
Abstract
Reduced physical activity is considered a key feature of major depressive disorder (MDD). However, research directly comparing non-depressed controls and patients yielded mixed findings. In contrast to most previous research, this study compared objective as well as subjective activity levels of individuals with MDD with non-depressed controls and used an ambulatory assessment method. Moreover, we investigated whether objective and subjective measures of activity could predict mood. On two consecutive days, physical activity of 35 MDD patients and 36 non-depressed control participants were assessed objectively using an accelerometer and subjectively with hourly ecological momentary assessments. During the same assessment, participants mood was monitored. No significant differences between MDD patients and control participants in objective and most of the subjective activity measures were observed. We found significant associations between objective and subjective measures of activity in non-depressed as well as in MDD patients. Objective but not subjective measures of activity predicted subsequent mood. Our results support the notion that the association between MDD and activity level is complex and depends on moderating factors.
Introduction
Over the years, the assessment of physical activity in everyday life has received major attention in research on major depressive disorder (MDD) (see reviews and meta-analyses by Burton et al., 2013; Schuch et al., 2017; Vancampfort et al., 2017). This is not surprising given that low levels of physical activity and energetic drive have long been suggested a key feature of MDD (DSM-5: MDD criterion A5 and A6; American Psychiatric Association, 2013). However, despite evidence that suggests deficits in the levels of physical activity in MDD, research directly comparing non-depressed controls and patients has yielded mixed findings. In detail, although recent meta-analyses reported overall lower levels of physical activity in depressed individuals (e.g., Burton et al., 2013; Schuch et al., 2017; Vancampfort et al., 2017), a number of studies failed to show differences between groups. For example, of the 14 papers included to compare overall activity levels between non-depressed controls and depressed patients in two recent meta-analyses (see, Burton et al., 2013; Schuch et al., 2017), six found no, or only partial support for less daytime physical activity in depressed individuals.
Interestingly, several moderating factors have been identified influencing the amount of physical activity depressed patients engage in. For example, differences in physical activity were found between inpatients, outpatients and those recruited from community samples (see, Schuch et al., 2017). Moreover, as Burton and co-workers (2013) pointed out in their meta-analysis, of the few studies investigating outpatients, many examined patients with seasonal depression or other subgroups, potentially casting further doubt on the generalizability of results to other forms of depression (i.e., MDD). In fact, only two studies in this meta-analysis investigated outpatients suffering from major depression, with both yielding mixed findings (Burton et al., 2013).
Another important issue in research on physical activity in depression is the accuracy of physical activity assessments. Most studies used either self-report measures or objective measures to assess daytime physical activity, but not both. This might be problematic. Indeed, recent reviews and meta-analyses with non-clinical samples put into question the correspondence between objective and self-report measures of daytime activity (Prince et al., 2008; Schuch et al., 2017) and report overestimation of physical activity using self-report measures. This might be even more problematic since mostly retrospective questionnaires and only rarely ecological momentary assessments were used.
Our present study aimed to address these methodological shortcomings. Therefore, we compared physical activity of MDD outpatients with non-depressed control participants matched for age and gender in everyday life. Outpatients in contrast to inpatients is a population which has not been studied extensively before. Moreover, other than most previous research we did not measure self-reported activity retrospectively, but utilized an ecological momentary assessment method. To assess whether the correspondence between subjective and objective measures might have been relevant for previous inconsistent findings, we used both objective measures as well as self-reports of physical activity. Indeed, previous work repeatedly confirmed significant differences in the amount of activity between studies reporting objective or subjective measures of activity in depression (e.g., Vancampfort, et al., 2016; Vancampfort et al., 2017). Moreover, in a recent meta-analysis comparing differences in physical activity between healthy controls and patients with mood disorders, four out of five studies using subjective measures of physical activity did not find differences between patients and controls. In contrary, in another meta-analysis on studies using only objective measures to assess physical activity, the majority found significant differences between patients and controls (Burton et al., 2013). The assessment of objective as well as subjective measures of activity will allow us to explore whether potential differences between depressed and non-depressed individuals can be observed predominantly in the objective or subjective measures.
