
Abstract
Cognitive behavioral therapy (CBT) focuses on decreasing negative affect rather than increasing positive affect and is ineffective for some individuals. A trial comparing novel Positive Affect Treatment (PAT) to Negative Affect Treatment (NAT; a form of CBT) showed that PAT more effectively increased positive affect and decreased negative affect, depression, and anxiety (Craske et al., 2019). The present exploratory study examined threat sensitivity as a treatment moderator. Threat sensitivity was operationalized as pre-treatment skin conductance response and unconditional stimulus (US) expectancy rating during extinction recall. Participants (N = 43) then received 15 sessions of PAT or NAT. Growth curve models were tested to explore interactions between extinction recall and treatment condition over time. For skin conductance, weaker extinction recall predicted faster improvement in depression and anxiety in NAT than PAT, whereas stronger extinction recall predicted faster improvement in symptoms in PAT than NAT. Reduced US expectancy ratings predicted a faster decrease in symptoms, regardless of treatment condition. Individuals showing greater threat sensitivity, indexed by weaker extinction recall, may benefit more from a treatment that targets threat sensitivity than a treatment that targets reward sensitivity. Individuals showing the converse may benefit more quickly from a treatment that targets reward sensitivity than threat sensitivity.
Keywords
Exploratory study of threat sensitivity as a moderator of positive affect treatment and negative affect treatment for depression and anxiety
Depression and anxiety are highly comorbid conditions that share diagnostic features (Eysenck & Fajkowska, 2018; Lamers et al., 2011; Winer et al., 2017). Initiatives such as the Research Domain Criteria (Cuthbert & Insel, 2013; Sanislow et al., 2019) utilize a dimensional approach to conceptualize depression and anxiety as dysfunctions in core constructs, including the positive and negative valence systems. The positive valence system is primarily responsible for positive motivational situations or contexts, whereas the negative system is predominantly responsible for defense against threats and punishments.
Cognitive behavioral treatments (CBT) for depression and anxiety have mainly targeted negative affect and threat sensitivity (Craske et al., 2016), with the exception of behavioral activation, which is designed to increase response contingent positive reinforcement (Martell et al., 2021). Given that behavioral activation has limited effects upon positive affect in the few studies in which it has been reported (Dichter et al., 2009; Moore et al., 2013), newer psychological treatments have emerged, such as Amplification of Positivity Therapy (Taylor et al., 2017) and Positive Affect Treatment (PAT; Craske et al., 2016). PAT was explicitly designed to increase positive affect by targeting deficits in reward processing (Craske et al., 2016). In a randomized controlled trial for depressed or anxious individuals, PAT was compared to negative affect treatment (NAT), or a form of cognitive behavioral therapy focused explicitly upon reducing negative affect and threat sensitivity (Craske et al., 2019). Whereas both treatments led to significant improvements in depression, anxiety, suicidal behavior, and positive affect, individuals receiving PAT showed superior outcomes on all measures. Nonetheless, certain individuals may respond more strongly to one treatment than another, depending on pre-treatment characteristics (Kraemer et al., 2006). Therefore, the goal of the current study was to evaluate pre-treatment threat sensitivity as a treatment moderator. Since NAT focuses on reducing negative affect and threat sensitivity, it was hypothesized that individuals who show elevated threat sensitivity could benefit more from NAT than PAT.
Fear conditioning (FC) is a well-validated assessment of threat sensitivity (Lonsdorf et al., 2017). FC paradigms assess acquisition and extinction of fear to a conditional stimulus (CS), and this extinction learning process forms the foundation for exposure therapy, a core feature of NAT (Craske et al., 2019, 2022). Thus, we specifically focused on impairment in extinction learning as a potential predictor of differential treatment response, where NAT is best suited to target this impairment. Relative to healthy controls, anxious individuals show elevated CS fear in simple FC paradigms (where a single CS is paired with an aversive unconditional stimulus [US]), decreased differentiation between a CS+ and CS- (where a CS+ is paired with an aversive US and CS- is unpaired), and elevated conditional fear during extinction training or at extinction recall (Duits et al., 2015; Scheveneels et al., 2021). Group differences are particularly evident neurally during extinction recall, a measure of long-term extinction learning (Marin et al., 2020; Schwarzmeier et al., 2019). Weak extinction training/extinction recall has been identified as a potential risk factor for anxiety (Duits et al., 2015). FC findings in depressed individuals are mixed, with some evidence for enhanced fear acquisition and enhanced extinction training compared to healthy controls (Kuhn et al., 2014; Nissen et al., 2010) and enhanced fear acquisition compared to individuals with anxiety (Dibbets et al., 2015), and others reporting no differences compared to healthy controls (Kuehl et al., 2020). With respect to treatment outcome, superior extinction training predicted superior response to exposure interventions in persons with anxiety disorders, for example, adults with public-speaking anxiety (Ball et al., 2017), adults with spider phobia (Forcadell et al., 2017), children with obsessive compulsive disorder (Geller et al., 2019), and a mixed sample of children with anxiety (Waters & Pine, 2016), although one study of adults with specific phobia failed to replicate this effect (Wannemueller et al., 2018).
