
Abstract
Negative mental imagery contributes to symptom maintenance in social anxiety disorder (SAD). Here, we investigated the effects of image morphing, a brief mental strategy designed to facilitate access to positive images. Participants with SAD and healthy control (HC) participants were randomly assigned to receive either image morphing or supportive counseling. Although initial training and 1-week daily practice were successful in equipping morphing participants across groups with the required skill, those assigned to morphing failed to demonstrate differential improvements in positive affect, negative affect, or self-perception relative to control participants during a subsequent social stress task. Ancillary analyses revealed that the number of positive details contained in retrieved or morphed images prior to the task significantly predicted the level of positive affect reported after the task, but this effect was observed only for HC participants. We discuss the need for future research to refine innovative imagery-based psychotherapeutic strategies for social anxiety.
Introduction
Cognitive models of psychopathology have long recognized the importance of both maladaptive thoughts and mental images in the persistence of psychological disorders (Beck, 1976; Holmes, Arntz, & Smucker, 2007). Unlike thoughts, mental images often engage multiple sensory modalities (e.g., visual, auditory, kinesthetic; Çili & Stopa, 2015; Kosslyn, Ganis, & Thompson, 2001) and activate similar brain pathways as those involved in the actual perception of sensory events (Holmes & Mathews, 2010), thus helping to facilitate the simulations of real-life experiences within the mind’s eye. As such, mental images can have particularly powerful effects on emotional experiences (e.g., Borkovec, Lyonfields, Wiser, & Deihl, 1993; Holmes et al., 2007; Holmes & Mathews, 2005, 2010).
Intrusive imagery plays a key role in various psychological disorders, including post-traumatic stress disorder (Conway, Meares, & Standart, 2004; Ehlers & Clark, 2000), body dysmorphic disorder (Osman, Cooper, Hackmann, & Veale, 2004), major depressive disorder (Gilbert & Irons, 2004), obsessive-compulsive disorder (Speckens, Hackmann, Ehlers, & Cuthbert, 2007), and social anxiety disorder (SAD; Hackmann, Surawy, & Clark, 1998; Hirsch, Clark, Mathews, & Williams, 2003; Hirsch, Meynen, & Clark, 2004). Negative images are often rooted in distressing autobiographical memories in which the themes of recollected events evoke central features of each specific disorder (Hirsch & Holmes, 2007; Holmes, Geddes, Colom, & Goodwin, 2008; Romano, Ma, Moscovitch, & Moscovitch, In Press). In SAD, it is common for individuals to experience distressing images of themselves appearing socially inept and undesirable and to associate the formation of such images with past experiences of perceived social failure or humiliation (Moscovitch, 2016; Moscovitch et al., 2018). Despite being excessively negative and distorted, these images of the self are believed by socially anxious individuals to represent accurate portrayals of how they appear to others (Hackmann, Clark, & McManus, 2000; Moscovitch, Gavric, Merrifield, Bielak, & Moscovitch, 2011; Stopa & Bryant, 2004).
Negative mental images work to maintain the symptoms of social anxiety by directly impacting present-day behavior. For example, holding negative images in mind has been shown to elicit increased internal monitoring and use of safety behaviors (e.g., Hirsch et al., 2004), which detract from skillful social engagement and adversely affect social performance (Çili & Stopa, 2015; Rowa et al., 2015). Persistent experiences of negatively distorted self-imagery can also prevent new learning in the face of disconfirmatory evidence, thus facilitating the persistence of maladaptive and inaccurate beliefs about the self (Ng, Abbott, & Hunt, 2014) and unduly influencing the perceived probability that feared social outcomes will occur in the future (Holmes & Mathews, 2005).
Prior research has demonstrated that socially vulnerable individuals may benefit from accessing and holding positive images in mind. In one study, individuals diagnosed with SAD who were instructed to hold a positive, as opposed to negative, mental image in mind experienced less anxiety during a conversation task and were found to perform both subjectively and objectively better on an in-lab interaction (Hirsch et al., 2003). Other work has demonstrated that the use of positive self-imagery leads to decreased anxiety and increased performance ratings during laboratory-based speech tasks (Stopa & Jenkins, 2007; Vassilopoulos, 2005) and that holding in mind positive mental images is associated with higher levels of explicit self-esteem among those experiencing social exclusion (Hulme, Hirsch, & Stopa, 2012). Despite the potential benefits of positive imagery in social anxiety, however, individuals with high levels of trait social anxiety tend to access fewer positive images than those with low levels of social anxiety, and the images that they are able to access tend to be impoverished in episodic detail (Moscovitch et al., 2011). Taken together, these findings suggest the potential importance of investigating methods that may enhance positive image accessibility among socially anxious individuals.
