
Abstract
Shame and dissociation play pivotal roles in the pathogenesis and treatment of (complex) post-traumatic stress disorder. However, the causal relationship between these two symptoms remains unclear. We tested the association between state shame and state dissociation in 249 participants (Mage = 27.55; SDage = 8.74; 60.24% female; 84.7% no mental illness). After completing questionnaires (trait shame and dissociation, trauma history), participants were randomly allocated to an imaginative shame or dissociation induction group, and changes in state shame and dissociation were measured. The data were analyzed using latent change score modeling. We found significant changes in both state shame and dissociation, with an isolated change of state shame in the shame induction group but changes in both shame and dissociation in the dissociation induction group. Thus, state shame and dissociation correlated only with the induction of dissociation. We found an effect of trait variables only on state dissociation and no effect of trauma history on state variables. The interaction between shame and dissociation remains complex and is only partially understood. Our study adds to research supporting the assumption that dissociation leads to shame. In addition, in experimental psychopathology approaches, imaginative procedures seem more suitable for studying shame than for studying dissociative symptoms.
Keywords
Introduction
Although post-traumatic stress disorder (PTSD) has long been conceptualized as a fear-based disorder (Ehlers & Clark, 2000), research now provides ample support for a more complex concept of PTSD, with subtypes that differ in terms of triggering events, relevant emotions, neurobiological correlates, and best treatment options. Since the introduction of complex PTSD in the International Classification of Diseases (ICD-11; World Health Organization, 2019) and new PTSD criteria in the Diagnostic and Statistical Manual of Mental Disorders (DSM-5; American Psychiatric Association, 2013), the core role of shame and dissociative symptoms in development, maintenance, and treatment has been widely recognized. However, the precise relation between these two symptoms remains unclear. Although a recent meta-analysis found evidence of a correlation between the two constructs, only five studies with an experimental design were included (Rudy et al., 2022).
Shame and dissociation—theory and definitions
The feeling of shame is one of the most unpleasant emotions. In extreme manifestations, the neural regions and patterns involved while feeling ashamed are similar to those activated by physical pain (Bastin et al., 2016; Brockman, 2017; Kross et al., 2011; Lewis, 1971). Often, shame is conceptualized as feelings of inadequacy, violations of social norms, and (real or anticipated) social exclusion (Lewis, 1971; Lewis, 1992, 1998; Miceli & Castelfranchi, 2018). While shame is relevant to many psychiatric disorders (Scheel, Schneid et al., 2013), it may be central to the development of PTSD, especially after interpersonal trauma (Badour et al., 2018; Bomyea & Allard, 2017; Feiring et al., 2002; Feiring & Taska, 2005; Ford et al., 2006; Freed & D'Andrea, 2015; Kubany & Watson, 2003). However, the mechanism through which trauma triggers shame remains unclear.
There is some empirical evidence for the role of domination and subjugation in interpersonal traumatic events (Finkelhor & Browne, 1985; Herman, 2011; Kallstrom-Fuqua et al., 2004), moral injury (Jordan et al., 2017; Litz et al., 2009), self-blame mechanisms to protect the relationship with the offender (Goldsmith et al., 2012), and feelings of humiliation or loss of wholeness and integrity (Saraiya & López-Castro, 2016). It has been stated that addressing shame (Saraiya & López-Castro, 2016) and guilt (Pugh et al., 2015) may be central to recovery from PTSD. Fear of social exclusion may drive humans to avoid shame or quickly counteract the emotion (Dorahy, McKendry et al., 2017; Nathanson, 1994). Dissociation may serve as a (dysfunctional) emotion regulation mechanism creating emotional numbing, thereby lessening the perceived intensity of shame (Cavicchioli et al., 2021).
Controversial approaches exist for defining dissociation (Brown, 2006; Giesbrecht et al., 2008; Loewenstein, 2018; van der Hart, 2021). However, operationalized on a descriptive level (Dorahy, McKendry et al., 2017), symptoms and experiences include feelings of depersonalization, derealization, confusion about the self, and amnesia. Dissociative symptoms are associated with many psychiatric disorders, especially traumatic sequelae (Lyssenko et al., 2018; Van Ijzendoorn & Schuengel, 1996) and correlate with illness severity (La Mela et al., 2010; Parlar et al., 2016) and poor treatment outcomes (Bae et al., 2016; Kleindienst et al., 2016). Therefore, improving understanding of the relationship between shame and dissociation is crucial.
A vast body of research has proven the correlation between trait shame and trait dissociation (Dorahy, McKendry et al., 2017; Thomson & Jaque, 2013), but scant research exists on the potential causal relationship between shame and dissociation, especially in the context of traumatic events. Knowledge of the direction of the association would have major implications for the best practice of psychologists or officers in emergencies. Suppose that shame leads to an increase in dissociative experiences. In that case, professionals should be trained to detect signs of dissociation as a potential response, for example, when questioning a victim of sexual assault or when addressing shameful topics in a therapy session. However, if dissociation antecedes shame, professionals should focus on psychoeducation, therapeutic relationships, and anti-dissociative techniques.
Shame and dissociation relationship theories
There are several theories concerning the potential causal relationship between shame and dissociation with three possible directions: Shame causing dissociation, dissociation causing shame, or a bi-directional relationship.
The most prominent theory regarding shame as a cause of dissociation is the bypass theory (Lewis, 1971; Platt et al., 2017), which proposes that dissociation helps people avoid feelings of shame via emotional numbing and distancing from the current situation. There is some empirical evidence for this theory. However, it is difficult to test because it proposes a brief, possibly unconscious surge of shame quickly followed and "gilded" by the appearance of dissociative symptoms. It is difficult to measure this brief surge of shame. Some researchers see dissociations as emotion regulation mechanisms, which would explain their occurrence after or during aversive feelings of shame, hence supporting bypass theory. However, most evidence can only support a correlation between trait shame and trait dissociation (Irwin, 1998; Rudy et al., 2022; Talbot et al., 2004; Thomson & Jaque, 2013).