As a measure of long-term learning, extinction recall arguably is a more sensitive index than extinction training per se for treatment prediction, but results to date are limited and contradictory. Stronger extinction recall predicted weaker outcomes (less fear reduction) in an exposure therapy analog (Forcadell et al., 2017), but superior outcomes (greater completion of an exposure task within a pre-determined time) in another study (Raeder et al., 2020). However, both studies tested extinction recall immediately following extinction training when a more appropriate evaluation is at least 24 hours following extinction training, and neither controlled for fear acquisition. Further research is therefore needed to examine extinction recall as a predictor of treatment outcome.
The current study aimed to explore FC, a measure of threat sensitivity, as a moderator of treatment outcome for PAT and NAT. Individuals with greater threat sensitivity are presumed to benefit more from a treatment that specifically targets such sensitivity (i.e., NAT) than a treatment that targets reward sensitivity (i.e,. PAT). In this exploratory study, using extinction recall as a measure of threat sensitivity, we hypothesized that individuals with weak extinction recall, measured as greater pre-treatment difference between CS+ and CS- in skin conductance response and in US expectancy, will show more rapid symptom reductions in NAT than PAT.
Material and methods
Participants
Participants were part of a multi-site, randomized controlled trial comparing PAT and NAT for depression and anxiety and were recruited from the University of California, Los Angeles (UCLA) and Southern Methodist University (SMU) in Dallas, Texas. The study obtained ethical approval by the UCLA Medical Institutional Review Board (IRB#13-000315) and the SMU Institutional Review Board (2021-122-MEUA) and all participants provided written informed consent. Participants met inclusion criteria if they were 18–65 years of age, English-speaking, stable on psychotropic medications (1 month for beta-blockers and benzodiazepines, 3 months for selective serotonin reuptake inhibitors and heterocyclics) or not taking any medications, and agreed to refrain from starting or adjusting psychotherapy or pharmacotherapy until after the 6-month follow-up. Participants had to meet moderate to severe depression or anxiety and functional impairment using cut-offs on the Depression Anxiety Stress Scales (DASS-21; Lovibond & Lovibond, 1995)
The sample for this secondary analysis comprised participants previously reported on in Craske et al. (2019; n = 96 randomized to PAT or NAT), plus data from additional participants collected beyond the prior publication (n = 22). Data collection for psychophysiological assessments began partway through the trial. Therefore, out of the 118 total participants in the trial, 67 participants were excluded because they were not administered the psychophysiological assessment. Eight additional participants were excluded because they did not complete at least two treatment sessions. A total of 43 participants were therefore included in present analyses (UCLA n = 18; SMU n = 25). For the FC task extinction recall analysis, 7 participants were excluded due to equipment failures/errors in task administration (e.g., portions of extinction training or extinction recall protocols not run), leaving 36 participants (PAT n = 21, NAT n = 15) out of the original 43. Because of the repeated assessments obtained in this study, there were a total of 502 data points available for analysis. Given the small number of participants, analyses are considered exploratory and findings should be interpreted with caution. On the other hand, simulations from (Maas & Hox, 2005) have shown that multilevel modeling, as conducted in the present study, produces accurate and unbiased estimates in sample sizes as small as n = 30.
Sample characteristics
Demographic Characteristics (N = 43).
