
Abstract
Background: Medically unexplained physical symptoms (MUPS) are highly prevalent, frequently co-occurring with psychiatric symptoms such as depression, alexithymia, and anxiety. Objective: To evaluate the relation between depression, anxiety, and alexithymia and severity of somatic symptoms in patients with MUPS. Method: This is a cross-sectional study conducted on 196 patients suffering from MUPS. The patients were recruited from tertiary care internal medicine and neuropsychiatry clinics during the first quarter of 2019. The Patient Health Questionnaire (PHQ-15), (PHQ-9), Generalized Anxiety Disorder (GAD-7), Structured Clinical Interview for DSM-IV Axis I Disorders Clinician Version (SCID-I-CV), and Toronto Alexithymia Scale (TAS-20) were employed to assess somatic severity, depression, anxiety, major mental disorders, and alexithymia in the sample of patients. Results: The results of the study indicate that GAD-7 and PHQ-9 scores had a positive correlation with PHQ-15 (p < 0.05) in multivariate regression. In contrast, TAS-20 was not independently correlated with PHQ-15. Adding TAS-20 to GAD-7 and PHQ-9 in the equation of the regression model enhances the predictive capacity of the model (p < 001). Conclusion: The results of the study indicate that only anxiety and depressive symptoms, but not alexithymia, were associated independently with MUPS severity.
Introduction
Alexithymia was first described by Sifneos in 1973. Sifneos showed that some patients, particularly those affected by psychosomatic disorders, had great difficulties explaining and distinguishing their feelings during therapy. These patients were incapable of finding the words to describe their feelings (Sifneos, 1973). Numerous studies have reported a correlation between alexithymia and depression, but whether these two terms are separate and distinct or whether they overlap is still subject to discussion (Banzhaf et al., 2018; Lankes et al., 2020; Lipsanen et al., 2004). In other words, whether it is a lifelong phenomenon (as distinct from depression) or a secondary syndrome formed in response to particular psychological distress (coexisting with depression), as originally suggested by La Barbera et al. (2017) this debate is relevant, as it is crucial in deciding whether alexithymia is a personality attribute (La Barbera et al., 2017).
Alexithymia as a psychological construct has been subject to diverse conceptualizations and theoretical perspectives. Whether it is due to a defective cognitive ability to associate perceived feelings with their mental representations (affective agnosia), defective cognitive interoceptive processing of physical symptoms accompanying emotions, or faulty appraisal of attention is still discussed in recent literature (Ferraro & Taylor, 2021; Preece et al., 2017; Taylor & Bagby, 2021).
The importance of an in-depth understanding of alexithymia and its relation to somatization and other psychiatric psychopathologies has been highlighted in recent literature. Alexithymia has been identified as an independent risk factor predicting a poor outcome in patients with major depressive disorder (Serafini et al., 2020). Similar predictive value of alexithymia has been replicated in other disorders as relapse rates among patients with substance misuse (Palma-Álvarez et al., 2020) and depression among patients with chronic pain (Blaettler et al., 2019).
In a recently published review, it was concluded that alexithymia as a personality trait is a risk factor for suicide in psychiatric patients (De Berardis et al., 2017). A 10-year longitudinal prospective study on 1380 participants concluded that alexithymia is independently correlated with an increased mortality rate, particularly among men (Terock et al., 2021).
Medically Unexplained Physical Symptoms (MUPS) is a term often used in research to alleviate the stigma associated with somatization. A systemic review that included 32 epidemiological studies from 24 countries (N = 70,085) found that unexplained physical symptoms were not uncommon in primary care settings; the prevalence of at least one medically unexplained physical symptom ranged between 40.2% and 49% (Haller et al., 2015).
Though the diagnostic label of MUPS was removed from DSM-5 and replaced by somatic symptoms disorder (American Psychiatric Association Division of Research, 2013), the new paradigm shift was subject to criticism due to the confusing and misleading effect that could result from attributing mental illness to patients with comorbid medical conditions (Frances & Chapman, 2013; Toussaint et al., 2020). In fact, the term MUPS is still widely used by primary health physicians and other medical disciplines (Lamahewa et al., 2019; Olde Hartman et al., 2017; van Westrienen et al., 2019; Ziadni et al., 2018)
The coexistence and overlap between depression, anxiety, and alexithymia in patients with unexplained physical symptoms attending primary care facilities have been identified and discussed by psychosomatic specialists (Löwe et al., 2008). The high comorbidity rates across those three symptoms have been highlighted in recent literature tackling various pathologies such as unexplained dyspepsia or fibromyalgia (Kani et al., 2019; Melin et al., 2018).
