
Abstract
In the ICD-11, posttraumatic stress disorder (PTSD), adjustment disorder (AjD), and prolonged grief disorder (PGD) belong together to the new grouping of disorders specifically associated with stress, which are all characterized by intrusive core symptoms. As previous studies suggest that intrusive symptoms are associated with attentional biases, it is plausible that PTSD, AjD, and PGD are characterized by the same attentional biases as a transdiagnostic feature. The present study investigated 90 participants with symptoms of PTSD, AjD, or PGD. Individuals with a subclinical symptom presentation were also able to participate, resulting in an analogue sample with the group labels aPTSD, aAjD, and aPGD. All participants completed a symptom induction task to provoke symptoms related to attentional biases. Subsequently, a visual search task (VST) was implemented. This test assessed reaction times to trials that include stress-related, neutral, and generally negative stimuli. The VST featured an interference and facilitation condition to investigate different types of attentional biases. Findings showed that all groups were characterized by particularly fast reaction times to trials which included stress-related stimuli in the interference condition, which indicates a reversed attentional interference bias. This bias has not been reported before and is perhaps related to an avoidance behavior.
Keywords
Introduction
Empirical studies suggest that most individuals experience a traumatic event, a bereavement, or another significant stressor during their lifetime (Karatzias et al., 2022). With the introduction of the ICD-11, the diagnostic guidelines for disorders related to such stressful life events have been improved and specified (Maercker & Eberle, 2022; WHO, 2022). The newly created grouping of disorders specifically associated with stress includes posttraumatic stress disorder (PTSD), complex PTSD, adjustment disorder (AjD), and prolonged grief disorder (PGD). Each disorder features its own profile with a specific combination of symptoms. However, all stress-related disorders are defined by intrusive core symptoms as transdiagnostic similarity (Eberle & Maercker, 2023; WHO, 2022).
Already in 1997, Horowitz categorized different stress-related reactions in one overarching “stress-response syndrome.” He found that after experiencing severe life events, individuals are often profoundly disturbed and shocked by what has happened. Subsequently, the aversive event is reprocessed in the form of intrusive symptoms. Successful cognitive-emotional processing of the aversive life event should finally lead to integration of this experience into one’s identity. It is assumed that such a process generally occurs in stress-related disorders, including PTSD, AjD, and PGD (Horowitz, 1997). This generic process indicates that there might exist a basic underlying mechanism that facilitates the processing of stressful life events in all stress-related disorders. The identification of such an underlying factor could profoundly enhance understanding and classification of these disorders. Even though the theory of Horowitz (1997) is well known, there is, to date, a lack of empirical investigation of all of these theoretical assumptions.
Attentional biases are closely related to intrusive symptoms. Intrusive symptoms include a sustained cognitive attention on a stressor (Wisco et al., 2013). This sustained attention is also a central element of attentional interference (Wisco et al., 2013). Research has shown that a selective attention toward a stressor is manifested in PTSD in the form of re-experiencing as flashbacks (Pineles et al., 2007, 2009). Analogously, it is conceivable that preoccupation in AjD and yearning in PGD also feature such a shift of attention toward the stressful experience (Eberle & Maercker, 2022). For instance, an individual with PTSD might exhibit repetitive memories about a sexual abuse, causing a sustained attentional focus on the trauma. Similarly, an individual with PGD or AjD may exhibit a sustained attentional focus regarding a person lost by a lethal accident or by a divorce. A shift in the attentional focus in grieving individuals has also been demonstrated empirically. For instance, a study by Schneck et al. (2018) showed that bereaved people exhibit a strong attentional focus toward decease-related words, independent of loss type, time since loss, or depression levels. Moreover, it was found that these grief-related attentional biases were particularly linked to intrusive thoughts about the loss. These findings are consistent with the PTSD-based results from Pineles et al. (2007; 2009). Research on bereavement furthermore showed that the selective attentional focus on reminders of the loss is crucial for the development and maintenance of other grief symptoms such as dysphoric mood. It is therefore plausible that an attentional bias represents a general, underlying mechanism of stress-related conditions. This assumption is also consistent with the theory that many groups of mental disorders are based on cognitive and attentional biases, as is the case, for example, for anxiety disorders (e.g., Öhman et al., 2001) or depression (e.g., Joormann and Gotlib, 2007).