Moreover, we explored the associations between subjective and objective measures of physical activity in depressed and non-depressed participants to explore whether the accuracy of self-report differs between both groups.
Finally, several studies using objective (i.e., accelerometer data, Hollands et al., 2020; Reichert et al., 2016; Reichert et al., 2017) and subjective measures of activity (i.e., ecological momentary assessments, Mata et al., 2012), have shown that mood and non-exercise activity level are associated. We aimed at replicating this relationship and tested whether objective and subjective levels of activity were associated with mood and whether the degrees of this association differ between depressed patients and never depressed controls (see Mata et al., 2012).
Method
Participants
Demographic and clinical characteristics.

Note. BMI = Body Mass Index; BDI-II = Beck Depression Inventory.
1 = χ2 Test, 2 = t-test.
Parts of the data of this study have been reported previously in relation to different research questions (Adolph et al., 2021). The study was approved by the local Ethics Committee of the University Hildesheim (number of ethic approval: 210) and was conducted in agreement with the Declaration of Helsinki. Participants provided informed written consent
Assessment of body activity
Objective activity data were assessed following published guidelines (Foerster & Fahrenberg, 2000; Reichert et al., 2015) with two accelerometers (Vitamove, Valkenswaard, Netherlands) placed over the participant’s trunk (three-channel accelerometer: sagittal, longitudinal, transversal axes) and on the outer part of the upper right leg (one-channel: sagittal axis). Data were sampled continuously with a sampling rate of 128 Hz within a range of +/− 6 g. The participant’s overall body activity was measured by the mean cumulative acceleration (in g), that was calculated in accord with previous reports (Van Someren et al., 1996). In brief, in order to remove the gravitational component each axis of the raw acceleration signal is high-pass filtered. Then a low-pass filter is applied to remove non-body movement accelerations (Van Someren et al., 1996). After combing the three axis signals by calculating the vector magnitude, movement acceleration intensity (range 0 to 2G) can be calculated for each period in time by averaging the vector magnitude signal (See also von Haaren et al., 2016)
In addition, the percentage of active behavior in upright position (e.g., walking, bicycling) was defined following published recommendations (Tremblay et al., 2017) and quantified automatically for each one-hour interval preceding the experience sampling prompts according to published movement pattern identification algorithms (Bussmann et al., 2001) using commercial software (Vitascore, Temec, Netherlands).
Experience sampling (i.e., self-reported activity and mood) data were assessed in 1 hour intervals with Palm Tungsten T3 handhelds running the freely available software Experience Sampling Program (ESP, version 4.0). Upon participants’ response, a number of questions concerning the participants’ physical activity during the past hour were released. To this end, participants were asked to indicate if they had been engaging in any kind of physical activity since the last beep. Upon confirmative response, they were asked the following questions: “How long have you been active?” (i.e., activity duration, range 0–5 corresponding to 0–10 min|10–20 min|20–30 min|30–40 min|40–50 min|50–60 min), “How intense was the activity you were engaging in?” (i.e., activity intensity, range 1–3, corresponding to mild activity—moderate activity—strenuous activity). After answering questions concerning their activity, we assessed participants mood. Therefore, participants were asked how they felt during the same period of time (i.e., during the last hour, that is, “How did you feel during the last hour?”). The response option on the screen ranged from −2 to 2, corresponding to very negative and very positive, respectively. Data were assessed on two consecutive days for 14 hours each (i.e., 8 a.m. to 10 p.m.). We choose a 2-day period, which is shorter than in most previous studies on physical activity and depression (Burton et al., 2013), because the apparatus to assess activity we used was less comfortable to strap on and wear than the wrist-worn devices usually used in this field of research. The two accelerometers placed on participant’s trunk and the outer part of the upper right leg were utilized, because we wanted to assess gait characteristics (e.g., posture, vertical body movements, walking speed, see Adolph et al., 2021) in addition to activity level. Therefore, to decrease burden and stress for our vulnerable participants and to reduce problems in the recruitment process we restricted the assessment period to 2 days.