To our knowledge, only two empirical projects have investigated the activation of dissociative symptoms through shame. One study by Dorahy, McKendry et al. (2017) induced acute feelings of shame in students with shameful and neutral scenarios. After listening to one randomly selected shame or neutral scenario, the participants were asked to recite the scenario sentence by sentence in the first person. State shame and dissociation were significantly higher after shameful scenarios, even when controlling for trait shame and dissociation. The co-occurrence of state shame and dissociation contradicts the bypass theory. The authors could only partially replicate these findings in a clinical sample. While state dissociation could be induced, increases in state shame were only marginal and even smaller when controlling for trait shame. This might point toward different mechanisms in people with a history of trauma and mental illness; however, it remains unclear why no differences in trait shame were found between clinical and healthy participants. The authors concluded that shame leads to dissociation but the latter does not effectively decrease state shame, as suggested by the bypass theory.
A second experimental study by Platt et al. (2017) investigated this postulated relationship between shame and dissociation. Researchers asked participants to remember a situation with feelings of detachment, followed by the presentation of sentences associated with dissociative symptoms. They argued that, according to bypass theory, there should be a negative correlation between state shame and dissociation. However, similar to the results of Dorahy, McKendry et al. (2017), state shame and state dissociation were positively correlated. Platt et al. (2017) suggested that future studies should always control for trait shame in the statistical analysis using, for example, latent change structural equation modeling (SEM).
Furthermore, Platt et al. (2017) proposed betrayal trauma theory as an alternative explanation for the positive relationship between dissociation and shame. Both shame and dissociation may protect the relationship with the aggressor after interpersonal trauma through a known offender. Following this theory, one would expect higher trait shame and stronger reactions to shame and dissociation in this subgroup. However, the results of Platt et al. (2017) did not corroborate this notion. The authors argued that the induction of dissociation may, in return, trigger shame about being in a (humiliating/undesired) dissociative state.
Dissociation theory suggests that dissociation triggers feelings of shame because one perceives dissociation as a flaw that is disapproved by others. Furthermore, dissociative states can be considered signs of failure to control mental and behavioral processes (Cardeña, 1994; Holmes et al., 2005). Hence, McKeogh et al. (2018) argue that this loss of control is perceived as not meeting internal and external social standards, which leads to feelings of shame as theorized by Lewis (1998). Using data from structured interviews, Dorahy (2010) found that state dissociation works as a mediator between trait shame and relationship problems. The analysis of questionnaire data showed that both trait shame and dissociation were significant predictors of relationship problems, a finding replicated in a later study by Dorahy, Corry et al. (2017) in patients with PTSD.
Building on these findings, McKeogh et al. (2018) hypothesized that dissociative experiences, especially in the presence of other people, may lead to increased feelings of shame via negative comparisons, thoughts about the inability to maintain contact, and rejection. They investigated this theory and the question of whether dissociation also leads to shame when alone. Participants received one of three vignettes about dissociative experiences or one of three vignettes about sad experiences. Furthermore, descriptions were set in different contexts (alone, meeting an old acquaintance, or meeting a close friend). Only the context “close friend” resulted in higher shame after the dissociation vignettes than after the sadness vignettes. The authors concluded that dissociation is a marker for discontinuity and destabilization in close relationships leading to concerns about relational ruptures and social exclusion. They called dissociation a “natural shamer when occurring with close others” (McKeogh et al., 2018, p. 53). Dorahy et al. (2021) replicated the above study with a college sample as well as with a small sample of participants with mental illness; however, rather than standardized vignettes, they used a memory retrieval task similar to that used by Platt et al. (2017) and Zoellner et al. (2007). State shame increased after the successful induction of dissociation in the non-clinical sample, and higher state shame was reported compared to the baseline.
Interestingly, state dissociation did not increase through the memory retrieval task in the clinical sample but still significantly predicted state shame after computing a median split on state dissociation measures. Although the hypothesis was only partly confirmed, this study supports the theory of dissociation causing shame. The study gives more insight into the potential causes of dissociation leading to shame, as participants reported feeling “flawed” and “exposed” after the induction, which aligns with the assumptions of Lewis (1998).
In summary, the results point toward the third potential relationship, which is a bi-directional relationship between shame and dissociation, implying a mutual influence at the state and trait level. However, due to methodological differences between the studies, some questions remain unanswered.
In this study, we aimed to investigate the relationship between shame and dissociation and the role of trait markers using an experimental approach with healthy participants. The focus of this study was two-fold: First, we wanted to address methodological questions and replicate the results of Dorahy, McKendry et al. (2017) using McKeogh et al.’s (2018) dissociation induction method. We aimed to explore whether all six scenarios worked equally well for provoking shame and dissociation. Additionally, we planned to replicate the provocation of shame using vignettes (McKeogh et al., 2018) and explore their usefulness and potential for provoking dissociative states. Furthermore, we sought to explore the unique effect of the shame vignettes on state shame and dissociation vignettes on state dissociation.
Second, we sought to investigate the nature of the relationship between shame and dissociation by testing contradicting theories against each other. Bypass theory predicts that participants with high trait shame will show a more pronounced change in state dissociation and a less pronounced increase in shame in both induction conditions. The dissociation theory predicts that an increase in state dissociation is associated with increased state shame. Furthermore, in the dissociation induction condition, trait shame should positively predict state shame and changes in state shame. Meanwhile, under shame induction conditions, trait dissociation should positively predict state dissociation and changes in state dissociation. Lastly, we explored the role of interpersonal trauma, as stated in betrayal trauma theory. We hypothesized there would be a significant positive correlation between the number of interpersonal traumata, trait shame, and trait dissociation and that the number of interpersonal traumata predicts an increase in state shame and state dissociation in the shame induction condition.
