98% of hospitals and 100% of home and community care organizations in Ontario that were connected to the systems maintained by eHealth Ontario and over 106,000 healthcare professionals viewed patients’ records at their fingertips. 51
Despite the achievements, however, technological barriers were present during the time of the LHINs, including the lack of shared electronic records, the time taken by clinicians to become literate in new systems, and the need for IT support to manage transitions to new platforms. 52 A recent survey of digital health experts indicated that Ontario Healthcare IT systems still lacked interoperability. 53 Over years, the Auditor General bluntly pointed out a few issues with eHealth projects including the lack of EHR strategy,5455 the lack of a clear budget for eHealth projects, 56 and incomplete patient information in some of EHR systems (e.g., Laboratory Information System) that were up and running. 57 In the 2016 report, the Auditor General pointed out that the EHR project was already over time and there was no clear timeline as to when it would be completed. 58
Ontario Health Teams: Moving closer to integrated care?
The provincial government believed that Ontario Health Teams (OHTs) represented a new way of organizing and delivering care, and cost saving would be achieved after reducing the bureaucracy that troubled LHINs. 59 In their document detailing OHTs, the Ministry of Health and Long-term Care articulated its motivation for the new model, “… patients experience fragmented care as they transition from one provider to the next. They wait too long for care and find that they have to repeat their health history and fill out duplicate forms when moving from one level of care to the next.” 60
Unlike LHINs, OHTs would offer a wider range of services including primary care, secondary care, homecare, rehabilitation, and complex care and were expected to provide a seamless digital health experience for providers, patients, and caregivers. 61 The hallmark of the Ontario Health Teams model was “connected” where patients’ journey in the healthcare system from initial hospital admission to the scheduled home visits would be seamless and smooth. 62
However, the fate of OHTs was shrouded in doubt and uncertainty. 63 As each team would be funded through “an integrated funding envelope based on the care needs of their attributed patient populations” (p. 15), 64 it remained unclear as to how funding would be shared among turf-conscious health service providers. 65 There also lacked a clear direction from the Ministry as to governance within each team. In particular, the Ministry would let teams to determine their own governance structure and offer care based on “the best available evidence and clinical standards, with an ongoing focus on quality improvement” (p. 15). 66 Not only decisions on digital health solutions were also left to each team, but it also remained unclear whether patient data were accessible across OHTs.
Black was concerned with how the current IT systems would facilitate or enable the transition. While placing eHealth Ontario and other agencies under Ontario Health was good news for IT governance, health data were still fragmented. 67 The Ministry of Health admitted that, “consistent standards are lacking across sectors – making it extremely difficult to integrate patient records” (p. 4). 68 Budgeting and planning of digital health was still not entirely collaborative under the OHT structure. Black understood the importance of integrated IT systems to integrated care. He wondered that with Ontario Health overseeing all IT systems in Ontario, whether the Ontario healthcare system was one step closer to integrated care?
Assignment questions
1. What is integrated care? 2. How did the LHIN model work? 3. How was the IT governed under the LHIN model? 4. Did the LHINs fail at implementing integrated care in Ontario? 5. What were the challenges LHINs faced in integrated care? 6. What takeaways from the LHIN model should be applied to Ontario Health Teams?
