
Abstract
The co-occurrence between anxiety and depression symptoms among children with anxiety disorders is well-known, yet there is considerable heterogeneity in terms of explanatory factors. Although cognitive–affective processes have been hypothesized to play a prominent role, surprisingly, no research to date has examined the role of anxiety sensitivity in this co-occurrence. The present investigation examined the role of anxiety sensitivity in the co-occurrence of anxiety and depression symptoms among clinically anxious children. We expected that anxiety sensitivity would moderate the co-occurrence between anxiety and depression symptoms, such that higher anxiety would be related to higher depression among boys and girls with high (but not low) anxiety sensitivity. Participants (N = 44, age range = 8–12 years; 52% female; 52% African American) were interviewed with the Anxiety Disorders Interview Schedule-IV: Children and Parent Versions and completed self-report measures of anxiety sensitivity, anxiety, and depression symptom severity. Controlling for child age, moderation analyses revealed that higher anxiety was related to higher depression only among girls with high anxiety sensitivity. Among girls with low anxiety sensitivity, the relation between anxiety and depression symptoms was not significant. Anxiety and depression symptoms were strongly correlated among clinically anxious boys irrespective of their levels of anxiety sensitivity. Anxiety sensitivity is an important factor related to anxiety–depression symptom co-occurrence among clinically anxious females in particular. Targeted interventions focused on anxiety sensitivity reduction may prove useful for reducing anxiety–depression symptom co-occurrence among clinically anxious girls. Future research should explore additional moderators that may explain the high correlation between anxiety and depressive symptoms observed among clinically anxious boys.
The co-occurrence between anxiety and depression symptoms among children and adolescents with anxiety disorders is well-known (Costello, Egger, & Angold, 2005a, 2005b; Costello, Mustillo, Erkanli, Keeler, & Angold, 2003), yet there is considerable heterogeneity in terms of explanatory factors (Cummings, Caporino, & Kendall, 2014). Among youth with a principal diagnosis of anxiety, the presence of comorbid depression symptoms is associated with greater functional impairment, including lower family functioning, more severe anxiety, and lower ratings of global functioning (O’Neil, Podell, Benjamin, & Kendall, 2010). These findings underscore the need for increased understanding of the conditions (i.e., when or for whom) under which the association between anxiety and depression symptoms among clinically anxious children weakens or strengthens (moderation; Marsh, Hau, Wen, Nagengast, & Morin, 2011), in order to identify which youth are at greatest risk.
Although cognitive–affective processes (e.g., negative affectivity, rumination, response styles) have been hypothesized to play a prominent role (Chorpita, 2002; Nolen-Hoeksema, 2000; Zahn-Waxler, Klimes-Dougan, & Slattery, 2000), anxiety sensitivity, a robust cognitive risk factor for anxiety and depressive psychopathology (Naragon-Gainey, 2010), has remained largely unexplored as a potential moderator of the anxiety–depression symptom co-occurrence among clinically anxious youth. This is surprising, given that anxiety sensitivity consistently predicts both classes of symptoms (Naragon-Gainey, 2010), is malleable (Schmidt, Norr, Allan, Raines, & Capron, 2017), and easy to assess (Silverman, Goedhart, Barrett, & Turner, 2003). Anxiety sensitivity is defined as the fear of anxiety-related sensations due to the belief that these sensations signal potentially catastrophic consequences (Chorpita & Lilienfeld, 1999; Silverman, Fleisig, Rabian, & Peterson, 1991). To illustrate, a child high in anxiety sensitivity may believe that the visible signs of anxiety (e.g., blushing) will have catastrophic social consequences, or that an increase in heart rate due to anxiety may be a sign of a serious medical problem.