Materials and methods
Participants
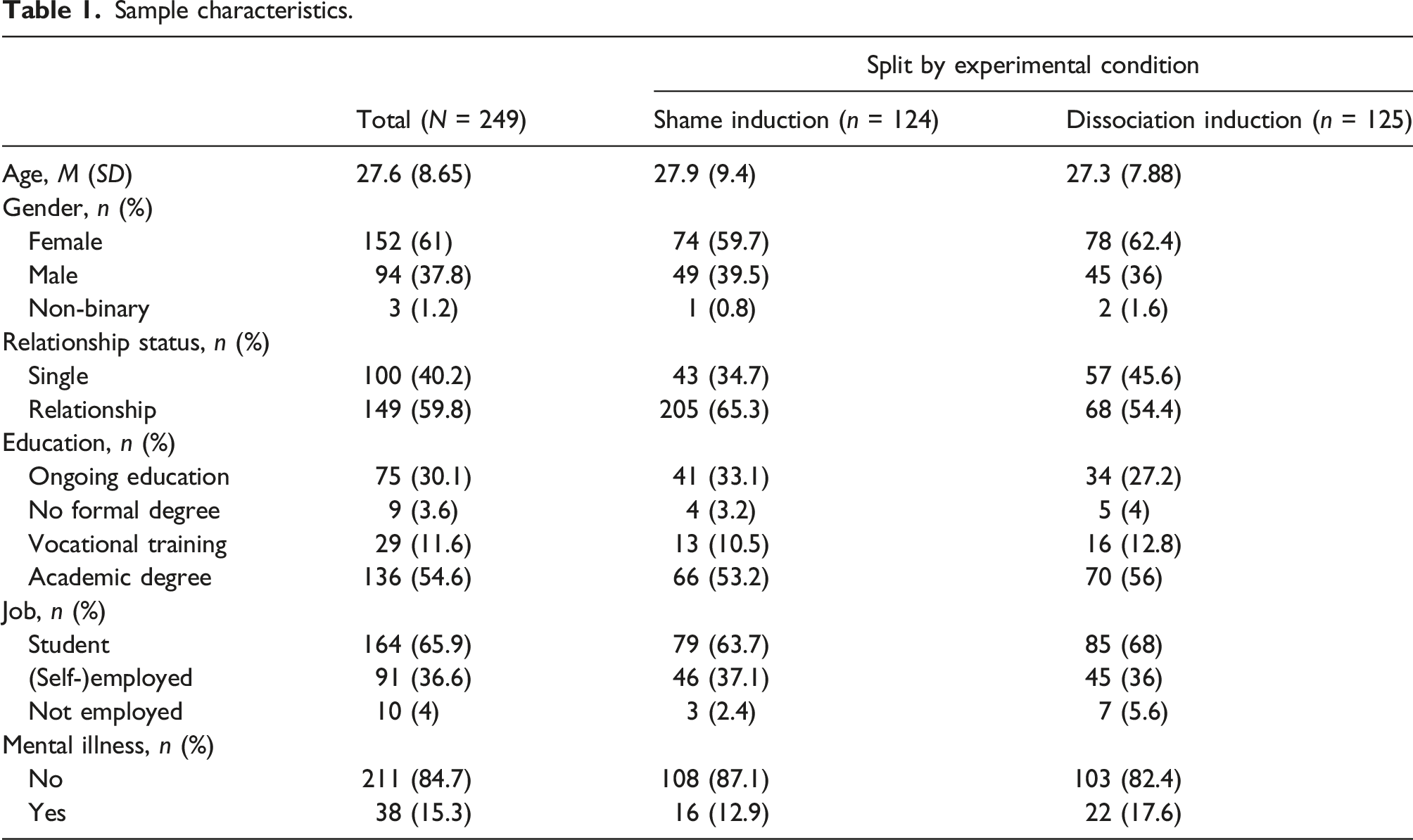
Sample characteristics.
Materials and procedures
Participants first completed a brief demographic and trauma survey (see Table 1). After randomization 1, group A completed trait variable questionnaires (FDS-20, SHAME, randomized order). Then, all participants completed state questionnaires (DSS-akut and EES) at T1. They were then randomly allocated to one of 6 vignettes (3 for dissociation induction (amnesia, depersonalization/derealization, and flashback), 3 for shame induction (bank, bedroom, and public pool)), after which they completed state questionnaires at T2. Group B filled out trait variables (FDS-20, SHAME, randomized order) after assessing state variables at T2. The full procedure is shown in Figure 1. Experimental procedure.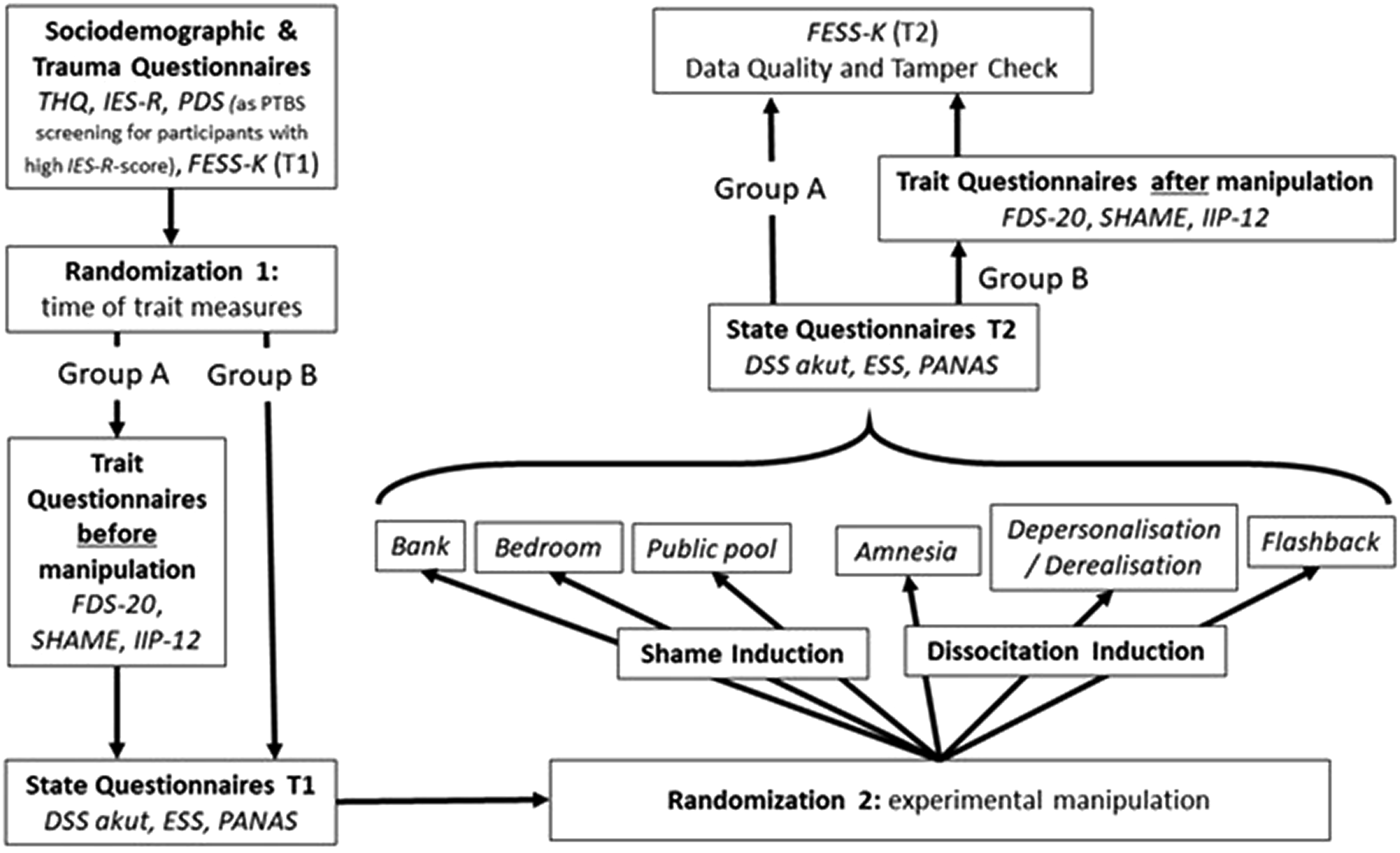
Vignettes were created based on the original vignettes used by McKeogh (2019) for dissociation and Dorahy, McKendry et al. (2017) for shame. They were translated and retranslated in order to secure their validity and then audio recorded with a mean duration of about 3.5 minutes. Before the audio file started, an audio instruction invited participants to repeat each sentence in the first person and to imagine the scenes as vividly as possible. While the audio file was playing, with a short break after each sentence to enable repetition, a white screen was presented. A black screen was deliberately omitted during the scenario presentation because reflections that would result from glass monitors could also induce dissociative symptoms (cf., Mirror-Gazing Task, Caputo (2010)). The mean duration of the experiment was 50 minutes.
Further information on the materials as well as on the questionnaires not included in this analysis, can be found at OSF.
The Dissociation-Tension-Scale acute (Dissoziations-Spannungs-Skala akut, DSS-akut) was used to assess state dissociation (Stiglmayr et al., 2003). The scale comprises 21 items and measures the acute experience of dissociative symptoms by means of a 10-point scale. It correlates highly with the DES, and other trait dissociation measures. It is reliable and satisfactorily valid and has a high sensitivity to change (Stiglmayr et al., 2010). In the present study, the internal consistency of the DSS-akut at T1 was α = .94 and α = .96 at T2.