The question as to whether alexithymia, independent of depressive and anxiety disorders, correlates with the severity of somatization in patients with MUPS remains unanswered. Our study aims to address this question using a multivariate analysis model.
Methods
This is a cross-sectional study conducted on 196 patients suffering from MUPS. The patients were recruited from tertiary care internal medicine and neuropsychiatry clinics during the first quarter of 2019. The enrolled patients gave their informed consent after having been informed, verbally and in writing, about the purpose of the research and its protocols. The study was approved by the review board of the Alexandria University School of Medicine, and it was conducted in accordance with the Declaration of Helsinki.
The inclusion criteria comprised recruiting patients aged between 18 and 60 years old with persistent MUPS for which no identifiable medical cause was found after proper medical examination and investigations for at least 3 months and which led to dysfunction.
The exclusion criteria included immunocompromised patients, pregnant women, patients with chronic debilitating diseases, current medical conditions contributing to the presenting symptoms, active substance or alcohol abuse or dependence, and psychosis.
The selected patients took part in a structured interview. The data collected included sociodemographic data (age, gender, residence, educational level, marital status, socioeconomic level, and employment status), present and past medical history, psychiatric history (psychiatric comorbidities, history of substance abuse, and stressors), family history, and personal habits.
The Arabic version of the Patient Health Questionnaire PHQ-15
The severity of somatic symptoms among the patients was recorded using the Arabic version for PHQ-15 (AlHadi et al., 2017). The PHQ-15 is one of the most suitable scales for assessing somatic symptoms in large-scale clinical trials. It has well-established psychometric characteristics, includes the relevant symptoms, and is relatively short. The Arabic version of the PHQ-15 has been validated and proved to be a reliable tool (Cronbach’s alpha was 0.826). It consists of a self-report questionnaire composed of 15 items, each of which is scored from 0 to 2, providing a 0 to 30 severity score. Item 4 related to menstrual cramps is only reported for females. The score was calculated by assigning scores of 0, 1, and 2, respectively, to the response categories of “not at all,” “bothered a little,” and “bothered a lot.” PHQ-15 scores of ≤4, 5, 10, and 15 represented cut-off points for no/minimal, low, medium, and high somatic symptom severity, respectively and for both genders.
The Arabic version of the Patient Health Questionnaire PHQ-9
The Patient Health Questionnaire PHQ-9 (Sawaya et al., 2016) is a standardized and accurate instrument used to screen or diagnose depression, assess the severity of symptoms, and measure the response of a patient to medication. This is a self-report questionnaire consisting of nine items, each with a score of 0–3, providing a severity score of 0–27. This is determined by awarding ratings of 0, 1, 2, and 3 to the “not at all,” “several days,” “more than half of the days,” and “almost every day” response categories, respectively. The cut-off points for mild, moderate, moderately severe, and severe depression were 5, 10, 15, and 20, respectively. The PHQ-9 Arabic version has been tested and shown to be a reliable instrument (Cronbach’s alpha 0.88). The sensitivity of the PHQ-9 in detecting depressive symptoms based on 10 as a cut-off score, compared to clinician diagnoses was 77%, and specificity was 46% (Sawaya et al., 2016).
The Arabic version of the Generalized Anxiety Disorder GAD-7
GAD-7 is a questionnaire used for diagnosing generalized anxiety disorder. As a screener for fear, social anxiety, and post-traumatic stress disorder, GAD-7 is known to have high sensitivity and precision (Sawaya et al., 2016). It is a self-report questionnaire consisting of seven items, each with a score of 0–3, giving a severity score of 0–21. The score is determined by assigning ratings of 0, 1, 2, and 3 to the “not at all,” “a few days,” “more than half of the days,” and “almost every day” response categories, respectively. Cut-off points for none/minimal, slight, moderate, and extreme anxiety, respectively, were expressed by ratings of 4, 5, 10, and 15. The GAD-7 was validated in the Arabic version and proved to be a reliable instrument (Cronbach’s alpha 0.95). The sensitivity of the GAD-7 in detecting anxiety symptoms based on 10 as a cut-off score, compared to clinician diagnoses was 57%, and specificity was 53% (Sawaya et al., 2016).