Data reduction and analyses
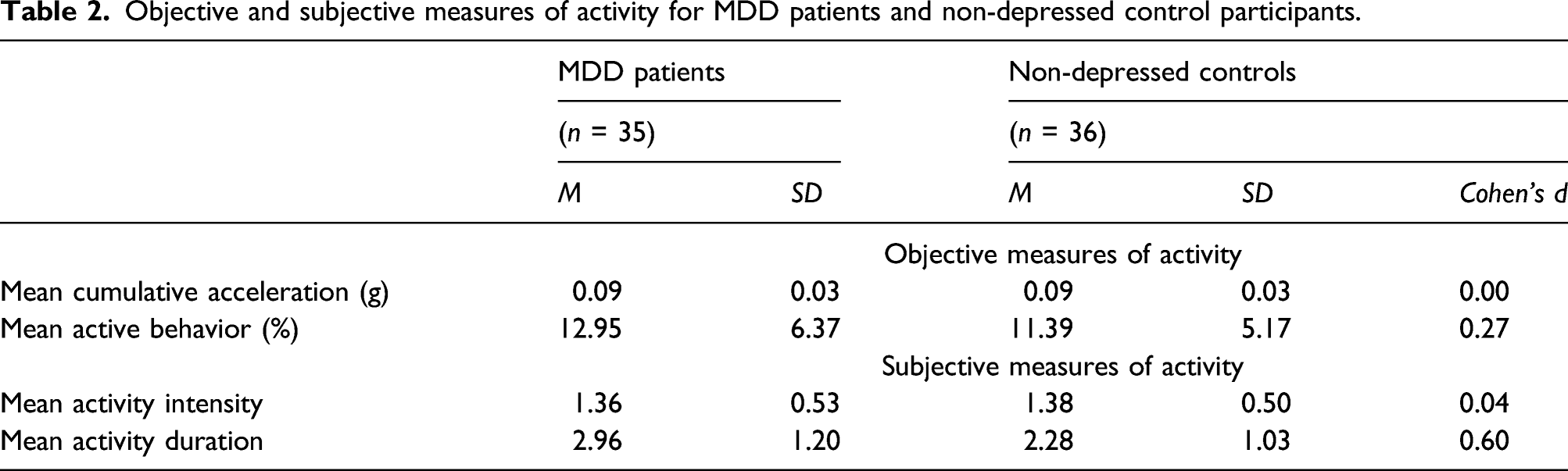
To obtain descriptive statists mean activity scores were calculated by averaging over the 2-day assessment period parameters of objective and subjective body activity. Mean scores of self-reported mood were obtained in the same way. Effects sizes (Cohen’s d) were computed to get an estimate of the magnitude of group differences between MDD patients and non-depressed individuals in aggregated objective and subjective activity level.
Since our data are unbalanced repeated measures taken over time, mixed-effects models are recommended (Snijders & Bosker, 2012). Therefore, in a next step, to test differences between non-depressed controls and MDD patients in subjective and objective levels of activity, a series of mixed-effects models with group as predictor (depressed patients vs. non-depressed control participants) were calculated.