State shame was measured using the German translation of the Experiential Shame Scale (ESS, Rüsch et al., 2007; Turner, 1998), which was designed to measure physical, emotional, and social markers of feelings of shame. The 11 items of the ESS are presented as 7-level polarity profiles. The ESS has shown satisfactory internal consistencies of .74 ≤ α ≤ .81, and construct validity has been reviewed and confirmed (Turner, 2014; Turner & Waugh, 2001). In the present study, Cronbach’s alpha at T1 was α = .73 and at T2 α = .85.
The Fragebogen zu Dissoziativen Symptomen 20 (FDS-20, Spitzer et al., 2004) is a well-validated short form of the German Version of the Dissociative Experience Scale for assessing trait dissociation (Carlson & Putnam, 1993; Rodewald et al., 2006). The scale consists of 20 items. On an 11-point scale, participants are asked about their experience of dissociative symptoms during the last 2 weeks. In contrast to the long form, the FDS-20 has a one-factor structure. It has been shown to be a time-stable measure and hence is suited for assessing trait markers. Internal consistency in the current study was Cronbach’s α = .95.
The Shame Assessment for Multifarious Expressions of Shame (SHAME) questionnaire was used to assess trait shame (Scheel, Bender et al., 2013). For this purpose, participants are presented with 21 potentially shameful events and asked to indicate how much they would feel ashamed in those situations, with six graduations from “I am not ashamed (0)” to “I am very ashamed (5).” The questionnaire exhibits construct validity (Scheel et al., 2020). Cronbach’s alpha was α = .88 for the total scale in this study.
For assessing trauma, the Trauma History Questionnaire – German Version (THQ, Maercker & Bromberger, 2005) was used. This original self-report checklist contains 24 items listing traumatic events. Participants state if they have ever experienced the event described. We adapted the scale by omitting the item “exposure to chemicals/radioactivity” and added eight items describing events based on a slightly broader trauma definition due to the non-clinical sample. For the analysis, we coded relevant items as interpersonal trauma and calculated the sum of interpersonal trauma (see supplemental material on OSF).
Data analysis
Two 2 × 3 ANOVAs with repeated measures were computed to compare the three scenarios within each group. The interaction between time (T1 vs. T2, within factor) and scenario (shame: bank vs. bedroom vs. public pool; dissociation: amnesia vs. depersonalization/derealization vs. flashback, between factors) was investigated in each experimental group separately using a Bayesian approach. A multivariate Cauchy distribution was chosen as a prior probability distribution, defined by a distance to the grand mean of 0.5.
