
Abstract
Impairments in executive attention control, such as the ability to inhibit processing task-irrelevant information, are believed to play a key role in the development and maintenance of social fear and anxiety. However, the underlying attentional mechanisms related to social anxiety are not well understood. The aim of the present study was to investigate associations between actual and perceived executive attention control deficits and social anxiety symptoms in children. Participants included 134 school children drawn from the community between the ages of 8–13 years. Children completed the Attention Network Task (ANT) along with self-report measures of executive attention control and social anxiety. The ANT is a reaction-based task that assesses alerting, orienting, and control of executive attention. Results showed that only self-reported executive attention control was negatively associated with heightened levels of social anxiety. Also, objectively and subjectively measured executive attention control were not related to each other. Findings suggest that social anxiety may only be associated with perceived deficits and not with an actual impairment of executive attention control. Further studies are needed to examine the role of actual versus perceived deficits in childhood social anxiety.
Introduction
The primary aim of the present study was to investigate the role of executive attention control in children with heightened levels of social anxiety symptoms. Specifically, the study assessed whether social anxiety levels in children were associated with (1) actual performance in an objectively measured executive attention control task, (2) perception of performance on the task, and (3) a subjective measure of executive attention control. A secondary aim of the present study was to examine the unique contribution of the different executive attention control types to predict social anxiety. We chose to study social anxiety for several reasons. First, social anxiety is highly prevalent in typically developing children, with a peak onset in early adolescence (Kessler et al., 2005). Second, childhood social anxiety disorder is associated with lower well-being and social functioning (Cillessen & Mayeux, 2004), including impairments in education and early dropout (Stein & Kean, 2000). Knowing more about the underlying attentional mechanisms that drive social anxiety is important to direct interventions to help overcome social anxiety. Specifically, objective versus subjective evaluations of social or performance situations might help us to understand whether children with social anxiety show actual or perceived deficits in attention.
Executive attention control is a heterogeneous concept which can be challenging to define. It includes the abilities to inhibit processing of task-irrelevant information, to focus on relevant information, and to shift attention when necessary. According to Attentional Control Theory, executive attention control is impaired in children with heightened levels of anxiety (Eysenck & Derakshan, 2011; Eysenck et al., 2007). Anxiety-prone children with poorer executive attention control are thought to have greater difficulties in inhibiting negative thoughts and regulating emotional responses, relative to those with better executive attention control (Rueda et al., 2004). This impairment in executive attention control is purported to explain greater levels of attentional bias for emotional stimuli in adults and children with high levels of anxiety (Eysenck et al., 2007). Attentional bias is the allocation of processing resources to certain stimuli or aspects of the environment, generally at the expense of processing other concurrent stimuli or aspects. Empirical findings support this notion in adults (e.g., Reinholdt-Dunne, 2009) as well as in children with varying levels of anxiety (Muris et al., 2008). Executive attention control dysfunction in children with high levels of social anxiety is thought to be due to prolonged processing of information related to worry and rumination about social situations and the self (Brozovich & Heimberg, 2008; Heimberg et al., 2014). However, research has yet to determine the specific role that executive attention control mechanisms play in childhood social anxiety.
To date, only a few studies have investigated the relation between executive attention control and social anxiety. These studies found support for an association between impaired executive attention control and higher levels of social anxiety, in both adults (e.g., Moriya & Tanno, 2008; Morrison & Heimberg, 2013; Taylor et al., 2016) and youth (Pergamin-Hight et al., 2016). However, all four studies are greatly limited by only using a self-report measure of executive attention control. The participants were asked to self-report about their own executive attention control, and no objective measurement or an external view on their executive attention control was administered. This is unfortunate, especially in studying social anxiety, as socially anxious children fear social and performance situations and evaluate themselves as being less capable than their peers. Indeed, several studies suggest that children with social anxiety might partly underestimate their social and performance skills (see also Miers et al., 2011), and some studies even found no significant relation between social anxiety and performance skills deficits (Baartmans et al., 2019). To the best of our knowledge, only one study in adults, and none in children, has examined executive attention control and social anxiety using an objective measure of executive attention control. Morrison et al. (2016) used an attentional blink paradigm (Martens & Wyble, 2010) in 166 patients with social anxiety disorder and a group of 37 healthy controls. Interestingly, their findings showed that only patients with comorbid depression exhibited impaired executive attention control abilities. Their study, however, was limited by unequal sample sizes, and further investigations are needed. Some studies have examined the role of executive attention control in socially anxious adults under high and low perceptual load, using an experimental measure of executive attention control (Moriya & Tanno, 2010, 2011). However, provided that perceptual load is purported to modulate early pre-processing at involuntary levels of executive attention control (Berggren & Derakshan, 2013), these findings may not be related to the focus of the present paper. The current study examines executive attention control at the cognitive voluntary level of processing and not at the pre-conscious level of awareness. The role that executive attention control impairment may play in social anxiety is thus an area relatively unexplored using objectively measured executive attention control in both adults and children, and it highlights the need for further investigation.