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Notes
Author biography
▪▪▪
Appendix APopulation and expenses of each LHIN
Population and expenses of each LHIN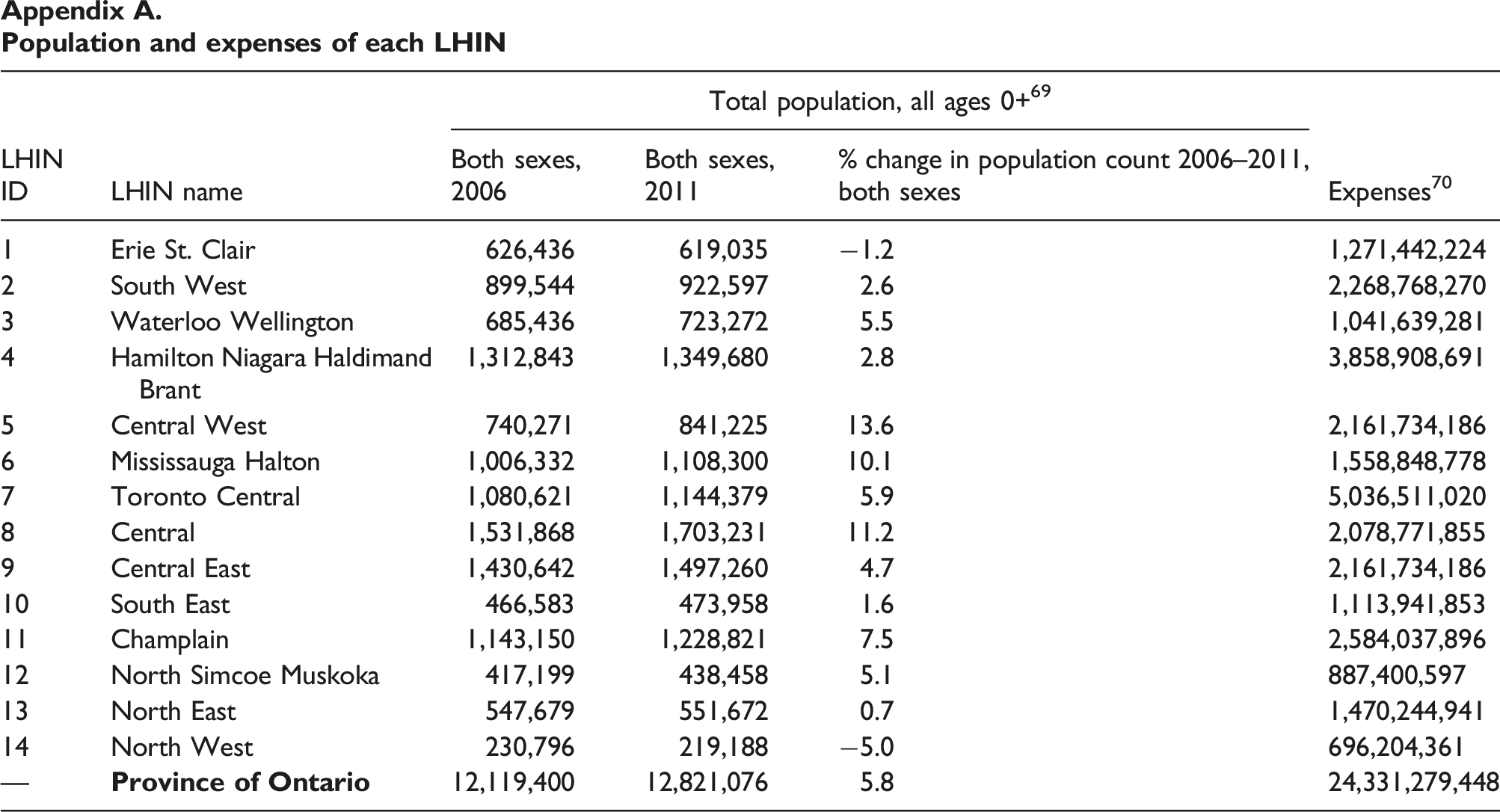
LHIN ID
LHIN name
Total population, all ages 0+
69
Expenses
70
Both sexes, 2006
Both sexes, 2011
% change in population count 2006–2011, both sexes
1
Erie St. Clair
626,436
619,035
−1.2
1,271,442,224
2
South West
899,544
922,597
2.6
2,268,768,270
3
Waterloo Wellington
685,436
723,272
5.5
1,041,639,281
4
Hamilton Niagara Haldimand Brant
1,312,843
1,349,680
2.8
3,858,908,691
5
Central West
740,271
841,225
13.6
2,161,734,186
6
Mississauga Halton
1,006,332
1,108,300
10.1
1,558,848,778
7
Toronto Central
1,080,621
1,144,379
5.9
5,036,511,020
8
Central
1,531,868
1,703,231
11.2
2,078,771,855
9
Central East
1,430,642
1,497,260
4.7
2,161,734,186
10
South East
466,583
473,958
1.6
1,113,941,853
11
Champlain
1,143,150
1,228,821
7.5
2,584,037,896
12
North Simcoe Muskoka
417,199
438,458
5.1
887,400,597
13
North East
547,679
551,672
0.7
1,470,244,941
14
North West
230,796
219,188
−5.0
696,204,361
—
12,119,400
12,821,076
5.8
24,331,279,448
Population with chronic diseases across LHINS
Population with chronic diseases across LHINS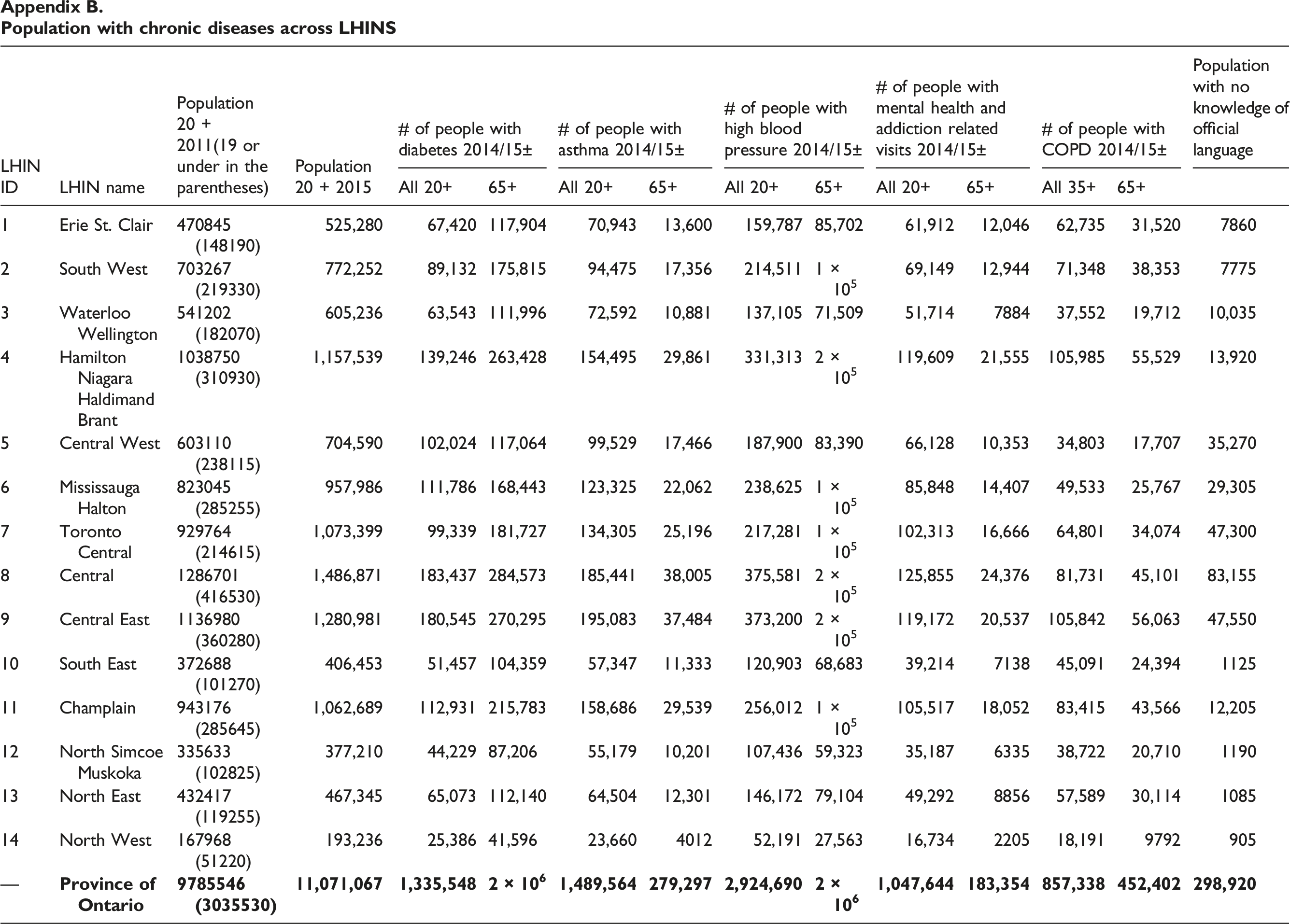
LHIN ID
LHIN name
Population 20 + 2011(19 or under in the parentheses)
Population 20 + 2015
# of people with diabetes 2014/15±
# of people with asthma 2014/15±
# of people with high blood pressure 2014/15±
# of people with mental health and addiction related visits 2014/15±
# of people with COPD 2014/15±
Population with no knowledge of official language
All 20+
65+
All 20+
65+
All 20+
65+
All 20+
65+
All 35+
65+
1
Erie St. Clair
470845 (148190)
525,280
67,420
117,904
70,943
13,600
159,787
85,702
61,912
12,046
62,735
31,520
7860
2
South West
703267 (219330)
772,252
89,132
175,815
94,475
17,356
214,511
1 × 105
69,149
12,944
71,348
38,353
7775
3
Waterloo Wellington
541202 (182070)
605,236
63,543
111,996
72,592
10,881
137,105
71,509
51,714
7884
37,552
19,712
10,035
4
