
Abstract
The objective of this study is to test the dysregulation of goal/activity identification hypothesis and the role of psychological flexibility within it. A nonclinical sample of 247 adults completed the Personalized Psychological Flexibility Index (PPFI) and DASS-21. Participants' goal on the PPFI were categorized into abstract or concrete. The moderating effect of psychological flexibility on the relationship between goal abstraction and stress, depression and anxiety were examined. These relationships were explored using specific dimensions of psychological flexibility: harnessing, avoidance and acceptance. A significant interaction was found between psychological flexibility and goal abstraction on stress. Individuals who stipulated an abstract goal and had lower levels of psychological flexibility had significantly higher levels of stress. This relationship was not evident for concrete goals. These findings did not emerge when examining specific dimensions of psychological flexibility suggesting that multiple facets of psychological flexibility contribute to these findings. Harnessing was, however, unique. Individuals with a concrete goal and higher levels of harnessing had significantly higher stress. This study provides preliminary findings regarding the influence of psychological flexibility within the dysregulation of goal/action identification hypothesis. Future research, particularly in clinical samples is needed to confirm these associations and their combined role as a transdiagnostic process.
Introduction
The dysregulation of goal/action identification hypothesis has been identified as a possible transdiagnostic process underpinning psychopathology (Watkins, 2011). This hypothesis proposes that dysregulation, or an inability to shift between abstract and concrete levels of goal/action identification, contributes to a range of psychological disorders (Watkins, 2008, 2011; Watkins & Roberts, 2020). An abstract level of identification involves general, superordinate and decontextualized mental representations which convey the essential meaning of goals, events and actions; it denotes the ‘why’ aspect of an action including the ends that are consequential to it (Fujita & MacGregor, 2012a, 2012b). In contrast, a more concrete level of identification involves contextual, subordinate and specific details of goals, events and actions which denote the mechanics and means of ‘how’ to do the action (Cooper, 2013). The dysregulation of goal/action identification hypothesis is grounded in Control Theory (Powers, 1973) and Action Identification Theory (AIT) (Vallacher & Wegner, 1987). Control theory postulates that goals, events and behaviours are hierarchically organized and are processed at different levels of abstraction; abstract goals inform more concrete goals and standards (Broadbent, 1977; Carver & Scheier, 1982, 1990, 1998; Powers, 1973). Similarly, within Action Identification Theory (AIT; Vallacher & Wegner, 1987), an abstract identification denotes the purpose and ends of an action (‘why it is carried out’), whereas a concrete identification represents the process and means of the action (‘how it is carried out’). Thus, within AIT, the same action (e.g. ‘giving my partner a hug’) can be identified in abstract terms (e.g. ‘showing sympathy’) or in more concrete terms (e.g. ‘lifting my arms up’).
The dysregulation of goal/action identification hypothesis suggests the level of abstraction used to represent goals, behaviours and events plays a role in the onset and maintenance of psychopathology. Hawkins (2011) argues this hypothesis is based on three lines of evidence. First, different levels of goal/action identification are related to cognitive, emotional and behavioural symptoms of psychological disorders and/or the processes implicated within them. For example, there is consistent evidence that when faced with a stressor, adopting a concrete level of goal/action identification results in less negative affect and/or less reduction in positive affect than adopting an abstract level of goal identification (e.g. Houser-Marko & Sheldon, 2008; Moberly & Watkins, 2006; Watkins et al., 2008). The negative consequences of repetitive thought (i.e. rumination and worry) are characterised by an abstract level of goal/action identification processing with a focus on meaning and implications and asking ‘why?’ (Rimes & Watkins, 2005; Watkins, 2008; Watkins & Moulds, 2007). Recently, Watkins and Roberts (2020) presented the H-ES-A-FO-N model that proposed that abstract processing is a critical process that accounts for the onset and maintenance of rumination. Additionally, the level of goal/action identification is implicated as part of the influence that problem-solving, planning, impulsivity and self-regulation has on psychological symptoms (Vallacher & Wegner, 1987; Fujita & Han, 2009; Watkins & Moulds, 2005). Second, the optimal level of goal/action identification has been found to shift in response to context, suggesting that the level of goal/action identification is adaptive in individuals without a psychological disorder (Vallacher & Wegner, 1987; Forgas & East, 2008; Hetherington & Moulds, 2015; Flink et al., 2018; Bornstein et al., 2021). For example, the level of goal/action identification shifts with mood; happy mood is associated with a more abstract level of goal/action identification, whereas sad mood is associated with a more local concrete level of goal/action identification (e.g. Forgas & East, 2008; Storbeck & Clore, 2005; Seebauer et al., 2016; Hetherington & Moulds, 2013). Thus, based on this line of evidence, Watkins (2011) concludes that impaired regulation of the level of goal/action identification may be evident in psychological disorders. In support of this, third and finally, there is evidence that the level of goal/action identification is biased in certain psychological disorders, with evidence of an elevated tendency to adopt more abstract levels of goal/action identification for negative outcomes and events in depression, anxiety disorders, PTSD, psychotic experiences (Maurage et al., 2017; Samtani et al., 2018; Schaich et al., 2013; Stavropoulos & Berle, 2020; Van Lier et al., 2015; White & Wild, 2016) and evidence that addictions and binge eating involve an elevated tendency for concrete levels of goal/action identification (Grynberg et al., 2016; Kadriu et al., 2019). Although there is evidence that psychopathology may also increase mental abstraction and thus contribute to more abstract goal representations (Felt, 2018; Felt et al., 2021). Thus, it is likely that a bidirectional relationship exists between these constructs.