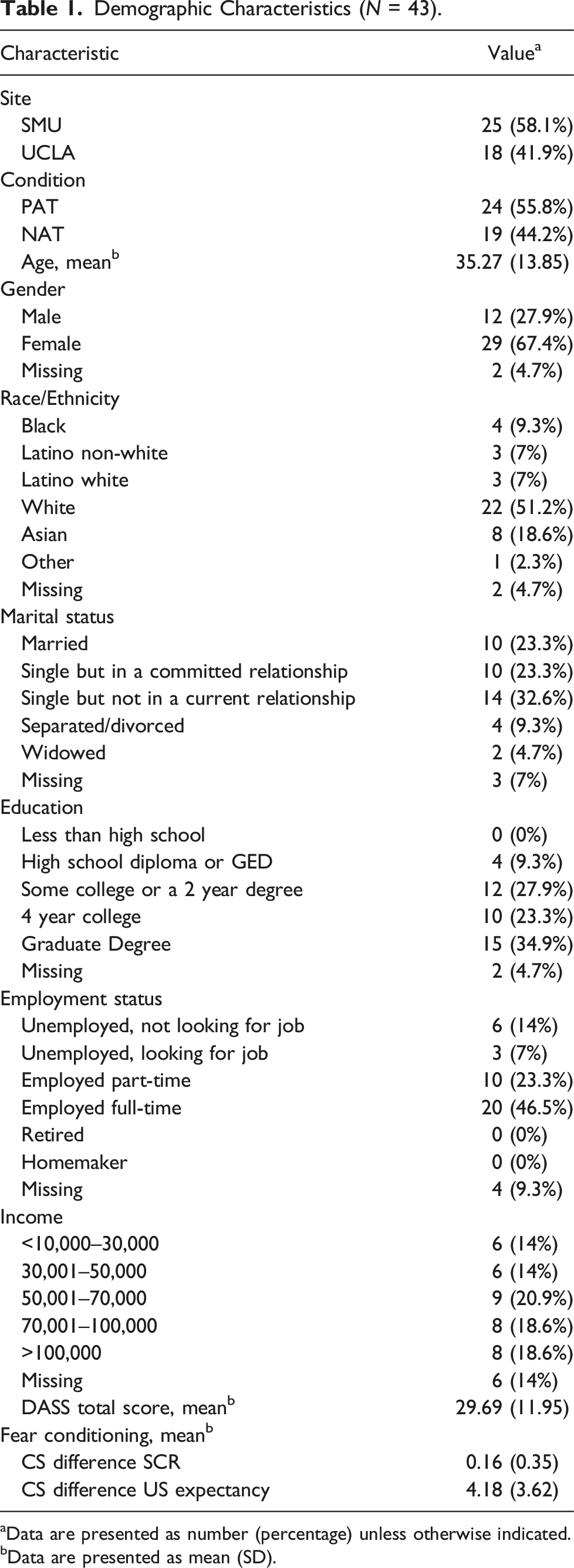
aData are presented as number (percentage) unless otherwise indicated.
bData are presented as mean (SD).
Treatment
Both treatments comprised 15 weekly, one-on-one sessions. PAT aims to increase positive affect and associated deficits in reward sensitivity (see Craske et al., 2016, 2019) and consists of three modules: Augmented Behavioral Activation Training (sessions 1–7), Cognitive Training: Attending to the Positive (session 8-10), and Compassion Training: Cultivating the Positive (sessions 11–14). NAT aims to decrease negative affect and associated threat responsivity and comprised three modules: Augmented Exposure Training (sessions 1–7), Cognitive Training (sessions 8–10), and Respiratory Training (sessions 11–14). In both conditions, Session 15 consisted of relapse prevention. Participants were randomly assigned to a trained study therapist, advanced clinical psychology graduate students supervised by licensed clinical psychologists, and to PAT or NAT. See Craske et al. (2019) for further intervention and therapist details.
Fear conditioning (FC)
The US was a one-second, loud scream set at 107 dB delivered through Sony stereophonic headphones, similar to previous studies (Culver et al., 2018; Staples-Bradley et al., 2018). Unpleasant sound stimuli such as this elicit comparable or superior conditioning effects to electric shock (Neumann & Waters, 2006). The to-be-conditional stimuli (CS) were two neutral faces (8.5 cm wide and 10.5 cm high): each presented for 8 seconds at a distance of 6.5 cm either to the right or left of a central fixation cross on equal number of trials, presented on a Dell 21” color monitor at a distance of one m and a visual angle that averaged 9.6°. During acquisition, participants received 16 trials, eight CS+ and eight CS-, presented in random order with the caveat that no more than two trials of either CS would be presented sequentially and that the first two trials would be a CS+ and a CS-. CS+ was paired with a US (offset commensurate with CS offset) with 100% reinforcement rate. The CS- was always presented alone. Intertrial intervals (ITIs; from one CS onset to the next) varied across 20, 25, and 30 seconds (mean = 25 seconds). Extinction training consisted of eight trials: four CS + trials and four CS- trials. Trials were presented in random order with no more than two sequential presentations of either CS. Extinction recall replicated extinction training and took place an average of 12 days later, immediately before the first treatment session.