Preceding the main analyses, all scales were centered using the mean of the shame group. The centering was conducted to increase model fit. A random group was chosen to center the data rather than using the mean of the whole sample to simplify the model. The intercepts of the shame group could be fixed to one, and a significant intercept for the dissociation group indicates group differences. The hypotheses were then tested using structural equation modeling, based on maximum likelihood estimation. First, a multi-group base model was estimated, depicted in solid black in Figure 2. The two experimental groups, the shame and dissociation groups, were fitted within the model. State at T1 and change between T1 and T2 were estimated as latent variables for dissociation and shame, based on the DSS-akut and ESS, respectively. The latent variable estimating state dissociation at T1 was allowed to covary with the latent variable estimating state shame at T1. Structural equation models: Multi-group base model (black) and full multi-group model (black and gray).
Further, a covariance between both change variables was added to the model. The intercepts of both state measures at T1 latent variables were fixed to zero in the shame group and estimated freely in the dissociation group. This was in line with the centering of the variables and meant that a significant intercept within the dissociation group would indicate baseline differences between both groups. Intercepts for both latent change variables were estimated freely in both groups.
In a second step, covariates were added to the model, building the full multi-group model depicted in black and gray in Figure 2. The added covariates were trait dissociation, trait shame, and interpersonal trauma. Intercepts for each of these variables were again fixed to zero within the shame group and estimated freely within the dissociation group. Each of the three variables was regressed on all four latent variables. In addition, trait dissociation and trait shame were regressed on interpersonal trauma.
The two experimental conditions (shame induction vs. dissociation induction) differed with regard to the trait variables: participants in the shame induction condition reported significantly lower values on trait variables. Additional analyses revealed that university students reported significantly lower baseline values than the other subsamples. Furthermore, trait measures were—in contrast to our expectations—influenced by the experimental manipulation. As for some participants, trait measures were assessed after the experimental manipulation (groups A and B, see Figure 1); this resulted in significantly lower values in group A for trait variables. By chance, the randomization resulted in a higher rate of university students and people from group A in the shame induction condition. This led to significant differences in trait variables between experimental groups. These aspects were controlled for in all analyses.
The 2 × 3 ANOVAs with repeated measures were computed in JASP. The main analyses were conducted using lavaan (Rosseel, 2012). Scripts, including our model specifications, are provided on OSF. Model fit was evaluated using the chi-square test, the comparative fit index (CFI), the root-mean-square error of approximation (RMSEA), and the standardized root-mean-square residual (SRMR). CFI above .95, RMSEA below .06, and SRMR below .08 are considered to indicate good model fit (Hu & Bentler, 1998).
Results