The goal/action identification hypothesis (Watkins, 2011) emphasizes the significance of flexibility to ensure adaptivity in the level of abstraction of goals and actions to match circumstances. Dysregulation, or inflexibility in the level of abstraction, is consequently the core feature underpinning the transdiagnostic feature of this process in psychopathology (Watkins, 2011). Accordingly, it would be proposed that if an individual has lower levels of flexibility, the resources or adaptability to pursue this goal would be more limited, thus making the individual more vulnerable to psychological distress. This is also consistent with a recent conceptualization of transdiagnostic processes (Cherry et al., 2021; Faustino, 2021; Morris & Mansell, 2018). In a recent systematic review, Morris and Mansell (2018) examined the relationship between rigidity/flexibility and a range of transdiagnostic processes (i.e. rumination, perfectionism, impulsivity and compulsivity). Most studies included found that transdiagnostic cognitive and behavioural processes and inflexibility were correlated, co-occurring or predictive of each other. Consequently, it was concluded that transdiagnostic processes are not inherently maladaptive. It is individual differences in the inflexible implementation of these processes that determine the degree to which they impact mental health.
Psychological flexibility has been proposed as being a core psychological construct that supports the pursuit of goal attainment when it aligns with an individual’s values (Bond et al., 2006; Doorley et al., 2020; Kashdan & Rottenberg, 2010). Hayes et al., (2004) originally defined psychological flexibility as ‘the ability to change or persist with functional behavioural classes when doing so serves valued ends’ (Hayes et al., 2004, p. 15). Psychological flexibility has been found to be associated with several well-being indices including positive responses to stressful life situations, quality of life, resilience and adaptive coping strategies (Densham et al., 2016; Kashdan & Rottenberg, 2010; Omreore & Nwanzu, 2022; Silberstein et al., 2012; Wąsowicz et al., 2021). Psychological flexibility involves adapting to changing situational demands, allocating mental resources, shifting perspective and finding balance between competing demands to facilitate the pursuit of personal goals or values (Cherry et al., 2021; Kashdan & Rottenberg, 2010). Thus, there appear to be conceptual similarities between psychological flexibility and the dysregulation of goal/action identification hypothesis. First, both constructs involve personal goals and aim to support goal attainment. Second, dysregulation, or an inability to shift between abstract and concrete levels of goal/action is likely to be hindered by an inability to allocate mental resources, change situational demands and shift perspective, core tenets of psychological flexibility. Third and finally, the dysregulation of goal/action identification hypothesis and psychological flexibility both contribute to psychological well-being. Thus, psychological flexibility may be a particularly pertinent psychological process within the dysregulation of goal/action identification hypothesis.