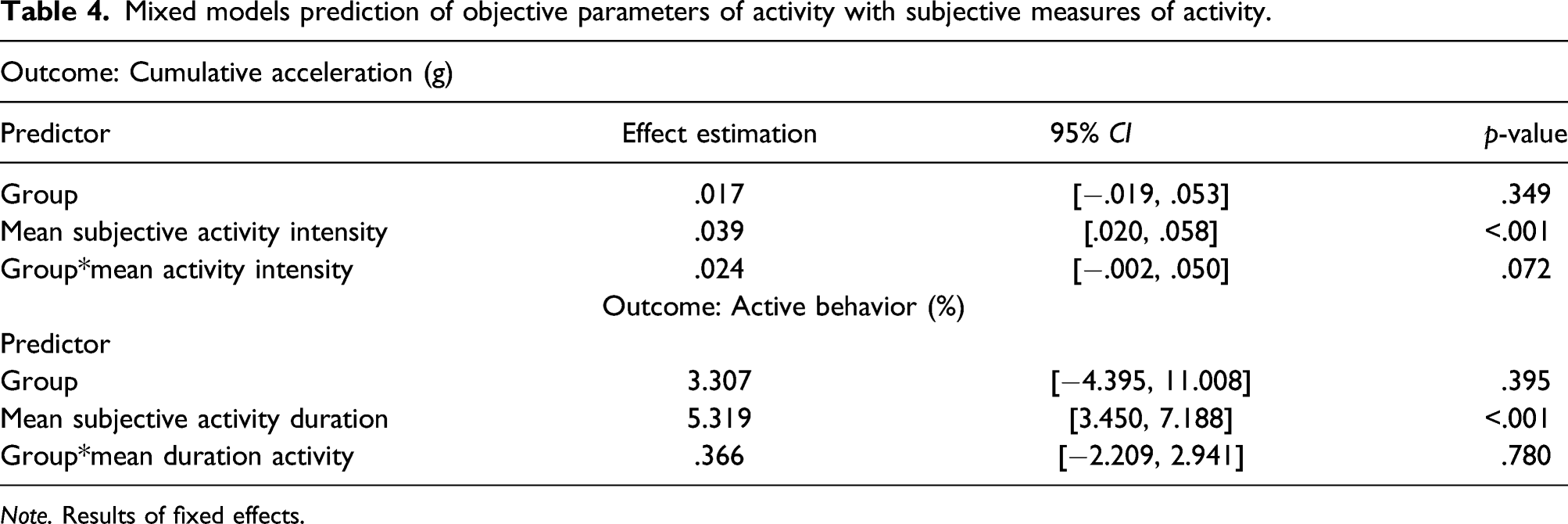
Moreover, to examine the associations between subjective and objective measures of physical activity, two mixed-effects models were conducted with group, self-reported activity intensity/self-reported mean activity duration and a two way-interaction between them.
Finally, to assess the association of objective and subjective parameters of physical activity duration and intensity with subsequent mood we conducted four mixed-effects models with mood as dependent variable, model 1 with group (depressed patients vs. non-depressed control participants), active behavior, and interaction between group and active behavior, model 2 with group (depressed patients vs. non-depressed control participants), cumulative acceleration, and interaction between group and acceleration, model 3 with group (depressed patients vs. non-depressed control participants), subjective activity duration, and interaction between group and subjective activity duration, model 4 with group (depressed patients vs. non-depressed control participants), subjective activity intensity, and interaction between group and subjective intensity of activity, as predictors.
All mixed-effects models were fitted with random intercept at the participant level while using REML and p-values were derived using the Satterthwaite approximations. Continuous predictors were group-mean centered. All analyses were conducted with SPSS.27.
Results
Differences in physical activity between non-depressed controls and MDD patients
Objective and subjective measures of activity for MDD patients and non-depressed control participants.
Mixed models comparing activity of MDD patients with non-depressed control participants.

Note. results of fixed effects.
Associations between subjective and objective measures of physical activity
Mixed models prediction of objective parameters of activity with subjective measures of activity.
Note. Results of fixed effects.
Association between objective/subjective measures of activity and mood
Results of four linear mixed-effects models with mood as dependent variable and subjective and objective parameters of activity as predictors.

Activity level in depressed individuals.
Discussion
The major aim of our study was to compare physical activity between MDD patients and non-depressed control participants. In correspondence with previous meta-analyses showing that a relatively high proportion of studies did not find differences between MDD patients and non-depressed controls (Burton et al., 2013; Schuch et al., 2017), we found no indication of a reduced activity level in MDD patients in objective measures as well as in subjective reports of activity. In contrast, in subjective measures patients even reported being active for longer durations as compared to non-depressed controls. Although this group difference in subjective duration of activity was not large and might therefore be interpreted with caution, it runs counter to the general notion that depression is characterized by an overall reduced activity level.
Our results support the notion that the association between MDD and activity is complex and that depressed individuals do not uniformly show reduced levels of activity. In contrast to the inpatient samples most often investigated in previous research, in our outpatient sample we did not find reduced objective or subjective levels of activity. Therefore, setting (outpatient vs. inpatient) might be a moderating factor in research on physical activity and depression and reduced levels of activity might be predominantly observable in inpatients but not in outpatients. This might be a consequence of level of depression. The average depression scores of our sample are on the borderline from moderate to severe. It is possible that significant reductions in activity level can be observed primarily in more severely depressed individuals. Moreover, the participants of our study lived in their everyday live with the usual demands and incentives that might have prevented pronounced decreases of the activity level. Future studies directly comparing activity level of depressed inpatients and outpatients should be conducted to more thoroughly test the potential moderating role of setting.