Skin conductance response (SCR) was recorded with two Ag/AgCl electrodes (6 mm inner diameter) filled with isotonic electrolyte gel. Electrodes were attached to the thenar and hypothenar eminences of the non-dominant hand. Throughout the tasks a constant voltage of 0.5 V was applied across the electrodes that were connected to a BIOPAC SCR 100 C amplifier with a gain of 2 mS/V. SCR was recorded continually via AcqKnowledge 3.73 software at a sampling rate of 1000 Hz. SCR was calculated by subtracting baseline skin conductance level (−2 to 0 seconds before CS onset) from maximum response (1–6 seconds after CS onset). Range corrections were calculated by identifying the maximum SCR to any CS for each participant. SCRs were square-root transformed and divided by the range correction value, as recommended by Lonsdorf et al. (2017).
Participants also completed self-reported US expectancy ratings after each CS+ and CS- trial, using a 0 to 9 scale (“certain no scream sound would occur” to “certain scream sound would occur.”). For extinction recall, difference scores for SCR and US expectancy ratings were calculated (CS + minus CS-) from the first two CS+ and CS- trials of extinction recall, averaged, similar to previous studies (Forcadell et al., 2017; Garfinkel et al., 2014).
Outcome measures
Self-report measures were assessed at pre-treatment, before each treatment session, post-treatment, and at 6-month follow-up, for a total of 18 assessment time-points. Treatment outcome was measured using the DASS-21, a short-form of the original 42-item DASS (Lovibond & Lovibond, 1995). The DASS-21 includes three 7-item subscales, depression (DASS-D; low mood and hopelessness), anxiety (DASS-A; physiological arousal and fear), and stress (DASS-S; difficulty relaxing and irritability). Symptoms are rated within the past week from 0 (did not apply to me at all) to 3 (applied to me very much or most of the time). Due to small sample size and to capture the transdiagnostic features of our sample, analyses were limited to only the DASS total score. The DASS total and subscales have demonstrated strong psychometric properties in clinical and non-clinical samples, including internal consistency (Osman et al., 2012), convergent, discriminant (Brown et al., 1997), construct (Henry & Crawford, 2005), and concurrent validity (Antony et al., 1998).
Procedures
Before initiating treatment, clients attended two in-person laboratory assessments, separated by an average of 12 days (range 5–42). On Day 1, participants completed pre-treatment questionnaires, then completed the FC acquisition and extinction training phases, followed by two other tasks not analyzed herein (International Affective Picture System task and paced breathing). On Day 2, participants again completed paced breathing, then the FC extinction recall phase, followed by three tasks not analyzed herein (monetary incentive task, mental arithmetic task, and fear potentiated startle).
Data analysis
To assess effects of the FC task, we used the mixed command in Stata 16 to conduct multilevel modeling. Level one predictors were Stimulus (CS+, CS-) and Trial (1, 2, etc.). For both SCR and US expectancy ratings, we modeled Trial as a continuous variable to assess effects across trials of the task (acquisition, extinction, and extinction recall), allowing for linear and quadratic slopes. Quadratic models included intercept, linear slope, and quadratic slope. Linear models included intercept and linear slope. If the quadratic slope was not significant, it was dropped and linear models were run instead. If the linear slope was not significant, it was dropped and models were run without Trial as a factor. When assessing spontaneous recovery (last trial of extinction to first trial of extinction recall), we ran a linear model because a quadratic model is not possible with only two trials. Treatment condition (PAT, NAT) was also tested in models to assess for any baseline differences across treatment groups in FC task performance and was dropped if not significant.