Hamilton Niagara Haldimand Brant
1038750 (310930)
1,157,539
139,246
263,428
154,495
29,861
331,313
2 × 105
119,609
21,555
105,985
55,529
13,920
5
Central West
603110 (238115)
704,590
102,024
117,064
99,529
17,466
187,900
83,390
66,128
10,353
34,803
17,707
35,270
6
Mississauga Halton
823045 (285255)
957,986
111,786
168,443
123,325
22,062
238,625
1 × 105
85,848
14,407
49,533
25,767
29,305
7
Toronto Central
929764 (214615)
1,073,399
99,339
181,727
134,305
25,196
217,281
1 × 105
102,313
16,666
64,801
34,074
47,300
8
Central
1286701 (416530)
1,486,871
183,437
284,573
185,441
38,005
375,581
2 × 105
125,855
24,376
81,731
45,101
83,155
9
Central East
1136980 (360280)
1,280,981
180,545
270,295
195,083
37,484
373,200
2 × 105
119,172
20,537
105,842
56,063
47,550
10
South East
372688 (101270)
406,453
51,457
104,359
57,347
11,333
120,903
68,683
39,214
7138
45,091
24,394
1125
11
Champlain
943176 (285645)
1,062,689
112,931
215,783
158,686
29,539
256,012
1 × 105
105,517
18,052
83,415
43,566
12,205
12
North Simcoe Muskoka
335633 (102825)
377,210
44,229
87,206
55,179
10,201
107,436
59,323
35,187
6335
38,722
20,710
1190
13
North East
432417 (119255)
467,345
65,073
112,140
64,504
12,301
146,172
79,104
49,292
8856
57,589
30,114
1085
14
North West
167968 (51220)
193,236
25,386
41,596
23,660
4012
52,191
27,563
16,734
2205
18,191
9792
905
—
Six bundled care projects 71
Six bundled care projects
71
Project
Team
Targeted patient population
Details
Connecting Care to Home
5 partners including community health providers, one Community Care Access Centre, the South West LHIN, and 1 family health team
Chronic obstructive pulmonary disease and congestive heart failure patients in London Middlesex
eHomecare model that enabled remote monitoring, with 24/7 access to a clinical team
Integrated Comprehensive Care 2.0
16 partners including 3 hospitals, 1 Community Care Access Centre, Hamilton Niagara Haldimand Brant LHIN, and community health providers
Chronic obstructive pulmonary disease and congestive heart failure in Hamilton Niagara Haldimand Brant LHIN