In attentional bias theory, a facilitation bias can be differentiated from an attentional interference bias (Pineles et al., 2007). Attentional facilitation is characterized by a particularly fast detection of personally relevant stimuli, which is why facilitation is also labelled as attentional engagement and associated with a hyperarousal or startle behavior (Öhman et al., 2001). Attentional interference is characterized by a sustained focus on a personally relevant stimulus, which is also labelled as attentional disengagement difficulties (Lazarov et al., 2018). It has been demonstrated that individuals who have experienced a stressful life event are not only characterized by the occurrence of an attentional interference bias but also by the absence of a facilitation bias (Pineles et al., 2007, 2009). This attentional pattern was additionally confirmed in meta-analytic evaluations (Lazarov et al., 2018). Furthermore, a study of Bardeen et al. (2020) investigated PTSD patients with eye-tracking methods. The authors found that an attentional interference was specifically associated with reduced attentional control of participants. When attentional control was high, then attentional interference no longer occurred and an avoidance behavior of participants became more prominent. The results show that the investigation of attentional interference, facilitation, and its related constructs, such as avoidance or other stress-related symptoms, can provide meaningful insights into the psychopathology of stress-related conditions.
Past research investigating attentional biases has relied on paradigms such as the dot-probe task or the Stroop task, which measure reaction times to aversive stimuli (for an overview, see Bar-Haim et al., 2007). However, such tests mostly measure one single cognitive bias mechanism, as it is the case for the stroop test, which only assesses cognitive interference (van Maanen et al., 2009). In contrast, newer test procedures allow for further differentiation of attentional mechanisms. The visual search task (VST) is an example for such a test protocol, as it enables a simple but reliable differentiation between interference and facilitation biases (Pineles et al., 2007; Woud et al., 2017). Therefore, research applying VST methods could provide new insights into attentional features of mental disorders. As it can be expected that PTSD, AjD, and PGD are sensitive to facilitation and interference mechanisms, the use of VST to research stress-related disorders could yield particularly promising results. Understanding whether PTSD, AjD, and PGD share an attentional interference bias as transdiagnostic mechanism could have important implications not only for psychopathological classification of stress-related disorders but also for clinical practice. For example, if research would indicate similar attentional processing in PTSD, PGD, and AjD, then a unified psychotherapy program, such as a cognitive bias modification for attentional interference, could be implemented for all individuals who experienced stressful life events.
A connection between attentional biases and psychopathological symptoms might be particularly yielded when symptom induction procedures are included in the study design. Symptom induction tasks, also known as symptom provocation procedures, are well established in psychopathology and psychotherapy research (e.g., De Putter et al., 2017; Lewis et al., 2019; Santa Maria et al., 2012; Woud et al., 2018). In relation to disorders which emerged from a stressful life event, some sort of re-activation is often useful to investigate specific reactions related to the event (see also Santa Maria et al., 2012). As attentional biases are often linked to intrusive symptoms, an intrusion symptom induction task could be particularly advantageous for attentional bias research.
The aim of the research was to examine if participants, divided into the study groups associated with PTSD, AjD, or PGD, are characterized by attentional interference and facilitation biases. Attentional biases are assessed by measuring reaction times to trials which include stress-related, generally negative, and neutral stimuli. It is hypothesized that an attentional interference bias will be observed in all three study groups. More specifically, it is predicted that in the interference condition, individuals in all groups show slower reaction times to trials with stress-related distractors than trials with neutral and negative distractors. Furthermore, it is hypothesized that no facilitation bias would be detected in any of the three study groups. More specifically, it is expected that no significantly different reaction times among stress-related, neutral, and negative stimuli would be detected for the facilitation condition. As interference biases are assumed to be a result of intrusive processes, it is further hypothesized that in the interference condition, reaction times to trials with stress-related stimuli would be positively associated with measures of intrusive processes in all three study groups.