Recently, Kashdan et al. (2020) derived the Personalized Psychological Flexibility Index (PPFI), a self-report measure of psychological flexibility. In this measure, psychological flexibility is explicitly linked to a personally relevant goal that an individual is currently pursuing. The PPFI captures three dimensions of psychological flexibility; avoidance or an inflexible/rigid response to discomfort, that is, escaping particular feelings, thoughts, and situations because of discomfort, or delaying goal pursuit altogether; acceptance or a flexible or more open response to discomfort, that is, being aware of and receptive to the natural discomfort that arises during goal pursuit; and harnessing or being able to flexibly respond to discomfort to motivate and facilitate valued goal pursuit. Kashdan et al. (2020) examined the association between psychological flexibility as measured by the PPFI and meaningful real-life outcomes. The objective here was to test the prediction that psychological flexibility predicts goal-related activity and responses to potential barriers to these. Specifically, using a community sample of adults (N= 508), a multimethod study was conducted with a comprehensive assessment of a single day, a broader assessment of the personal striving that an individual is focused on, as well as a semi-structured interview of stressful life events and reactions to them. Consistent with predictions, individuals with higher psychological flexibility made more progress towards value-consistent goals; and this progress occurred irrespective of the severity of psychological distress experienced. Interestingly, relative to other PPFI subscales, only harnessing was associated with pursuing more difficult daily goals, greater effort expended, and greater extraction of meaning in life from daily goals. Harnessing also predicted what people were striving for across days and weeks, and was thus not only relevant to a single-day experience. Kashdan et al., (2020) consequently concluded that harnessing may play a pivotal role in the pursuit of meaningful goals, even when doing so is difficult. These findings are consistent with a body of evidence that harnessing or upregulating a negative emotion can be a healthy psychological strategy to support the pursuit of valued goals (Bylsma et al., 2008; Kashdan & Rottenberg, 2010; Tamir & Ford, 2009).
Currently, the PPFI has been concluded as being the most accurate measure of psychological flexibility available both from a psychometric and conceptual standpoint (for review see Cherry et al., 2021). It also provides a unique opportunity to explicitly test the role of psychological flexibility within the dysregulation of goal/action identification hypothesis (Watkins, 2011). The relevant goal that an individual stipulates on the PPFI will have varying degrees of abstraction from abstract (i.e ‘to be present’) through to concrete (i.e. ‘to wake up earlier and incorporate 30 minutes of exercise 5 times a week’). Further, an individual’s psychological flexibility in regard to the level of goal abstraction can be quantified and examined in relation to their mental health. This is the overall objective of this study. According to the dysregulation of goal/abstract identification hypothesis (Watkins, 2011), it is predicted that dysregulation, or an inability to shift between abstract and concrete levels of goal/action identification, contributes to psychopathology. It is proposed that psychological flexibility, which manifests as higher levels of avoidance, and lower levels of acceptance and harnessing, contributes to this dysregulation. Furthermore, adopting an abstract level of goal/action identification is associated with a range of cognitive, affective and behavioural symptoms and psychological disorders. Thus, it is hypothesised that individuals who have lower levels of psychological flexibility in relation to an abstract goal will have higher levels of mental distress (i.e. more depression, anxiety and stress symptoms). That is, individuals who have less psychological flexibility in the pursuit of an abstract goal, are more likely to get stuck in a specific behavioural response and have fewer resources to change this response if this is not adaptive towards goal attainment; this will consequently have a detrimental impact on the individual’s mental health. It is predicted that these relationships will not exist for individuals who provide a more concrete goal. To test this hypothesis, moderation analysis will be adopted to examine the moderating effect of psychological flexibility on the relationship between goal abstraction (i.e. abstract vs. concrete) and mental health outcomes. Additionally, in accordance with the findings of Kashdan et al. (2020), we will also explore if specific dimensions of psychological flexibility (i.e. avoidance, acceptance and harnessing) influence the relationship between goal abstraction and mental health.
Method
Sample
Participants were recruited from a nonclinical adult population via community advertisement and social media advertisements on social media platforms (i.e. Facebook, Twitter and Reddit). Inclusion criteria were adults aged 18 years or older and native-English speakers. This study formed part of a larger project to ascertain healthy control data to explore psychological flexibility in individuals with traumatic brain injury; thus, individuals were excluded from participating if they had a history of traumatic brain injury or neurological condition. Participants provided written informed consent and then completed the study measures remotely using an online platform (Qualtrics (Qualtrics, Provo, UT)). Ethical approval was granted by the Victoria University Human Ethics Committee (30287).