Arabic version of the Structured Clinical Interview for DSM-IV Axis I Disorders Clinician Version SCID-I-CV
The Structured Clinical Interview for DSM-4-Clinician Edition (El-Missiry, 2004; Hewedi et al., 2016) is a screening procedure used to diagnose DSM-4 Axis I disorders (major psychiatric disorders). It comprises seven diagnostic modules based on various diagnostic groups: mood disorders, depression, drug abuse, anxiety, somatoform disorders, eating disorders, and adjustment disorders. El-Missiry (2004) translated the SCID-I-CV into Arabic in 2004, and its use was confirmed in various studies performed in Egyptian study centers. In this analysis, only the mood and anxiety modules were used to validate the diagnosis of mood disturbances and anxiety disorders, respectively.
The Arabic version of the Toronto Alexithymia Scale TAS-20
The Toronto Alexithymia Scale TAS-20 is a multidimensional self-report instrument consisting of 20 items, each of which is scored from 1 (strongly disagree) to 5 (strongly agree) on a 5-point Likert scale. The three variables are difficulty identifying feelings (DIF), difficulty describing feelings (DDF), and externally oriented thinking (EOT). The overall score is on a 20 to 100 scale. DIF scores range from 7 to 35, DDF scores from 5 to 25, and EOT scores from 8 to 40. More serious alexithymia leads to higher scores. For categories such as alexithymic (scores >61), borderline/intermediate (scores between 51 and 60), and non-alexithymic (scores <50), the overall cut-off scores are used to classify respondents. A recently published review further confirmed the reliability and validity of the TAS-20 in evaluating alexithymia (Bagby et al., 2020). The Arabic version of the TAS-20 was used in this study (El Abiddine et al., 2017).
Statistical analysis
The data were evaluated using version 20.0.0 of the IBM SPSS software system. Numbers and percentages were used to define qualitative results. The Kolmogorov–Smirnov test was used to classify the quantitative data using the range (minimum and maximum), mean, standard deviation, median, and interquartile range to validate the normality of distribution. The significance of the findings obtained was measured at the 5% mark.
An hierarchical linear regression analysis was done. Firstly, a series of univariate analysis were carried out using PHQ-15 as the dependent variable while the independent variables GAD-7, PHQ-9, and TAS-20 were used separately to calculate the prediction model equation y = a + bx. Next, a bivariate analysis was done using both GAD-7 and PHQ-9 as the independent variables while PHQ-15 is the dependent variable. A prediction model equation was calculated y = a + b1 × 1 + b2 × 2. Finally, a multivariate regression analysis was done by adding TAS-20 to the independent variables to calculate a prediction model equation y = a + b1 × 1 + b2 × 2 + b3 × 3.
Multivariate regression model 1 (independent variables: GAD-7 and PHQ-9) was compared to model 2 where TAS-20 was added to the independent variables, using R squared of the both models to calculate how the predictors (the independent variables) explain the variance of the outcome (the dependent variable: PHQ-15). Then both models were compared using the standard error of the estimate to calculate the precision of the models to predict the outcome.
The R2 difference between both models was tested for significance using an ANOVA approach: F(H, N-K) = (RSSsmaller − (RSSlarger/H))/(RSSlarger/(N-K)), where F = F distribution statistic with H and (N-K) df; RSSsmaller = the residual sum of squares for the fewer parameters regression model; RSSlarger = the residual sum of squares for the greater parameters regression model; H = the number of parameters for the smaller (fewer parameters) model; K = the number of parameters for the larger (greater parameters) model; and N = total number of cases.
Results
The present study is a cross-sectional observational study that involved 196 patients with MUPS recruited from tertiary care medical and neuropsychiatry clinics, 86.7% of whom had persistent general fatigue, 61.2% had gastrointestinal tract symptoms, and 49% had back pains. There were 176 female patients and 20 male patients (F to M ratio = 9:1). The ages ranged from 18 to 60; 174 patients (88.8%) were aged under 35. Twenty-two patients were equally divided into two age ranges: 35–45 and 45–60. The marital status of the participants was distributed as follows: 54.1% were single, while 40.8% and 5.1% were married or divorced, respectively. In our sample, 85.7% (n = 168) originated from a city, while 13.8% (n = 27) were from the countryside. Only 0.5% (n = 1) were Bedouin. The most common complaint in patients with MUPS was easy fatigability (96.4%) followed by headaches (92.3%) with nausea and dyspepsia as the third presenting symptoms (90.8%).
Distribution of cases according to SCID-I mood and anxiety disorders (n = 196).