Methods
Participants
Ninety individuals (age: M = 26.91, SD = 9.85; gender: 88.9% female) who had experienced an identifiable and aversive life event with a significant stress reaction in the past 15 years were recruited via public advertisement, mailing lists, personal contacts, or professional networks such as the association of [blinded for review] paramedics. Additional eligibility criteria included a minimum age of 18 years, high subjective distress after and in connection with the stressful life event, and good German skills, which was necessary for the completion of the reaction time tests. Furthermore, all participants completed a diagnostic interview including allocation to the study groups. Participants with a mental health diagnosis were not the only persons who took part in the study. Individuals with a subclinical symptom presentation were also invited to participate, as stress-related reactions are additionally triggered by the symptom induction task (see Woud et al., 2018). Similar to the trauma film paradigm (Holmes & Bourne, 2008), the symptom induction as implemented in this study could be classified as analogue stressor. Henceforth, the description of the study groups was complemented with an analogue add-on, resulting in the group labels aPTSD, aAjD, and aPGD.
Diagnostic interviews were conducted by trained interviewers and in accordance with ICD-11 clinical descriptions and diagnostic recommendations (see Maercker et al., 2013; Perkonigg et al., 2021; WHO, 2022). For example, for the aPTSD group, individuals were required to express symptoms of re-experiencing, avoidance, and persistent perceptions of heightened current threat. In the case of a subclinical symptom presentation, individuals were still required to express the diagnostic symptoms of the corresponding disorder, but in a weaker manifestation. For example, individuals allocated to the aPTSD group might only show few flashbacks, as well as a moderate avoidance and moderate persistent perceptions of heightened current threat. This evaluation was also applied for aPGD and aAjD with the corresponding diagnostic symptoms. aPGD was characterized by the loss of a loved person and PGD symptoms of yearning, preoccupation, and so on. The individuals allocated to the aAjD group were required to express symptoms of preoccupation and failure to adapt, such as sleeping disturbances or concentration problems. This assessment based on the diagnostic symptoms also ensures a valid differentiation of the stress-related disorders included in the present study (see Brewin, 2014; Brewin et al., 2009; WHO, 2022). The diagnostic evaluation was also frequently trained and discussed between the researchers to promote a high assessment quality. Typical severe life events/stressors included involvement into an accident or cases of physical or sexual violence in the aPTSD group, unintended job loss or a divorce in the aAjD group, as well as the death of a loved person in the aPGD group.
Symptom induction
In order to measure and link intrusive symptoms to attentional biases, a symptom induction task was implemented, which was developed by Santa Maria et al. (2012) to specifically provoke intrusive symptoms. In the present study, the adapted symptom induction procedure of Woud et al. (2018) was used: Participants were instructed to report their aversive life event and to determine the distress peak of this experience. Further, participants were asked to describe the stressful moment, including impressions and emotions that were experienced at that time, as if it were happening again. Subsequently, individuals were asked to write a short description of the most distressing situation of the reported aversive life event. Finally, participants were instructed to close their eyes and to imagine the most distressing situation of the aversive event in detail for 30 seconds.
Intrusive process measurements
Sample characteristics.

Note. M = mean; SD = standard deviation. Intrusive symptoms for aPTSD were assessed by the IES-R, for aAjD by the ADNM, and for aPGD by the YSL-SF.
Visual search task
The VST is a reaction time test which measures attentional facilitation and interference biases. Individuals are asked to react to experimental trails which contain different word types, such as stress-related or neutral words. These stimuli are presented in word arrays where one target word needs to be identified as fast as possible. Different reaction times between word types indicate an attentional bias.
