
Abstract
Attachment theory has been used to explain the origin of psychotic phenomena. In this article we critically evaluate dominant models and assessment measures of attachment in the study of psychosis. We identify four problems aligning to current theory and assessment: (1) the reliability and/or validity of assessment tools, (2) the failure of current approaches to differentiate between psychotic and non-psychotic cases within attachment classifications, (3) the absence of an integrated conceptual framework and (4) poor clinical utility. We propose the Dynamic-Maturational Model (DMM) of Attachment and Adaptation as an integrative framework with potential explanatory power to address these problems. The DMM is a model of human adaptation, based in attachment theory and integrative of systems theory, psychodynamic psychology, cognitive neuroscience, ethology and behaviourism. We review the present state of knowledge about attachment and psychosis and consider a broader array of empirical information (e.g. cognitive, affective and somatic) to highlight how future investigations and therapeutic intervention might be reconceptualised advantageously within a DMM framework.
Introduction
There is a well-evidenced association between early childhood adversity and later psychosis (Read, 2005; Varese et al., 2012). Psychotic phenomena are understood to exist on a continuum, with some experiences reaching clinical severity whilst others do not (van Os et al., 2009). Psychotic-like experiences (PLEs) extend into the general population with distress demarcating phenomena of clinical concern (Shevlin et al., 2015). Individuals at clinical high-risk (CHR) are considered to be vulnerable to persistent psychotic experiences and potential psychiatric intervention (Beck et al., 2019). Similar risk factors have been identified above and below clinical thresholds (Rossler et al., 2011) and distinct aetiological pathways have been identified for specific phenomena (Bentall et al., 2014). For example, separate formulations are proposed for paranoia (Freeman & Garety, 2014) and voice hearing (Berry et al., 2017; Longden et al., 2012a, 2012b). There is a likely interplay between genetic and environmental factors in the aetiology and course of psychosis (Brent et al., 2014). Genetic and perinatal distal risk characterised by physiological, neurocognitive and social impairment is theorised to be offset or triggered by psychological mechanisms of resilience such as attachment security (Debbané et al., 2016). Social adversity and attachment-related danger impact on neuronal maturation and functioning, as a precipitant to psychosis (Brent et al., 2014; Read et al., 2014). Attachment theory has been increasingly recognised as a valuable framework through which to understand the development of psychosis (Berry et al., 2008; Carr et al., 2018; Gumley et al., 2014; Korver-Nieberg et al., 2014).
In this paper, we will present an overview of attachment theory as applied to the study of psychosis and consider the current empirical evidence that describes an association. Specifically, we will focus on paranoia and voice hearing as distinct psychotic phenomena. We will highlight important contributions from the field. However, we also note significant flaws in theory, method and assessment that undermine: (1) the reliability and/or validity of assessment, (2) the failure of current approaches to differentiate between psychotic and non-psychotic cases within attachment classifications, (3) the extent to which a formulation framework has been identified and (4) clinical utility. To address these issues, we will propose the Dynamic-Maturational Model (DMM) of Attachment and Adaptation (Crittenden, 2017b) as an alternative framework. We will introduce the core theory before offering an integrative formulation of (1) paranoia and (2) voice hearing. In this endeavour, our goal is to build on existing research and present the DMM as a model of significant theoretical and clinical advancement in the study of attachment and psychosis. We also provide two case study exemplars to demonstrate clinical utility and conclude with suggestions for future research and clinical intervention.
Theoretical Models of Attachment used in the Empirical Study of Psychosis
A contemporary understanding of attachment stems from original work by Bowlby (1969) and Ainsworth (1967) and Ainsworth et al. (1978). Bowlby posited that children possess a biological imperative to form attachment relationships with protective caregivers. He theorised attachment to be underpinned by internal representations of the self, world and other, based on the integration between semantic and episodic memory systems (Bowlby, 1969). It was proposed that Internal Working Models (mental representations of self and other) were foundational for mental and behavioural organisation around relationships with different individuals in different contexts (Bowlby, 1973). It was argued that the development of an attachment bond occurred quickly, by the end of the first year of life, and that this bond was a tie that endured across time and space to protective others whom one turns to at moments of vulnerability (Bowlby, 1969). It was further identified that disruption to the attachment relationship (e.g. separation and loss) could be associated with significant psychopathology (Bowlby, 1973, 1980). This finding has become well-established in subsequent research (Anda et al., 2006; Trotta et al., 2015; Varese et al., 2012).
Ainsworth (1967) and Ainsworth et al. (1978) introduced individual differences and evidenced three patterns of attachment that represented individuals’ unique expectations regarding the availability, attunement and responsivity of specific attachment figures when in need of comfort and/or protection. The Type B pattern represented balanced (secure) information processing and behaviour. Of the ‘insecure’ patterns, Type A reflected avoidant behaviour (e.g. inhibition of attachment signalling) whilst the Type C pattern was characterised by ambivalence (exaggeration of attachment signalling). Ainsworth identified a continuum from inhibition to exaggeration of attachment behaviours under conditions of stress (Figure 1: Howe, 2011). Ainsworth's continuum of attachment behaviours under conditions of stress (from Howe, 2011).
ABCD and Adult Attachment
Certain attachment behaviours do not conform to Ainsworth’s organised ABC patterns. Main and Solomon (1986) theorised that overwhelming fear deactivated the attachment system and precipitated non-strategic approach/avoidance behaviour (Howe, 2011). This was termed ‘disorganisation’ (Main et al., 1985). Frightening occurrences were formulated to disrupt the attachment process in childhood, which led to disorganised attachment and subsequent lack of resolution in adulthood (Main et al., 1985; Main & Goldwyn, 1985; Main & Hesse, 1990). Main’s model used the ABC patterning structure of Ainsworth, with the addition of ‘D’ to represent disorganised attachment. Duschinsky (2020) has noted that Main did not consider disorganisation to be solely caused by fear, nor to be a pattern comparable to ABC. Rather, it was a transient conflict state generated when the individual was motivated both towards and away from their caregiver; in conditions of lower stress, the individual might organise effective attachment patterning (Lyons-Ruth and Spielman, 2004). However, in much of the psychosis literature, disorganisation has been framed as a pattern comparable to ABC (e.g. Pollard et al., 2020).
Bartholomew and Horowitz (1991) proposed a model to explain attachment ‘styles’ in adulthood. Foundational to this theory is the concept of two Internal Working Models, which are developed in early childhood: Internal Working Models of self (self-esteem) and other (sociability). The authors formulated a quadrant (Figure 2) to explain the development of attachment styles on the basis of Internal Working Models and the dichotomy of positive/negative views of self/other. In this model, secure children (Type B) are hypothesised to become secure adults, avoidant children (Type A) become dismissive adults and ambivalent (Type C) children become preoccupied adults. The style ‘fearful-avoidant’ is posited to capture the notion of disorganisation (Bartholomew & Horowitz, 1991; Pietromonaco & Barrett, 1997). The Bartholomew/Horowitz quadrant model is the dominant model used in research that has explored the association between attachment and psychosis. Bartholomew and Horowitz Model of Adult Attachment (from Korver-Nieberg et al. 2014).
Assessment of Attachment
Investigations into the association between attachment and psychosis have used self-report or narrative assessment methods. A brief description of each approach is detailed in the following section.
