
Abstract
Although instable negative emotions and problems in emotion regulation (ER) are common in patients with psychosis and are discussed as potential factors involved in the formation and maintenance of paranoia, it is unclear whether they increase the risk of developing paranoia in nonclinical controls. The present study aims to investigate whether the instability of negative emotions leads to paranoia in healthy participants. It should be further analyzed if the application of maladaptive ER strategies enhances subclinical paranoid ideation and if the use of adaptive ER strategies reduces subclinical paranoid ideation.
Method:
Nonclinical controls (n = 83) repeatedly reported the presence and instability of negative emotions, paranoia, and the use of maladaptive (expressive suppression, rumination) and adaptive (reappraisal, acceptance) ER strategies in their daily life on six consecutive days using electronic mobile assessment.
Results:
Hierarchical linear regression analysis revealed that nonclinical controls reporting a pronounced instability of negative emotions showed more pronounced paranoia at a subsequent time point. Moreover, participants who used expressive suppression at a certain time experienced more severe paranoia at the subsequent time point.
Conclusion:
If these findings are confirmed in high-risk samples, ER processes could be considered as an additional factor in theoretical models of paranoia formation.
Introduction
Paranoia is defined as the persistent belief of a person that another person intentionally seeks to inflict severe physical, social, or psychological harm in the present or in the future (Garety & Freeman, 2013). Paranoid delusions are the most common delusions in patients with psychosis (Brakoulias & Starcevic, 2008; Gecici et al., 2010) and also found in lower, but varying levels in the general population (Nuevo et al., 2012). Thus, paranoid delusions are considered as a continuous phenomenon (Bell, Halligan, & Ellis, 2006), with hypothesized similar mechanisms acting in patients with psychosis and in nonclinical individuals (De Sousa, Sellwood, Griffiths, & Bentall, 2019; Hajdúk, Klein, Harvey, Penn, & Pinkham, 2019; Oestreich, Randeniya, & Garrido, 2019).
Over the past decade, the focus of research has increasingly shifted to emotional processes involved in the development and maintenance of paranoia (Freeman & Garety, 2014; Garety & Freeman, 2013; Preti & Cella, 2010). A common concept of emotions is the concept of discrete emotions (Lench, Flores, & Bench, 2011), which are also categorized as positive and negative emotions (Heiy & Cheavens, 2014; Visser, Esfahlani, Sayama, & Strauss, 2018). Negative emotions, defined as brief and intensive aversive states in reaction to a specific event (e.g., Ekman, 1992; Lench et al., 2011), have been found to be predecessors of paranoia in studies using the experience sampling method (ESM) in nonclinical individuals (Kramer et al., 2014) and patients with psychosis (Thewissen et al., 2011). ESM is a structured self-assessment diary to collect data on people’s current experiences in the realm of daily life at quasi-random times during a day. This technique could better adapt to the fluctuating experiences of paranoia in daily life (Thewissen et al., 2011; Udachina, Varese, Myin-Germeys, & Bentall, 2014).
Additionally, experimental studies revealed that the induction of negative emotions leads to an increase in paranoia in nonclinical individuals (Lincoln, Lange, Burau, Exner, & Moritz, 2010). Moreover, there is evidence that negative emotions mediate the association between stressors and paranoia (Hartmann, Sundag, & Lincoln, 2013; Lincoln et al., 2010).
Studies with nonclinical individuals indicated that paranoia is not only associated with negative emotions (Kramer et al., 2014; Lincoln et al., 2010), but also associated with more rapid changes of negative emotions, defined as emotional instability (Broome, Saunders, Harrison, & Marwaha, 2015). In a general population sample, these rapid changes of negative emotions predicted paranoid thoughts both cross-sectionally and longitudinally (Marwaha, Broome, Bebbington, Kuipers, & Freeman, 2014). Nevertheless, rapid changes of negative emotions are difficult to investigate with the application of retrospective questionnaires. Therefore, the present study uses ESM to assess emotional instability prospectively in daily life.
Since emotional instability is a risk factor for paranoia in nonclinical individuals, it is important to consider how these individuals regulate their emotions and whether this might affect subsequent subclinical paranoia. Emotion regulation (ER) is defined as the increase, maintenance, or decrease of emotions using various strategies (Gross & Thompson, 2007). According to Gross’ emotional process model (Gross, 2013), emotions can be influenced in two phases: first, they can be modified by antecedent-focused strategies before they are present: (1) selection of situations: leaving or not attending a specific situation; (2) modification of the situation; (3) attentional deployment: focusing one’s attention on a different aspect of the situation; and (4) cognitive change (changing one’s thoughts with regard to the situation). Second, response-focused strategies can be used after the emotion has been evoked, and these strategies focus on “intensifying, diminishing, prolonging or curtailing ongoing emotional experience” (Gross, 1998, p. 225).