Anxiety sensitivity has been found to serve as a risk factor for the development of anxiety disorders by increasing preexisting levels of anxiety. It is hypothesized that this increase in anxiety and its symptoms is further interpreted by an individual with high anxiety sensitivity as more evidence of danger, which, in turn, generates more anxiety. This positive feedback mechanism results in an amplifying response that may culminate in severe anxiety (Reiss, 1991). Research suggests that anxiety sensitivity develops early (Taylor, 1999), has strong genetic underpinnings (Taylor, Jang, Stewart, & Stein, 2008), is linked to the development of anxiety problems (Hayward, Killen, Kraemer, & Taylor, 2000), and correlates significantly with indices of anxious temperament (Arden & Linford, 2009; Hagopian & Ollendick, 1996).
Several investigations with samples of children have found that anxiety sensitivity is elevated among anxiety disordered groups (Kearney, Albano, Eisen, Allan, & Barlow, 1997), and that anxiety sensitivity scores remain associated with anxiety and fearfulness above and beyond related constructs(Chorpita, Albano, & Barlow, 1996; Silverman et al., 1991; Weems, Hammond-Laurence, Silverman, & Ferguson, 1997), thereby adding to the validity and reliability of the construct among anxious samples. Second, longitudinal data (Hayward et al., 2000; Weems, Hayward, Killen, & Taylor, 2002), as well as challenge studies (Rabian, Embry, & MacIntyre, 1999), have contributed to the knowledge base of anxiety sensitivity as a predisposing or risk factor for childhood anxiety. For example, a cluster analysis of anxiety sensitivity scores over time (Weems et al., 2002) found that groups with high or escalating anxiety sensitivity were significantly more likely to have ever experienced a panic attack than those with low anxiety sensitivity. That said, although originally conceptualized as a risk factor for anxiety disorders, numerous studies have found that anxiety sensitivity is associated with disturbances outside of the anxiety domain, including, but not limited to, substance use (Paulus et al., 2016; Stewart, Samoluk, & MacDonald, 1999), traumatic stress (Viana et al., 2018; Vujanovic, Zvolensky, & Bernstein, 2008), personality-related pathology (Gratz, Tull, & Gunderson, 2008), and depression (Allan, Albanese, Norr, Zvolensky, & Schmidt, 2015; Viana, Dixon, Berenz, & Espil, 2017).
In terms of depression, significant associations between anxiety sensitivity and depression have been reported using samples of clinical and nonclinical adults and children alike (Capron, Allan, Ialongo, Leen-Feldner, & Schmidt, 2015; Lambert et al., 2004; Varela, Weems, Berman, Hensley, & de Bernal, 2007). In an outpatient clinical sample of 209 children and adolescents (Weems et al., 1997), anxiety sensitivity was significantly related to depression symptoms (Kovacs, 1992), even after controlling for anxiety. A significant relation was also found between the anxiety sensitivity and depression—controlling for anxiety—in a community sample of African American adolescents (Lambert et al., 2004). Yet, the vast majority of extant studies have examined anxiety sensitivity either as a predictor of depression severity (Grant, Beck, & Davila, 2007; Tull & Gratz, 2008; Viana & Rabian, 2009; Weems et al., 1997) and associated outcomes (e.g., suicide ideation; Capron et al., 2015) or in relation to anxiety and depressive symptomatology by way of emotion dysregulation (Kashdan, Zvolensky, & McLeish, 2008; Tull & Gratz, 2008). Surprisingly, however, studies examining whether anxiety sensitivity moderates the association between anxiety and depression symptom severity in clinically anxious children are lacking.
Greater understanding of factors that may increase or decrease the strength of the co-occurrence between anxiety/depression symptoms is clinically relevant and apt to lead to identification of malleable risk factors (Schmidt et al., 2007) within subgroups of children at especially high risk for this type of symptom co-occurrence. To illustrate, if the anxiety–depression symptom co-occurrence in clinically anxious youth increases as function of anxiety sensitivity, it stands to reason that targeted treatments that explicitly address anxiety sensitivity may benefit this population. Given that anxiety sensitivity is malleable (Schmidt et al., 2017) and that an excessive focus on internalizing experiences may be a key factor in the anxiety–depression symptom co-occurrence among children (Zahn-Waxler et al., 2000), the relevance of anxiety sensitivity as a candidate in this co-occurrence is apparent.