Measures
Psychological Flexibility
The Personalized Psychological Flexibility Index (PPFI; Kashdan et al., 2020) is a goal-specific self-report measure of psychological flexibility. Participants are asked to respond to the items based on ‘an important goal that you are working on’. The PPFI consists of 15 items on a seven-point Likert scale (1 = strongly disagree to 7 = strongly agree). Higher scores on this measure indicate higher psychological flexibility. It consists of three subscales avoidance, acceptance and harnessing. A total score is produced by combining scores from the three subscales, with the Avoidance subscale reverse scored (i.e. higher scores indicate less avoidance). Kashdan et al. (2020) provided initial evidence regarding the psychometric adequacy and validity of the PPFI across a range of samples (college students, general adult populations in the community and working professionals). In accordance with its theoretical conceptualisation, the PPFI was found to be associated with healthy emotional expressions of personality (e.g. conscientiousness and openness to experience), healthy emotional experiences and regulatory strategies, well-being and low levels of emotional disturbances. Importantly, using factor analysis, the PPFI could also be differentiated from measures of negative emotionality, a shortcoming of existing measures (i.e. AAQ-II and BEAQ) of psychological flexibility (e.g. Wolgast, 2014; Tyndall et al., 2019). In addition, the reliability (Cronbach’s alphas = 0.77–0.84), test-retest reliability, incremental validity and construct validity, have been deemed acceptable (Kashdan et al., 2020).
Goal Abstraction
Goal abstraction categorisation criterion and examples.

Psychological Distress
The Depression, Anxiety and Stress Scale-21 (DASS-21; Lovibond & Lovibond, 1995) is a 21-item self-report with three subscales that measure depression, anxiety, and stress over the previous week. It consists of a 4-point Likert scale with 0 = never, 1 = sometimes, 2 = often, and 3 = always. Higher scores are indicative of elevated levels of depression, anxiety and stress. The DASS-21 has good psychometric properties (Cronbach’s alpha = 0.73–0.81; Lovibond & Lovibond, 1995) and the internal consistency of each factor was very good (Cronbach’s alpha = 0.82–0.90, Antony et al., 1998).
Data Analysis
Data were analysed using SPSS version 28. As the study occurred online, there was no missing data in the dataset. Cooks distance (Cook’s D) was applied to the dataset and no outliers were identified. Descriptive statistics were used to characterise psychological flexibility and mental health outcomes by goal characterisation type. To test the moderating role of psychological flexibility on the relationship between goal abstraction and mental health outcomes, regression-based moderation analysis was performed with Process Model 1 (Hayes, 2018). Continuous predictors that were built into the interaction term (i.e. psychological flexibility) were mean-centred. Three models were computed for each mental health outcome: depression, stress and anxiety. The conditional effects (simple slopes) of goal abstraction, psychological flexibility and the interaction term (goal abstraction x psychological flexibility) on each of the mental health outcomes were estimated. A 95% bootstrap was plotted using the data generated by PROCESS to visualise significant moderating=75/aza g effects. Given that there are no theoretical cut-off points for the moderator (psychological flexibility), goal abstraction was plotted at the following psychological flexibility cut-off point values: one standard deviation below the mean, the mean, and one standard deviation above the mean. The significance of the effects was tested using the bootstrap method (with 5000 samples). Finally, models in which psychological flexibility emerged as a significant interaction were further examined using the three dimensions of psychological flexibility (acceptance, avoidance, and harnessing). Given the primary hypothesis regarding the moderating effect of psychological flexibility was tested across three mental health outcomes, more stringent significance levels of p < .01 and 99% confidence intervals were used to control for Type 1 error. The subsequent moderation analyses conducted on the dimensions of psychological flexibility were exploratory in nature, and thus the more conventional significance levels of p < .05 and 95% confidence intervals were retained.
Results
Demographic characteristics of participants by goal categorisation.

Descriptive statistics by goal abstraction.

Moderation analysis for psychological flexibility, goal abstraction and mental health outcomes.

*p < .05, **p < .01.
To further figure out the essence of the interaction effects, simple slope analyses was conducted. As illustrated in Figure 1, among individuals with an abstract goal, psychological flexibility significantly predicted stress symptoms (b = -0.09, p = .002). That is, participants who had low levels of psychological flexibility and an abstract goal had significantly higher stress symptoms, whereas participants with an abstract goal and higher levels of psychological flexibility had significantly lower stress symptoms. In contrast, among participants with a concrete goal, psychological flexibility did not predict stress symptoms (b = 0.02, p = .526). Similarly, as shown in Figure 2, among individuals with an abstract goal, psychological flexibility significantly predicted depressive symptoms (b = -0.16, p < .0001). That is, participants who had low levels of psychological flexibility and an abstract goal had significantly higher depressive symptoms, whereas participants with an abstract goal who had higher levels of psychological flexibility had significantly lower depressive symptoms. In contrast, among individuals with a concrete goal, psychological flexibility did not predict depressive symptoms (b = -0.04, p = .317). The interaction effect between psychological flexibility and goal categorisation on stress symptoms. The interaction effect between psychological flexibility and goal categorisation on depression symptoms.