Integrated care coordinators, who will provide patients with a single point of contact in hospital and at home; 24/7 access to medical expertise and care for patients; unified health records; and the use of technology to support team and patient communication
The Central West Integrated Care Model
5 partners including the Central West LHIN, Central West Community Care Access Centre, Ontario Telemedicine network, one community health provider
Initially support patients requiring short-term nursing interventions, later expanding to support those with more complex needs
Provided eVisits and, where appropriate, leverage telewound to safely transition and care for patients in the home
Putting Patients at the Heart
3 partners including the Mississauga Halton Local Health Integration Network and two community health providers
Cardiac Surgery Patients in Mississauga Halton
Continued specialist engagement and care in the home for up to 30 days post-discharge. An integrated care coordinator would work with patients beginning at pre-op, a 24/7 contact center and telemonitoring in the home
One Client, One Team
5 partners involving 2 CCACs, 2 community health providers, and 1 research center
Central and Toronto Central Local Health Integration Network Integrated Stroke Care
Started after patients discharged from hospital to home for up to 60 days
Integrating Specialized and Primary Care
8 partners including 1 hospital, 1 CCAC, 1 LHIN (Central), 1 family health team, and 4 community health providers
The North York Central Collaborative for chronic obstructive pulmonary disease and congestive heart failure patients
Supported patients for up to 18 weeks post-discharge. The integrated care approach included dedicated care coordinators, a 24/7 access line for patients, remote consults, and specialist follow-up including ambulatory rehabilitation
General key performance indicators of the LHINs 72
adenotes 2013-2015 indicators b2015-2018 indicators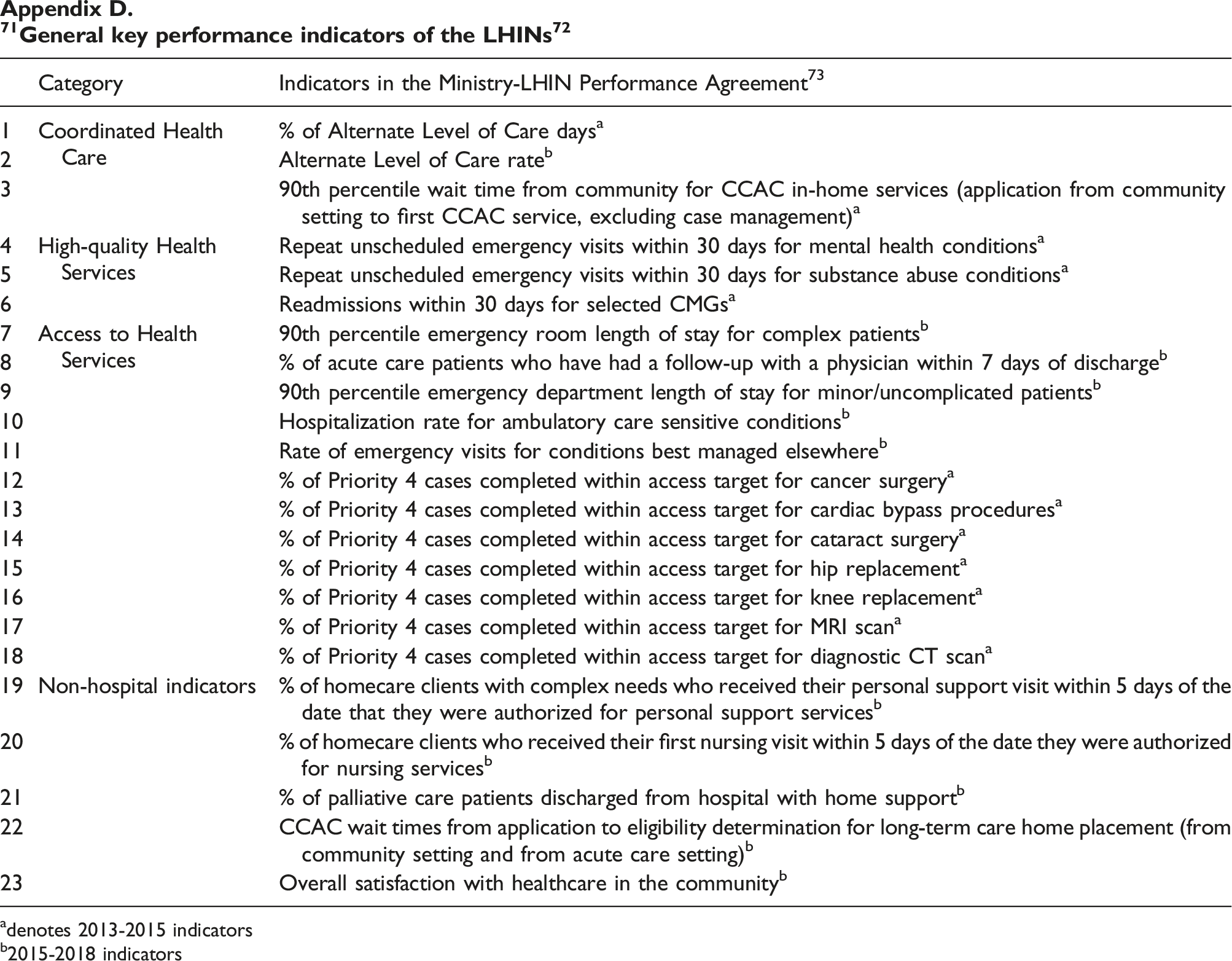
Category
Indicators in the Ministry-LHIN Performance Agreement
73
1