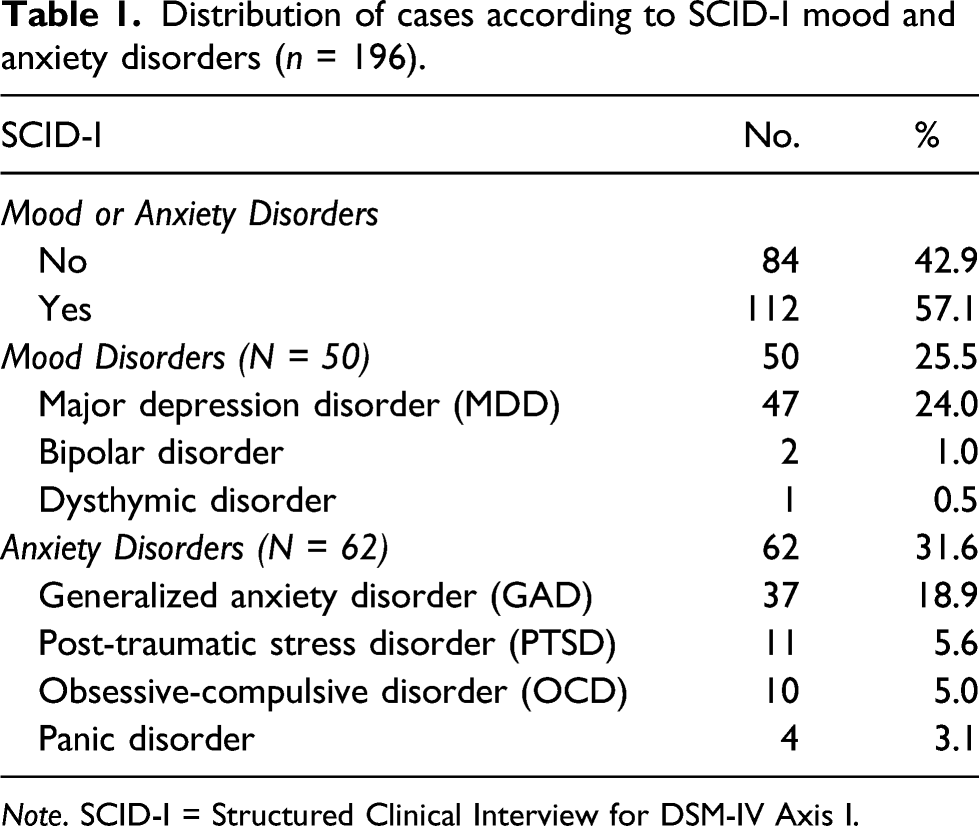
Note. SCID-I = Structured Clinical Interview for DSM-IV Axis I.
The severity of somatic symptoms was measured based on the PHQ-15 total score. Patients were distributed over four subgroups: minimal, low, medium, and high severity. The majority of patients (73.5%) had high PHQ-15 scores. Patients with medium severity somatic symptoms followed at 17.9%. Around 8% and 0.5% of the participants had low and minimal somatic symptoms, respectively. The mean for PHQ-15 total score was 17.31 ± 5.02, while the median was 18 (Figure 1). Distribution of PHQ-15 score according to severity in the sample (N = 196). PHQ: The Patient Health Questionnaire.
Depressive symptoms were assessed using the Patient Health Questionnaire PHQ-9. Based on the total score, patients were categorized into five categories. Those with severe depressive symptoms represented 37.2% of the studied sample, followed by patients with moderately severe depressive symptoms (24.5%). Minimal, mild, and moderate depressive symptoms constituted 4.1%, 14.8%, and 19.4%, respectively. The mean for PHQ-9 total score was 16.39 ± 6.68, while the median was 17 (Figure 2). Distribution of PHQ-9 score according to severity in the sample (N = 196). PHQ: The Patient Health Questionnaire.