Although the functionality of ER strategies may depend on the context (Aldao & Nolen-Hoeksema, 2012a; Koole, 2009), certain response-focused strategies, such as expressive suppression and rumination, are considered as maladaptive since they are associated with high levels of general psychopathology, reduced interpersonal functioning and well-being across different mental disorders (Aldao & Nolen-Hoeksema, 2010, 2012b; Moritz et al., 2015). Other ER strategies such as reappraisal and acceptance are considered as adaptive as they are associated with lower levels of general psychopathology and enhanced interpersonal functioning and well-being (Aldao & Nolen-Hoeksema, 2010, 2012b; Moritz et al., 2015).
As maladaptive ER strategies are associated with higher levels of general psychopathology, it can be assumed that they might also enhance subclinical paranoia in daily life. This assumption is supported by the fact that patients with psychosis tend to engage in more maladaptive ER strategies, such as expressive suppression and rumination, more frequently than nonclinical individuals in questionnaires studies (Kimhy et al., 2012; Martinelli, Cavanagh, & Dudley, 2013; O’Driscoll, Laing, & Mason, 2014; Simpson, MacGregor, Cavanagh, & Dudley, 2012; van Der Meer, van’t Wout, & Aleman, 2009) and experimental studies (Flower, Newman-Taylor, & Stopa, 2015; Jones & Fernyhough, 2008). A recent ESM study that investigated positive and negative emotions, ER strategies, and psychopathology in daily life showed that patients with schizophrenia tend to use expressive suppression more often than nonclinical controls (Visser et al., 2018). A second ESM study found that the use of the ER strategy expressive suppression in daily life predicted pronounced paranoia at the subsequent moment of the ESM assessment in patients with psychosis (Nittel et al., 2018). However, it is unclear whether the use of expressive suppression predicts pronounced subclinical levels of paranoia in nonclinical individuals in daily life.
With regard to more adaptive strategies, there is some evidence that the habitual use of reappraisal is associated with less pronounced levels of paranoid distress in a community sample (Westermann, Kesting, & Lincoln, 2012). However, while some studies failed to find conclusive associations between paranoia and more adaptive ER in nonclinical individuals (Flower et al., 2015; Westermann Boden, Gross, & Lincoln, 2013), others even report opposite associations (Westermann & Lincoln, 2011; Westermann, Rief, & Lincoln, 2012).
Nevertheless, most findings described above on the association between paranoia and ER strategies were obtained using ER questionnaires that are prone to memory effects (Stone, 2018) and do not correlate highly with momentary assessments of ER (Ben-Zeev, McHugo, Xie, Dobbins, & Young, 2012; Rydén, Leavy, Halling, & Stone, 2016). Studies using ESM may adapt better to measure the fluctuating experiences in paranoia (Thewissen et al., 2011; Udachina et al., 2014) and the use of ER strategies (Brans, Koval, Verduyn, Lim, & Kuppens, 2013).
Finally, it would be interesting to test whether the extent of emotional instability a person experiences might influence and moderate his/her success in employing different adaptive or maladaptive ER strategies. This is suggested by the fact that persons with borderline personality disorder who experience pronounced emotional instability have more problems with the effective use of ER strategies (Carpenter & Trull, 2013).
Thus, the present study used the advantage of an ESM design to assess changes in emotions from moment to moment and to investigate long-term associations between paranoia, emotional instability, and the use of ER strategies in a naturalistic setting without potential recall biases that arise during retrospective assessment (Marwaha et al., 2013). We assessed nonclinical subjects to investigate if a link between ER processes and paranoia can be established in individuals without mental disorders. If such a link can be identified, it would justify further assessment of the role of ER processes in the potential formation of paranoia in individuals with an enhanced risk of psychosis.
Our objectives were, first, to examine the impact of emotional instability on paranoia in daily life (hypothesis 1) and, second, to investigate longitudinal associations between the maladaptive ER strategies such as expressive suppression (hypothesis 2) and rumination (hypothesis 3) and subsequent paranoia. Third, the present study examines longitudinal associations between the adaptive ER strategies cognitive reappraisal (hypothesis 4) and acceptance (hypothesis 5) and subsequent paranoia. Furthermore, the study assesses whether emotional instability moderates the associations between these ER strategies and paranoia (hypothesis 6).
Method
Participants
Eighty-three nonclinical individuals without present mental disorders were included to this study. Inclusion criteria were an age between 18 years and 65 years and the absence of a mental disorder in the last five years as controlled using the Structured Clinical Interview for Diagnostic and Statistical Manual, Fourth edition (DSM-IV), Axis I Disorders (SCID-I: Wittchen, Wunderlich, Gruschwitz, & Zaudig, 1997), furthermore, based on recommendations by Delespaul (1995), missing data at level II (baseline questionnaires) as well as less than 20 valid responses during the assessment were considered as a reason for exclusion.