Finally, in the models where psychological flexibility emerged as having a significant interaction with goal abstraction, the specific dimensions of psychological flexibility were examined (see Table 4). In regards to depression, only harnessing emerged as having a significant interaction with goal abstraction (b = −0.21, SE = 0.11, t = −1.99, p = .048). Simple slope analyses found that for individuals with abstract goals, harnessing’s ability to predict depressive symptoms was approaching significance (b = −0.15, p = .055). As shown in Figure 3, individuals with an abstract goal and lower levels of harnessing were more likely to have higher levels of depressive symptoms. For individuals with concrete goals, harnessing did not predict depressive symptoms (b = 0.06, p = .388). The interaction effect between harnessing and goal categorisation on depression symptoms.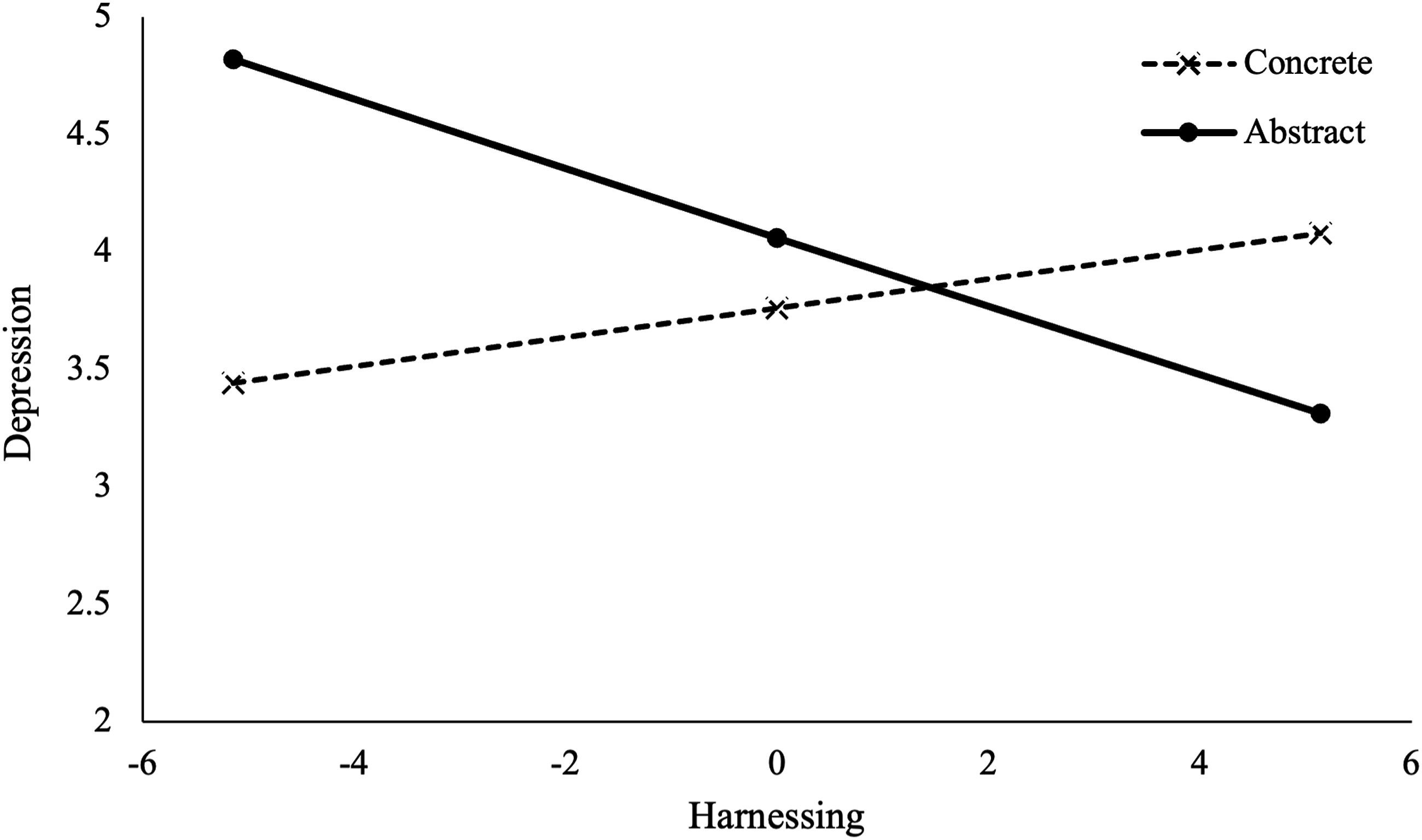
In regards to stress, similarly, only harnessing emerged as having a significant interaction with goal abstraction (b = −0.18, SE = 0.09, t = −2.00, p = .047) However, in this analysis, simple slope analyses found that for individuals with concrete goals, harnessing significantly predicted stress symptoms (b = 0.16, p = .012). As shown in Figure 4, individuals who had higher levels of harnessing and a concrete goal had significantly higher stress symptoms, whereas participants with a concrete goal and lower levels of harnessing flexibility had significantly lower stress symptoms. Harnessing did not predict stress symptoms for individuals with an abstract goal (b = −0.02, p = .747). (Table 5) The interaction effect between harnessing and goal categorisation on stress symptoms. Moderation Analysis for components of psychological flexibility, goal abstraction, stress and depression.

Discussion
The objective of this study was to test the dysregulation of goal/action identification hypothesis (Watkins, 2011) in a non-clinical adult sample and the role of psychological flexibility within it. In partial support of our hypothesis, we found a significant interaction between psychological flexibility and goal abstraction on stress symptoms. More specifically, individuals who stipulated a more abstract goal on the PPFI and had lower levels of psychological flexibility, had significantly elevated levels of stress symptoms, whereas individuals who had higher levels of psychological flexibility had significantly lower stress symptoms. This