In the current study, we investigated the relation between social anxiety and executive attention control, while focusing on subjective versus objective executive attention. We also tested which aspects of executive attention control would best predict social anxiety: objective executive attention control, subjective perceived attention control, and/or the evaluation of one’s own performance on the objective control task. Executive attention control was measured objectively with the Attention Network Task (ANT; Fan et al., 2002) and subjectively with the Attentional Control Scale (ACS; Derryberry & Reed, 2002) in children aged 8–13. The ANT is a non-stressful computer task of approximately 10 minutes that uses reaction times to assess alerting, orienting, and control of executive attention.
Based on studies investigating executive attention control and social anxiety using self-report methodology (e.g., Pergamin-Hight et al., 2016), we hypothesized to find negative correlations between the levels of social anxiety and performance on the ANT, self-reported executive attention control, and evaluation of the performance on the ANT. In addition, we expected that performance on the Attention Network Task would be positively related to self-reported executive attention control scores. Regarding our secondary aim, given the nature of social anxiety, we would expect that social anxiety was best predicted by the three variables in combination (i.e., objective ANT performance, subjective self-reported attention control, and evaluation of the ANT performance). To summarize, high levels of social anxiety are hypothesized to be related to (1) lower levels of objective attention control, (2) underestimation of performance, and (3) lower levels of self-reported perceived attention control, which should all explain unique variance, and thus distinct aspects, of social anxiety (see also Baartmans et al., 2019, 2020).
Methods
Participants
This study was part of a large community-based project about both childhood social anxiety and spider fear, for which an unselected sample of children was recruited from regular elementary schools in the Netherlands. After parental active written consent had been granted, a total of 718 children took part in the screening phase of the study. Because we were unable to test all children individually using the experimental procedure, children filled in the social anxiety subscale of the Screen for Child Anxiety Related Emotional Disorders (SCARED; Bodden et al., 2009). In addition, as part of the larger project, children also filled in the Spider Anxiety and Disgust Screening for Children (SADS-C) to assess their levels of spider fear (Klein, van Niekerk, Baartmans et al., 2017). In total, 141 children (101 girls; 72%) between 8 and 13 years of age (M = 10.0, SD = 1.1) were selected, such that (1) levels of social anxiety and spider fear were approximately normally distributed, and (2) approximately the same number of girls/boys scored in the lower and higher regions of self-reported anxiety. Due to incomplete data sets, the data of seven participants were excluded (ANT missing: n = 4; ACS missing: n = 2; ANT-question missing: n = 1). As a result, the data of 134 children (95 girls; 70.9%) between 8 and 13 years of age were included in the analyses. This sample size yields very good power (1-ß = .96) to detect medium-sized values (r = .30) of the correlations of interest (see below), with p = .05, one-sided. The conventional power of 1-ß = .80 is reached for small-to-medium correlations of r = .21 (with p = .05, one-sided). The current sample partly overlapped with three other studies that focused on the specificity of interpretation biases (Klein et al., 2018), on biases in spider fear (Klein, van Niekerk, ten Brink et al., 2017), and on the relation between state and trait anxiety (van Niekerk et al., 2017). The Ethical Committee of the Social Sciences department of Radboud University, The Netherlands, approved this study.
Materials
Attention network task
The ANT assesses alerting, orienting, and control of executive attention, derived from manual reaction times (RTs) to target arrows (Fan et al., 2002). The current paper focuses solely on the executive attention control component of the task to keep a narrow perspective on the possible associations between constructs. Each trial of the task began with a warning display, where the warning cue was an asterisk (none, one, or two). The response frame display comprised a target arrow and four flankers, which were either four arrows or four lines. There were two flankers on each side of the target arrow. The stimuli were presented in black on a white background. Each line or arrow was 20 mm, and the contours of adjacent arrows or lines were separated by 10 mm. The row of stimuli (i.e., a target and four flankers) was 14 cm in length. The warning cue, target, and flankers were presented either 3 cm above or below the central fixation point. The task comprised 24 practice trials followed by 96 experimental trials.