Changes in DASS over time were analyzed using multilevel growth curve models and run in Stata 16 using the mixed command. Multilevel modeling (MLM) accounts for longitudinal data and allows for examination of within and between subject effects both over time and between treatment conditions. MLMs provide unbiased estimates when data are missing at random. The level one predictor was time (pre-treatment, Sessions 1–15, post-treatment, 6-month follow-up) and the level two predictors were treatment condition (PAT, NAT) and the moderators, including their main effects and interactions. Pre-treatment levels of the outcome were included as covariates to minimize their influence on the outcome measures (Tabachnick & Fidell, 2019). Fear acquisition response was also included as a covariate to control for differences in acquisition of response to the CS’s. Sensitivity analyses showed that results did not significantly differ when acquisition was not included as a covariate. Similar to previous analyses (Craske et al., 2019; Roque et al., 2020), time was natural log-transformed and centered at 6-month follow-up so that the regression coefficient for time reflected the amount of change in the outcome variable per log week. All other variables were grand mean centered so that regression coefficients reflected average effects. Models were fit using restricted maximum likelihood estimation and the Kenward–Roger method was used to estimate degrees of freedom. This approach accounts for the non-independence of individual-level repeated measurements and is recommended for small sample sizes (McNeish, 2017). All models included random effects of intercepts and an autoregressive error covariance structure to account for correlations among residuals. There were a total of 502 data points included in the analyses. Three-way interactions were tested using the following growth curve model:
If three-way interactions were not significant, two-way interactions between Moderator and Time were examined to assess whether FC variables predicted outcomes, regardless of treatment condition. For significant interactions, post-hoc simple slopes were examined to assess group differences.
Post-hoc power analyses were conducted to determine our power to detect significant effects in our actual analyses. We used the program PinT 2.12 (Snijders & Bosker, 1993) to calculate obtained power. PinT uses data on the number of subjects (n = 36), the number of repeated measures (average = 14/participant), the means, variances, and covariances of the predictors, the residual level-1 variance from the model, and the variance and covariances of the random effects to estimate the standard errors of regression coefficients in the models. From these standard errors, power can be estimated (see equation (1), p. 4, of the PinT Users Manual, version 2.1; Bosker et al., 2003). For both SCR as a moderator and for expectancy as a moderator, we determined that we would have ≥.80 power to detect a medium effect size (d = 0.50) for the moderator × week interaction of the moderator x condition × week interactions, and power ≥.80 to detect a medium effect size (d = 0.50) for the level-2 main effect for the moderator. These results are consistent with results from Monte Carlo simulations (Arend & Schäfer, 2019).
Results
Fear conditioning task performance
Results across experimental phases are presented in Tables A1–A3 and Figures 1–2. During acquisition, results showed significant quadratic effects for both SCR (χ2(1) = 19.10, p < .001) and US expectancy (χ2(1) = 35.67, p < .001), linear effects for both SCR (χ2(1) = 22.13, p < .001) and US expectancy (χ2(1) = 55.99, p < .001), and greater responding for CS + trials compared to CS- trials for both SCR (z = 4.70, p < .001) and US expectancy (z = 7.48, p < .001). Additionally, in the quadratic model for SCR, there was a simple interaction between Condition and quadratic slope (χ2(1) = 4.51, p = .034). However, there was no simple interaction between Condition and linear slope (χ2(1) = 3.241, p = .072), which reduces interpretability of the result. Therefore, we ran the linear model and found no significant effects involving Condition (p’s > .220), including no significant Condition by linear slope interaction (χ2(1) = 1.51, p = .220). We can thus conclude that during acquisition, there were no meaningful effects involving Condition. Skin conductance response performance across acquisition, extinction, and extinction recall during fear conditioning. US expectancy performance across acquisition, extinction, and extinction recall during fear conditioning.

During extinction, there were no significant quadratic effects for SCR or US expectancy, so quadratic slopes were dropped from the models. For SCR, there were no significant linear effects. There was no significant main effect of Stimulus (χ2(1) = 0.65, p = .42). Results showed a significant main effect of Trial (z = −2.48, p = .013) with a decrease across extinction. For US expectancy, results showed significant interaction between Stimulus and linear slope (χ2(1) = 6.83, p < .01), with greater decrease for CS + trials compared to CS- trials (z = −2.61, p < .01).