Coordinated Health Care
% of Alternate Level of Care days
a
2
Alternate Level of Care rate
b
3
90th percentile wait time from community for CCAC in-home services (application from community setting to first CCAC service, excluding case management)
a
4
High-quality Health Services
Repeat unscheduled emergency visits within 30 days for mental health conditions
a
5
Repeat unscheduled emergency visits within 30 days for substance abuse conditions
a
6
Readmissions within 30 days for selected CMGs
a
7
Access to Health Services
90th percentile emergency room length of stay for complex patients
b
8
% of acute care patients who have had a follow-up with a physician within 7 days of discharge
b
9
90th percentile emergency department length of stay for minor/uncomplicated patients
b
10
Hospitalization rate for ambulatory care sensitive conditions
b
11
Rate of emergency visits for conditions best managed elsewhere
b
12
% of Priority 4 cases completed within access target for cancer surgery
a
13
% of Priority 4 cases completed within access target for cardiac bypass procedures
a
14
% of Priority 4 cases completed within access target for cataract surgery
a
15
% of Priority 4 cases completed within access target for hip replacement
a
16
% of Priority 4 cases completed within access target for knee replacement
a
17
% of Priority 4 cases completed within access target for MRI scan
a
18
% of Priority 4 cases completed within access target for diagnostic CT scan
a
19
Non-hospital indicators
% of homecare clients with complex needs who received their personal support visit within 5 days of the date that they were authorized for personal support services
b
20
% of homecare clients who received their first nursing visit within 5 days of the date they were authorized for nursing services
b
21
% of palliative care patients discharged from hospital with home support
b
22
CCAC wait times from application to eligibility determination for long-term care home placement (from community setting and from acute care setting)
b
23
Overall satisfaction with healthcare in the community