Stimuli
The VST featured four stimulus types: stress-related words, neutral words, generally negative words which were not stress-related, and non-words (random letter strings). Apart from non-words, which were implemented in several conditions, each stimulus group consisted of 10 words. The three experimental conditions only differed with regard to the stress-related words: for aPTSD, words like “helpless,” “brutal,” or “shock” were implemented; for aAjD, words such as “crisis,” “disappointment,” or “loss” were used as stimuli; and for aPGD, participants were shown words like “bereaved,” “dying,” or “cemetery.” To select appropriate stress-related stimuli for VST programming, an expert rating took place. Twelve independent experts with research background and clinical experience in the fields of PTSD, AjD, and PGD (four experts per field) were asked to rate a list of words in terms of presumed distress caused in individuals suffering from these disorders. Based on the expert’s ratings, the 10 most distressing words per condition were implemented into the VST. Generally negative and neutral words were implemented into the VST as control and comparison conditions. The purpose of non-words is explained below. Negative words (e.g., “toxic,” “noise,” or “lying”), neutral words (e.g., “paper,” “cottage,” or “flag”), and non-words (e.g., “Copns,” “sodfter,” or “Ramffldwe”) were derived from Wittekind et al. (2019). All presented words were semantically similar to avoid unintended linguistic effects of the study.
Test procedure
Participants started the VST by reading detailed instruction to the test procedure and were given the possibility to ask questions. After written informed consent was obtained, individuals started 20 practice trials with feedback on their performance before proceeding to the experimental trials. One experimental VST trial consisted of a total of eight words, displayed in black font on white background, that were presented simultaneously in a squared array. One word, the target word, differed from the other seven words. The location of the target word in the array of eight words was randomly selected in each trial. Participants were instructed to find the target word and to decide as quickly and accurately as possible whether the target word was a real word or a non-word by pressing a keyboard key. For non-words, participants were asked to press the key “X,” whereas for real words, participants were instructed to press the key “N.” Each trial began with a fixation cross in the middle of a blank screen, followed by the word array and the decision task.
Half of the VST trials were part of the interference condition, the other half were facilitation trials. The facilitation condition consisted of seven non-words in combination with one word (target) that was a stress-related, neutral, or negative word. The array of words in the interference condition always included one non-word (target) as well as seven identical stress-related, neutral, or negative words. For example, one trial of the interference condition in the aPTSD condition consisted of seven times the word “helpless” in combination with one non-word “sodfter.” This way, participants were potentially interfered in their lexical decision due to the presence of the seven stress-related words. Facilitation trials, on the other hand, intended a potential facilitation of attention by finding the target word more quickly. Interference and facilitation trials appeared sequentially within individuals and were balanced between participants.
A total of 160 experimental trials, divided into 4 blocks, were implemented. The four blocks were separated with a break of 30 seconds in-between. All stress-related, neutral, and negative words appeared once in every block. Ten trials per block were catch trials. Those trials consisted of an independent set of neutral words (e.g., “gravel,” “import,” or “content”) and were only implemented for engagement purposes (see also Pineles et al., 2009). Thus, catch trials were not further analyzed in this study. The catch words used in the study were derived from Wittekind et al. (2019). Together with the practice trials at the very beginning of the reaction time test, the VST included a total of 180 trials.
Apparatus and programming
An HP laptop with a 15.7´´ monitor was used for all reaction time tests. The VST was running on Inquisit Version 5.0.14.0 (Millisecond, 2018), which directly recorded all reaction times. The Inquisit script for the VST was adapted from Wittekind et al. (2019).
Study procedure
After interested individuals contacted the study team, a telephone screening took place. In this screening, it was assessed if individuals met all the requirements to participate in the study. Participants were then invited to the actual study session, which took place in a quiet study room at the [blinded for review]. The sessions started with a diagnostic interview and by arranging written informed consent. Next, for research ethic reasons, a short distress screening was implemented to make sure that individuals were not under acute stress and ready to proceed to the symptom induction. For screening, participants were asked to complete a first symptom measurement, including the Impact of Event Scale-Revised (IES-R; Maercker & Schützwohl, 1998). No individuals with more than 80 sum points were allowed to proceed with the study; however, none of the participants exceeded this cutoff and had to be excluded. Subsequently, the symptom induction was implemented, which took around 15 minutes to complete. After this process, pre-VST intrusive symptoms were assessed, followed by the VST reaction time test for approximately 25 minutes. Next, a post-VST intrusion measurement took place. The study ended with debriefing and compensation of participants. All individuals received either [blinded for review] or one test subject hour if they were students. All study procedures were approved by the [blinded for review] (approval number 20.4.8).