Of note, there is evidence that anxiety–depression symptom co-occurrence among children in general, and clinically anxious children specifically, varies in intricate ways as a function of gender. Longitudinal investigations find higher anxiety–depression symptom co-occurrence over time for girls compared to boys (Hankin, 2009). Others have found that preexisting anxiety increases the risk for depression among boys but not girls, who have a higher risk for depression compared to boys regardless of preexisting anxiety (Gallerani, Garber, & Martin, 2010). Moreover, gender differences in anxiety sensitivity have also been reported in nonclinical samples of youth; specifically, girls report higher anxiety sensitivity and are more concerned about the physical consequences of anxiety relative to boys, whose concerns about the social and psychological consequences of anxiety can feature more prominently (Walsh, Stewart, McLaughlin, & Comeau, 2004). Likewise, high anxiety sensitivity often involves ongoing monitoring and evaluation of bodily symptoms that may signal danger. Such state arousal may be more likely to increase risk for depression among girls than boys (Zahn-Waxler et al., 2000). Together, these data point to a complex interplay between these constructs as a function of gender.
With this background, the present investigation examined the moderating role of anxiety sensitivity in the anxiety–depression symptom co-occurrence observed in a sample of clinically anxious youth. Given considerable evidence for differential co-occurrence in anxiety-depressive symptomology (Gallerani et al., 2010; Hankin, 2009), as well as in anxiety sensitivity (Walsh et al., 2004) as a function of gender, analyses were conducted separately among boys and girls. We expected that anxiety sensitivity would moderate associations between anxiety and depression symptom severity in boys and girls, respectively.
Method
Participants
The current study is based on secondary analyses of data from a larger study on temperamental, parental, and information processing risks for childhood anxiety disorders (e.g., blinded for review, 2017). Forty-four children between 8 years and 12 years of age (M = 9.61 years, SD = 1.63; 52% female) and their mothers participated in this study. Maternal age ranged from 26 years to 50 years (M = 38.48 years, SD = 6.86; 57% were married). Fifty-two percent of the children identified as African American, 39% as White, and 9% as mixed race. Fifty-four percent of the mothers identified as African American and 46% as White. The mean annual income of families was in the range of US$50,000 to US$60,000 (overall range = <US$10,000 to >US$150,000), although 34% reported an annual income of <US$30,000. Fourteen percent of mothers had a high school diploma or General Education Diploma (GED), 30% had some college education, 18% had a 2-year college degree, 16% had a 4-year college degree, 2% had completed some graduate level courses, and 20% had at least a master degree. Fifty-one percent of mothers worked full time.
Children met Diagnostic and Statistical Manual of Mental Disorders (4th ed., text revision; American Psychiatric Association [APA], 2000) criteria for at least one anxiety disorder diagnosis based on results from semi-structured interviews conducted (separately) with both the child and the mother. Specific phobias were the most common primary anxiety disorder (43%), followed by generalized anxiety disorder (20%), social anxiety disorder (20%), separation anxiety disorder (11%), post-traumatic stress disorder (2%), and obsessive compulsive disorder (2%). Most of the sample (75%) had comorbid diagnoses, the most common being other specific phobias (30%), attention deficit/hyperactivity disorder (18%), generalized and separation anxiety disorder (6%, respectively), and social anxiety disorder (5%). Exclusionary criteria in the larger study from which the sample was drawn included (a) physical disability impairing ability to use a computer, (b) borderline or extremely low intellectual functioning (estimated full scale IQ < 80), (c) below average reading comprehension (standard score < 85), (d) psychosis, and/or (e) suicidality.