To assess whether effects of extinction persisted, a measure of spontaneous recovery was calculated using the last trial of extinction and first trial of extinction recall. Since only two trials were used, quadratic slopes could not be tested. Results showed a marginally significant interaction between Stimulus and linear slope for SCR (χ2(1) = 3.53, p = .060) and marginally greater increase in responding for CS + trials compared to CS- trials (z = 1.88, p = .060). Additionally, there was a significant interaction between Condition and linear slope (χ2(1) = 5.66, p = .018) with a significantly greater increase for PAT versus NAT. Importantly, there was no significant difference between PAT and NAT at the last trial of extinction (z = −1.26, p = .207) or the first trial of extinction recall (z = 1.67, p = .094). All other effects during acquisition, extinction, and extinction recall involving Condition were not significant (p’s > .072). There was a marginally significant main effect of Stimulus (χ2(1) = 3.37, p = .066) and a significant main effect of Trial (z = 10.10, p < .001). Furthermore, results showed a significant interaction between Stimulus and linear slope for US expectancy (χ2(1) = 43.72, p < .001), as well as greater responding for CS + trials compared to CS- trials (z = 6.61, p < .001).
Moderating effects of fear conditioning (Extinction Recall) on PAT and NAT
Skin conductance
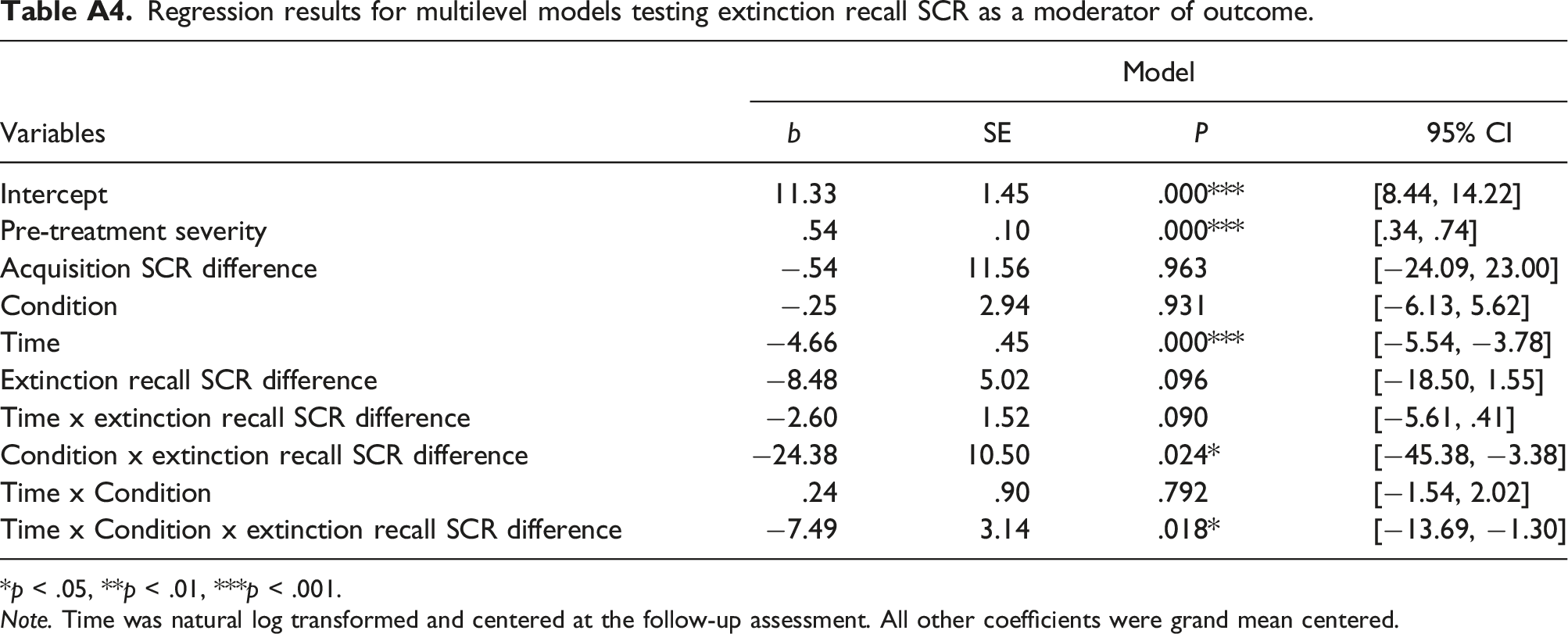
As expected, the pre-treatment SCR measure of extinction recall was a significant moderator of the Condition × Time interaction affecting DASS scores ( Interaction between time, treatment condition, and skin conductance response conditional stimuli difference predicting DASS.