The ANT required participants to indicate whether a central arrow pointed left or right. Feedback (a beep which sounded if participants made an error) was given on practice, but not experimental, trials. The trials reflected the combination of the following conditions: warning cue (4: no cue, center cue, double cue, or spatial cue), target-arrow location (2: top or bottom), target-arrow direction (left or right), flanker (3: neutral, congruent, or incongruent). There were four repetitions of each trial type. The experimental trials were presented in a randomized order and took approximately 10 minutes to complete.
Each trial consisted of five events. First, there was a centrally located fixation cross which remained on the screen during the whole trial, except when being replaced by a center cue. After a random interval (between 400 and 1600 ms), the warning condition was presented for 100 ms, which was either; (1) no warning cue, participants only saw the fixation cross for 100 ms, (2) single center cue, (3) double cue, with one cue above and one below the fixation cross, or (4) single spatial cue, one cue either above or below the fixation cross in the position of the following target. Next, the centrally located fixation cross was presented alone again for 400 ms, followed by the simultaneous appearance of five stimuli (target and four flankers) either above or below the central fixation cross. The target was a central arrow. The flankers (two on each side of the target) were either arrows or lines, which determined the three flanker conditions: (1) neutral, where the flankers were lines (e.g., – – ← – –), (2) congruent, where the flankers were arrows pointing in the same direction as the central target arrow (e.g., ← ← ← ← ←), or (3) incongruent, where the flankers were arrows pointing in the opposite direction of the target arrow (e.g., → → ← → →). The target and flankers were presented until the participant made a response, or a maximum duration of 1700 ms. Participants were asked to indicate the direction of the center arrow (i.e., whether it was pointing left or right) and press the appropriate key on the button box as quickly and accurately as possible. The button-box used in the current experiment was designed and built by the Technical Support Group of Radboud University and had a time accurate (1 ms) button press registration. After the response, the central fixation cross was displayed for a variable duration, such that the interval between target onset on one trial and warning cue onset on the next trial was 3500 ms. (see Figure 1). Sample stimuli and schematic of types of trials.
RT outliers (<200 ms and >3 SDs above each participant’s mean) were excluded. Executive attention control was then calculated by subtracting the mean RT of incongruent flanker trials (flanker arrows point in different direction from target arrow) from congruent trials (flanker arrows point in the same direction as target arrow). Thus, less negative values reflect better executive attention control. This score is the opposite of the attention conflict score calculated by Fan et al. (2002), but is more convenient here in order to allow comparison with the self-report executive attention control measures. Trials with incorrect responses were excluded from the computed scores.
Attention network task-question
After completion of the ANT, the children answered the question “How do you think you did?”. The question was rated on a 7-point scale with “very bad,” “bad,” “alright,” “average,” “quite good,” “good,” and “very good”.
Executive attention control scale for children
The ACS is a 20-item self-report questionnaire measuring the ability to focus and shift attention if necessary (e.g., ‘‘When concentrating, I do not notice what happens around me’’, ‘‘I can easily write or read, while I am talking on the phone’’) (Derryberry & Reed, 2002). Items were scored on a 4-point scale with 0 = never, 1 = sometimes, 2 = often, and 3 = always. After recoding inversely formulated items, a total score can be computed by summing up relevant items. In all cases, higher scores reflect higher levels of executive attention control. In this study, internal consistency was satisfactory (α = .84).
Social anxiety scale for children
The SASC-R is a self-report questionnaire that measures responses to 18 descriptive self-statements reflecting activity preferences (“I like to read”) or social preferences (“I like to play with other kids”) (La Greca & Stone, 1993). Each item is rated on a 5-point scale according to how much the item “is true for you” (1 = not at all, 5 = all the time). In this study, internal consistency was excellent (α = .96). The clinical cutoff scores on the SASC-R are based on samples of schoolchildren, and subsequent work has provided support for the cutoffs (see La Greca, 1998). The cutoff for high social anxiety on the SASC-R is a total score at or above 54 for girls and 50 for boys. Low social anxiety is defined as a total score at or below 40 for girls and 36 for boys (La Greca, 1998; Silverman & La Greca, 1992). In the current sample, 51 girls scored below the lower cutoff, 26 girls scored above the upper cutoff, and 18 girls scored between the cutoffs. For boys, the corresponding numbers were 17, 15, and 7, respectively.