Measures
Anxiety Disorders Interview Schedule-IV: Children and Parent Versions
The Anxiety Disorders Interview Schedule-IV: Children and Parent Versions (ADIS-IV: C/P; Silverman & Albano, 1996) is a semi-structured diagnostic interview that assesses anxiety disorders and other childhood disorders, including affective and externalizing disorders according to DSM-IV-TR criteria (APA, 2000). It is considered the gold standard for evaluating the presence and severity of childhood anxiety disorders. A clinician severity rating ranging from 0 to 8 is assigned to each disorder and ratings of 4 or higher indicate that DSM-IV-TR diagnostic criteria have been met. Studies report test–retest reliability for composite parent–child diagnoses in the excellent range (Silverman, Saavedra, & Pina, 2001). Assessors were trained to use the ADIS-IV: C/P by observing videotaped samples of interviews conducted by the first author. Inter-rater agreement for primary diagnoses was assessed in 20% of the interview protocols and found to be in the excellent range (κ > .85). Mothers and children were interviewed separately using the parent and child versions, respectively, of the ADIS-IV: C/P. The assessor assigned diagnoses taking into account the perspective from both sources regarding the severity and interference of the disorder. All current diagnoses were included and ranked in order of severity. Discrepancies between the child and parent regarding primary diagnoses of the same severity rating were resolved during supervision sessions with assessors. In these cases, videotapes were reviewed and the first author made a final determination regarding the final diagnosis (Albano & Silverman, 1996).
Child Anxiety Sensitivity Index
The Child Anxiety Sensitivity Index (CASI; Silverman et al., 1991) is an 18-item self-report questionnaire that assesses the fear of anxiety-related sensations in children and adolescents. Children are asked to rate the extent to which they experience fearful reactions to normal anxiety responses on a 3-point scale (1 = none, 2 = some, 3 = a lot). Sample items include “It scares me when I am nauseous” and “When I can’t keep my mind on my schoolwork, I worry that I might be going crazy.” A total score is computed by summing the responses to all items with a possible range of scores from 18 to 54. Silverman, Fleisig, Rabian, and Peterson (1991) reported an α coefficient and test–retest reliability estimates of .87 and .76, respectively, in a nonclinical sample, and .87 and .79, respectively, in a clinical sample. In this study, the internal consistency of the CASI was α = .79.
Revised Children’s Manifest Anxiety Scale
The Revised Children’s Manifest Anxiety Scale (RCMAS; Reynolds & Richmond, 1978) is a widely used 37-item child self-report scale designed to assess anxiety symptoms in children. Twenty-eight items (e.g., “I am afraid of a lot of things,” “I worry a lot of the time”; 0 = no, 1 = yes) are summed to yield the anxiety score, with total scores ranging from 0 to 28. The remaining 9 items comprise a social desirability scale and are not part of the total anxiety score. Pela and Reynolds (1982) reported a test–retest reliability of .98 for the total anxiety scale using a 3-week interval. In this study, the internal consistency of the RCMAS was α = .82.
Children’s depression inventory
The children’s depression inventory (CDI; Kovacs, 1992) is a widely used, 27-item (e.g., “I am sad many times,” “nothing will ever work out for me”; rated 0, 1, or 2) child self-report questionnaire assessing depressive symptomatology over the preceding 2 weeks. Studies indicate that the CDI discriminates between depressed and nondepressed youth (Kovacs, 1985, 1992; Matthey & Petrovski, 2002) in outpatient and inpatient populations (Friedberg & Sinderman, 2011). Reliability and concurrent validity have been found to be high, and age- and gender-based norms are available (Kovacs, 1992). Internal consistency of the CDI in the present study was α = .86.
Procedure
All procedures were approved by the Institutional Review Board of the University of Mississippi Medical Center. Families were recruited to participate in a two-session study on temperamental, parental, and information processing risks for childhood anxiety disorders through local advertisements, child-oriented events, and flyers. Interested mothers initially contacted study staff or were contacted by study personnel via telephone. A description of the study was provided and a brief screen was conducted to assess for child exclusionary criteria. An initial 3-hr session was scheduled with eligible families.
Upon arrival, informed consent from mothers and informed assent from children were obtained. Self-report questionnaires were completed by the child, and mothers also completed questionnaires that are not relevant to the present analyses. Separate clinical interviews with the mother and child about the child’s symptoms were subsequently conducted by doctoral-level clinicians. Participants were then scheduled for a second final visit, yet only assessment data from the first session was used in the present analyses. Upon completion of the study, the mother and child were fully debriefed. Families received $25 per session for their participation, and children were also able to choose a small toy after each session.