From the total sample (n = 90), two participants were excluded due to missing data at level II as they did not complete the baseline questionnaires, three participants were excluded due to an existing diagnosis of a mental disorder within the last 5 years (n = 3), and two participants were excluded due to technical problems during the assessment resulting in data loss. Thus, a total number of n = 7 participant had to be excluded from further analyses.
The recruitment was carried out via notices in public places or university student mailing lists. For compensation, participants received financial imbursement (10 €) or a confirmation of attendance to complete their curriculum requirements. All participants gave written informed consent. The local ethics committee approved the present study.
Procedure
Participants were first contacted via telephone, screened for adequate age, and subsequently invited to an interview appointment. During the interview, the presence of mental disorders was assessed with the SCID-I. Participants then completed baseline questionnaires to investigate habitual paranoia, depression, and estimated verbal intelligence (see the “Measures” section for further information). In an initial, approximately 1 hr, briefing, a research assistant instructed participants how to use the ESM mobile device. All ESM-items were explained in detail and examples were provided in order to illustrate each of the ER strategies (see Table 1). Participants also received an additional take-home manual with an explanation of all ESM variables. After 3 days, the research assistant called all participants and asked for additional questions and technical problems and gave instructions on how to solve them in case of occurring difficulties.
Explanation of emotion regulation strategies assessed in electronic mobile assessment that were given to participants.

Note. ER = emotion regulation.
aItem derived from an experience sampling method study by Brans, Koval, Verduyn, Lim, and Kuppens (2013) and translated from English to German and backward by two native speakers.
bItem derived from German questionnaire Selbsteinschätzung emotionaler Konsequenzen (SEK-27: Berking & Znoj, 2008) that assesses ER strategies.
Measures
Baseline questionnaires
The Paranoia Checklist (PCL; Freeman et al., 2005; German version: Lincoln, Peter, Schäfer, & Moritz, 2009) is a self-report questionnaire consisting of 18 items rated on a 5-point Likert-type scale to assess the frequency, conviction rate, and distress caused by several delusions of persecution and delusions of reference. For the present study, we used only the frequency scale and the distress scale. Internal consistency was acceptable for the frequency scale and high for the distress scale (Cronbach’s α: α = .77 and α = .97, respectively).
Depressive symptoms were assessed with Beck Depression Inventory (BDI-II: Beck, Steer, & Brown, 1996; German version: Hautzinger, Keller, & Kühner, 2006), a 21-item self-report questionnaire that investigates levels of depressive symptoms on a 4-point Likert-type scale. Internal consistency in the present sample was good (Cronbach’s α: α = .80).
Verbal intelligence was assessed with the multiple choice vocabulary test (MWT-B; Lehrl, 2005), a widely used German instrument to estimate verbal intelligence.
ESM
ESM is a quasi-random time-sampling self-assessment technique, which has proven its feasibility, validity, and reliability in previous studies of paranoia in nonclinical samples (Thewissen, Bentall, Lecomte, van Os, & Myin-Germeys, 2008; Udachina et al., 2009). In the present study, a preprogrammed iPod touch® (Apple, Cupertino, California, USA) emitted a signal at unpredictable quasi-randomized times on 6 consecutive days 10 times daily between 9.30 a.m. and 11:40 p.m. After each signal, participants answered 13 items addressing their present paranoia, their feelings (negative emotions: anxiety, loneliness, sadness, guilt, anger, insecurity; positive emotions: happiness, relaxation, satisfaction), and the use of the ER strategies (expressive suppression, rumination, reappraisal, acceptance, social sharing, reflection, distraction, savoring). Results on positive emotions and the ER strategies social sharing, reflection, distraction, and savoring will be reported elsewhere. Items used to assess paranoia and negative emotions have been applied in previous ESM studies (Myin-Germeys, van Os, Schwartz, Stone, & Delespaul, 2001; Oorschot et al., 2013). For the present study, the items were translated by forward–backward translation from Dutch to German by two native speakers.
Paranoia was assessed by the mean score of 3 items (“I feel that others dislike me,” “I feel that others might hurt me,” “I feel suspicious”) previously used in ESM studies (Collip et al., 2011; Oorschot et al., 2013; Thewissen et al., 2008, 2011). Items were rated on a 7-point Likert-type scale (1 = not at all and 7 = very much). As a benchmark for the internal consistency of ESM measures, within-person reliability was used, which is defined as the internal consistency of a set of responses collected at each measurement occasion and a functional equivalent of Cronbach’s α (for a detailed description, see Nezlek, 2016). Internal consistency of the state paranoia score was moderate, α = .68, classified according to the guidelines of Shrout (1998).