Anxiety symptoms were assessed using the Generalized Anxiety Disorder Scale GAD-7. Patients were assigned to one of four categories based on their total score. Those with severe anxiety symptoms represented 48.0% of the studied sample, followed by patients with moderate symptoms (25.5%). Minimal and mild anxiety symptoms constituted 4.1% and 22.4% of the participants, respectively. The mean for GAD-7 total score was 13.44 ± 5.35, while the median was 14 (Figure 3). Distribution of generalized anxiety disorder-7 score according to severity in the sample (N = 196).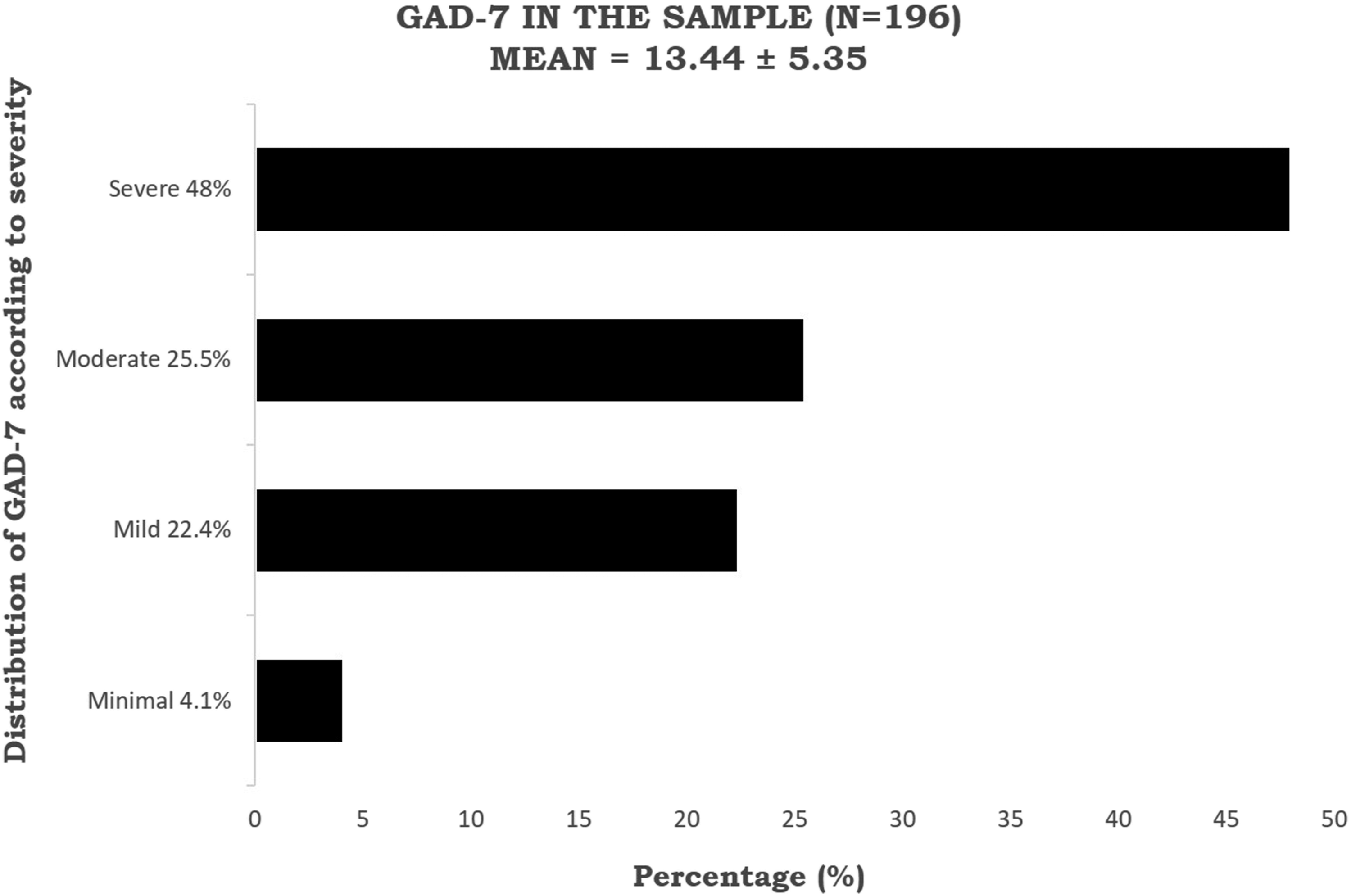
Descriptive analysis of the studied cases according to dimensions of TAS-20 score (N = 196).

Note. TAS = Toronto Alexithymia Scale; DIF = difficulty identifying feelings; DDF = difficulty describing feelings; EOT = externally oriented thinking.

Distribution of level of alexithymia Toronto Alexithymia Scale-20 score (TAS) in the sample (N = 196).
Multivariate linear regression analysis for variables affecting TAS-20 score (n = 196).

Note. F, p = f and p values for the model; R2 = coefficient of determination; B = unstandardized coefficients; SE = estimate standard error; Beta = standardized coefficients; t = t-test of significance; CI = confidence interval; LL = lower limit; UL = upper limit.
*Statistically significant at p ≤ 0.05.
Univariate linear regression analysis models using the severity of somatic symptoms (PHQ-15) as the dependent variable while levels of depression (PHQ-9), levels of anxiety (GAD-7), and levels of alexithymia (TAS-20) were fed separately as the independent variables.