Self-Report Assessment of Attachment
A wide range of self-report measures have been developed to assess attachment empirically. Self-report tools are used extensively in the study of attachment and psychosis. These measures fall into two categories: scales (e.g. Psychosis Attachment Measure: PAM: Berry et al., 2006; Pollard et al., 2020) and self-selection tasks that require respondents to give their perspective on which of four statements best describes their functioning in a relationship (e.g. the Relationship Questionnaire: RQ: Bartholomew & Horowitz, 1991). Self-report measures align to the Ainsworth patterns or attachment styles approach (Bartholomew & Horowitz, 1991). Researchers who use self-report measures have suggested that they demonstrate adequate reliability and validity in the studied populations (Gumley et al., 2014). However, Olbert and colleagues (2016) have suggested that the PAM had poor construct validity and that ‘attachment measures in psychosis with better psychometric properties are needed’ (p. 77).
Narrative Assessment of Attachment
The narrative approach to assessing attachment is typically organised around the Adult Attachment Interview (AAI: George et al., 1984). The AAI is a semi-structured interview protocol that is used to explore childhood relationships with caregivers, and topics such as loss, separation and rejection (Howe, 2011). The AAI has two analytical methods, with preference given to how the narrative is told, rather than the literal content (Main et al., 2008). This offers a phenomenological advantage over self-report assessment. The Main and Goldwyn approach (1984) uses discourse analysis to determine the integration between semantic and episodic memory, with disparity between the two considered a determinant of insecure attachment. Coherence versus dysfluency is a further indicator (Gumley et al., 2014; Hesse, 2008). The AAI evaluates ‘state of mind’ in relation to attachment. Classifications are made on the basis of how attachment-salient information is organised by the speaker. Speakers are classified as secure-autonomous (F), insecure-dismissing (D) or insecure-preoccupied (E). A classification of unresolved (U) is given to demarcate unresolved trauma that is superimposed over the primary strategy with cannot classify (CC) noted for transcripts that do not fit one of the three primary strategies (Hesse, 2008).
The second approach to interpreting the AAI is the Q-Sort method (Kobak, 1989; Kobak et al., 1993). This method purports to identify primary (attachment activating) and secondary (attachment deactivating) strategies as continuous variables (Dozier & Kobak, 1992). The technique makes use of 100 Q-items that describe aspects of the AAI interviewee’s speech (e.g. information processing, emotion regulation and Internal Working Models), which are coded into hierarchies relevant to the speakers’ coherence and use of ‘secondary strategies’. The method is used to organise individuals on dimensions of secure versus anxious (primary), and then dismissing versus anxious (secondary), or into classifications of secure, dismissing or preoccupied attachment (Hesse, 1999). The Q-sort is reported to hold approximately 80% correspondence to classifications generated on the Main and Goldwyn AAI (Kobak et al., 1993).
ABCD and Adult Attachment: The Association With Psychotic Phenomena
Attachment and Psychosis
Three reviews (Berry et al., 2007; Gumley et al., 2014; Korver-Nieberg et al., 2014) and a meta-analysis (Carr et al., 2018) have been conducted to collate the findings relating to attachment and psychosis. These reviews suggest an association between ‘attachment insecurity’ and psychosis. However, differentiated associations and clinical utility have been hard to establish with the methods of assessment used. Notably, attachment is typically defined as a trait in this literature and not an organising framework.
Some studies have moved beyond secure versus insecure attachment and reported on particular patterns/styles. Avoidant (or dismissing) 1 attachment has been linked to positive psychotic phenomena in clinical (Berry et al., 2007; Kvrgic et al., 2012; Ponizovsky et al., 2007), at-risk (Gajwani et al. (2013) and non-clinical samples (Korver-Nieberg et al., 2014; MacBeth et al., 2008; Pickering et al., 2008). This has been reported in studies using the AAI (Dozier et al., 1990; 1991) and self-report tools, such as the PAM (Berry et al., 2008). However, research has also indicated anxious (or preoccupied) attachment to be associated with psychosis (Berry et al., 2006; Ponizovsky et al., 2007; Strand et al., 2015), with Chatziioannidis et al. (2019) noting that this pattern mediated the relationship between childhood trauma and schizophrenia-spectrum psychosis.
Higher symptom severity and associated psychopathology have been noted in those with reported anxious attachment styles (Carr et al., 2018; Korver-Nieberg et al., 2014; Ponizovsky et al., 2013). Fearful attachment has also been strongly implicated in severe symptomatic expressions (Bucci et al., 2017; Carr et al., 2018; Korver-Nieberg et al., 2014). Carr et al. (2018, p.152) concluded from their meta-analysis ‘the majority of people with psychosis were shown to have a fearful attachment style’.
Attachment and Paranoia
The contribution of attachment to the development of paranoia has been well-explored. Lavin et al. (2020) conducted a systematic review and reported that insecure attachment and paranoia were correlated across the continuum of experience. To offer greater specificity, they concluded that anxious attachment was best correlated with paranoia. This finding has been evidenced in non-clinical (e.g. Strand et al., 2015), first-episode (e.g. Fett et al., 2016) and clinical samples (Castilho et al., 2017). Lavin et al. (2020) also noted that avoidant and fearful attachment styles were associated in the reviewed literature, though with less frequency. Associations have been reported, though these have lost significance when confounders have been measured (e.g. Korver-Nieberg et al., 2015). In studies that have found a relationship (e.g. Dozier & Lee, 1995; Fett et al., 2016), it has been noted that statistical controls for comorbid phenomena were not conducted (Lavin et al,. 2020). Nonetheless, Korver-Nieberg et al. (2013) and Berry et al. (2008) have reported significant associations between attachment avoidance and paranoia in community and clinical samples. The findings of Lavin et al. (2020) were supported by meta-analysis in a subsequent review (Murphy et al., 2020).
Some studies have moved beyond testing associations and explored the role of attachment in relation to childhood trauma and later paranoia. Pearce et al. (2017) reported that dissociation and self-reported fearful attachment mediated the relationship between childhood trauma (measured with a questionnaire) and paranoia, though dismissing and preoccupied attachment did not. Sitko et al. (2014) reported that both avoidant and anxious insecure attachment mediated between childhood experiences of neglect and paranoia. Ponizovsky et al. (2013) reported fearful-avoidant attachment to be associated with paranoia. Affect dysregulation and mentalisation deficits (Osswald, 2010), hypersensitivity to noncontingent behaviour (Fornells-Ambrojo et al., 2016), hyperactivated emotion regulation and bias towards blaming others (Ascone et al., 2020) have also been implicated.
Models of Association Between Attachment and Paranoia
The most frequently presented hypotheses to associate attachment insecurity and paranoia draw upon Bowlby’s (1969) Internal Working Models, as adapted by Bartholomew and Horowitz (1991). This model has been integrated with cognitive models of paranoia (e.g. Freeman et al., 2002). Supposed negative views of self (attachment anxiety) and other (attachment avoidance) have been central to this approach based on the assumption that explicit processing is reliable in this domain. Lavin et al. (2020) suggested that preoccupation/worry, increased negative affect, and interpersonal sensitivity, as aspects of anxious/preoccupied attachment, could precipitate over-attention to threat in the social world, thus culminating in paranoia. This is consistent with the threat-anticipation model (Freeman et al., 2002; Freeman & Garety, 2014). A perception that the self is vulnerable is a reported characteristic of attachment anxiety and a precipitant to paranoia (MacBeth et al., 2008). It is argued that such attachment representations can encompass low self-esteem, which may drive the anticipation of social threat.
Attachment avoidance has been associated with downregulated affect, a negative view of others and social withdrawal (Berry et al., 2007; Ponizovsky et al., 2013). The notion of social withdrawal is important within the context of paranoia, as it is an identified contributor to cognitive models (e.g. Freeman et al., 2002; Freeman & Garety, 2014). For paranoid individuals, social withdrawal may be viewed as a ‘safety behaviour’ (Freeman et al., 2007), which temporarily alleviates discomfort, though prevents the individual from disconfirming negative schema about others over the long-term.