Data analyses
First, correlational analyses were used to examine associations among study variables. Second, two separate linear regressions were conducted with CASI scores as potential moderators of the association between RCMAS scores (predictor variable) and CDI scores (criterion variable) among girls and boys, respectively. The PROCESS macro (Hayes, 2012) was used to compute regression analyses with centered means, bias-corrected confidence intervals (CIs), and 95% bootstrapping of 5,000 resamples (Hayes, 2013). The interaction term, as well as tests of the simple slopes as +/− 1SD of the mean level of the moderator, is automatically computed in PROCESS. The form of the interaction was examined both graphically, as per recommendations from Cohen and Cohen (1983), and statistically (Holmbeck, 2002) by examining the 95% bootstrapped CIs for the effect of anxiety symptoms on depression symptoms at each level of the moderator (PROCESS; Hayes, 2012). Finally, we employed the Johnson–Neyman technique (Johnson & Neyman, 1936) to evaluate the region of significance of the interaction. This procedure identifies the precise values of the moderator variable (CASI) for which the anxiety–depression severity association is estimated to be significantly different from zero.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Results
Descriptive statistics and correlations for all variables are reported in Table 1. Mean levels of anxiety (RCMAS), depression (CDI), and anxiety sensitivity (CASI) were consistent with those reported in past randomized clinical trials using these measures in clinical samples of children with anxiety disorders (Alfano et al., 2009; Kendall, 1994; Silverman et al., 1999; Weems, Berman, Silverman, & Saavedra, 2001). No gender or race differences were found on mean scores for any of the study variables (all analysis of variance p’s > .157), indicating comparable mean levels of anxiety, depression, and anxiety sensitivity between girls and boys and between White and ethnic minority children.
Correlations and descriptive statistics (N = 44).

Note. Correlations for boys presented above the diagonal and correlations for girls presented below the diagonal. Ethnicity = percentage of African Americans; CASI-total = Childhood Anxiety Sensitivity Index, total score; CDI-total = children’s depression inventory, total score; RCMAS = Revised Children’s Manifest Anxiety Scale, total score.
*p < .05; **p < .01.
Statistics for the regression analyses examining the interactions between RCMAS and CASI scores predicting CDI scores in girls and boys, respectively, are presented in Table 2. Among girls, the overall model was significant and accounted for 62% of variance in CDI scores; 15% of this variance was accounted for by a significant interaction of RCMAS and CASI scores, B = .08, SE = .03; t = 2.72, p = .014; 95% CI [0.02, 0.13]. Examination of the interaction indicated that as anxiety symptoms increased, so did depression symptoms, but only among girls with high anxiety sensitivity (Figure 1). This finding was supported by statistical examination of the simple slopes, in which the association between RCMAS and CDI scores was significant for girls with high, B = .96, SE = .27; t = 3.53, p = .002; 95% CI [0.39, 1.52], but not low CASI scores, B = −.02, SE = .26; t = −0.01, p = .993; 95% CI [−0.55, 0.54]. The Johnson–Neyman technique revealed that for CASI scores above 29.38 (47.83% of girls), the association between RCMAS and CDI scores was significantly positive.
Summary of regression analyses testing the interaction of anxiety symptoms and anxiety sensitivity predicting depressive symptoms (N = 44).

Note. CASI-total = Childhood Anxiety Sensitivity Index, total score; RCMAS = Revised Children’s Manifest Anxiety Scale, total score; CI = confidence interval.
*p < .05; **p < .01.