Note. B = unstandardized coefficients; CI = confidence interval; β = standardized coefficients; r = correlation coefficient; R2 = determination coefficient; SE = standard error.
*Statistically significant at p ≤ 0.05.
Multivariate regression analysis using the score of PHQ-15 as the dependent variable and scores of PHQ-9 and GAD-7 as the independent variables at one step and then multivariate regression analysis was repeated after adding score of TAS-20 to the independent variables (n = 196).

Note. F, p = f and p values for the model; R2 = coefficient of determination; R = coefficient of regression; B = unstandardized coefficients; Beta = standardized coefficients; t = t-test of significance; CI = confidence interval; LL = lower limit; UL = upper limit.
*Statistically significant at p ≤ 0.05.
In the second regression model, the TAS-20 score was added to the independent variables. A multivariate linear regression was calculated to predict the score of PHQ-15 based on scores of TAS-20, PHQ-9, and GAD-7. A significant regression equation was found (F (3, 192) = 19.828, p < 0.001), with an R2 of 0.237. Participants predicted PHQ-15 is equal to 9.711 + .025 (TAS-20) + .188 (PHQ-9) + 0.228 (GAD-7), where TAS-20, PHQ-9 and GAD-7 are measured as score points. PHQ-15 increased 1 point for each 0.188 points of PHQ-9 score and 0.228 points of GAD-7 score. Both PHQ-9 and GAD-7 were predictors of PHQ-15. In contrast, TAS-20 was not independently correlated to PHQ-15 (p > 0.05) (Table 5, lower bloc).
Comparison between the two regression models where the PHQ-15 was the dependent variable. In model 1, the independent variables were level of depression (PHQ-9) and anxiety (GAD-7). In model 2, level of alexithymia (TAS-20) was added to the independent variables.
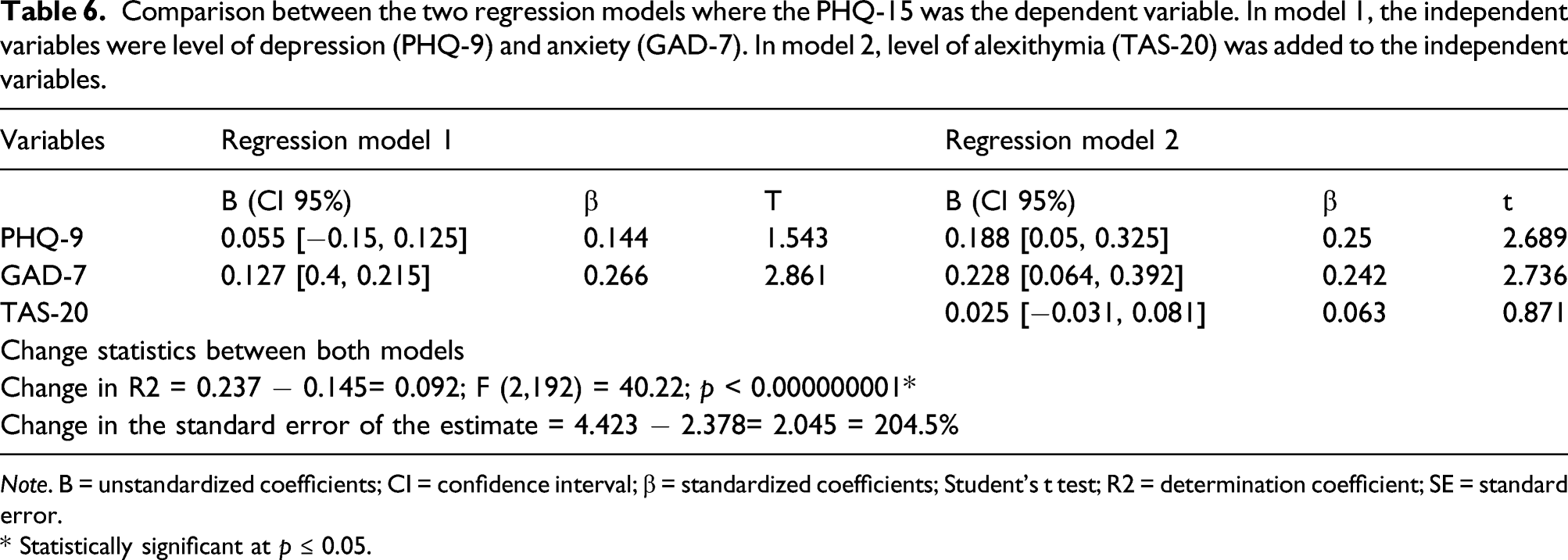
Note. B = unstandardized coefficients; CI = confidence interval; β = standardized coefficients; Student’s t test; R2 = determination coefficient; SE = standard error.