It has been hypothesised that exaggerated anxious and avoidant attachment can result in a self-concept based on vulnerable self and malevolent other (Murphy et al., 2020). It has been suggested that this could represent fearful attachment, with oscillations between anxious approach and avoidance. Fearful attachment has been correlated with paranoia (Lavin et al,. 2020) and other psychopathology (Korver-Nieberg et al., 2015).
Attachment and Voice Hearing
The findings in relation to attachment and voice hearing (auditory hallucinations) are somewhat equivocal. Berry et al. (2008) reported that anxious attachment was associated with voice hearing in a clinical sample, whilst attachment avoidance (Berry et al., 2012; Ponizovsky et al., 2013) has also been implicated. Insecure and/or disorganised attachment has been noted within the context of early life trauma and voice hearing (Bucci et al., 2017; Pilton et al., 2016). Despite these findings, other investigations have reported non-significant associations (Bentall et al., 2012; Wickham et al., 2015) This demonstrates challenges with replication in the field of inquiry.
Models of Association Between Attachment and Voice Hearing
Exposure to danger and subsequent psychological trauma are antecedents to later voice hearing (Cole et al., 2016; Perona-Garcelán et al., 2012; Pilton et al., 2015). Attachment is formulated to mediate between psychological trauma and voice hearing. Dissociation and source monitoring difficulties have been found to be implicated (Berry et al., 2017). Notably, a pathway from childhood sexual abuse to voice hearing has been specifically described (Bentall et al., 2012).
Longden and colleagues (2020) described voice hearing as a dissociative response and trauma-related intrusion, and Berry et al. (2017, p.5) have noted ‘voices can be understood as dissociated components of the self “or compartmentalized” trauma-related memories’. Dissociation is often cited as a feature of psychological trauma (e.g. Van der Kolk, 2014). It is said to be a common sequalae when danger is overwhelming and neither fight nor flight are viable escape options (Schimmenti, 2017). Dissociation has been defined as ‘a disruption and/or discontinuity in the normal integration of consciousness, memory, identity, emotion, perception, body representation, motor control, and behaviour’ (APA, 2013). Dissociation is thought to consist of ‘detachment’ and ‘compartmentalisation’ phenomena. Detachment refers to experiences of derealisation, depersonalisation and detachment from present-moment experience. Compartmentalisation refers to splitting or separation from parts of the self (Holmes et al., 2005). Dissociation is a primitive and adaptive defence, one that has an analgesic effect to protect against pain (Van der Kolk, 2014).
Source monitoring (reality discrimination) deficits such as the misattribution of internal phenomena to external sources are suggested as a possible mechanism that links dissociation and voice hearing. Brookwell et al. (2013) conducted a review and concluded that non-clinical and clinical voice hearers experienced source monitoring difficulties.
Berry et al. (2017) developed the Cognitive Attachment model of Voices (CAV). This model incorporated disorganised (fearful) attachment to complement trauma, dissociation and source monitoring difficulties in the aetiology of voice hearing. Self-reported disorganised and/or fearful attachment have otherwise been linked to trauma and dissociation in previous research (e.g. Ogawa et al., 1997; Sandberg et al., 2010). The CAV outlines a pathway to suggest that experiences of abuse (or subtle yet significant disruptions in the attachment relationship) contribute to the formation of disorganised attachment. The authors argue that this heightens the risk of dissociative responding when confronted by danger. Relatedly, Liotti (2004) considered that the inability to form a coherent response to danger (based on early experiences of frightening parenting) led to attempted coping that failed to integrate memory, consciousness and self-identity. Extrapolated, the inability to access a coherent self-protective strategy could prompt oscillation between ‘fight and flight’, with the outcome ‘freeze’. This could suggest possible overwhelm and a resultant dorsal-vagal shutdown (Porges, 2001). Intrusions of unknown, ‘compartmentalised’ and dissociated experiences into the conscious mind could manifest in voices.
Conceptual and Assessment Limitations
The existing literature has demonstrated that attachment insecurity is associated with paranoia and voice hearing, as distinct psychotic phenomena. However, conceptual and assessment limitations undermine the theoretical and clinical utility of findings. Disorganised attachment is unreliable (Duschinsky & Solomon, 2017; Granqvist et al., 2017) and assessment tools such as the RQ are overly simplistic and prone to conceptual error. There are four key issues: (1) the reliability and/or validity of assessment, (2) the specificity of categorisation and absence of within-classification differentiation, (3) the absence of an integrated formulation of paranoia and voice hearing within a conceptual framework and (4) clear guidelines for therapeutic intervention. In the following section we introduce the DMM and hypothesise how it may resolve the four problems identified above.
Dynamic-Maturational Model (DMM) of Attachment and Adaptation
The DMM is a further development of the work of Bowlby and Ainsworth. However, beyond the normative strategies, there are significant theoretical developments and a departure from the concept of disorganisation. Attachment is defined as: ‘(1) a unique, enduring, and affectively charged relationship (e.g. with one’s mother, with one’s spouse); (2) a strategy for protecting oneself (of which there are three basic strategies, Type A, B and C, as identified by Ainsworth, and many sub-categories, as described by the DMM); and (3) the pattern of information processing that underlies the strategy’ (Crittenden, 2017a, p12). The DMM is based on Bowlby’s original evolutionary foundation, with a focus on adaptation and self-protection in the context of danger (Crittenden, 2017b). Within the DMM, attachment reflects how humans process information regarding the safety of the self in relation to (1) their attachment figure’s ability and availability to protect them and (2) danger. The DMM does not conceptualise security as the optimal strategy; rather, each strategy develops to match the individual’s environment and family context (Farnfield & Stokowy, 2014).