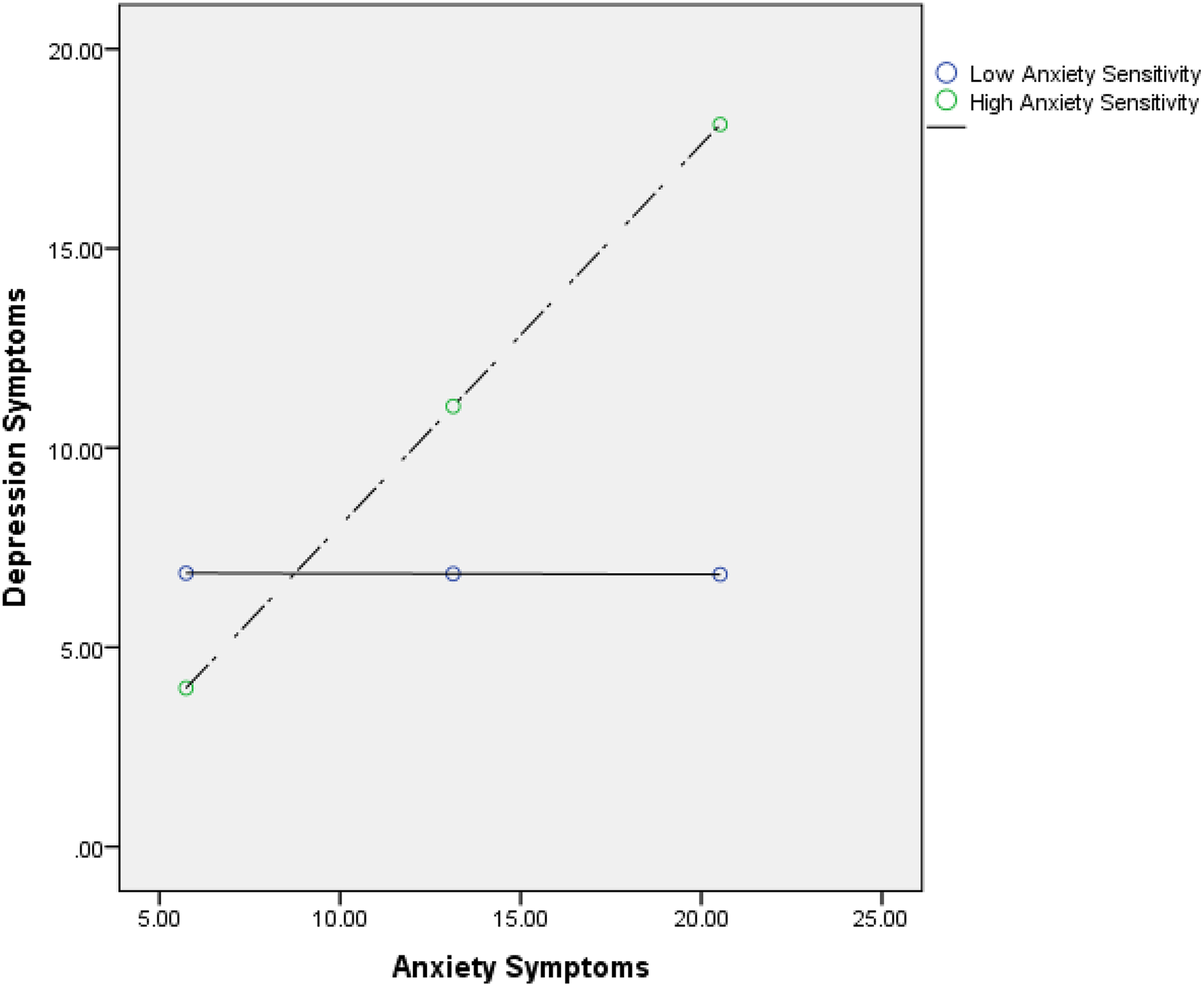
Predicted levels of depression symptom severity (CDI-total) among girls as a result of the interactive effect of anxiety symptoms (RCMAS-total) and anxiety sensitivity (CASI-total). The association between RCMAS-total and CDI-total was significant for girls with high (vs. low) CASI scores. CDI = children’s depression inventory; RCMAS = Revised Children’s Manifest Anxiety Scale; CASI = Child Anxiety Sensitivity Index.