Data analysis
For the statistical analysis, R Statistical Software (v4.1.3; R Core Team, 2022) and RStudio Version 1.4.1717 were used. Analysis of the error rates of the decision tasks led to exclusion of one participant (error rate exceeding 20%). Average reaction times of the VST were calculated in milliseconds for each participant and condition. A mixed ANOVA was performed on the VST data to investigate differences in reaction times using the rstatix package (v0.7.1; Kassambara, 2022). In addition, linear regression analyses were calculated by using the stats package (v3.6.2; R Core Team, 2022) to examine if intrusive symptoms were positively associated with reaction times for stress-related stimuli in the three study groups in the interference condition. For this purpose, pre- and post-VST intrusive symptom measurements were averaged to regress the mid-term intrusion score while performing the VST on stress-related reaction times. To investigate demographic differences between the three study groups, Chi-square tests for gender and an ANOVA for age were calculated. Unless otherwise indicated, an alpha-level of .05 was used for all statistical calculations.
Results
Sample and trial characteristics
Detailed sample characteristics are summarized in Table 1. Chi-square test revealed no significant group differences with regard to gender (p < .05). Additionally, ANOVA results did not show any significant age differences between the groups (F (1, 88) = 2.337, ηp2 = .026, p > .05).
Spearman–Brown corrected split-half reliabilities.

Note. r SB = Spearman-Brown corrected split-half reliability. 95% CI = confidence interval. Split-half reliabilities were estimated by 5000 random splits.
Attentional interference
Pairwise comparisons of stimulus conditions.
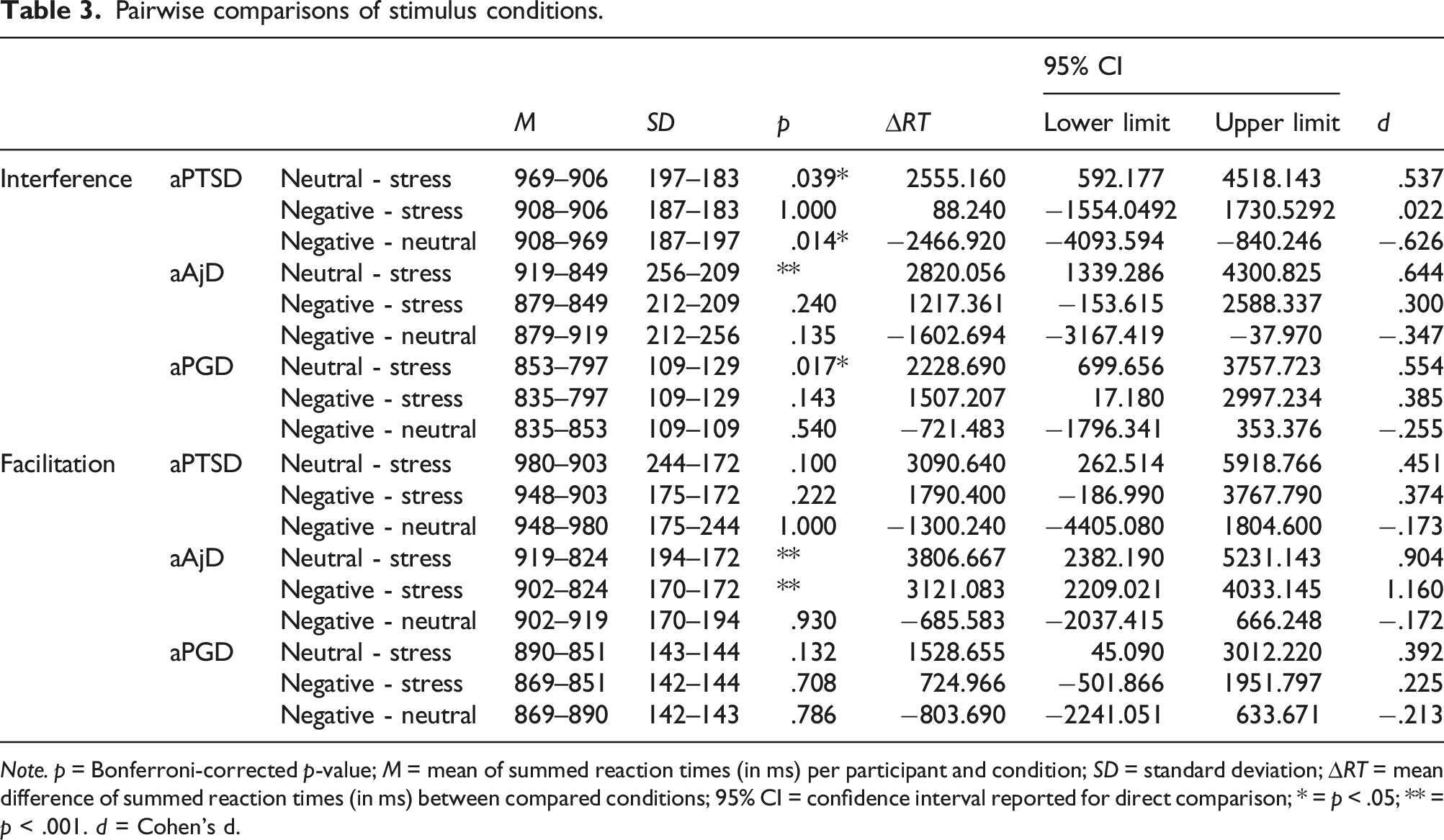
Note. p = Bonferroni-corrected p-value; M = mean of summed reaction times (in ms) per participant and condition; SD = standard deviation; ∆RT = mean difference of summed reaction times (in ms) between compared conditions; 95% CI = confidence interval reported for direct comparison; * = p < .05; ** = p < .001. d = Cohen’s d.