Crittenden extended Bowlby’s use of information-processing theory to incorporate contemporary neuroscience. As such, the DMM incorporates eight memory systems (Figure 3) that relate to three types of information: somatic, cognitive and affective. This represents an advancement on core ABC+D theory, which relies on the integration of only semantic and episodic memory (Crittenden & Landini, 2011). In the DMM, the concept of cognitive and affective processing is most well-defined. Cognitive information has a basis in behaviourism and refers to cognitive contingencies (e.g. cause and effect). Affect relates to how arousal changes in different environments and includes desire for comfort (approach), anger (fight) and fear (flight/freeze). With maturation, around the time of puberty, sexual desire is incorporated. Memory Systems represented in the DMM (from Crittenden & Landini, 2011).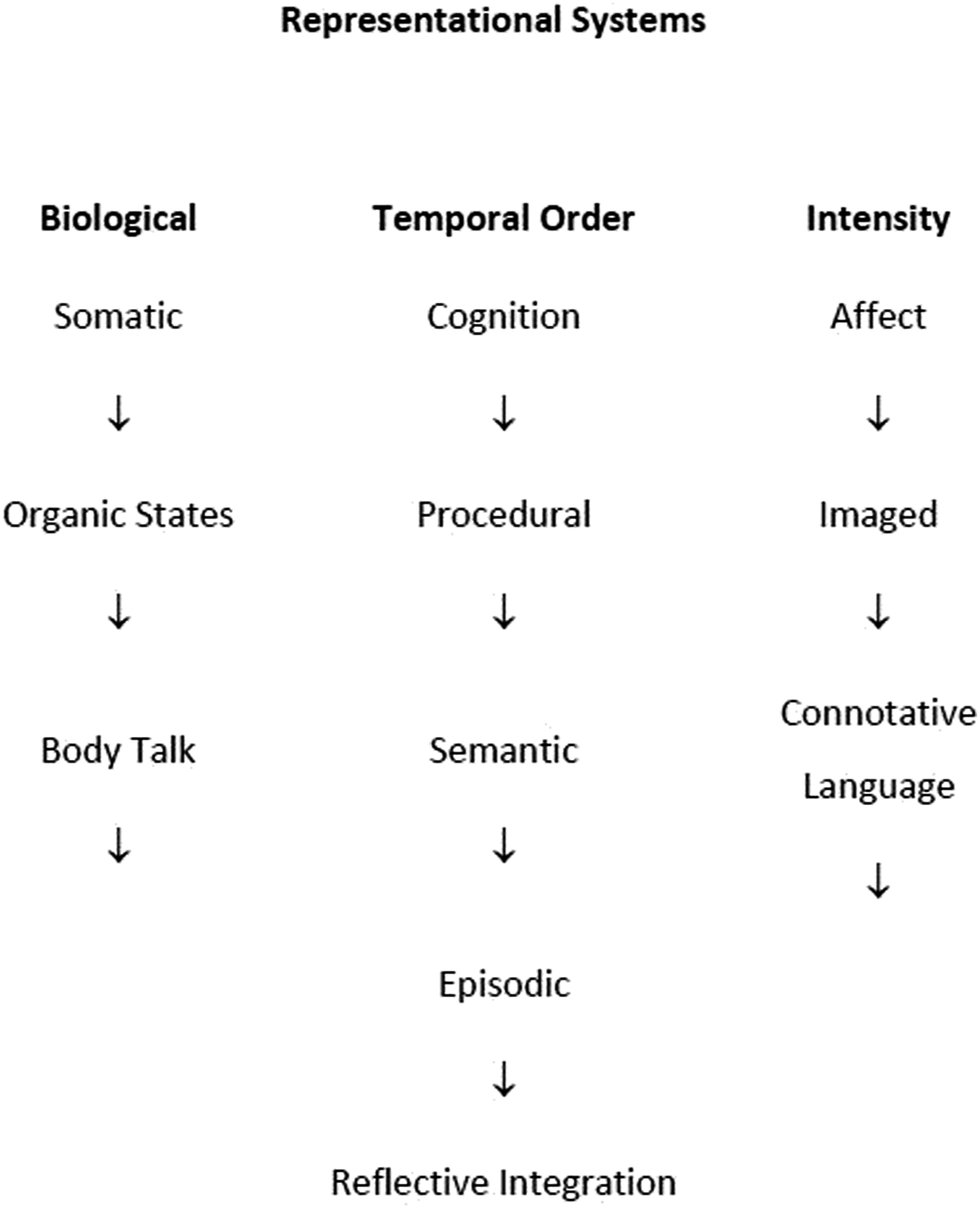
Sensory information contributes to the formation of dispositional representations (Crittenden, 2017b; Damasio, 2000; Devitt et al., 2017), which are conceptualised as dispositions to act in pursuit of self-protection, sexual opportunity, and/or protection of one’s progeny. Developing Bowlby’s Internal Working Model further, the DMM postulates that neuromaturation precipitates the possibility of increasingly complex strategies to adaptively self-protect in environments where danger is present. In response to environmental and parenting cues, different sorts of information about danger are organised as more or less predictive and protective. If, for example, caregivers are unpredictable and variably attuned, the child learns that temporal order contingencies are not predictive of safety (e.g. it is not possible to form the if/then construction of ‘if I cry then my mother will comfort me’), as such contingencies are based upon reinforcement schedules. Consequently, the child implicitly forms Dispositional Representations that prioritise affective information (‘If things feel unsafe, they probably are’) over, poorly predictive, cognitive information. Resolution to competing Dispositional Representations can be achieved by psychological integration, which is a ‘slow’ process. Endangered individuals whose primary concern has been survival are more likely to prefer quicker ways of choosing a Dispositional Representation to motivate protective behaviour. They are less likely to bring the required cortical processing ‘on-line’ to integrate discrepant information (Perry & Szalavitz, 2017; Porges, 2001). Consequently, some individuals more often use associative and dissociative ‘shortcuts’ and may continue to apply this quick way of responding to impending danger even in safer situations, when such processing is not as necessary to ensure safety (Crittenden & Landini, 2011).
Attachment Strategies
DMM attachment strategies are conceptualised as an individual’s best attempt to self-protect within their developmental environmental niche (Figure 4).
2
Within normative samples, the Ainsworth strategies (e.g. B1-4,
3
A1/2 and C1/2: see Figure 1) suffice to ensure protection. However, with greater cognitive maturation, the child, adolescent, then adult has access to a fuller range of complex strategies to protect against danger. As these strategies are not classified within the ABC+D model, individuals using them would be considered disorganised or ‘cannot classify’ using traditional models of attachment. Thus, the DMM can offer greater specificity in endangered samples and within-classification differentiation. Further, the application of Ainsworth’s childhood strategies into adolescence and adulthood without expansion of the range of strategies does not allow for neuromaturation and the consequent complexity of adult information processing and behaviour. Herein, the DMM confers significant advantage over alternative attachment models, particularly in cases where psychopathology is observed. For a comprehensive overview of the DMM strategies, their function and underlying information processing, see Crittenden and Landini (2011), and Farnfield and Stokowy (2014). The Dynamic-Maturational Model of protective strategies. Used with permission of Patricia M. Crittenden.
Type B
The B strategy reflects integration of cognitive and affective information treated as truly predictive (across multiple memory systems), though B1-2 (reserved) are slightly orientated towards cognitive information and B4-5 (reactive) towards affective. Individuals using a naïve B strategy have grown up in environments whereby cognitive and affective information has been reliable in protecting the self from danger and maintaining the availability of the caregiver. Individuals with ‘acquired B’ strategies have reorganised to abandon previous psychological shortcuts and engage into fuller processing of information. For example, a person who used a Type A strategy in childhood might reorganise to Type B when they manage danger using previously inhibited negative affect and also their own perspective, which they had historically disavowed to function in their early relationships.
Type A
Individuals using a Type A strategy give precedence to cognitive information (temporal order reinforcement) over affective information. Type A strategies develop in contexts where danger is predictable, and expressions of negative affect (anger, fear or desire for comfort) are met with mild discouragement (A1-2: inhibited/socially facile), rejection or abuse (A3-8). Affective information is inhibited within normative samples (A1/2) and distorted, falsified (A3/4: compulsive caregiving/compliance), denied (A5/6: compulsive promiscuity/self-reliance) or deluded (A7/8: delusional idealisation/externally assembled self) within endangered individuals. In conditions of greater danger, the individual relies more compulsively on cognitive – to the exclusion of affective – information. For example, an individual using an A4 (compulsive compliance) strategy might be hypervigilant, compliant and habitually ‘well-behaved’ to appease and mollify a hostile parent. They may be unaware of painful affect. Someone using an A6 (compulsive self-reliance) strategy might compulsively maintain a self-reliant ‘stoic’ stance and disavow negative affective states, having learned that close or intimate relationships are painful. Individuals that use a Type A strategy are characterised by a tendency to dismiss the self, idealise/exonerate caregivers and/or partners, and/or deny vulnerable feelings.