Among boys, the overall model was significant and accounted for 37% of the variance in CDI scores. A significant main effect of RCMAS on CDI scores was significant, B = .48, SE = .20; t = 2.40, p = .027; 95% CI [.06, .89]. The interaction of RCMAS and CASI scores was not significant, R 2 change due to the interaction = .001, F (1, 17) = .02, p = .878. Consistent with the significant main effect found for RCMAS, examination of the interaction plot indicated that as anxiety symptoms increased, so did depression symptoms, irrespective of boys’ level of anxiety sensitivity (Figure 2).

Predicted levels of depression symptom severity (CDI-total) among boys as a result of the interactive effect of anxiety symptoms (RCMAS-total) and anxiety sensitivity (CASI-total). The interaction of RCMAS-total and CASI-total was not significant. CDI = children’s depression inventory; RCMAS = Revised Children’s Manifest Anxiety Scale; CASI = Child Anxiety Sensitivity Index.
Discussion
The anxiety–depression symptom co-occurrence among clinically anxious children is a frequently encountered phenomenon in both research and clinical settings (Starr, Stroud, & Li, 2016). Although progress has been made in terms of identification of relevant cognitive–affective factors related to this symptom overlap (e.g., negative affectivity, rumination), no study to date has examined anxiety sensitivity as a moderator of the relationship between anxiety and depressive symptomology among clinically anxious youth. The present investigation filled this void by examining the moderating role of anxiety sensitivity in the anxiety/depression symptom co-occurrence evinced by a diverse sample of children with anxiety disorders.
Consistent with hypotheses, there was a positive association between anxiety and depressive symptomology among girls with high (versus low) anxiety sensitivity. These findings suggest that girls who perceive anxiety as a frightening experience with potentially catastrophic consequences may be at increased risk for depressogenic feelings of despair and hopelessness. Likewise, high anxiety sensitivity often involves an excessive focus on monitoring and evaluating internal cues for potential danger. Such a state of sustained arousal may, in theory, “overtax” girls’ psychological resources and lead them to become increasingly depressed (Zahn-Waxler et al., 2000). Such a proposition would be consistent with cognitive models attempting to explain the anxiety–depression symptom overlap among adolescent and adult populations, which indicate that excessive attention to internalizing experiences may be responsible for the higher rates of anxiety, depression, and anxious-depressive comorbidity present among females (Hankin, 2009; Zahn-Waxler et al., 2000). Indeed, girls with high anxiety sensitivity may be excessively focused on and fearful of the physical consequences of anxiety sensations in particular (e.g., shortness of breath and heart palpitations) (Walsh et al., 2004). Over time, these beliefs may increase risk for depression to the extent that these physical sensations are perceived as uncontrollable. It is also possible that girls (vs. boys) are more likely to experience physiological arousal when anxious, which over time may produce feelings of depression if such physiological hyperarousal is thought to signal catastrophe (Walsh et al., 2004). Alternatively, albeit yet to be examined among children, the anxiety–depression symptom relation among girls with high anxiety sensitivity may be especially strong because high anxiety sensitivity in this group may signal increased genetic risk to anxiety and depressive disorders more broadly (Taylor et al., 2008). Indeed, more severe forms of AS appear to be more strongly influenced by genetic factors among females (Taylor et al., 2008).
Contrary to hypotheses, anxiety sensitivity did not moderate the anxiety–depression symptom overlap among clinically anxious boys, suggesting that other mechanisms might be operative. Negative affectivity (Chorpita, 2002) or certain environmental experiences such as parenting practices (van der Bruggen, Stams, & Bogels, 2008) may be more predictive of anxiety–depression symptom co-occurrence in boys. For instance, parents of anxious boys may be less accommodating of anxiety symptoms than parents of anxious girls (van der Bruggen et al., 2008), which may lead to feelings of isolation. Likewise, parents are more likely to discuss emotions with daughters than with sons, which may leave clinically anxious boys ill-equipped to understand and appropriately label anxious and depressed feelings (Fivush, Berlin, Sales, Mennuti-Washburn, & Cassidy, 2003). Anxiety may also be less socially acceptable to boys than girls, which may lead to increased feelings of rejection and isolation (Cummings et al., 2014). Lastly, research also has found that anxiety–depression symptom co-occurrence among boys may be linked to deficits in frontal lobe functioning and executive functions (Emerson, Mollet, & Harrison, 2005). Together, these studies suggest several important avenues for future investigation of this symptom co-occurrence among boys in particular.