Negative emotions were assessed with 6 items (“I feel…sad, lonely, guilty, angry, insecure, anxious”) rated on a 7-point Likert-type scale (1 = not at all and 7 = very much). Reliability analysis indicated moderate internal consistency of the negative emotions scale (α = .72, see Nezlek, 2016). The mean score of the 6 items was used to compute the level of emotional instability: it was calculated using the mean square successive difference (MSSD) previously used in several ESM studies (Ebner-Priemer, Eid, Kleindienst, Stabenow, & Trull, 2009; Jahng, Wood, & Trull, 2008). The MSSD is the average of the squared difference between successive observations of negative emotions,
ER strategies were assessed in daily life using strategies included in Gross’s emotional process model (Gross, 1998): expressive suppression, rumination, and reappraisal. Strategies were each assessed with a single item rated on a 7-point Likert-type scale (1 = not at all and 7 = very much). Items assessing expressive suppression, rumination, and reappraisal were previously used in a different ESM study (Brans et al., 2013) and translated from English to German and backward by two native speakers. The authors added 1 item that assesses acceptance of negative emotions (“I accepted my feelings”). It is based on an item used in the German Questionnaire for self-assessment of emotional competencies (Selbsteinschätzung emotionaler Kompetenzen [SEK-27]; Berking, 2007). Table 1 depicts the items that were used to assess ER and the explanation participants received in order to detect the ER strategies during the ESM assessment.
Statistical analysis
Demographic and clinical variables were analyzed using the statistical software IBM SPSS Statistics 22 (IBM Corp., 2013). All hypotheses were tested indirectly by using two-tailed tests.
Skew, kurtosis, and normality of distributions of the ER strategies were analyzed using the Kolmogorov–Smirnov test. Z-scores of values of skew indicated positive skew and kurtosis for the variables expressive suppression (z s 1 = 7.88, z k 2 = 8.96), rumination (z s = 7.24, z k = 6.95), reappraisal (z s = 5.80, z k = 3.80), and paranoia (z s = 8.17, z k = 9.67). The Kolmogorov–Smirnov test indicated non-normally distributed data (p- values <.001 for the variables paranoia, expressive suppression, rumination, reappraisal, acceptance).
First, a manipulation check was performed to test whether ER strategies were employed to regulate negative emotions. Bivariate associations between positive and negative emotions and ER strategies were investigated with Spearman’s ρ (two-tailed) on the basis of positively skewed data.
Hierarchical linear modeling (HLM)
Because the ESM data comprised a multilevel structure with repeated momentary observations (level I) nested in persons (level II), we analyzed the data using HLM. State paranoia, negative emotions, and ER strategies were located at level I (within-person level) and emotional instability at level II (between-person level). Time lagged variables for all ER strategies were created representing ER strategies at one observation moment earlier (t − 1).
Variables at level I were centered around the group mean and variables at level II were centered around the grand mean. The β coefficients of the hierarchical models can be interpreted analogous to unstandardized linear regression coefficients. To provide additional information regarding the effect size, a pseudo-R
2 statistic was computed using the equation:
Hypotheses testing with HLM
In order to test first whether HLM is appropriate, a null model, that is, an unconstrained model without predictors for the dependent variable paranoia, was computed (Woltman et al., 2002). As the null model of the dependent variable paranoia presented a statistically significant variance component (p < .001), the indication for HLM was confirmed. Intra-class correlations (ICCs) for all ESM-variables were calculated as the ratio of between-person variance to the total variance in the null-model. The ICC is used to determine which part of the variance was caused by variations within person and which part by the variance between persons.
Second, in order to test the relationship between emotional instability and paranoia (hypothesis 1) and the relationship between change in paranoia and the use of the ER strategies expressive suppression, rumination, reappraisal, and acceptance (hypotheses 2 to 5), five separate multilevel linear random regression models were analyzed. In each of the models, paranoia was used as the dependent variable. In Model 1, emotional instability was defined as the independent variable. In Models 2 to 5, one of the ER strategies (expressive suppression, rumination, reappraisal, and acceptance) was used as independent variable. Finally, hypothesis 6 was assessed by including emotional instability as a moderator to test the cross-level interaction between ER strategies at level I and paranoia at level II (for an introduction to cross-level interaction, see Woltman et al., 2002).
Results
Sample characteristics
Sociodemographic and descriptive data of the 83 participants are illustrated in Table 2. Most of the participants were female, relatively young, and well educated. Depressive symptoms (BDI-II) and frequency and distress of paranoid thoughts (PCL) were low, while the verbal intelligence (MWT-B) was in the midrange.
Sociodemographic and clinical characteristics of the participants (n = 83).

Note. SD = standard deviation; MWT-B = multiple choice vocabulary test; BDI-II = Beck Depression Inventory-II; PCL = Paranoia Checklist; ESM = experience sampling method.