Type C
The Type C strategy is the inverse of the Type A strategy. Affective information is given greater emphasis and cognitive information is inhibited from processing and/or transformed. The Type C organisation relies on a split between anger (C1: threatening, C3: aggressive, C5: punitive and C7: menacing) and fear/desire for comfort (C2: disarming, C4: feigned helpless, C6: seductive and C8: paranoid) that are alternated contingently with the changes of other significant persons, in a push-and-pull coercion. This strategy develops when cognitive information has been unreliable; it operates by oscillating between exaggerated push/pull, attack and defence, with cognitive information omitted, falsified, denied or deluded. The individual does not trust the temporal order of events to have protective meaning and instead forms Dispositional Representations that ascribe victim status to the self, with increasing suspiciousness towards others. Functionally, the strategy maintains proximity to caregivers/partners with ever-changing foci to capture their attention and prevent abandonment. With maturation, all individuals develop the capacity to deceive and mentalise (Fonagy et al., 2018); those who use C5-8 strategies make preferential and frequent use of these skills. Strategies that develop in endangered adolescents hide anger and use emotional hooks to achieve retribution and/or rescue. Odd (e.g. C1) and even (e.g. C2) strategies are always used in tandem when they are well adapted to the context, with greater prominence sometimes attributed to the affective display that secures sustained availability from the caregiver.
Alternating and Blended Strategies
Within the DMM, alternating (A/C) and blended (AC) strategies are formulated to develop to meet the adaptive requirements of complicated environments and family contexts. A/C strategies develop due to a necessity to organise strategically to different caregivers or levels of threat, whilst AC is an integrated strategy, though one characterised by increasing levels of transformation (culminating in fully integrated transformed information and the information-processing profile characteristic of psychopathy). In endangered samples, alternating or blended strategies might have some theoretical crossover with notions of fearful-dismissive attachment (e.g. they represent information-processing and behavioural characteristics of the A and C strategies). However, the DMM emphasises that such strategies are organised and adaptive rather than disorganised (Crittenden & Landini, 2011).
Modifiers
DMM strategies are conceptualised to serve an organised and self-protective function. However, Crittenden (1997; 2015) has suggested that when strategies are maladaptive in the current context of use, they are observed as being in modified states. Such modifiers describe ways in which the behaviour and underlying information processing appear non-strategic. If a strategy is applied too pervasively it can become maladaptive in contexts different to the environment within which it first developed. This can heighten the risk of it failing to function effectively and the individual becoming vulnerable to psychopathology. Firstly, reorganisation is a process whereby new integration of previously transformed information occurs, disrupting previous strategic organisations. In the DMM, depression is formulated to occur with the awareness that the self-protective strategy has been non-functional for some time (i.e. the individual has learned that they cannot influence the danger that they experience). Importantly, intrusions of negative affect [ina] and disorientation are of potential relevance to psychosis. [Ina]s occur in individuals using compulsive Type A strategies and can be understood as the intrusion of inhibited or denied affect, such as anger, fear, desire for comfort, and sexual desire that occur when inescapable and unsolvable conflicts occur, and the protective function of their strategy is inactivated. This ‘double-bind’ (Bateson et al., 1956) can give rise to a ‘flood’ of dysregulated behaviour that can appear as a disruption to the individual’s sense of self and family order. This is consistent with psychodynamic theory (Martindale & Summers, 2013) and the Cognitive Attachment model of Voices (Berry et al., 2017). Landini (2021) proposed that an [ina] could indicate that a family is reaching the limit of its functional capacity, and present as a signal for extrafamilial systems to intervene (e.g. via religious ritual or pharmacological intervention, depending on the culture).
The DMM-AAI as an Alternative Method of Assessment
The DMM discourse method utilises a modified AAI with a significantly different coding method to the Main and Goldwyn method. The amendments were designed to capture the experiences of endangered individuals (Crittenden & Landini, 2011; Farnfield, 2008). Additionally, the DMM-AAI probes a wider array of memory systems, consistent with the development of cognitive neurosciences (Figure 2: Damasio, 2000; Devitt et al., 2017). One significant difference between the DMM-AAI and the Main and Goldwyn approach is the coding method. Main and Goldwyn (1985) emphasise the presence of dysfluency as a crucial marker of insecurity, whereas DMM-AAI discourse analysis seeks to identify the self-protective function of transformed information processing (Crittenden & Landini, 2011). Speakers otherwise coded as disorganised or Cannot Classify in the Main and Goldwyn method, are understood to have organised complex and sophisticated strategies to adapt to their environments and family contexts (Baldoni et al., 2018). The DMM-AAI purports to identify such strategies (e.g. A3+ or C3+, as well as alternating, blended and modified strategies). Conversely, the Main and Goldwyn approach offers little to within-classification differentiation (e.g. subtle variations within the A, B or C strategies).
The DMM-AAI has similar validity to the Main and Goldwyn method within normative samples, as the Ainsworth patterns are largely comparable and have the fewest transformations. The DMM-AAI has been shown to have greater validity for at-risk groups (Farnfield et al., 2010), whilst the Main and Goldwyn method has reportedly failed to differentiate between such cases and normative samples (Bakermans-Kranenburg & van IJzendoorn, 2009). Using the Main and Goldwyn approach, secure attachment has been identified in cases of maltreatment, hospitalisation and criminality, with insecure attachment implied in normative samples (Crittenden & Landini, 2011). Baldoni et al. (2018) compared the Main and Goldwyn and DMM-AAI methods and found that they were only convergent in some normative samples. The Main and Goldwyn method identified security in transcripts that the DMM approach coded as non-secure. The authors concluded that ‘the attachment classifications resulting from [Main and Goldwyn and DMM-AAI] should not be considered measurements of the same phenomena’ (p. 1). Pace and Bufford (2018) reported that the DMM-AAI had strong construct validity when tested in the context of psychological treatment status.
There are barriers to using the DMM-AAI clinically and in research. Firstly, whilst the method is conceptually well-formed and fosters good psychometric properties, the training programme is expensive and reliability is ‘rarely achieved within 2 years’ (Farnfield, 2008). Additionally, the interview and coding method are time-consuming to learn (Crittenden & Landini, 2011). Some have opined that the DMM is too complex, difficult to learn and subject to modification based on research (van IJzendoorn et al., 2018). However, Crittenden and Spieker (2018) have noted these features to be strengths of the DMM and necessary for a model capturing the richness of human adaptation. Perhaps due to these restrictions, there is a paucity of large sample studies to investigate the DMM and psychopathology. However, in smaller investigations, promising findings have been reported in relation to a wide range of psychological and psychiatric complaints (e.g. Crittenden & Newman, 2010; Kozlowska et al., 2021; Syrjanen et al., 2018; Zachrisson et al., 2011). Theoretical formulations of numerous clinical presentations have also been posited and require empirical testing. We posit that, compared to the Main and Goldwyn AAI, the DMM-AAI is a superior method of assessment in the study of attachment and psychosis because: (1) it is consistent with the DMM theory of how humans adapt to danger, (2) it addresses concerns about the use of self-report in individuals who have experienced danger as it assesses complexity and implicit processes, (3) it offers greater within-classification specificity than the alternative approaches, (4) it is possible to identify modifiers of relevance to psychosis (e.g. [ina]) and (5) it has clinical utility for informing treatment.