Although not the focus of the present investigation, it is also worth noting that anxiety and depressive symptomology were interrelated, yet distinct constructs, sharing 39% (i.e., squared correlation) of the variance with one another (Table 2). The same proportion of shared variance was found between anxiety sensitivity and anxiety versus depressive symptoms, underscoring the unique contribution of the anxiety sensitivity construct to the anxiety/depression co-occurrence among clinically anxious children. Additionally, although African American youth scored somewhat higher than White youth on the CASI, this difference was not significant. This is inconsistent with previous studies reporting higher anxiety sensitivity among ethnic minority youth relative to White youth (Rabian et al., 1999; Weems et al., 2002), yet likely attributable to the present study’s sample size, which makes the detection of small effects challenging.
The findings should be interpreted in the context of several limitations. The data are cross-sectional, which precludes any causal inferences about the directionality of associations between variables. Although most studies suggest that anxiety precedes depressive symptoms (Cummings et al., 2014), it is plausible that depressive symptoms precede anxiety in some cases (Epkins & Heckler, 2011). The small sample size also impacted statistical power and precluded the evaluation of additional factors that may be implicated in the anxiety–depression association, such as other cognitive vulnerabilities like rumination, which has known relations to this symptom overlap (Nolen-Hoeksema, 2000). Incorporating these constructs would allow for exploration of their relative contribution vis-à-vis anxiety sensitivity to the anxiety–depression symptom co-occurrence among clinically anxious youth. A larger sample would also allow for exploration of the role of lower order facets of anxiety sensitivity in the anxiety–depression symptom co-occurrence. The study sample also limited the ability to examine relations within anxiety disorder specific subgroups. Investigating these relations in samples with greater representation of each anxiety disorder would also be an important extension in order to test whether similar patterns of moderation are found among the different anxiety disorders. It is also important to note that this study focused on anxiety–depression symptom co-occurrence in a sample of children with anxiety disorders with mild depression symptoms (see, e.g., Alfano et al., 2009; Kendall, 1994; Silverman et al., 1999; Weems et al., 2001, for similar CDI scores); it remains to be seen whether the same pattern of findings would emerge among children with higher depression symptoms and/or a primary diagnosis of major depressive disorder. This work could clarify whether the moderation effect found for anxiety sensitivity is transdiagnostic in nature. Finally, although most of the variance among constructs was not shared, the study is limited by method variance. A multi-method assessment of anxiety and depression would enhance methodological rigor.
Despite these limitations, there are several clinical implications that can be drawn from the findings. First, the assessment of anxiety sensitivity among clinically anxious youth in general and among girls in particular may be beneficial for identifying those who may be at high risk for depression symptoms. Second, targeted interventions for anxiety sensitivity could potentially be used with anxious girls to explore their effect on co-symptom reduction. Brief interventions exist to reduce anxiety sensitivity (Keough & Schmidt, 2012) and have been found to prevent the development of mental health problems 2 years later (Schmidt et al., 2007). Targeting anxiety sensitivity through these interventions may also reduce the vulnerability for depressive disorders among youth with anxiety disorders. However, these interventions have primarily been conducted with adults; evaluation of both the short- and long-term treatment outcomes of these interventions among youth with clinical anxiety is needed.
Together, the present investigation highlights a clinically meaningful role for anxiety sensitivity as a cognitive risk factor that strengthens the anxiety–depression symptom comorbidity among clinically anxious girls. Examining whether evidence-based interventions targeting this malleable construct result in reductions in the co-occurrence of these internalizing symptoms is warranted.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by an intramural grant from the University of Mississippi Medical Center (PI: Viana).