Procedure
The children participated in a session of 1 h. They performed the ANT individually in a quiet room at the school during school hours. Windows in the room were taped with black paper and lights were dimmed, in order to create a standardized testing environment. A trained master student administered the task. Directly after completion of the ANT, the children answered the question “How do you think you did?”. At the end of the session, the children filled out the SASC-R and the ACS. We chose this order because of the necessity to measure reliable reaction times during the ANT, given a limited attention span in children.
Statistical analysis
To investigate the relation between social anxiety and executive attention control, we conducted partial correlations (controlled for age and gender) between SASC-R scores, ACS scores, ANT performance scores, and ANT-question scores. To predict social anxiety, we used hierarchical regression analysis with SASC-R scores as the dependent variable. ACS scores, ANT performance scores, and ANT question scores were used as predictors.
Results
Relations with age and gender
Descriptive statistics for age, error rates, missing values, SASC-R, ACS, ANT, and ANT-question (n = 134).

Note. SASC-R: Social Anxiety Scale for Children; ACS: Attentional Control Scale; ANT: Attention Network Task, ANT-question: “How do you think you did?”, which is the question that is asked to the participants following the ANT paradigm.
Relations between social anxiety and executive attention control
Hierarchical regression analysis predicting SASC-R scores from age, gender, ACS scores, ANT scores, and ANT-question scores (n = 134).
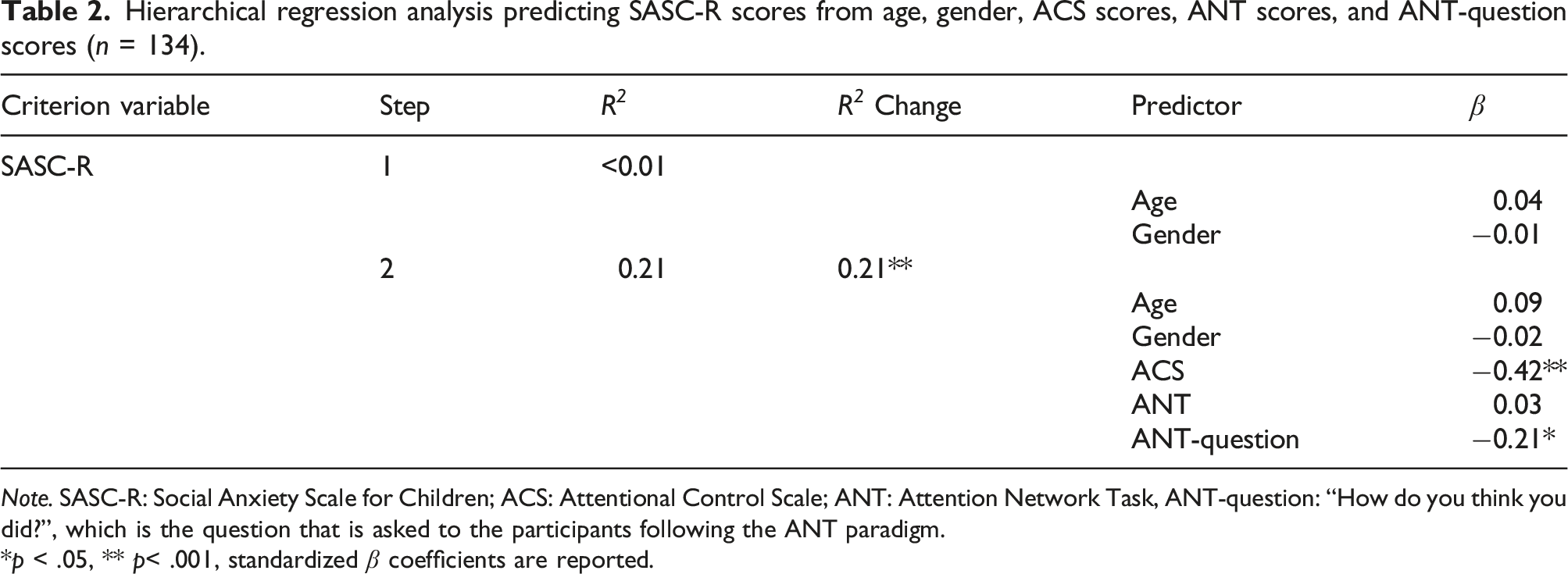
Note. SASC-R: Social Anxiety Scale for Children; ACS: Attentional Control Scale; ANT: Attention Network Task, ANT-question: “How do you think you did?”, which is the question that is asked to the participants following the ANT paradigm.