A DMM-Informed Critique of the Present Empirical Evidence
Existing research has established the role of insecure attachment in psychosis. However, attempts to determine specificity, replicability and satisfactory explanatory models are incomplete. Further, clinical implications from this research lack targeted mechanisms for therapeutic change. No study has investigated the association using the DMM-AAI and method of discourse analysis, or conceptualised findings within a DMM framework. Based on the existing research base, the majority of studies have used variations on the Bartholomew and Horowitz (1991) model or Ainsworth categories. Despite it being well-established that individuals with psychosis have often experienced early life dangers, most studies used assessment methods that were designed for normative populations (e.g. primarily self-report questionnaires to assess attachment with a minority using the AAI Main and Goldwyn or Q-Sort methods). We argue that the conceptualisation and methods of assessing attachment have been flawed to date. Conceptually, the best that self-report measures can achieve is perception of attachment style/pattern/strategy based on explicit self-knowledge. Tools such as the RQ cannot be robustly applied to this population and lack validity. Outside of normative samples, adaptation requires that significant cognitive, affective and somatic transformations of information occur. Adaptation to early life adversity demands the development of Dispositional Representations that are further removed from what less endangered individual’s might construe as realistic and attachment strategies are often misunderstood by the individual. There is a significant risk that self-reported strategies are different from (and at times, opposite to) the underlying implicit information processing (e.g. Crittenden, 2017b; Crittenden & Landini, 2011). A failure to account for this when using self-report assessment could explain the disparate and inconsistent findings across studies. There is also a risk that compulsive compliant reporters are classified as secure (e.g. behaviours or attitudes characteristic of the A4 strategy can appear, on the surface, as culturally desirable since the speaker performs well during assessment and appears co-operative). As compulsive strategies (those classified as A3-8) have theoretical relevance to [ina]s and psychosis, misclassification has consequences for the veracity of data. There is sufficient evidence from experimental cognitive psychology to triangulate the position that psychopathology impairs perception of implicit processes (e.g. Kyrios et al., 2015). This is also understood by psychodynamic theorists (Martindale & Summers, 2013). Importantly, contemporary theory from the ABC+D field of attachment has disavowed the disorganised classification as a discernible pattern (Forslund et al., 2021; Granqvist et al., 2017). This is significant as the literature concerning attachment and psychosis has not incorporated these critiques. Rather, the conceptualisation of disorganised/fearful attachment has increasingly been cited in the attachment and psychosis literature (e.g. the PAM has been revised to ‘measure’ disorganisation: Pollard et al., 2020). The alternative notion of functional alternating (A/C) and blended (AC) strategies can be helpful here (Crittenden & Landini, 2011). Further, neurobiological research has developed significantly in the past 40 years (e.g. Damasio, 2000; Debbané et al., 2016; Devitt et al., 2017). The notion of Internal Working Models based on brain functionality at 2 years of age is simplistic. Yet, this is the concept that underpins ABC+D theory as has been applied to psychosis. Developmental models must account for neuronal maturation. Disorganisation can be critiqued and reinterpreted as organised functional adaptation with reference to brain maturation (e.g. maturation allows greater information-processing complexity, as per the DMM). Unresolved loss and trauma can disrupt the functional organisation of the strategy (Crittenden & Heller, 2017; Crittenden & Landini, 2011; Debbané et al., 2016).
Further criticism can be targeted at the conceptualisation of attachment by research psychologists as a variable within a multi-factorial statistical model (e.g. Cassidy & Shaver, 2016). This has been the predominant approach in the literature to date. Attachment is better understood as an adaptive framework that integrates neurobiology, and cognitive, affective, and somatic information (Crittenden & Landini, 2011). Cognitive and affective biases can be understood within attachment strategies (as information processing), as opposed to alongside it. This error is evidenced in attempts to describe linear relationships between attachment, trauma and psychotic phenomena. Attachment represents an individual’s self-protective strategy in the face of danger. Crittenden has defined trauma as the psychological response to a dangerous event that occurs outside of the individual’s zone of proximal development (ZPD) particularly in the absence of comfort and/or protection and limits the ability to make sufficiently accurate predictions about future danger (Crittenden, 1997; Crittenden et al., 2015). Trauma can disrupt the functioning of a self-protective attachment strategy. Further, the existing research implicates attachment strategies/patterns/styles per se. However, little is said about the impact of a failing strategy. A failed Type A or Type C strategy can precipitate psychopathology (Crittenden, 2017b). We understand that psychotic-like phenomena have distinct aetiological pathways (e.g. Bentall et al., 2014) and we propose that psychotic experiences can manifest within attachment strategies and as a consequence of failed strategies.
Theoretical Predictions and Theory-Knitting With the DMM
The DMM is an overarching framework through which to understand human adaptability and psychopathology within the context of danger (Crittenden & Landini, 2011; Crittenden, Landini, & Spieker, 2021). This position is consistent with views held by Bowlby and Ainsworth (Landa & Duschinsky, 2013; Duschinsky & Solomon, 2017). Within this framework, information about danger, safety and sex is processed. Consequently, trauma, dissociation and psychotic phenomena can be explained within attachment theory.
We propose distinct potential pathways to discrete psychotic-like phenomena, above and below clinical thresholds. We argue that ‘simple’ psychosis (and psychotic-like experiences) can be explained via (a) the overwhelm of a compulsive Type A (A3-8) strategy and subsequent [ina]s or (b) within strategy maladaptation (delusional idealisation and themes of protection/rescue at A7/8 or paranoia and fantasies of revenge at C5-8). Severe psychopathology (e.g. schizophrenia) is hypothesised to result from complex and endangering alternating (A/C) organisations in interaction with unresolved trauma and loss. There is a small amount of existing literature to describe psychosis from a DMM perspective (e.g. Crittenden, 2017b). We build on these ideas and offer novel hypotheses, with a focus on paranoid delusions and voice hearing.
Pathway Through Type A Attachment Strategies
We hypothesise that voice hearing is the consequence of a non-functional compulsive Type A strategy (A3-8). When the strategy fails in response to environmental danger, [ina]s may occur and manifest as auditory hallucinations. This would occur when significant affect is transformed, blocked or denied, and danger (trauma) remains unresolved. Dallos et al. (2020) used the DMM and hypothesised that psychosis can manifest when the individual is required to employ incompatible strategies at a point of transition. Within-classification specification is apparent here and the following hypothesis likely relates to A3-8 strategies only. Crittenden (2017b) notes similar processes for psychotic delusions. Delusional beliefs of protection can form at A7/8 (delusional idealisation/externally assembled self) within strategy.
The Type A strategy requires the transformation of affective information when it has historically not been predictive of safety. In dangerous conditions, negative affect may be omitted or denied from processing (Crittenden, 2017b). This is consistent with a psychodynamic formulation of psychosis (Martindale & Summers, 2013) and the Cognitive Attachment model of Voices: voices are understood to be disavowed parts of the self (Berry et al., 2017). Dissociative compartmentalisation occurs as a functional mechanism within the compulsive Type A strategy to omit the perspective of the self and split off affective information that would be dangerous if it motivated behaviour (anger, fear and desire for comfort). A functioning strategy will protect the individual from the harmful consequences of displaying negative affect. However, danger that occurs outside of the zone of proximal development can overwhelm the self-protective capacity and heighten the risk of [ina]s (voices), which would be consistent with recognised post-traumatic experiences (Olff et al., 2005) and dorsal-vagal shutdown (Porges, 2001). Such intrusions could represent a continuum between generalised negative affect and ‘flashback’ phenomena. The depth of dissociated affect could contribute to the severity of the [ina] experience.
Source monitoring deficits are implicated in the development of auditory hallucinations (Brookwell et al., 2013). Dissociated parts of the self can be understood to represent omitted or denied forbidden affect (e.g. anger, fear and desire for comfort). When [ina]s occur, such affect may be experienced as alien to the individual. This is akin to deficits in embodied mentalisation. That is, the ability to recognise and integrate internal states (Debbané et al. (2016); Luyten et al., 2012). We hypothesise that functionally or incidentally such experiences are externalised from the self and may subsequently manifest in the form of voices. The intrusion of anomalous experiences, dissociated alien self and embodied mentalisation deficits could also precipitate delusion in a search for meaning (e.g. Freeman & Garety, 2014) and as a consequence of erroneous information processing (Crittenden, 2017b).