b
Digital health partners developing systems for EHR projects 74
Digital health partners developing systems for EHR projects
74
Owner
Information systems
Description
Clinical Practice Guidelines, standards and other resources
The online, evidence-based resources provided cancer profiles and recommendations for healthcare providers and patients
Data Submission Portal
A online application for submitting and validating data for a number of cancer and screening programs
Drug Formulary
A public repository for clinicians, administrators, patients, and caregivers
eClaims
An online application for adjudication and reimbursement of approximately $400 million cancer drugs
Electronic Canadian Triage and Acuity Scale (eCTAS)
The award-winning cloud-based provincial system assisted clinicians in interpreting and applying the CTAS guidelines
E-Learning
Online educational resources with a focus on the Aboriginal Relationship and Cultural Competency Courses
InScreen
Contained existing breast, cervical, and colorectal cancer screening data
Interactive Symptom Assessment and Collection (ISAAC) application
An online platform that supported symptom management for oncology and functional assessment for orthopedic patients. The application was implemented at 14 regional cancer centers and at over 50 hospitals
Integrated Client Management System (ICMS)
The system stored the data required for breast screening
iPort
The Business Intelligence (BI) platform provided service providers self-serve analytics and automation of analytics reports and decision support models
KidneyWise
An online clinical toolkit for primary care providers to identify patients at higher risk of developing chronic kidney disease (CKD)
My Cancer IQ
An award-winning website to educate people about cancer and to perform cancer risk assessment
Ontario Renal Reporting System (ORRS)
ORRS served as the primary funding data source for renal services for renal care providers
Oncology Patient Information System (OPIS)