Manipulation check
Associations between the emotion regulation strategies expressive suppression, rumination and reappraisal and negative emotions were statistically significant (all p < .01). The size of Spearman’s correlation coefficients for associations between emotion regulation strategies and each single negative emotion were between r = .17 and r = .35 for negative emotions and between r = −.14 and r = −.10 for positive emotions (see Table 3). Associations between the emotion regulation strategy acceptance and negative and positive emotions were statistically significant (all p < .01) and Spearman's correlation coefficients were between r = −.13 and r = −.05 for negative emotions and between r = .23 and r = 27 for positive emotions. Accordingly, ER strategies were mostly used to cope with negative emotions (with the exception of the strategy acceptance).
Bivariate correlations (Spearman’s ρ, two-tailed) of associations between positive and negative emotions and emotion regulation strategies.
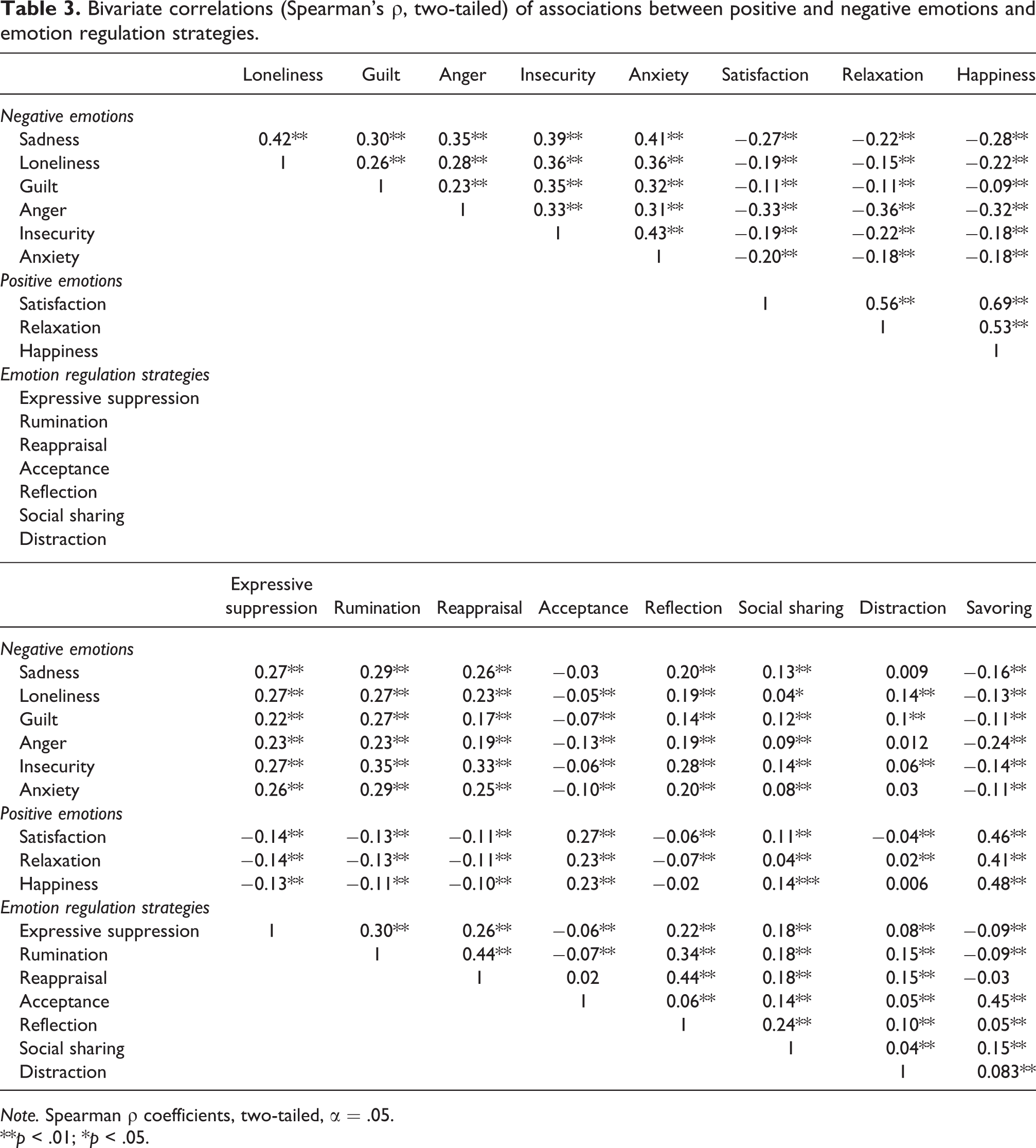
Note. Spearman ρ coefficients, two-tailed, α = .05.
**p < .01; *p < .05.
Bivariate correlations between ESM paranoia and ESM ER strategies
Bivariate correlations revealed that ESM paranoia was significantly related to expressive suppression (r = .32, p < .01), rumination (r = .29, p < .01), and reappraisal (r = .22, p < .01), whereas paranoia and the ER strategy acceptance were not associated with each other (r = .01, p = .66).