finding was not evident in individuals who stipulated a more concrete goal. This is consistent with the dysregulation of goal/action identification hypothesis (Watkins, 2011) which not only predicts that a more abstract level of goal, action or behaviour identification is associated with psychological symptoms and psychopathology, but it is the dysregulation or, an inability to shift between abstract and concrete levels of goal/action identification, that contributes to psychopathology (Watkins, 2008, 2011; Watkins & Roberts, 2020). Watkins (2011) argues that the level of goal/identification is functionally regulated and shifts adaptatively in response to context (Vallacher & Wegner, 1987) and mood state (Forgas & East, 2008; Hetherington & Moulds, 2013). Thus, an inability to ‘shift adaptivity’, when pursuing an abstract goal, due to lower levels of psychological flexibility, may consequently impact this process and possibly contribute to increased stress.
This finding provides some support for the proposal that it is the inflexible implementation of transdiagnostic processes that contributes to the development and maintenance of psychological symptoms and psychology (Cherry et al., 2021; Faustino, 2021; Morris & Mansell, 2018). Consistent with the goal/abstract and identification hypothesis, Morris & Mansell (2018) highlight that transdiagnostic processes are not inherently maladaptive and there is increasing evidence that such processes relate to psychological distress when applied in a rigid or inflexible manner. This is consistent with our findings. Although it has been proposed that an abstract level of identification is associated with a range of psychological symptoms and psychological disorders, we found that its impact on stress symptoms was only evident in individuals with low levels of psychological flexibility. Said another way, if an individual is currently pursuing an abstract goal, which has the potential to impact mental well-being, if they have higher levels of psychological flexibility, they are more likely to have the resources to shift their responses, mitigating its detrimental impact. According to the dysregulation of goal/abstraction identification hypothesis (Watkins, 2011), and consistent with Control Theory (Powers, 1973) and AIT (Vallacher & Wegner, 1987), it would be argued that this ‘shift’ supports moving towards a more concrete level of thinking and behaving which results in goal progress.