OPIS was used in 15 hospitals and 19 satellite facilities for ordering and administering systemic treatments
Positron Emission Tomography (PET) eTool
The tool supported physicians to order PET scans
Screening Activity Report (SAR)
The report was supported by an online portal that allowed physicians to access patient reports for cervical, breast, and colorectal cancer screening
Client Health and Related Information System (CHRIS) suite of applications
An online platform supporting home and community care core patient management system and contained functions including home and community care management (health partner gateway), placement management (for managing long-term care home waitlists, booking for short stay beds), and CCP (care coordination plan)
Electronic Child Health Network (eCHN)
A portal for accessing pediatric digital health records of Ontario
Immunization records
Information in immunizations, vaccine catalogue, and cases of outbreaks of infectious diseases
Integrated Assessment Record (IAR)
A secure centralized integrated repository for clinical assessment data of clients
Health Report Manager (HRM) and eNotification Service
A digital health solution that enabled 10,000 primary care clinicians to exchange patient medical reports electronically
OntarioMD i4C Dashboard (formerly ERM Quality Dashboard)
An EMR-integrated tool that offered clinicians with a real-time view of primary care indicators
Provincial Telehomecare Program
A 6-month coaching and monitoring program supporting patients with chronic diseases
Digital mental health—online peer support tool
An online platform supporting a round-the-clock online peer support community. Since October 2018, over 16,000 patients enrolled in the program
Ontario eConsult Program (eConsult)
A secure web-based tool for physicians/nurses to access specialist advice
OTN Health Service Directory (HSD)
A database contained the information of service providers (e.g., patient host sites, specialists, and community services)
Retinal screening
An online application captured and shared ophthalmological images