*p < .05, ** p< .001, standardized β coefficients are reported.
Prediction of social anxiety
In order to test our hypothesis that the different measures of executive attention control would all have a unique contribution to social anxiety, we used hierarchical regression analysis with SASC-R scores as the dependent variable. ACS scores, ANT performance scores, and ANT-question scores were used as predictors. We also included age and gender in step 1 of the regression, in order to control for these variables. In step 2, we included the ACS scores, the ANT performance scores, and the ANT-question scores.
The model with only age and gender did not reach significance F (2,131) = .13, p = .878. After the second step, the model was significant F (5,128) = 7.90, p < .001, and it explained 21% of the variance in SASC-R scores. For this second regression, ACS scores (β = −.42, p < .001) and ANT-question scores (β = −.21, p = .011) were significant predictors. Lower ACS scores and ANT-question scores both predicted higher SASC-R scores. Thus, self-reported executive attention control and the self-reported estimation of performance on the ANT each predicted unique variance components of social anxiety measured by the SASC-R, but the actual performance on the ANT did not (β = .03, p = .750) (see Table 2).
Discussion
According to the Attentional Control Theory, higher levels of anxiety are associated with lower levels of executive attention control (Eysenck & Derakshan, 2011; Eysenck et al., 2007). The goal of the current study was to investigate the role of executive attention control in children with varying levels of social anxiety symptoms. Results with regard to our first hypothesis indicated only partial support for an association between poorer executive attention control and higher social anxiety levels. Self-reported executive attention control (measured with the ACS) was associated with higher levels of social anxiety. However, the experimental objective measure of executive attention control (measured with the ANT) was not related to self-reported social anxiety levels. These findings are similar to findings from the adult (e.g., Moriya & Tanno, 2008; Morrison & Heimberg, 2013; Taylor et al., 2016) and child literature using self-report measures of executive attention control (Pergamin-Hight et al., 2016). In addition, this finding supports the findings by Morrison et al. (2016) that objectively measured executive attention control is not related to social anxiety. One might be tempted to attribute this lack of relations to insufficient reliability of the ANT scores. However, the reliability was actually quite good for a reaction time task, and sufficient for a correlation with age. Taken together, the data of our study in children and the study by Morrison and colleagues (2016) in adults indicate a likely continuity across age in the relation between self-reported, but not experimentally tested, executive attention control and social anxiety symptoms. It may be that patterns of self-reported executive attention control associated with emotional states are established at a relatively early age, and continue into adulthood.
These findings do, however, pose the question whether the executive attention control impairment in social anxiety is an actual deficit or just a perceived deficit. The question, “How do you think you did?”, was related to social anxiety in that lower perception of performance was associated with higher levels of self-reported social anxiety. Moreover, in answer to our second hypothesis, both the self-perceived executive attention control and the subjective evaluation of the ANT predicted unique variance in social anxiety, but not the actual performance on the ANT. This suggests that social anxiety may bias different aspects of the perception of overall performance (both the evaluation of performance and perceived executive attention control). This might indicate that social anxiety is related to a perceived deficit in executive attention control, and not necessarily to a real impairment in executive attention control. Alternatively, this could also be explained by heightened levels of fear of negative evaluation and/or performance anxiety in children with high levels of social anxiety. Clearly more research is needed to test this hypothesis before firm conclusions can be drawn.
Besides the unique relation of social anxiety and the different measures of subjective executive attention control, we also examined the relationship between self-reported executive attention control and experimentally measured executive attention control. The results showed no significant relationship between the two measures. This finding may seem surprising, however, it is similar to previous studies in adults (Reinholdt-Dunne et al., 2013) and children (Muris et al., 2008). Both studies examined self-reported executive attention control and experimentally measured executive attention control in relation to broader levels of psychopathology (i.e., general levels of anxiety, depression, and aggression). These studies highlight the discrepancy between self-report and objectively measured executive attention control in general. Several explanations may be given for this low overlap between self-reported and experimentally measures attention control. First, the fact that the reliability of the ANT scores was lower than the reliability of the questionnaires may have contributed to low correlations of the ANT scores with other variables, but it can hardly explain the total lack of correlations observed here. Second, a more likely explanation states that self-reported attention control measures a different construct than experimentally measured executive control. Self-reports might measure the subjective belief of being able to control attention (see also Muris et al., 2008). Third, it might be that attention control is more complicated, and cannot be measured with a single experimental paradigm. In the future, it may be useful to use tests of executive attention control that address specific components such as the abilities to inhibit, to focusing, or to shift attention. Additionally, future studies could, for example, combine the ANT with other measures such as the Test of Everyday Attention for Children (Teach-Ch; Manly et al., 2001) that was used in the study by Muris et al. (2008). In sum, clearly more research is needed that includes both self-reports and experimental measures. Furthermore, the findings stress the importance of using multiple measures of cognitive control, instead of only relying on either self-reported attention control or a single experimental measure of it.