Moreover, the fact that we used an ambulatory assessment method in contrast to retrospective reports often used in previous research might be a factor that influenced our results. The ambulatory assessment method might less prone to retrospective negative biases that are characteristic for individuals with MDD (Gotlib & Joormann, 2010). Therefore, we recommend that future research should use a multimethod approach to assess activity level to investigate the effects of method factors on the activity depression association.
We found consistent associations between objective and subjective measures of activity. Subjective intensity of activity was associated with objective cumulative acceleration and subjective activity duration was associated with objective measured proportion of active behavior during the day. We found no group difference in the association between objective and subjective measures of activity indicating that depressed and healthy individuals show comparable subjective estimates of the motor activity during the day. These findings of a correspondence between self-reported and objective measure of activity are in line with previous meta-analytic work. Comparing a total of 148 studies on the correspondence between self-report and objective measures of physical activity in adult participants (with most studies using accelerometer data as an objective measure), previous work determined a mean correlation of 0.37 (Prince et al., 2008), a medium sized effect which had been confirmed recently using data from a large cohort study (i.e., r = 0.33; see Sabia, et al., 2014). Taken together, these findings support the validity of our current approach and underscores the integrity of our data.
A rather puzzling result of our study was that MDD patients reported longer durations of activity. Because MMD patients experience a number of motivational barriers toward physical activity (Firth et al., 2016) they perceive activity as more aversive (Carpiniello et al., 2013) and might therefore show a tendency to overestimate the duration of activity.
We could replicate the finding, that objective measures of activity and mood are associated (Hollands et al., 2020; Reichert et al., 2016; Reichert, et al., 2017). This result indicates, that in a relatively small time frame there is an interconnection between activity and mood. The non-significant group interactions in the linear mixed-effects models testing associations between objective activity and mood indicate, that this interconnection can be observed in depressed as well as in non-depressed individuals. However, the non-significant differences between depressed and non-depressed individuals in objective activity parameters case some doubts, whether mere activity level in the long run is associated with mood. The study by Adolph et al. (2021) has shown that the way people walk (walking speed and vertical movements during walking) differ between depressed and non-depressed individuals and predicted mood change within an hourly mood assessment. Therefore, one can speculate that not activity per se, but the style of movement might have stronger effects on mood.
In contrast to the activity/mood association in objective measures we did not observe significant associations between subjective ratings of activity and mood. We therefore could replicate the finding from Mata et al. (2012) that self-reported physical activity is not reduced in depressed individuals. However, in our study we only could show that objective activity predicted mood and could not replicate the associations between self-reported activity level and positive mood reported in study of Mata and colleagues. Change or methodological differences between our study and that of Mata and colleagues (i.e., sample size, other regional background of participants) might be responsible for the divergent results.
The results of our study have to be interpreted on the background of several limitations. The sample size was small. This might have especially compromised the power to detect group interaction effects in the mixed model analyses. Moreover, the measurement period of 2 days was shorter than the period used in most other studies on physical activity and depression. This might have affected the reliability of our assessment. Another limitation was that the current correlational approach does not allow for direct conclusions about causal associations.
Keeping these limitations in mind, our data from outpatients indicates that reduced overall activity levels in depression reported by previous reviews might not be easily generalized. Compared to non-depressed control participants we found no indication of reduced activity level of depressed patients in objective as well as in subjective measures of activity. Moreover, both groups show similar associations between objective and subjective activity level and in both groups objective but not subjective level of activity predicted mood. Therefore, our results may serve as a starting point for future research into the complex associations between depression and physical activity. Future research should take potential moderating factors like setting (outpatient vs. inpatient setting), assessment method (objective vs. retrospective vs. ambulatory assessment) and severity of depression into account.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by German Research Foundation (DFG) grant Mi 700/5-1 awarded to JM and German Research Foundation grant AD 452/1 awarded to DA.