The dysregulation of goal/action identification hypothesis (Watkins, 2011) is proposed to be a transdiagnostic process contributing to a range of psychological symptoms and psychopathology. However, in this study, we found that psychological flexibility did not moderate the relationship between goal abstraction and anxiety and depressive symptoms. This finding was not expected and is inconsistent with findings that abstract goal identification is associated with anxiety and depressive symptoms, that is, worry and a range of anxiety disorders such as GAD, Social Anxiety (Maurage et al., 2017; Stavropoulos & Berle, 2020; Van Lier et al., 2015; White & Wild, 2016). Although the results of this study do not initially support this hypothesis, these conclusions may be limited based on the methodology of our study and future research is needed to test this hypothesis. Specifically, we adopted a more stringent significance level to control for possible type 1 errors because multiple statistical analyses were conducted. As a result, the interaction between goal abstraction and psychological flexibility on depression was deemed not significant (p = .019). Additionally, the significance value for the interaction between goal abstraction and psychological flexibility on anxiety was slightly over the more lenient cut-off of .05 (p = .055). Furthermore, we used a very broad self-report screening tool of psychological distress. For example, in regard to anxiety, questions focus on physiological symptoms (i.e. hard to wind down, dryness in the mouth and increased breathing), and there is only one question about cognitive symptoms. Future studies would benefit from examining these relationships using a more comprehensive assessment of anxiety and depression. Finally, our participants were a heterogenous non-clinical sample recruited from various community sources and as a result, the variability in psychological distress and psychological flexibility will be more restricted than in clinical populations, that is, those with a formal diagnosis of an anxiety disorder. Thus, currently, it is not possible to determine whether our findings are statistical artifacts, are reliable or limited based on the measures and the sample used. Further examination of the goal/action identification hypothesis as a transdiagnostic process is therefore needed.
In this study, we also explored how the dimensions of psychological flexibility, acceptance, avoidance and harnessing, may influence the relationship between goal abstraction and mental health outcomes; we did this for both stress and depression. Interestingly, we found that no specific dimension of psychological flexibility could explain the interaction between psychological flexibility and abstract goals and its influence on stress symptoms. This suggests that multiple facets of psychological flexibility (i.e. avoidance and acceptance) may contribute to these findings. We did however find that harnessing or using discomfort to motivate and facilitate valued goal pursuit, was unique. Specifically, we found that harnessing significantly interacted with concrete goals and significantly predicted stress. That is, individuals who had a concrete goal and higher levels of harnessing were also significantly more likely to have higher levels of stress.
Currently, it is difficult to tease out the directionality of our findings. There is evidence that low affect is associated with a more abstract identification of goals and actions (Maurage et al., 2017; Samtani et al., 2018; Schaich et al., 2013). However, it is difficult to infer if it is low affect that drives a more abstract identification or vice versa, or if a bi-directional relationship exists. Irrespective of directionality, our study presents novel findings regarding the impact of psychological flexibility, and more specifically the dimensions within this construct, on these relationships. These findings may have important clinical implications. Exploring a goal, that an individual is currently pursuing, whilst also assessing their psychological flexibility, could reveal a psychological process contributing to and maintaining an individual’s psychological distress. This could then be addressed using evidence-based psychological therapies to increase psychological flexibility, value-based action, and harnessing, that is, Acceptance and Commitment Therapy (Hayes et al., 1999) as well as supporting clients to increase their concrete identification of goals and actions, that is, using SMART goal framework (Locke & Latham, 2002; Weintraub et al., 2021).
There are limitations that need to be considered when interpreting the results of this study. First, it must be noted, that this study was conducted in the non-clinical sample which will have lower levels of psychological distress. This is likely to have implications on the study and possibility account for the low amount of variance accounted for in our findings. In this study, we had no measure of closeness or progress towards the stipulated goal on the PPFI. That is, we cannot infer if psychological flexibility is actually supporting this process, and at present, we only know that a relationship exists between goal abstraction and negative affect. Future studies would benefit from a longitudinal design where progress towards the goal stipulated can be explicitly assessed and its relationship with psychological flexibility, goal abstraction and well-being examined. The demographic characteristics of our sample are also likely influenced by the method of using an online survey for data collection. Our sample is skewed towards a more educated ethnic majority, and as such, the ability to generalise the findings to more diverse populations is limited. In summary, in accordance with the dysregulation of goal/action identification hypothesis, psychological flexibility may influence the impact that goal abstraction has on mental well-being. However, before any conclusions can be inferred regarding the combined role of these constructs as transdiagnostic processes, replication is needed, particularly in clinical samples, to confirm these associations.
Footnotes
Acknowledgements
We thank Matthew Lamb for this role in data collection, as well as all participants for kindly agreeing to participate in this research.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by a Health Research Council small project grant (20/588).