* Statistically significant at p ≤ 0.05.
Comparing both models using the standard error of the estimate showed that the standard error of estimate was 2.378 in the first model, and increased to 4.423 in the second model. A difference of 2.045 was found between both models. The higher the standard error of the estimate for a regression model, the less precise the model is, for prediction. This translates clinically as follow: In model 2, when level of alexithymia TAS-20 was added to the equation, considering the three variables GAD-7, PHQ-9, and TAS-20 decreases the precision to predict PHQ-15 by 53.764% compared to model 1 where only GAD-7 and PHQ-9 were the independent variable and was more precise in prediction than model 2 (Table 6).
Discussion
The present study was designed to evaluate the correlation of depression, anxiety, and alexithymia with the severity of somatic manifestations among patients with MUPS.
Depression, anxiety, chronic benign discomfort, obesity, and increased cardiovascular mortality were correlated with alexithymia, which was also marked by low emotional sensitivity and expressiveness (Melin et al., 2017). In a longitudinal study, alexithymia raised the risk of depression, and the manifestations of alexithymia tended to escalate during periods of depression. Depression, anxiety, and alexithymia were correlated with greater prevalence rates of MUPS, especially the “difficulty identifying feelings” alexithymia sub-component (De Gucht et al., 2004). In primary care patients and specialist hospital clinics, MUPS were common, with prevalence rates of up to 50% (Aamland et al., 2014).
In multiple types of research in primary care, the association between unexplained symptoms on the one hand and mental wellbeing issues on the other has been explored. However, the results of these experiments are not consistent. Our study indicates that the total GAD-7 and PHQ-9 scores positively correlated with PHQ-15 (p < 0.05), implying that anxiety and depressive symptoms are independently associated with MUPS severity.
Some researchers found that most patients with unexplained symptoms did not have an overarching mood, distress, or somatoform disorder (Jackson & Passamonti, 2005). However, other research shows that patients with medically unexplained symptoms had elevated depression or anxiety levels relative to patients with medically explained symptoms. Unexplained manifestations are also exacerbated by psychiatric issues. The higher the likelihood of depression or anxiety disorder, the more severe the symptoms (Duddu et al., 2008; Katon & Walker, 1998; Kroenke et al., 1994). Another study reported that MUPS, also after correction for depression and anxiety disorders and personality features, were positively correlated with frequent health care facility use over 2 years (Den Boeft et al., 2016).
De Waal et al. found that people with somatoform symptoms were 3.3 times more likely to be diagnosed with depression or an anxiety disorder in primary treatment with problems on the extreme side of the somatoform continuum (De Waal et al., 2004). A substantial overlap (approximately 50% of cases) in depression, anxiety, and somatization was also seen in numerous studies involving primary care participants. Therefore, screening for depression and anxiety is advocated based on these findings (Löwe et al., 2008). The presence of substantial somatosensory amplification, anxiety related to one’s health state, and alexithymia may be the reasons that people with GAD have greater vulnerability to excessive concern resulting from negative feedback. The advancement of unique psychotherapeutic interventions to treat somatosensory amplification, health anxiety, and alexithymia can complement and contribute to better response rates in psychotherapeutic interventions in GAD (Kumar et al., 2008). Cognitive therapy in combination with psychoeducation used to target depression, anxiety, and alexithymia had a substantial influence on the elimination of comorbid somatic symptoms in a review involving 15 Randomized Controlled Trials (N = 1671) (Liu et al., 2019).
In the present study, the total TAS-20 score was not independently correlated with PHQ-15 score in a multivariate regression analysis. Alexithymia was premised as a personality trait marked by difficulty in distinguishing and understanding emotions, reduced ability to envision and imagine, and thought focused outward rather than inward on conscious feelings. Patients with alexithymia were expected to be inadequately conscious that physical stimuli can be the somatic expressions of feelings. Therefore, these patients were susceptible to falsely attributing innocent physical signs to physical illness and to seeking medical attention for signs with no apparent medical cause. This is why alexithymia was hypothesized as a predisposing and maintaining factor in MUPS, potentially contributing to one of the somatoform disorders (Taylor et al., 1999). Alexithymia is a culturally sensitive psychological construct that was correlated with rural residence, low parents’ education, low socioeconomic status, social contacts, marital status and poor economic conditions during childhood (Kauhanen et al., 1993).