The quality and severity of voice hearing could relate to the robustness of the self-protective strategy. For example, low levels of resilience could result in perpetual minor [ina]s, whereas a psychotic break could occur in otherwise more robust individuals when danger is immediate, unexpected and exceeds the zone of proximal development. Periods of transition are noted risk factors for the onset of psychopathology (Schulenberg et al., 2004). The transition into adulthood is a risk period that requires flexibility in how the adolescent organises to self-protect (e.g. changes in relationships and role can generate conflicting Dispositional Representations that require resolution for successful adaptation). Maladaptive attempts to use pre-existing strategies in new conditions, such as those that could be described as ‘double-binds’ (Bateson et al., 1956), could precipitate a failed strategy and vulnerability to psychosis. Debbané et al. (2016) noted that a combination of neurobiological markers constitute vulnerability to later psychosis. Temperamental variance could explain why some individuals who experience life stressors migrate to clinical disorder, whilst others do not.
For all [ina]s (e.g. voices and delusions), specified dissociated affect could predict how the psychosis manifests. Psychotic content is associated with real-world anxiety and existential threat (Longden et al., 2012a, 2012b) and meaning is drawn from contemporary social events (Cannon & Kramer, 2012). We hypothesise that the omitted affect specific to the individual may predict the emotional quality of psychosis. For example, inhibited desire for comfort may become displaced and result in sexually disinhibited [ina]s (sexual desire becomes relevant in adolescence: Crittenden et al., 2015; Fonagy & Luyten, 2016), whereas forbidden fear may manifest in paranoia. Feelings of guilt and shame associated with inhibited affect could be associated with incidence of ‘bad me’ paranoia (Trower & Chadwick, 1995). These hypotheses require empirical investigation.
The A7 (delusional idealisation) and A8 (externally assembled self) strategies are consistent with a fragmented sense of self and delusions may occur within strategy (Crittenden & Landini, 2011). Functionally, A7 is theorised to occur when a caregiver is the source of danger or fails to protect the child. To maintain an acceptable image of the caregiver, the child omits the negative information from their processing and falsely constructs a preferable reality with delusional idealisation. This is akin to Stockholm Syndrome. Negative aspects of the dyad are owned by the individual with falsely constructed positives ascribed to the other. We hypothesise that danger that extends the strategy beyond the zone of proximal development in adolescence and adulthood will heighten the risk of delusions that have themes of rescue and idealisation. The A8 strategy has its root in institutional and foster care; fragmentation results from the inability to form consistent source memories, with self-narratives formed from professional reports and the perspectives of others. An incoherent sense of self, complete denial of negative affect (to the point of denial of physical pain) and tendency towards dissociative states might heighten the risk of a psychotic break in response to danger. Notably, institutional care is an evidenced risk factor for psychosis (Bentall et al., 2012).
Pathway Through Type C Attachment Strategies
We hypothesise that ‘simple’ psychosis through the Type C pathway could occur within strategy, with paranoia formulated to manifest as an extreme form of a self-protective strategy (Crittenden & Landini, 2011). In the context of deceptive harm, the individual cannot build a cognitive model of safety. Resultantly, undifferentiated high arousal and fear may be experienced pervasively and as trait paranoia. An orientation towards mistrust and suspiciousness could be apparent across the spectrum of Type C strategies. However, psychotic-like paranoia is hypothesised to manifest in Type C strategies that evidence the greatest transformations of information (e.g. C7/8 menacing/paranoid).
The omission of temporal order contingencies is integral to the DMM formulation of strategic (e.g. trait) paranoia. This occurs when the individual denies their causal role to endangering events and the response from others is construed as unwarranted oppression, persecution or conspiracy to heighten protective fear and anger (Crittenden & Landini, 2011). This could suggest ‘poor me’ paranoia at the extreme (Trower & Chadwick, 1995). Evidence from the cognitive literature supports this hypothesis. For example, cognitive biases ‘fill in the gaps’ when cognitive information is discrepant and unpredictive of danger. This is consistent with a tendency to ‘jump to conclusions’ (e.g. Dudley et al., 2016) and demonstrate ‘fast’ heuristic reasoning (Preti & Cella, 2010). Belief inflexibility is repeatedly evidenced in delusional samples (Garety et al., 2005; So et al., 2012). This can have its root in unpredictable environments that prohibit effective evaluation of cause and effect. Historically, deceptive danger is likely to have been a dominant evolutionary condition and there may be adaptive advantage to being on guard for potential threat. Paranoia has been mooted as an adaptive self-protective strategy (Raihani & Bell, 2019).
A failure to effectively formulate ‘cause and effect’ can precede ‘too much’ erroneous information being derived from past experience (Crittenden & Landini, 2011). Here, mentalisation is relevant. Debbané et al. (2016) posit that weak mentalisation and/or inadequate meta-cognition contribute to failed ‘top-down’ regulation of sensory activation in individuals prone to psychosis. The inability to mentalise the mind and behaviour of others as independent of self-interest, as a consequence of deceptive early danger, can render individuals vulnerable to forming trait paranoia. Conversely, the ability to mentalise can enhance resilience in response to neurobiological and developmental risk factors for psychosis (Bartels-Velthuis et al., 2011; Debbané et al., 2013). Mentalisation-based therapy (MBT) has demonstrated positive effects in the treatment of some psychoses (Weijers et al., 2020).
A bias towards affective information is a possible explanation for findings that suggest greater symptom severity in anxious attachment styles (Carr et al., 2018; Korver-Nieberg et al., 2014; Ponizovsky et al., 2013). The Type C strategy is organised to exaggerate affect with the function of preventing abandonment and maintaining presence in the mind of the other. Feigned helpless (C4) and seductive (C6) strategies may rely on exaggerated symptoms to elicit care and protection. It is possible that self-reported symptoms in empirical research reflect (a) greater awareness of affect (in contrast to individuals using an A strategy who minimise, omit or deny affect from their processing) or (b) over-disclosure. Notably, exaggerated symptoms would function well to elicit care in psychiatric services vigilant for psychotic phenomena.
Clinical Utility of a DMM-Informed Approach
A classification of dismissing, preoccupied or fearful attachment offers little to guide therapeutic intervention, nor does it differentiate between clinical and non-clinical cases within classification. A DMM-informed classification and approach to therapeutic intervention could address underlying information processing and non-functional self-protective strategies (Crittenden, 2017b; Crittenden et al., 2021). We now present two illustrative case exemplars, indicative of individuals resident within a medium-secure psychiatric hospital and their context should be considered when determining the functional utility of their self-protective strategy.
The first case describes an adult male with a history of physical abuse, victimisation and homelessness. He had experienced familial disruption, the loss of both parents and times in institutional care. Distressing, hostile voices and transient episodes of mild paranoia were identified, and a diagnosis of paranoid schizophrenia had been made. The psychosis was partially treated with neuroleptic medication. A putative DMM classification identified unresolved trauma in a dismissed form in combination with a formulated A4 (partial A8) strategy. The self-protective strategy did not function effectively and [ina]s were noted to manifest in voices. These intrusions represented blocked (dissociated) anger and fear. 4 This classification offered guidance for a treatment programme. The fundamental focus of therapy would be to support the integration of forbidden and dissociated negative affect and the reorganisation of the self-protective strategy to enhance body/arousal connectivity, enable the development of new Dispositional Representations with greater cognitive/affective balance, and promote the value of his own perspective. Systemic therapeutic approaches (Dallos et al., 2020) and modalities such as Eye Movement Desensitisation and Reprocessing (EMDR: Miller, 2015), psychoanalytic psychotherapy (Martindale & Summers, 2013), compassion-focussed therapy (CFT: Heriot-Maitland et al., 2019) and Radically Open Dialectical Behavioural Therapy (RODBT: Lynch, 2018) would be possible options in this case. Of note, intervention is not designed to eradicate a strategy. Rather, it is to promote the possibility of new, integrative strategies that could offer greater functional and self-protective advantage to the individual.