Fluctuation of ESM variables over the assessment period
The unconstrained models of the variables revealed an ICC of .33 for paranoia. Thus, 33% of the variance in paranoia scores is at the between-person level while 67% of the variance occurs between measurement points within a person. The remaining ICCs were as follows: maladaptive ER strategies: expressive suppression: ICC = .59, rumination: ICC = .20; adaptive strategies: reappraisal: ICC = .23, acceptance: ICC = .50.
Associations between emotional instability, ER strategies, and paranoia in daily life
First, in order to assess this question, a manipulation check was performed (see Table 3). More pronounced emotional instability was associated with higher levels of paranoia in daily life (hypothesis 1). Expressive suppression at t − 1 was associated with pronounced levels of paranoia at the subsequent time point (t) (hypothesis 2), whereas the use of the ER strategy rumination (hypothesis 3) predicted the level of state paranoia at trend level (p < .10, see Model 3). Neither the use of the strategy reappraisal (hypothesis 4) nor the use of the strategy acceptance (hypothesis 5) predicted the level of paranoia at the following time point. Finally, moderator analysis was merely performed for the association between expressive suppression and state paranoia and revealed that emotional instability did not moderate this association (see Table 4). After including expressive suppression and emotional instability into the model, the effect size pseudo-R 2 reached .05, indicating that the residual variance of paranoia was reduced by 5%.
Fixed effects of the hierarchical linear models testing the relation between emotional instability and paranoia (Model 1, hypothesis 1) and the influence of different emotion regulation strategies on paranoia (Models 2 to 5) and the moderating effect of emotional instability (hypothesis 6, Models 2 to 5).

Note. B = unstandardized regression coefficients; SE = standard error. Models were calculated using restricted maximum likelihood method. All random effects were significant (all p < .05),
Discussion
As expected, participants who experienced more severe emotional instability indicated pronounced levels of paranoia in daily life. In addition, participants who used expressive suppression to cope with negative emotions at one time point experienced more severe paranoia at the subsequent time point, whereas there was a trend toward increased paranoia in persons using the negative strategy rumination. In addition, using more adaptive strategies such as reappraisal and acceptance to cope with negative emotions did not lead to less pronounced paranoia at the following time point. Finally, pronounced emotional instability did not moderate the influence of the ER strategy expressive suppression on paranoia.
The present study is to the best of our knowledge the first ESM study that detected an association between pronounced emotional instability and subsequent pronounced levels of paranoia in a nonclinical sample. Our finding is in line with previous studies investigating general population samples (Marwaha et al., 2014) and patients with psychosis (Nittel et al., 2018). Although the finding is of interest on its own, future studies should further investigate the nature of the association between emotional instability and subclinical paranoia, for example in individuals with an enhanced risk of psychosis, to clarify the question whether emotional instability might be a risk factor for pronounced levels of paranoia and the transition to psychosis in this group. It is possible that emotional instability could amplify the triggering effect of negative emotions on paranoia (Kramer et al., 2014), potentially by enhancing sympathetic activation (Kreibig, 2010). If studies investigating high-risk samples demonstrate that emotional instability is involved in the transition to psychosis, first, it might be useful to integrate emotional instability into theoretical models for the development and maintenance of paranoia (Freeman & Garety, 2014; Garety & Freeman, 2013; Preti & Cella, 2010). Second, it might be beneficial to promote emotional stability in prevention programs for individuals at-risk for psychosis.
Future studies should assess the effects of emotional instability on paranoia over shorter time periods in order to provide more detailed insights into how to cope with emotional instability (Lincoln, Möbius, Huber, Nagel, & Moritz, 2014).
The present study is the first to report that nonclinical individuals who use the ER strategy expressive suppression to cope with negative emotions at one time point experience more pronounced paranoia at the subsequent time point. Our findings are in line with a questionnaire study by Jones and Fernyhough (2008), who found that nonclinical individuals who engaged in thought suppression and experienced high levels of anxiety reported more pronounced paranoia. This appears plausible, as expressive suppression has been found to amplify or maintain negative emotions (Lin & Wicker, 2007; Wenzlaff & Luxton, 2003) via post-suppression rebound (Campbell-Sills, Barlow, Brown, & Hofmann, 2006). Additionally, expressive suppression is associated with cognitive deficits such as memory loss (Richards & Gross, 2006) or a pronounced tendency to jump to conclusions (to decide quickly without gathering adequate information: Moritz, Van Quaquebeke, & Lincoln, 2012). It is therefore plausible that the use of expressive suppression in nonclinical individuals and the associated cognitive deficits could at a later stage lead to pronounced levels of paranoia.
Using expressive suppression to cope with negative emotions might even set a vicious cycle in motion, as a person experiences more paranoia as a long-term consequence and therefore engages more in expressive suppression of his/her feelings. In an ESM study in patients with psychosis, Visser, Esfahlani, Sayama, and Strauss (2018) showed that patients with psychosis used more maladaptive ER strategies earlier during the emotional process and failed to use these strategies because the intensity of their negative emotions did not decrease. Thus, using expressive suppression to reduce paranoia is neither successful in nonclinical individuals nor in patients with psychosis and might be an additional risk factor in the development and maintenance of paranoia.