Various, generally nonclinical, studies identified an association between alexithymia and different somatization measures (Kumar et al., 2018; Lanzara et al., 2020). A correlation between alexithymia and varying somatization measures has been found in numerous, often nonclinical trials. Other studies showed that most MUPS patients had alexithymia, but that alexithymia, independently, did not show a correlation with a therapeutic outcome, unlike depressive and anxiety psychopathologies (De Vroege et al., 2018). This finding resonates with the present study where alexithymia, independently, did not correlate with the severity of somatic symptoms, unlike depressive and anxiety symptoms.
Data from literature found that higher levels of alexithymia was associated with older age, lower levels of education and male gender by some authors in the literature (Moriguchi et al., 2007; Pasini et al., 1992; Lane et al., 1998). In the present study, no significant correlation was found between TAS-20 score and the covariates of gender, educational level, and age group. This difference in results can be attributed to the homogeneity of our sample where the vast majority were females (89.8%) of high educational level (96.9%) and in the middle age group (18, 35) years old (88.8%).
The present study showed that adding levels of alexithymia (TAS-20) as an independent variable added to levels of depression (PHQ-9) and anxiety (GAD-7) can better predict the severity of somatic symptoms (PHQ-15) as shown by a rising determination coefficient (R2) from 0.145 to 0.237, this increment of 0.092 was statistically significant (p < 0.001). The association between levels of somatic symptoms and alexithymia was highlighted in the literature (Riem et al., 2018; Taycan et al., 2017; Zunhammer M et al., 2013). However how alexithymia may contribute to the severity of somatic symptoms in presence of depression and anxiety symptoms is unclear in the literature.
Alexithymia is a psychological construct with wide variations across different ethnic and cultural backgrounds. The manner in which alexithymia and emotional expressions are affected by transcultural dimensions is an important research field (Chentsova-Dutton, 2018). The present study highlights research focusing on the relation between MUPS severity, depression, anxiety, and alexithymic symptoms in Egypt, a Middle Eastern country, where there is a lack of relevant epidemiological data. This research could enhance future understanding of alexithymia in other cultures.
Conclusion
Depressive and anxiety symptoms correlate positively and independently with the severity of somatic symptoms in patients with MUPS. In contrast, alexithymia severity does not independently correlate with the severity of somatic symptoms.
Given the complexity of alexithymia and findings of the present study demonstrating a lack of a direct relation between alexithymia and severity of somatic symptoms in patients with MUPS, future research should examine this subject in greater depth. Such a study would use a longitudinal prospective approach to evaluate the stability of alexithymia and its effects over a long period, and it would assess concomitant psychopathologies. The discussion should seek to examine the interplay between the symptoms of psychopathology and the symptoms of alexithymia. An understanding of this interaction, and the effect of alexithymia on symptomatology and treatment outcomes, would contribute to developing a potential psychotherapeutic approach focused on alexithymic traits.
Limitations
One major limitation of our findings arises from our sole use of self-reporting tools to assess alexithymia. The TAS-20, as a self-report questionnaire, has been subject to scientific criticism because alexithymia patients are required to fill in a questionnaire about their ability to identify and express emotions. At the same time, due to alexithymia, they are incapable of addressing questions of that nature (Preece et al., 2020). The present study did not use more detailed questionnaires and scales to assess depressive and anxiety symptoms (such as the Beck Depression Inventory BDI or the Hamilton Rating Scale HAM for Depression or Anxiety). The present study used the clinician version of SCID-I for DSM-4 as it is still systemically used in our hospital records, and yet no available Arabic version of the clinician edition for SCID-5 (for DSM-5) that has been validated yet. In the present study did not screen for underlying personality disorders. Future studies considering personality disorders or other psychological personality constructs can provide deeper insight on alexithymia and its relation to severity of somatic symptoms in patients with MUPS. The small sample size is also a limitation. Small sample size is inversely related to a potentially higher standard error and, consequently, to statistical error and decreased statistical power. The present study did not include a comparative control group of patients with medically explained symptoms. Future research of a comparative nature would contribute to an understanding of the specificity of MUPS in various contexts.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
All procedures performed in this study were in accordance with the standards of the ethics committee and research review board at Alexandria University Faculty of Medicine (IRB No. 00012098, expires Oct. 2022; FWA No. 00018699, expires Jan. 2026), approval No. 0105861. Informed consent was obtained from all individual participants included in the study.