Provincial virtual visit
A comprehensive system that supported secure real-time video visits including OTNhub (online eVisit solution), OTNconnect (mobile app for healthcare providers), and room-based video conferencing
MyChart
A patient portal to allow patient access to their health record
SPARK
An application helped protect health data through privacy and security risk assessments
Systems overseen by eHealth Ontario
Systems overseen by eHealth Ontario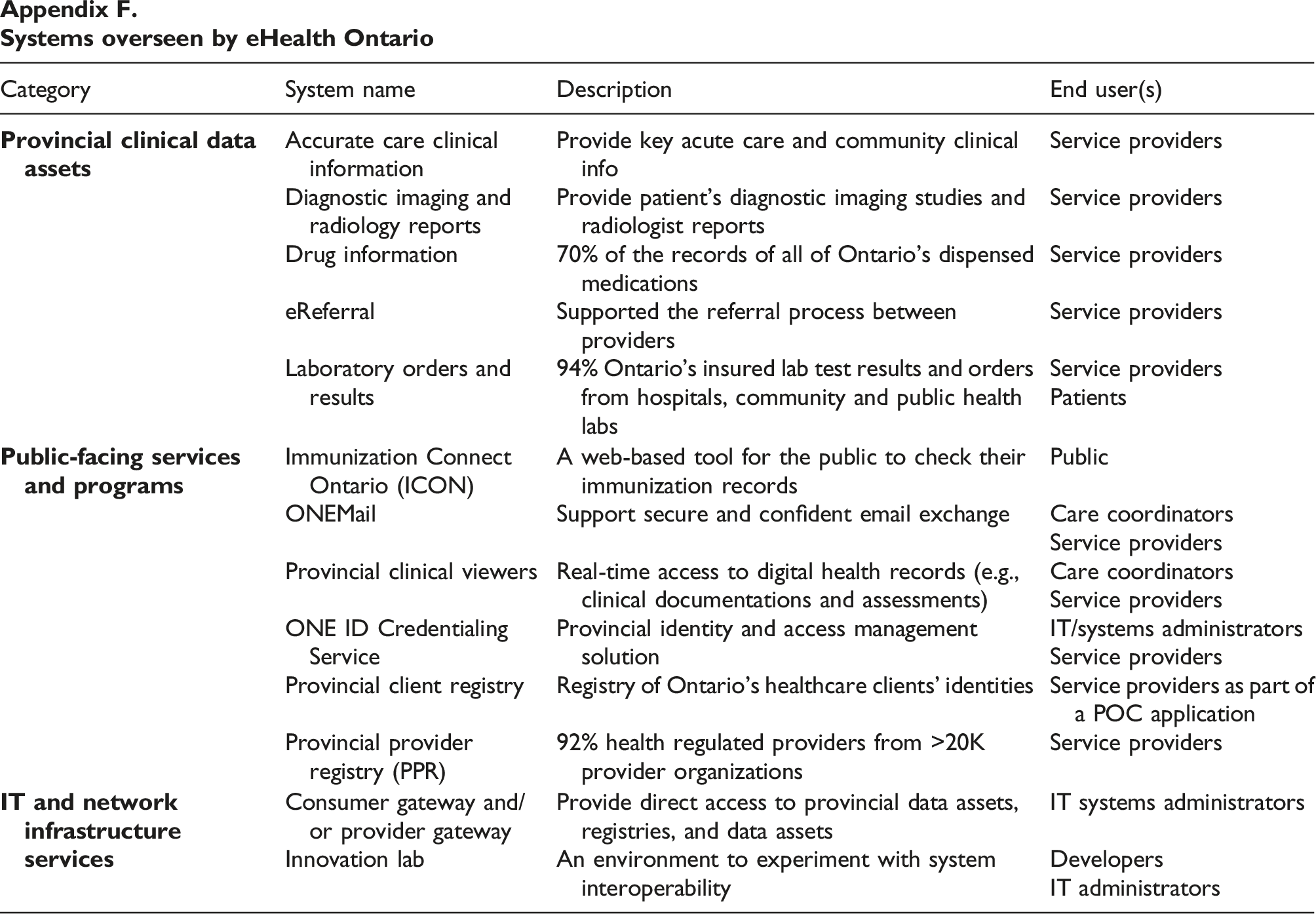
Category
System name
Description
End user(s)
Accurate care clinical information
Provide key acute care and community clinical info
Service providers
Diagnostic imaging and radiology reports
Provide patient’s diagnostic imaging studies and radiologist reports
Service providers
Drug information
70% of the records of all of Ontario’s dispensed medications
Service providers
eReferral
Supported the referral process between providers
Service providers
Laboratory orders and results
94% Ontario’s insured lab test results and orders from hospitals, community and public health labs
Service providers
Patients
Immunization Connect Ontario (ICON)
A web-based tool for the public to check their immunization records
Public
ONEMail
Support secure and confident email exchange
Care coordinators
Service providers
Provincial clinical viewers
Real-time access to digital health records (e.g., clinical documentations and assessments)
Care coordinators
Service providers
ONE ID Credentialing Service
Provincial identity and access management solution
IT/systems administrators
Service providers
Provincial client registry
Registry of Ontario’s healthcare clients’ identities
Service providers as part of a POC application
Provincial provider registry (PPR)
92% health regulated providers from >20K provider organizations
Service providers
Consumer gateway and/or provider gateway
Provide direct access to provincial data assets, registries, and data assets
IT systems administrators
Innovation lab
An environment to experiment with system interoperability
Developers
IT administrators