Using rumination as an ER strategy to cope with negative emotions was on the one hand associated with more pronounced paranoia at the same time point. On the other hand, the use of rumination at one time point predicted pronounced levels of paranoia at the subsequent time point only on trend level. Nevertheless, our results are in line with experimental studies by McKie, Askew, and Dudley (2017) and Martinelli, Cavanagh, and Dudley (2013). Both experimental studies reported that using the ER strategy rumination did result in more pronounced levels of paranoia over a short time period (approximately 5–8 min.). Repetitive ruminating on paranoid thoughts and their content might maintain negative emotions by blocking normal habituation processes that would arise if the individual would focus on their negative emotions and use different ER strategies in order to cope with them, similar to the role of rumination in the context of depression (Visted, Vøllestad, Nielsen, & Schanche, 2018). Thus, it would be interesting to focus on the short-term effect of rumination on paranoid thoughts and also addressing its physiological effects on habituation.
Nevertheless, it is unclear why nonclinical individuals and patients with psychosis engage in expressive suppression or rumination, even if that leads to higher levels of paranoia, whereby operative conditioning (Skinner, 1938) is a possible explanation for this phenomenon. The positive short-term effects of the above named maladaptive ER strategies, that is, the short-term reduction of negative affect, could serve as a positive reinforcement of the use of these ER strategies (Alberts, Thewissen, & Middelweerd, 2013; Liverant, Brown, Barlow, & Roemer, 2008). In the present study, assessment time points were at least 1.5 hr apart, thus, we solely assessed long-term consequences of expressive suppression. It is possible that using expressive suppression might lead to positive effects in the short term as it might reduce the impact of negative emotions in general, leading to a rebound effect later (Campbell-Sills et al., 2006). Future ESM studies should apply more fine-grain analyses of ESM processes and focus more closely both on short- and long-term consequences of ER strategies in order to enlighten the processes involved in their development and maintenance.
Interestingly, neither the use of the adaptive ER strategy reappraisal nor the use of acceptance predicted reduced levels of paranoia at the subsequent time point of the ESM assessment. On the one hand, this is consistent with the finding that adaptive ER strategies generally show weaker associations with psychopathology (Aldao & Nolen-Hoeksema, 2012b) and paranoia (acceptance: Westermann et al., 2013; reappraisal: Westermann et al., 2013; Westermann, Rief, et al., 2012) as compared to maladaptive ER strategies. On the other hand, intervention studies indicate different results: Patients with psychosis who received acceptance-based interventions (Gaudiano & Herbert, 2006; White et al., 2011) reported greater symptom improvement than individuals who received standard treatment. In contrast to intervention studies, we provided participants with a single briefing session instead of an elaborate introduction to the practices of acceptance and reappraisal during extensive therapy. It is possible that individuals might need longer periods of training and support to use the ER strategies acceptance or reappraisal effectively (Shallcross, Troy, Boland, & Mauss, 2010).
One additional explanation could be that participants may have engaged in acceptance and reappraisal at least partly in a maladaptive manner. Instead of using active acceptance strategies (e.g., “This seems inevitable. I have to learn to live with it.”), some participants might have used more passive acceptance strategies (e.g., “I cannot change anything, I have to accept it.”; Nakamura & Orth, 2005) and this may have a neutral or enhancing impact on paranoia. Moreover, while some of the participants might have used reappraisal strategies to change their attitude toward negative emotions, other participants could have found even more negative interpretations when trying to reappraise. This hypothesis is supported by studies reporting that cognitive flexibility and contextual factors play an important role in deciding whether an ER strategy is adaptive or maladaptive (Aldao, 2013; Aldao & Nolen-Hoeksema, 2012a; Aldao, Sheppes, & Gross, 2015).
In the manipulation check, bivariate correlations showed that participants used the ER strategy acceptance particularly when positive emotions were present. This might partly explain that the use of the ER strategy acceptance was not related to increased levels of paranoia at a later stage. Previous ESM studies revealed that increased negative affect (Kramer et al., 2014), especially anxiety (Thewissen et al., 2011), leads to a subsequent increase in paranoia in daily life. It therefore seems plausible that the acceptance of positive emotions did not predict higher levels of paranoia in the present study. The item assessing the ER strategy acceptance was derived from an established German questionnaire (Berking & Znoj, 2008), nevertheless, it has not been used in an ESM assessment prior to the present study. It may be necessary to use more distinctive items to further determine the acceptance of negative (“I accept my unwanted feelings because I know I cannot change them.”) and positive emotions (“I accept my pleasant feelings.”) in future studies.