Interference bias results.
Regression analyses were performed to investigate the relationship between intrusive symptom scores and stress-related reaction times in the interference condition. For aPTSD, the mean mid-term intrusion score was M = 2.21 (SD = .68), while for aAjD it was M = 2.30 (SD = .65) and M = 2.67 (SD = .73) for aPGD. Regression analyses between mean intrusion score and stress-related reaction times revealed no significant relation in any of the three groups (aPTSD: F (1, 23) = .524, p > .5; aAjD: F (1, 34) = 2.726, p > .5; aPGD: F (1, 27) = .148, p > .5).
Attentional facilitation
A 3 word type X 3 group X 2 order mixed-design ANOVA was conducted on the latency data with two between-subject variables, group (aPTSD, aAjD, and aPGD) and order (interference first and facilitation first), and one within-subject variable, word type (stress-related, neutral, and negative). All significance levels reported below for analyses including word type reflect the Greenhouse–Geisser correction for sphericity. However, to minimize confusion arising from different degrees of freedom for similar analyses, unadjusted degrees of freedoms are reported.
A significant main effect of word type was found (F (2, 168) = 18.207, η
p
2
= .178, p < .01). For aPTSD, averaged reaction times to stress-related words, to neutral words (p > .05), and to negative words (p > .05) did not differ significantly from one another. For aAjD, individuals exhibited significantly faster reaction times to stress-related words than neutral words (p < .05) as well as compared to negative words (p < .05). For aPGD, no significant difference in mean reaction times of stress-related words and neutral words (p > .05) and stress-related words and negative words (p > .05) was found. Reaction times of the facilitation condition are displayed in Figure 2. Facilitation bias results.