The second case exemplar describes an adult male given dual-diagnoses of paranoid schizophrenia and dissocial personality disorder. He had witnessed severe domestic violence in childhood, been the victim of sexual abuse and placed into residential care. He experienced persecutory and conspiratorial delusions that became more pervasive and distressing at times of danger. He also heard voices that he attributed to ‘djinn’ and experienced interpersonal dysfunction. A DMM classification identified unresolved trauma in a preoccupied form that related to physical and sexual abuse. A blended strategy suggested oscillation between A6 (compulsive self-reliance and C7/8 (menacing/paranoid). Voices were explained by [ina]s 5 and pervasive paranoia occurred within strategy (C8: paranoid). Distinct psychotic phenomena may co-occur as individuals search for meaning to explain anomalous experiences (e.g. Freeman et al., 2002; Freeman & Garety, 2014). Neuroleptic medication had been prescribed, though this did not resolve the psychosis. However, systemic interventions to secure safety (Dallos et al., 2020), EMDR (Miller et al., 2015) and targeted interventions such as MBT (Weijers et al., 2020), Dialectical Behavioural Therapy (Silva et al., 2021) or meta-cognitive training (Freeman & Garety, 2014) could be effective in a carefully sequenced treatment plan. Sequencing is important to ensure that interventions are offered hierarchically and within the individuals’ zone of proximal development (Perry, 2019).
The clinical application of the DMM could inform differentiated interventions based on a functional understanding of psychotic phenomena. It does not negate the need for psychopharmacology. However, it can provide a framework to identify appropriate therapeutic approaches that draw upon an existing evidence-base.
Directions for New Research
The current research into attachment and psychosis has demonstrated associations and provided a foundation for future investigations. However, the ABC+D and Bartholomew models are poorly supported empirically and fail to explain nuance beyond basic associations. We argue that the DMM is a more appropriate framework for understanding and treating individuals who have experienced danger, and it should now be incorporated into future research investigations. We posit that this can occur in two directions. Firstly, existing cognitive, affective and somatic knowledge of psychosis could be explored using the framework of the DMM. It is our view that this would highlight connections that have not yet been made in the literature (e.g. jumping to conclusion bias as a consequence of transformed cognitive information). This can be completed through review articles conducted by researchers with an understanding of the DMM and psychosis literature. Secondly, well-designed studies that use the Transition to Adulthood Attachment Interview (TAAI: Crittenden, 2005) and DMM-AAI should be commissioned to explore the association in greater depth. Such studies might test the hypotheses we have presented to explain the relationships between distinct psychotic phenomena and specific self-protective strategies, whilst also considering other factors of interest (e.g. relationship with clinicians, treatment outcomes and recovery). We hypothesise that neuroleptic medications likely manage simple Type A psychosis (e.g. the medication may function to bolster inhibition of affect, ‘sealing over’ [ina]s). However, endangered Type A3-8 (e.g. A7/8 delusional idealisation/externally assembled self), Type C, alternating (A/C) and blended (AC) manifestations will represent those often regarded as the ‘treatment resistant group’ due to the continued presence of experienced danger and strategic function of paranoia and delusional beliefs. This requires further study, which may prompt bespoke interventions based on the underlying functions of psychopathology and inclusion of relational and systemic formulations (Crittenden et al., 2021; Dallos et al., 2020). Attachment strategies are tested and can be stretched beyond the zone of proximal development when danger is high. Therefore, consideration of environmental danger that activates the attachment strategy might be an important aspect of treatment planning – ‘change the danger, not the strategy’ (Crittenden, personal correspondence).
We also believe that transitional stages require particular focus. Transitions demand the reorganisation of self-protective strategies. This is a period for potential psychological growth, though also danger. In particular, adolescents face transitional challenges at a time of brain maturation, hormonal changes and fluctuations in self-protective strategy (Crittenden et al., 2014). A failure to adapt to new conditions can precipitate strategy failure and consequent maladaptation (Crittenden & Landini, 2011). Transition into parenthood is also relevant and similar formulations have been applied to explain post-partum psychosis (Crittenden, 2017b). It is also important to establish factors that protect clinical high-risk populations from migration towards clinical disorder. For example, there is some evidence that mentalisation (e.g. Debbané et al., 2016) and reorganisation (Crittenden, 2017b) can offset risk at this life-stage. Meta-cognitive training (Freeman & Garety, 2014) might be relevant for some, and family level and systemic interventions are also likely to be important.
Further work is required in the assessment of attachment. Self-report measures are time-efficient, easily administered and allow large collections of data to be made (Demetriou et al., 2014). However, their application to endangered populations is conceptually flawed. We note that the complexity and arduousness of the DMM-AAI method are prohibitive. We also encourage (a) DMM-AAI training for researchers and (b) investment in the development of proxy assessment and algorithmic aids to the process.
We recognise that organic, drug-induced and other manifestations of psychosis might fall outside of this approach. Our aim in this paper has been deliberately narrow. We have sought to offer a framework to describe the psychological and environmental aetiology of paranoia and voice hearing. Future work is required to explore other psychotic phenomena. We have not fully incorporated contemporary ideas from neuroscience, though we believe arguments presented by Debbané et al. (2016) are complementary to our ideas. Therein, the authors also outline neurobiological mechanisms that suggest why some individuals might migrate to full psychotic disorder, whilst psychotic-like phenomena might dissipate for others.
Conclusion
Crittenden (2017a) quoted John Bowlby as saying, ‘we know more and more about less and less’ and explained that he was speaking about a tendency to see attachment as a variable without deeply understanding the concept. Cassidy and Shaver (2016) have identified that there are many thousands of studies guilty of this charge. We argue that attachment is a deeply complex concept and cannot be captured by simplistic questionnaires or reduced to a variable in a multi-factorial statistical model. Furthermore, the notion of disorganisation has somewhat collapsed empirically (Granqvist et al., 2017) and is misused in the psychosis literature. We identified four key problems within the existing research: (1) the reliability and/or validity of assessment, (2) a lack of specificity and absence of within-classification differentiation, (3) the absence of an integrated formulation framework and (4) inadequate clinical utility of findings. The DMM can address these concerns and offer an alternative and unifying framework through which to understand human adaptation, particularly psychopathology. It can place psychosis within the spectrum of human experience and not as a distinct phenomenon or disease. It is cited in the Power Threat Meaning framework (Johnstone & Boyle, 2018) and there is a theoretical, empirical and clinical rationale to explore its explanatory power further. In this paper, we have attempted to present evidence to support a shift in focus from ABC+D to the DMM. However, we note that much theory and knowledge has been omitted. To specialists in the field of psychosis, we propose the DMM as a new framework, to be explored, integrated and developed.
Footnotes
Acknowledgements
We would like to thank Clark Baim, Ben Grey and Andrea Landini for reviewing versions of this manuscript. Their comments and insights have improved our work significantly.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.