Further, future studies should more carefully examine whether participants have actually applied the ER strategies they claimed. As mentioned above, it is not always entirely clear if participants who claimed to use an adaptive ER strategy actually used the strategy in the assumed manner with regard to the assumed emotion.
For example, participants might claim to accept their negative emotions, while rather using a passive acceptance strategy (“I have to accept my feelings, because I can’t do anything about them.”). It may be useful to request more detailed questions from participants performing an ESM assessment on the ER strategies they have been using.
Finally, there is evidence that emotional instability did not moderate the effect of ER strategies on paranoia, while contradicting similar findings occur in persons with borderline personality disorder (Carpenter & Trull, 2013). It suggests that the application of strategies to more successfully regulate emotions does not depend on the individual level of emotional instability. Thus, learning strategies for people suffering from pronounced emotional instability may not be harder to learn and implement in daily life.
Strengths and limitations
A particular strength of the present investigation is the simultaneous assessment of different ER strategies that could be analyzed with regard to their impact on paranoia. However, our sample is not representative of the entire population, since it mainly consists of university students. Nevertheless, previous research indicates that students are more prone to paranoia than other population cohorts and, furthermore, exhibit higher levels of paranoia (Laursen, Munk-Olsen, Nordentoft, & Mortensen, 2007; Lincoln & Keller, 2008). Therefore, they represent a suitable research sample on the continuum of paranoia. However, although a nonclinical sample is appropriate to study the association between ER processes and subclinical paranoia, conclusions for clinical populations can only be drawn with great precaution. So far, studies on similarities and differences regarding ER processes in patients with psychosis and nonclinical individuals have been inconclusive (Laloyaux, Dessart, Van der Linden, Lemaire, & Larøi, 2016; Moritz et al., 2016; Visser et al., 2018) and future studies should focus on direct experimental comparisons of these groups.
In order to reduce the burden on participants, every ER strategy was assessed on the basis of only 1 item. However, prior ambulatory assessment studies reported that 1-item scales provide valid data in the assessment of ER strategies, so that our assessment can be considered sufficient (Brans et al., 2013; Heiy & Cheavens, 2014). Another limitation is that our assessment of ER strategies was solely based on self-reports. In fact, there is evidence that the use of the ER strategy acceptance only influences people’s physiological arousal and not their subjective ratings of emotions and, thus, might be hard to assess using merely self-ratings (Hofmann, Heering, Sawyer, & Asnaani, 2009). Therefore, an adjuvant validation using physiological measures (e.g., skin conductance level or heart rate variability) would be important in future studies to discern more implicit processes of ER.
Additionally, the present study categorized emotions in either “negative” or “positive” emotions using the discrete concept of emotions (Lench et al., 2011) without considering dimensional approaches of emotions (Coppin & Sander, 2016). Incorporating a dimensional assessment of emotions could yield further insights into the mechanisms of the association between emotions and paranoia.
Conclusions and implications
Our findings affect the common understanding of paranoia as well as future research on interventions for individuals with a pronounced risk of psychosis. If our results could be replicated in samples with a pronounced risk to psychosis, theoretical models on the genesis of paranoia could be expanded by integrating emotional instability and maladaptive ER strategies as one of the affective risk factors involved in the development and maintenance of paranoia or positive symptoms of psychosis (Freeman & Garety, 2014; Garety & Freeman, 2013; Preti & Cella, 2010).
For nonclinical participants with a low risk of developing paranoia, group trainings of ER skills as the Training of Emotional Competencies (Berking, 2007) could be used in order to enhance their ability to regulate negative emotions and their general mental health as part of a comprehensive primary prevention approach. Furthermore, if future research can establish ER processes as causal for the formation and maintenance of paranoia, it might be worthwhile to integrate interventions in order to cope with ER difficulties in Cognitive Behavior Therapy for psychosis (CBTp). Possibly, interventions from dialectic behavior therapy for borderline personality disorder (Linehan, 2018) or acceptance and commitment therapy (Hayes, Luoma, Bond, Masuda, & Lillis, 2006) could be integrated in CBTp manuals in order to improve both general and selective prevention interventions for individuals with a pronounced risk of a psychotic disorder. Including these interventions in the treatment of individuals with a pronounced risk of a psychotic disorder or patients with psychotic disorders might enhance the effectiveness of present CBTp interventions on reducing paranoia.
Footnotes
Acknowledgment
The authors would like to thank all participants of the study and C. Gross, S. Schraube, J. Zachlehner, and P. Haas, who helped collecting data.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Stephanie Mehl has published a manual and chapters of textbooks on CBTp for psychosis. S. Mehl and F. Lamster presented several workshops and supervision in CBTp for psychosis. The other authors report no conflict of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by resources provided by a cooperation contract between the Philipps-University of Marburg and Justus-Liebig-University of Gießen (Kooperationsvertrag, project no. 33/2012 MR).