Furthermore, no main effect of test order (F (1, 84) = .026, η p 2 = .000, p > .05) or group (F (2, 84) = 1.782, η p 2 = .041, p > .05) was found. Interaction effects of word type x group (F (4, 168) = 1.532, η p 2 = .035, p > .05), word type x test order (F (2, 168) = 2.556, η p 2 = .030, p > .05), and word type x group x test order (F (4, 168) = 1.608, ηp2 = .037, p > .05) did not show any significant results.
Discussion
The aim of this study was to assess attentional biases in individuals who have experienced a stressful life event. The study examined whether participants in the groups aPTSD, aAjD, and aPGD are characterized by attentional interference and facilitation biases. Contrary to the hypothesis, results showed that in the interference condition, individuals in all three study groups reacted significantly faster in trials which included stress-related words than trials with neutral words, which indicates a reversed interference bias. Furthermore, contrary to the hypothesis, the aAjD group showed significantly faster reaction times when a stress-related stimulus was the target word in an array of neutral words, indicating a facilitation bias. Again not in line with the formulated hypothesis are results of regression analysis which showed that stress-related words in the interference condition are not associated with intrusive symptoms.
To our knowledge, this is the first study that shows a reversed attentional interference bias in stress-related conditions. However, reversed cognitive processing patterns have been found for other psychological mechanisms, such as priming (e.g., Sand, 2016). With regard to attentional biases, previous studies have demonstrated, for example, regular interference biases in PTSD (Pineles et al., 2009) or facilitation biases in anxiety-related disorders (Öhman et al., 2001). The rationale of the reversed attentional interference bias remains ambiguous. Regression analysis revealed that stress-related interference reaction times are not related to intrusive symptoms. These results are plausible in light of previous studies that have shown that intrusive symptoms may be associated with a regular, but not reversed attentional interference bias (Pineles et al., 2009). The findings of the current study therefore imply that the attentional interference data is associated with a phenomenon or mechanism other than intrusions.
A reversed interference bias could potentially emerge from avoidance. Participants might have reacted particularly quickly to trials which included stress-related reminders in order to move on to other, less distressing stimuli of the VST, showing avoidance toward the stress-related trials. Avoidance has been frequently linked to attentional biases (e.g., Bardeen et al., 2020; Cisler et al., 2009; Lavy & van den Hout, 1994; Koster et al., 2006) and is therefore suitable for the explanation of the present results. Moreover, a reversed attentional interference could have been caused by a particularly high arousal of participants during the VST. As a confrontation with stress-related stimuli can create acute stress, participants may have been especially aroused and put in an alerted state of mind during the task which in turn accelerated participants’ reaction times (Wisco et al., 2013). More research is needed to better understand the underlying mechanism of (reversed) attentional interference bias.
A study of Bardeen et al. (2020) that investigated individuals with PTSD found that an interference bias mainly occurs if a low attentional control behavior of participants (e.g., low strategic control of higher order executive functions) was observed. In turn, high attentional control caused a pattern of “overcontrol,” resulting in an avoidance behavior. Conclusively, if the reversed interference bias would be associated with avoidance, then this behavior might resulted from a high attentional control of participants. Moreover, it is possible that a high attentional control was significantly triggered by the symptom induction task because high distress during the induction may have caused an increased urge for attentional control in the subsequent experimental tasks. Symptom induction procedures are particularly strong when they are individually tailored (De Putter et al., 2017), as it was implemented in the current study. Therefore, the symptom induction could be responsible for the surprising findings of the attentional bias test.
The present study demonstrated similar attentional bias results between the different stress-related groups. This finding is in line with previous research showing similar attentional mechanisms in PTSD (Lazarov et al., 2019) and grief (Schneck et al., 2018). A study by Schneck et al. (2018) also found a connection between attentional mechanisms and neurocognitive patterns in bereaved individuals. As PTSD is also related to neurocognitive alterations (e.g., Kunimatsu et al., 2020), it is possible that the similar findings on attentional biases across the stress-related groups are connected to neurophysiological changes related to stress.