First, descriptive statistics are provided for the sample. Second, the results of the 2 × 3 ANOVAs comparing the scenarios will be reported. Then the multi-group base model results are presented, investigating only state measures of shame and dissociation in both experimental groups. Lastly, the full multi-group model is reported, including trait shame, trait dissociation, and interpersonal trauma as covariates.
Descriptive statistics
Means and standard deviations of main measures on both experimental groups.

Note. Means with standard deviations are given in parentheses.
Comparison of different scenarios inducing shame and dissociation
We stated that state shame increases equally from T1 to T2 in all three scenarios in the shame group. In comparison, dissociation increases equally from T1 to T2 in all three scenarios in the dissociation group. The results of the 2 × 3 ANOVA for the shame group indicate that the data was 7.91 times less likely under the model, including the interaction between time and scenarios, than under those models, which only include the main effects. This is moderate evidence against the interaction, supporting our hypothesis. Computing the 2 × 3 ANOVA for the dissociation group, the data was 14.78 times less likely under the model, including the interaction between time and scenarios, than under those models, which only include the main effects. This is strong evidence against the interaction, supporting our hypothesis. Consequently, we aggregated the 2 × 3 scenarios to one shame and one dissociation induction condition.
Comparison of induced shame and dissociation in both experimental groups
Results of the multi-group base model.
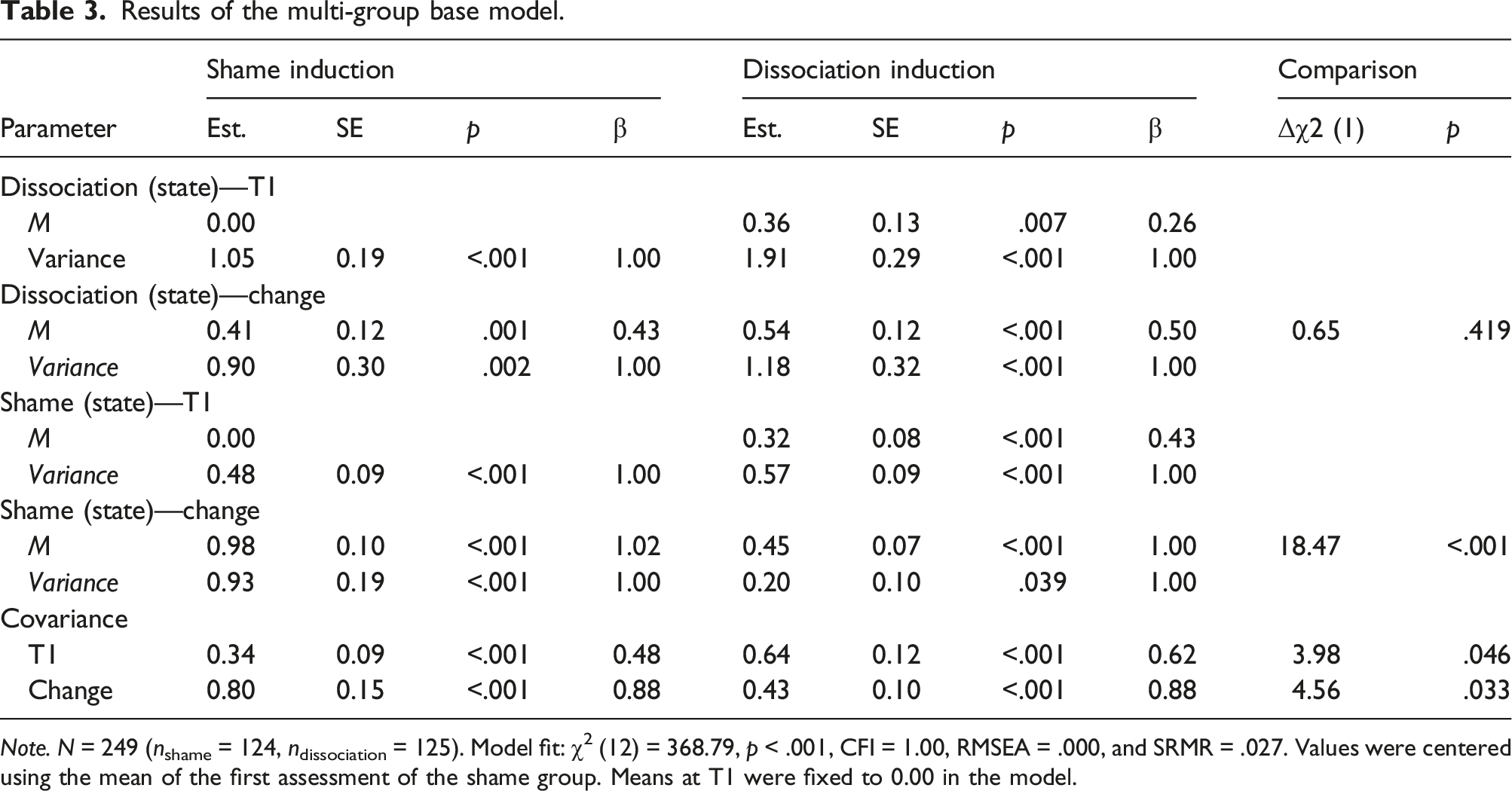
Note. N = 249 (nshame = 124, ndissociation = 125). Model fit: χ2 (12) = 368.79, p < .001, CFI = 1.00, RMSEA = .000, and SRMR = .027. Values were centered using the mean of the first assessment of the shame group. Means at T1 were fixed to 0.00 in the model.
We stated that state shame is expected to increase in the shame group, while state dissociation should increase in the dissociation group. To test the first half of the hypothesis, the change in state shame in the shame group was tested against zero. The results show that state shame significantly increased in the shame group (see Table 2). The change in state dissociation in the dissociation group was tested against zero to test the second half of the hypothesis. The results show that state dissociation significantly increased in this group (see Table 2). Therefore, the hypothesis is supported by the data.
We further stated that the shame induction condition elicits a stronger increase in state shame than the dissociation induction condition. In comparison, the dissociation induction condition elicits a stronger increase in state dissociation than the shame induction condition. The change in state shame was compared between both groups to test the first half of the hypothesis. State shame increased more strongly in the shame group than in the dissociation group (see Table 2). To test the second half of the hypothesis, change in state dissociation was compared between both groups. Because the increase in state dissociation did not vary between both groups, the data only partially supported the hypothesis.
Influence of covariates on induced shame and dissociation in both experimental groups
Results of the full multi-group model.
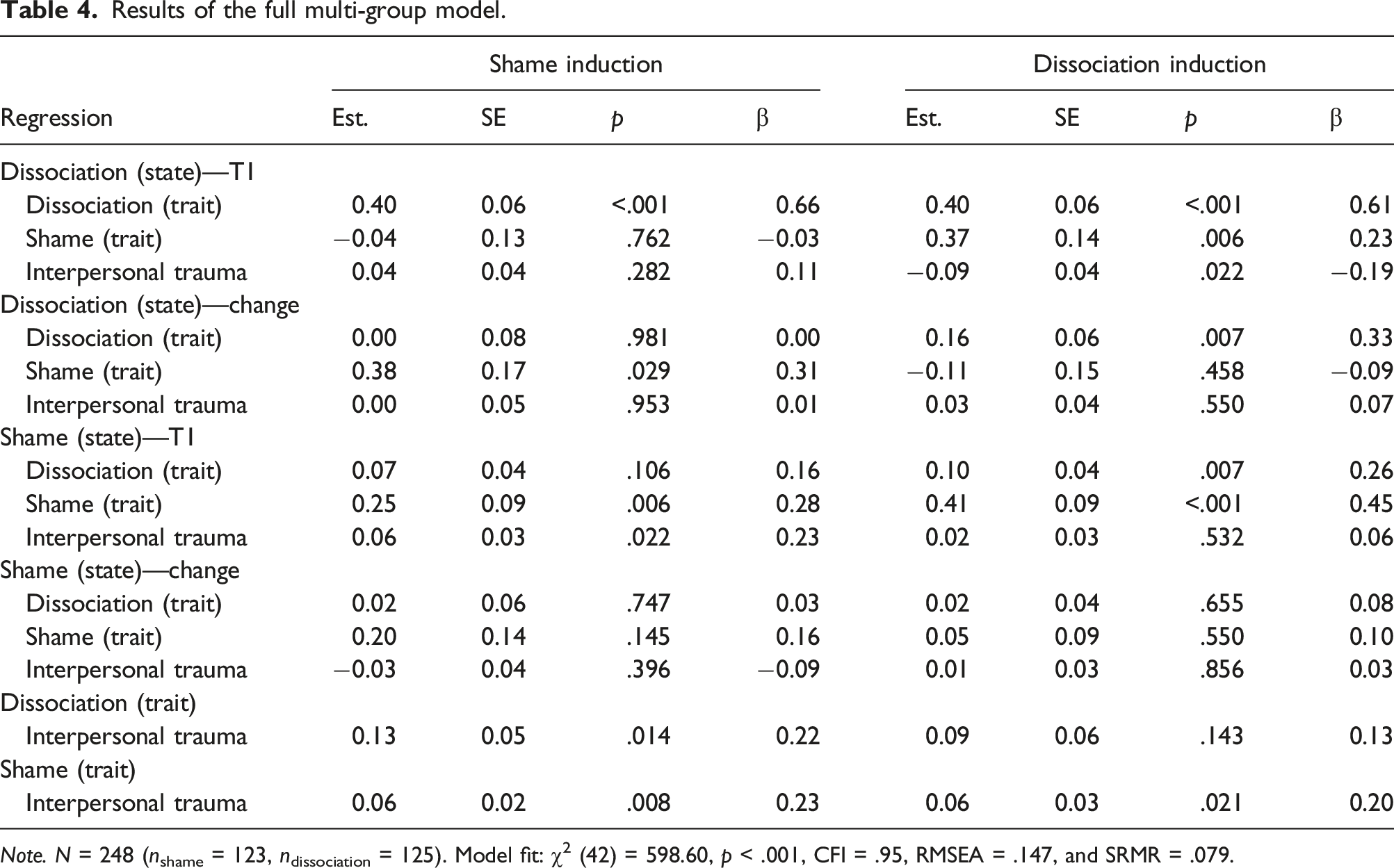
Note. N = 248 (nshame = 123, ndissociation = 125). Model fit: χ2 (42) = 598.60, p < .001, CFI = .95, RMSEA = .147, and SRMR = .079.