The Time x SCR recall interaction was significant for participants in NAT such that weaker extinction recall was related to faster reductions in DASS scores over time (
US expectancy
Pre-treatment US expectancy during extinction recall was not a significant moderator of treatment condition differences, but did predict improvement over time (Table A5). There was a significant US expectancy × Time interaction ( Interaction between time and US expectancy conditional stimuli difference predicting DASS.
Discussion
The present study explored whether a measure of threat sensitivity moderated treatment response between two treatment conditions for depression and anxiety. We hypothesized that individuals showing greater threat sensitivity, indexed by weaker extinction recall, would benefit more from a treatment that targets threat sensitivity (NAT) than a treatment that targets reward sensitivity (PAT). We found support for our hypotheses, such that individuals with weaker extinction recall (indexed by skin conductance) achieved more rapid symptom reduction in NAT than PAT. Individuals with stronger extinction recall achieved more rapid symptom reduction in PAT than NAT. These findings suggest that a treatment that targets threat sensitivity may be particularly effective for individuals with heightened threat sensitivity, relative to individuals with lowered threat sensitivity. Furthermore, a treatment that targets reward sensitivity may be particularly beneficial for individuals with lowered threat sensitivity.
Larger differences in SCR and US expectancy to the CS + versus the CS- during extinction recall reflect weaker extinction learning (Dibbets et al., 2015; Forcadell et al., 2017; Lissek et al., 2005). Herein, we focused upon extinction recall, given that long-term extinction learning is arguably a more relevant predictor of therapeutic response than short-term extinction training performance, and as such expands upon prior research which has been limited to the latter. We further expand upon prior research by evaluating baseline extinction recall as a moderator of two active treatment conditions. In support of hypotheses, individuals with weaker extinction recall showed more rapid changes in symptoms from NAT than PAT. Furthermore, although not initially hypothesized, individuals with weaker extinction recall achieved faster reductions in symptoms of depression and anxiety during NAT than individuals with average or stronger extinction recall. This finding is inconsistent with prior evidence that superior extinction training is associated with superior response to exposure therapies (Ball et al., 2017; Forcadell et al., 2017; Waters & Pine, 2016), but is consistent with findings from Forcadell et al. (2017) that weaker extinction recall is associated with superior response to exposure. In contrast, level of extinction recall did not predict rate of symptomatic change throughout PAT. These findings suggest that NAT may be most effective for individuals with deficits in long-term extinction learning, relative to individuals with strengths in long-term extinction learning. However, these findings were limited to skin conductance and did not extend to self-report measures of extinction recall (i.e., US expectancy).
We also found that individuals with stronger extinction recall (as measured by SCR) achieved faster reductions in symptoms of depression and anxiety with a treatment that targets positive affect and reward sensitivity compared to a treatment that targets negative affect and threat sensitivity. This finding suggests that PAT may be a more rapid treatment for individuals with strengths in long-term extinction learning. Again, however, the findings did not extend to US expectancy ratings, even though SCR and US expectancy ratings are both presumed to measure associative strength of fear learning and are shown to be positively correlated (Constantinou et al., 2021). The finding that individuals who had stronger long-term extinction in terms of US expectancy achieved faster reductions in depression and anxiety symptoms, regardless of treatment condition, may represent covariation in self-reported threat perception and self-reported symptoms. This may be best explained by the shared self-report methodology of both variables.
Given the limited research on fear conditioning and treatment response, this study served as an exploratory first step. However, several limitations to this study should be noted. First, this was a secondary analysis from an initial trial comparing PAT and NAT, with psychophysiological measures collected partway through the trial. Interpretations of findings are therefore limited by the small sample size and replication in a larger, independent sample is needed to establish reliability and robustness of findings. Relatedly, due to the small sample size, only DASS total scores were analyzed. Follow-up studies with larger samples should also examine DASS subscales. Since this study was conducted within two university psychology departments, results may have limited generalizability and future studies may test the implementation of these interventions in non-academic settings. Finally, the present study assessed a single moderator using pre-treatment timepoints. To address potential interactions among moderator variables, provide more powerful predictions, and increase clinical utility, future studies could implement a multivariate approach with multiple moderators, such as the Personalized Advantage Index (Cohen & DeRubeis, 2018). Some researchers have suggested that fear response during extinction training and recall may be driven by a sense of ambiguity or uncertainty (Bouton, 2002; Morriss et al., 2021). Therefore, future studies may extend this growing body of work by assessing intolerance of uncertainty prior to fear conditioning and examining whether uncertainty emerges as an important predictor of both fear response and treatment outcomes. Future studies may also expand upon these findings by assessing psychophysiological measures throughout treatment. This would allow for tests of mediation and could improve understanding of the mechanisms of PAT and NAT and how threat sensitivity in particular changes over the course of treatment. Finally, given the findings that both PAT and NAT are effective for individuals with depression and anxiety, future studies should examine whether a combination of PAT and NAT is superior to PAT or NAT alone.