There were only very few effects concerning generally negative stimuli that were not stress-related. For instance, in the interference condition, individuals in aPTSD reacted significantly faster in trials which included generally negative words and stress-related words than trials with neutral words. This indicates that individuals in the aPTSD group were generally affected by words with negative valence, including both generally negative and stress-related words. This specific finding is plausible as research shows that after experiencing a traumatic event, affected individuals are sensitive to all sort of negative reminders or triggers (Jovanovic et al., 2009). Furthermore, in the facilitation condition, participants in the aAjD group reacted significantly faster to stress-related words than negative words. This finding indicates that individuals in the aAjD group were only affected if they are confronted with direct reminders of a stressor and not by all stimuli with negative valence.
The present study has several limitations. First of all, no full diagnostic interview for various mental disorders was conducted. As attentional biases are associated with many different disorders, some individuals might have suffered from a disorder that is not directly stress-related but still had a relevant confounding impact on the attentional bias measure. Even though the interview and symptom induction process of the present study was directly related to the stressor of participants and therefore specifically targeted stress-related reactions, it is possible that many different psychological mechanisms were involved that influenced attention bias assessment. Furthermore, no healthy control group was involved in this study. Even though a control condition was implemented in the VST in the form of neutral words, as it is common for this type of reaction time test (e.g., Pineles et al., 2007, 2009), a comparison to individuals who did not experience a stressful life event could have provided more elaborate insights into the current findings. Moreover, the present study featured an analogue stressor with possibly limited transfer to a full-blown PTSD, AjD, and PGD. In addition, the current study did not implement a manipulation check for the symptom provocation task or a stress measurement of the VST. These limitations might have a significant impact on the conclusions of the study. Nevertheless, the reported results add up to the comprehension of underlying mechanisms of all disorders associated with an aversive life event. One of the main strengths of this study is the linking of stress-related disorders and symptoms to specific cognitive phenomena, which places mental disorders in a broader, trans-disciplinary context. As psychopathological conditions are often rooted in cognitive processes (e.g., Eberle & Maercker, 2022), the present study fosters a more comprehensive approach to psychological research questions.
The reversed interference bias found in all disorder-related groups needs to be further investigated in the future. The present findings raise the possibility that this particular bias may represent a mechanism that is associated with stress-related disorders. Even though several explanatory approaches have been laid out to interpret this phenomenon, the rationale of a reversed interference bias remains vague and should be studied in depth by conducting more empirical research. Eye-tracking methods could be particularly promising here, as they proved to be a reliable alternative to reaction time tests (Lazarov et al., 2019). In addition, the present results show that the consequences of a critical life event are prominently manifested on a cognitive level. Hence, cognitive therapy probably holds great potential for treatment of all stress-related disorders. For instance, it is probable that cognitive bias modification that applies reappraisal change principles could alter such attentional biases not only in PTSD but also in AjD and PGD. Consistent with existing literature in the field (e.g., Lazarov et al., 2019), in psychotherapy of stress-related conditions, a particular emphasis should be placed on the treatment of sustained and interfered attention processes. As the current study showed similar results between the different groups, transdiagnostic psychotherapy protocols should be considered more often in the future.
Conclusions
The current findings show that all three disorder-related study groups are characterized by the same kind of attention bias, a reversed attentional interference bias. This bias has never been previously reported in the literature and is perhaps related to avoidance. The present study supports the idea that PTSD, AjD, and PGD share a common psychopathological mechanism and thus have a transdiagnostic nature. Future studies should further investigate cognitive phenomena in general and attentional biases in particular in relation to trauma and stress. New insights in this area could not only enhance our psychopathological understanding of this specific group of disorders but also improve psychotherapy for individuals affected by a stressful life event.
Footnotes
Acknowledgments
The authors wish to thank Dr Marcella Woud and Dr Charlotte Wittekind for their valuable advices and for providing the Inquisit scripts.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.