The current results were observed in children with varying, non-clinical levels of social anxiety. If replicated in children with clinical levels of social anxiety, the findings from the present study, that is, that executive attention control deficits may be perceived rather than real, may be relevant for the development of interventions for social anxiety. Even though clearly more research is needed, our results suggest that treatments may benefit from focusing on perceived deficits, in addition to training actual deficits.
Of course, the present study is not without limitations. First, our sample partly overlapped with samples of previous studies, and it was a selected, but non-clinical sample. Clearly, further research is needed in order to determine if similar findings, for instance, the relation between executive attention control and levels of social anxiety, are also present in children with clinical levels of social anxiety. Some of the literature referred to in the introduction (e.g., Martens & Wyble, 2010; Morrison et al., 2016) is based on clinical samples, which poses a limitation when comparing the findings of these studies to the ones of the current study.
Second, the focus of this paper has been on executive attention control measured with neutral stimuli. Therefore, the findings cannot be compared to results from tasks using emotional materials, such as, for instance, the emotional Stroop paradigm (Williams et al., 1996). This is an important distinction because tasks with emotional materials assess so-called cognitive biases, that is, the preferred processing of some stimuli (usually disorder-related ones) over others (usually neutral ones). In contrast, tasks employing neutral materials like the one used here assess general processing deficits. This difference may be particularly relevant in social anxiety, as it has been related to both cognitive biases and cognitive deficits. Therefore, it would be important for future research and our current theoretical models of social anxiety to investigate this further by including both types of tasks in the same study. This will also have consequences for potential treatments: Depending on whether cognitive biases, cognitive deficits, or self-perceived deficits are most prominent in childhood social anxiety, one or the other approach should be most beneficial.
Third, our findings are limited to social anxiety, and additional research is needed before any conclusions can be drawn about other aspects of anxiety or to any anxiety disorder. Fourth, the ANT task is a very specific task for measuring executive attention control, and other tasks or parent/teacher reports may have higher ecological validity of the executive attention control ability in daily life and the impact of that on daily functioning. Before firm conclusions can be drawn, clearly more studies are needed that use varying experimental measures and observers, such as parents or teachers, besides self-reports and the ANT. Fifth, our study has a narrow focus on the executive attention control of the ANT. Future studies may wish to broaden the scope to also include the orienting and alerting measure of the ANT. Finally, the time of assessment was not standardized and not assessed. Preferably, we would have wanted to test early in the morning for all children. Unfortunately, this was not possible due to time restrictions and practical reasons for the schools we worked with. Variance in attention span could have influenced the reaction times on the ANT.
In conclusion, the present study was the first to investigate objectively measured executive attention control with non-emotional words in relation to social anxiety in children. Findings did not support theoretical notions that there is an actual impairment in executive attention control in social anxiety. Given that our results are similar to empirical findings from the adult literature, it supports the hypothesis that in social anxiety, executive attention control deficits for non-emotional stimuli are perceived rather than actual. This finding is important because innovative treatments of social anxiety disorder in both children and adults are using various ways of training information processing biases as a means of reducing social anxiety symptoms. Knowledge from this study may help researchers better understand the underlying attentional mechanisms present in childhood social anxiety. Even though clearly more studies are needed on the relation between subjectively and objectively measured executive attention control in clinical samples before any firm conclusions can be drawn, our results underscore the importance of studying executive attention control in more detail, using multiple measures of executive attention control when investigating this construct in relation to childhood social anxiety.
Footnotes
Acknowledgments
We thank the elementary schools, the children, and their parents for participating in the study and the reviewers for helpful comments on an earlier version of this paper. We also thank Rianne van Niekerk, Emmelie Flokstra, and Rian Bakens for their assistance with data collection. The Behavioural Science Institute of Radboud University Nijmegen supported the study financially.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.