Imagery rescripting (IR; Holmes et al., 2007; Holmes & Mathews, 2010) has emerged as an effective brief intervention for a range of disorders, including SAD (Arntz & Weertman, 1999; Holmes et al., 2007; Weertman & Arntz, 2007; Wild, Hackmann, & Clark, 2008). IR involves therapeutically guiding patients to retrieve a self-defining negative memory from their past, imagine the experience unfolding in detail from both first- and third-person perspectives, and ultimately modify the imagined memory content in ways that help to meet the needs of their younger self. In so doing, patients learn to update the idiosyncratic meaning that the event holds for them and to reappraise its significance in relation to their core beliefs about self, others, and the world (Reimer & Moscovitch, 2015). Thus, when implemented in the clinic, imagery-based interventions like IR appear to have tremendous potential for enhancing psychotherapeutic outcomes. However, little is known about the potential feasibility and effectiveness of briefer and simpler imagery-based strategies that could be taught to anxious individuals in order to help facilitate their access and use of positive imagery in an efficient and self-directed manner during their daily lives. Such strategies might be important for helping socially anxious individuals cope effectively with the negative image intrusions they tend to experience within anxiety-provoking contexts. One potentially viable coping option comes from Hirsch et al. (2004) research, which demonstrated that simply holding a nonnegative self-image in mind during a conversation task, as opposed to a negative one, was associated with both subjectively and objectively better performance, as well as less self-reported anxiety during the interaction. To this end, Hackmann and Holmes (2004) suggested that “image substitution”—the apparently simple process of accessing and holding a positive image in mind instead of a negative one—could represent a useful imagery-based coping strategy for anxious individuals who are vulnerable to negative image intrusions within anxiety-provoking contexts.
Given the ubiquity of negative image experiences, it is likely that many individuals have developed idiosyncratic ways of coping with mental image intrusions in the absence of professional guidance. For example, Moscovitch, Chiupka, and Gavric (2013) found that high social anxiety and low social anxiety individuals differed in the strategies they endorsed spontaneously using to cope with negative mental image intrusions, with 90% of low social anxiety individuals but only 50% of high social anxiety individuals reporting that they cope with image intrusions by actively entering their imagination and changing their content or perceptual features. Conversely, 50% of high social anxiety individuals but only 10% of low social anxiety individuals reported either suppressing or passively succumbing to their negative images (Moscovitch et al., 2013). Whereas actively attempting to change or reappraise undesirable features of negative images may be consistent with principles of effective emotion regulation, there is evidence suggesting that both expressive suppression (i.e., attempts to hide or suppress displays of emotion; e.g., Haga, Kraft, & Corby, 2009) and emotional suppression (i.e., attempts to suppress internal emotional experiences; e.g., Campbell-Sills, Barlow, Brown, & Hofmann, 2006) are not adaptive coping strategies. For instance, the use of suppression strategies for coping with negative emotions has been shown to heighten levels of negative affect, depressive symptomatology, and interpersonal difficulties, as well as reduce positive affect and life satisfaction (Gross & John, 2003; Kashdan & Steger, 2006; Moore, Zoellner, & Mollenholt, 2008), while the use of expressive suppression has been shown to increase physiological arousal (Harris, 2001). Similarly, passively accepting a distorted negative image as being an accurate self-representation can maintain the salience of negative social experiences, facilitating rumination and post-event processing (Brozovich & Heimberg, 2008; Rachman, Grüter-Andrew, & Shafran, 2000; Stopa & Jenkins, 2007). These differences in spontaneous types of coping strategies highlight the importance of teaching socially anxious individuals adaptive coping strategies in order to minimize the use of maladaptive strategies that may amplify the symptoms of anxiety. Accordingly, in the present study, we aimed to teach socially anxious individuals to cope with negative image intrusions by mentally morphing the negative features of their images into more positive ones. As such, they were trained to apply the same active strategy that non-socially anxious individuals report using spontaneously when negative images intrude (Moscovitch et al., 2013).
The present study
We aimed to test the effectiveness of imagery morphing in comparison to supportive counseling (SC), a nonspecific therapy control condition in which participants were provided with empathy and support but no specific imagery coping strategies. Participants included a clinical sample of individuals diagnosed with SAD and community controls, all of whom completed (a) an initial training session in the laboratory, (b) 1 week of daily homework assignments in which they practiced using their strategy, and (c) an in-lab speech task approximately 1 week after their initial training session, in which they were given an opportunity to implement their strategy within a stressful social context. The effectiveness of the morphing strategy was assessed by comparing self-report ratings of positive affect, negative affect, and self-perceptions during the speech task across the two conditions.