We hypothesized that participants with higher values in their trait shame show a stronger increase in their state dissociation and a weaker increase in their state shame. This hypothesis was not supported by the data. In the dissociation group, trait shame was neither associated with a change in state dissociation nor a change in state shame (see Table 4). While higher values for trait shame were associated with a stronger increase in state dissociation in the shame group, there was no association between trait shame and change in state shame. We further stated that in the dissociation group, an increase in state shame is associated with an increase in state dissociation. The data supported this as the covariance between both variables was positive and significant (see Table 4).
We assumed that trait shame positively predicts state shame prior to the intervention. The data within both groups supported this (see Table 4). The higher the trait shame is, the higher is the state shame at the first assessment. We further stated that trait shame additionally predicts the change in state shame in the dissociation group. This was not supported by the data, as no association between trait shame and change in state shame existed in the dissociation group. With regard to dissociation, trait dissociation positively predicted state dissociation prior to the intervention. This was only true for the dissociation group, where higher values in trait dissociation were associated with higher state dissociation at the first assessment. There was no association between these variables in the shame group. The hypothesis was, hence, only partially supported by the data. We further assumed that trait dissociation is positively associated with a change in state dissociation in the shame group. This was not supported by the data as there was no association between both variables in the shame group.
We expected that interpersonal traumata were associated with trait shame and trait dissociation. This was mostly supported by the data. In the shame group, trait shame and trait dissociation were higher for people with more interpersonal traumata (see Table 4). In the dissociation group, more interpersonal trauma was only associated with higher trait shame. There was no association with trait dissociation. Lastly, we assumed that more interpersonal traumata were associated with a stronger increase in state shame and state dissociation in the shame group. This was not supported by the data as interpersonal traumata were not associated with either change in state shame or a change in state dissociation.
Discussion
Using Bayesian analysis and latent change SEM, we investigated the relationship between shame and dissociation in a predominantly healthy student sample. In general, the results were in line with those of Dorahy, McKendry et al. (2017) and McKeogh et al. (2018). We found no differences between the three dissociation scenarios provoking dissociation or between the shame scenarios provoking shame. Future studies could hence use only one scenario. While shame vignettes led to a stronger increase in state shame without increasing state dissociation, dissociation vignettes resulted in increases in dissociation and shame. These findings contradict Dorahy, McKendry et al. (2017), who proposed the shame induction method as a possible dissociation induction method.
Nevertheless, our results are in line with those of Schultz (2018), who suggested that dissociative symptoms cannot be provoked specifically by using vignettes. Neither Zoellner et al. (2007) nor Leonard et al. (1999) assessed state shame; hence, they were unable to investigate whether their dissociation induction also led to increased state shame. Therefore, the reason for our failed attempt to provoke dissociative symptoms alone (without elevating state shame) remains unclear. This could be a characteristic of our study, a general result of the vignette induction method, or support for the theory by Dorahy et al. (2021) stating that dissociation inherently leads to shame. Future studies should use different methods to induce dissociation while assessing both state shame and dissociation.
Regarding bypass theory, our study mostly adds to the research that does not support its core assumptions. We did not find that shame induction in participants with higher trait shame led to a stronger increase in dissociation and a weaker increase in state shame. Trait shame was not associated with changes in state dissociation or state shame. One possible explanation for our results may be that the mechanisms proposed by bypass theory are only true for participants with high levels of shame, such as when experiencing interpersonal trauma. This means that the levels of shame evoked in our study were not intense enough to provoke a dissociative response. This assumption can only be tested in a more natural setting with real and intense experiences of shame, which is highly questionable from an ethical perspective.
Additionally, it is difficult to test the assumptions of the theory using self-report questionnaires. We tried to solve this by choosing the opaque ESS for the assessment of state shame with the expectation that it might be less influenced by dissociative states. One solution for the self-report problem could be the extension of the dependent variables to physiological markers, such as the electrocardiogram and skin conductance response, where one should see a short increase in sympathetic activation as a marker of shame, followed by a parasympathetic rise when dissociation occurs. Another possibility would be the integration of heat maps (Nummenmaa et al., 2014) or magnetic resonance imaging of pain centers associated with shame (Brockman, 2017). However, this method also relies partially on self-reporting, and it is still unclear how universally valid these results are. The fact that we did not find an association between state and trait shame in the dissociation condition could also be interpreted as indicating the avoidance of shame through dissociation. However, we did find elevated state shame in this condition, indicating that participants experienced shame, which challenges this interpretation. Overall, it seems crucial to clarify the core assumptions of the bypass theory.