In conclusion, our results suggest that individuals with greater threat sensitivity, indexed by weaker extinction recall, may benefit more from a treatment that targets threat sensitivity than a treatment that targets reward sensitivity. Individuals showing the converse may benefit more quickly from a treatment that targets reward sensitivity than threat sensitivity. However, additional work is needed to both replicate findings and further expand our understanding of the mechanisms by which these interventions work.
Footnotes
Acknowledgements
The authors would like to acknowledge the excellent work of the research assistants and therapists on the project.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was in part supported by National Institute of Mental Health (R61MH115138) (MPI Craske, Meuret, Ritz).
Appendix
Results for multilevel models testing effects of the fear conditioning task during acquisition. Significant results in Results for multilevel models testing effects of the fear conditioning task during extinction. Significant results in Results for multilevel models testing effects of the fear conditioning task on spontaneous recovery. Significant results in Regression results for multilevel models testing extinction recall SCR as a moderator of outcome. *p < .05, **p < .01, ***p < .001. Note. Time was natural log transformed and centered at the follow-up assessment. All other coefficients were grand mean centered. Regression results for multilevel models testing extinction recall US expectancy as a moderator of outcome. *p < .05, **p < .01, ***p < .001. Note. Time was natural log transformed and centered at the follow-up assessment. All other coefficients were grand mean centered.
Measure
Model
Simple Effects
χ2
df
p
z
SCR
US expectancy

Measure
Model
Simple Effects
χ2
df
p
z
SCR
Quadratic
0.52
1
.469
Linear
0.68
1
.410
Stimulus
0.65
1
.419
US expectancy
Quadratic
0.01
1
.937

Measure
Model
Simple Effects
χ2
df
p
z
SCR
Linear
3.53
1
.060
CS + vs CS-
.060
1.88
Stimulus
3.37
1
.066
US expectancy
Variables
Model
b
SE
P
95% CI
Intercept
11.33
1.45
.000***
[8.44, 14.22]
Pre-treatment severity
.54
.10
.000***
[.34, .74]
Acquisition SCR difference
−.54
11.56
.963
[−24.09, 23.00]
Condition
−.25
2.94
.931
[−6.13, 5.62]
Time
−4.66
.45
.000***
[−5.54, −3.78]
Extinction recall SCR difference
−8.48
5.02
.096
[−18.50, 1.55]
Time x extinction recall SCR difference
−2.60
1.52
.090
[−5.61, .41]
Condition x extinction recall SCR difference
−24.38
10.50
.024*
[−45.38, −3.38]
Time x Condition
.24
.90
.792
[−1.54, 2.02]
Time x Condition x extinction recall SCR difference
−7.49
3.14
.018*
[−13.69, −1.30]

Variables
Model
b
SE
p
95% CI
Intercept
11.29
1.30
.000***
[8.69, 13.88]
Pre-treatment severity
.60
.09
.000***
[−.84, .30]
Acquisition US expectancy difference
−.27
.28
.339
[−.84, .30]
Condition
.52
2.67
.845
[−4.80, 5.85]
Time
−4.74
.42
.000***
[−5.56, −3.91]
Extinction recall US expectancy difference
2.12
.39
.000***
[1.34, 2.89]
Time x extinction recall US expectancy difference
.58
.12
.000***
[.34, .81]
Condition x extinction recall US expectancy difference
1.52
.77
.052
[−.02, 3.05]
Time x Condition
.51
.85
.549
[−1.16, 2.18]
Time x Condition x extinction recall US expectancy difference
.43
.24
.075
[−.04, .91]