Our study supports Dorahy, McKendry et al. (2017), as we found a significant correlation in a non-clinical sample between state shame and dissociation in the dissociation group. This indicates that dissociation may lead to increased shame. All our dissociation vignettes described a close interpersonal situation, which is consistent with McKeogh et al. (2018), who found an increase in shame after the provocation of dissociation only in the "close friend" condition. However, this could also be because we asked participants to repeat each sentence in the first person, which creates a higher personal relevance and makes it difficult to differentiate this from the "close friend" condition effect. Given the potentially harmful consequences of shame after experiencing dissociation in settings such as a therapeutic relationship, the differential correlations as well as behavioral correlates should be examined with more detail and diverse methods.
Regarding the role of interpersonal trauma, we found correlations with trait shame and partly with trait dissociation. However, having experienced interpersonal trauma did not affect the change in state shame and state dissociation. This is somewhat contradictory to betrayal trauma theory. However, we did not assess whether the aggressor in interpersonal trauma was close. Furthermore, it might be that the association between trauma, shame, and dissociation, as stated in betrayal trauma theory, is only activated in a traumatic or at least a personal situation, making it difficult to investigate healthy subjects in a standardized experimental setting.
Limitations
Various methodological and content-related aspects limit the generalizability and informative value of the present study. Our sample consisted of mostly healthy participants, and it is unclear whether the processes we examined were not exclusively found in clinical populations. To ensure that processes and relationships are identical in clinical and healthy populations and to draw valid conclusions from studies using healthy participants, it is essential to examine the same study design in both populations (Waters et al., 2017). Hence, further studies should use this study’s methodology in a clinical population.
Furthermore, some aspects of the questionnaires were problematic. FDS-20 was used as a trait inventory for dissociation. Because of its one-dimensionality, it encompasses a range of dissociative experiences that originate from the pathological spectrum and, thus, cause large floor effects in the data. This could lead to lower robustness of statistical analyses and thus needs to be considered, the same being true for DSS-akut. Furthermore, we found significant baseline differences between the two experimental groups, as randomization did not work perfectly, and the FDS-20 was more susceptible to our experimental manipulation than anticipated based on prior studies (Spitzer et al., 2004). This indicates that the FDS-20 not only assesses trait dissociation measures but also seems to at least partly include some state-like aspects of dissociation. This could have confounded our results, most probably in the sense that the relations between "true" trait dissociation and state dissociation are weaker than the one we found. Investigating these findings, for example, by calculating confirmatory factor analysis with different state and trait dissociation measures (as in Latent-State-Trait-Theory, e.g., Kelava & Schermelleh-Engel, 2012) would be important as it is highly relevant for other studies investigating the relations between state and trait dissociation measures. It further seems advisable to include a “washing out task,” as in Dorahy et al. (2021), not only for shame but also for dissociation measures. Furthermore, the interpersonal trauma variable may represent a less valid construct because it was taken from subscales of the THQ, and only clearly interpersonal trauma was assigned to the category. A questionnaire measuring chronic interpersonal trauma during childhood and adolescence may have been more appropriate.
To replicate previous study findings, the dissociation and shame scripts from McKeogh et al. (2018) and Dorahy, McKendry et al. (2017) were adopted and presented via an online study in which subjects worked alone at their computers rather than in the laboratory with others present (e.g., investigators) due to the COVID-19 pandemic. This should be considered when comparing the results of the present work to those of previous studies.
We did not include a control group in this study, as our main goal was to test contradictory theories and assumptions against each other. We hence decided to test two "active" treatments (e.g., the induction of shame and the induction of dissociation) against each other. However, the dissociation vignettes used have not yet been tested against a control group with regard to their ability to provoke dissociative symptoms. Hence, future studies should test them against, for example, waiting for conditions or relaxation vignettes, as in Platt et al. (2017), to single out effects.
Conclusions
The interaction between shame and dissociation is complex. We identified trait shame as a risk factor for trait dissociation but not for state dissociation. High trait shame and trait dissociation can be risk factors for developing mental disorders, especially in combination with post-traumatic stress symptomatology or relationship problems.
As we were not able to specifically provoke dissociative symptoms using vignettes, it remains unclear whether the results of the imaginative dissociation induction procedures can be generalized to larger populations.
In regard to clinical practice, our findings indicate that therapists should be aware that clients may be ashamed of dissociative symptoms and, hence, may not talk about them. Establishing a basis for trust and informing patients about these phenomena could counteract this issue. Although we used a healthy sample, our findings might be generalizable to clinical samples as research has shown that shame-inducing events are stored in a type of trauma memory that manifests itself through intrusions, hyperarousal, and avoidance behaviors toward stimuli associated with the shame experience (Matos & Pinto-Gouveia, 2010). However, some assumptions regarding the relationship between dissociation, shame, and interpersonal trauma should be tested in clinical samples. In addition, future studies should integrate more objective measures of psychological constructs, as not all processes relevant to the relationship between dissociation and shame may be accessible through self-reports.
Overall, we found evidence for a bi-directional relationship between shame and dissociation, with slightly stronger evidence for dissociation leading to shame. The results of our study support the claim of Dorahy et al. (2015) that dissociation has implications for interpersonal relationships by eliciting shame and withdrawal. However, further research is still needed to better understand how and why these two phenomena influence one another.
Footnotes
Acknowledgments
We acknowledge the financial support for Open Access publication by Universität der Bundeswehr München. We thank Prof. Martin Dorahy for making the vignettes used in his studies available to us.
Author Contributions
Patricia Kulla: Conceptualization, data curation, methodology; project administration, roles/writing—original draft, and writing—review and editing.
Tim Reichenberger: Data curation, methodology, and roles/writing—original draft.
Tina Braun: Formal analysis, roles/writing—original draft, and writing—review and editing.
Joachim Kruse: Supervision and writing—review and editing.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: We acknowledge financial support from Universität der Bundeswehr München (FORScience - Open Acces Fund Journals).