Method
Participant characteristics
The sample for this study consisted of individuals whose symptoms met DSM-5 criteria for a current clinical diagnosis of SAD, as well as individuals without a history of significant mental health concerns who served as the comparison sample of healthy control (HC) participants. These community participants were recruited from a Canadian city with a population of approximately 120,000 as part of a collaborative anxiety disorders research group run through the University of Waterloo (see Moscovitch et al., 2015). All study procedures were approved by the University of Waterloo’s Human Research Ethics Board. A total of 71 individuals participated in the present study. All of the participants who completed the training session also completed the speech task approximately 1 week later.
From the 71 individuals who completed both in-lab sessions, four participants were excluded from analyses for failure to comply with experimental instructions. Additionally, 12 participants were excluded from analyses because they denied experiencing a mental image in anticipation of the speech task. Therefore, the final study sample included in all analyses consisted of 55 individuals (28 SAD and 27 HC). Within the SAD group, the mean age was 28.88 years (standard deviation (SD) = 10.10) and 67.9% of participants were female. Approximately, 57.1% of participants identified as White, 17.9% identified as Asian (e.g., Chinese, Japanese, and Korean), 10.7% identified as Latin American, 10.7% identified as “other,” and ethnicity data were missing for 3.6% of participants. Within the HC group, the mean age was 31.16 (SD = 15.60) and 70.4% of participants were female. Approximately, 70.4% of participants identified as White, 22.2% identified as Asian (e.g., Chinese, Japanese, and Korean), 3.7% identified as Arab, and 3.7% identified as South Asian (e.g., East Indian, Pakistani); there were no missing ethnicity data in the HC group.
Diagnostic assessment
All potentially eligible participants were administered the phone screen for the Mini International Neuropsychiatric Interview (MINI; Sheehan, 2014), which is a well-validated semi-structured diagnostic interview capable of capturing the presence or absence of any essential symptoms that would meet DSM diagnostic criteria (American Psychiatric Association, 2013; Pinninti, Madison, Musser, & Rissmiller, 2003; Sheehan et al., 1998). Participants who did not endorse any psychiatric symptoms on this phone screen were eligible for inclusion in the HC group, whereas individuals who endorsed symptoms consistent with a diagnosis of SAD were invited to complete the entire MINI in-person, administered by a trained clinical psychology graduate student. To augment the diagnostic assessment, this face-to-face interview was supplemented with symptom checklists for SAD, obsessive-compulsive disorder, generalized anxiety disorder, and specific phobia adapted from the Anxiety Disorders Interview Schedule (Brown & Barlow, 2014). Participants whose symptoms met DSM-5 criteria for a principal diagnosis of SAD were eligible to participate in this study, as long as they did not have active and clinically significant suicidality, mania, psychosis, or substance abuse or dependence.
All interviewers received formal training in the DSM diagnostic criteria and were required to reach proficiency in interview administration prior to participation in recruitment. Inter-rater agreement for the principal diagnosis of SAD was 100% when examined between two interviewers who interviewed 10 of the same clinical participants on different days and were blind to one another’s diagnostic impressions. All diagnoses were reviewed for consensus at a weekly meeting that was attended by all interviewers and at least one licensed clinical psychologist. Within the current clinical sample of 28 participants, 20 participants (71.4%) received an additional diagnosis secondary to principal SAD, with 1.32 (SD = 1.16) mean additional diagnoses per participant. The most common additional diagnoses were generalized anxiety disorder (n = 9; 32.1%), persistent depressive disorder (n = 6; 21.4%), and major depressive disorder (n = 5; 17.9%).
Measures
The Social Phobia Inventory (SPIN; Connor et al., 2000) is a well-validated 17-item measure of social anxiety symptoms (Antony, Coons, McCabe, Ashbaugh, & Swinson, 2006), in which items related to problems with social anxiety over the past week are endorsed on a scale from 0 = Not at all to 4 = Extremely. Participants in this study completed the SPIN in the initial study session. This scale demonstrated excellent internal consistency in this study, with Cronbach’s α of .95.
The Depression, Anxiety and Stress Scale–Short Version, depression subscale (DASS-21; Lovibond & Lovibond, 1995) is a valid and reliable measure of depression symptoms (Antony, Bieling, Cox, Enns, & Swinson, 1998), which was used to compare the levels of depressive symptoms across study conditions. The depression subscale asks how much 7 items (e.g., I felt down-hearted and blue) applied to the respondent over the past week, with responses rated on a 4-point Likert-type scale from 0 = Did not apply to me at all to 3 = Applied to me very much, or most of the time. Participants in this study completed the DASS-21 in the initial study session, with Cronbach’s α of .92, indicating excellent internal consistency on the measure in the present sample.
The Vividness of Visual Imagery Questionnaire–short form (VVIQ-short; Reisberg, Pearson, & Kosslyn, 2003) is a 4-item measure, used to assess the richness of individuals’ imagery experiences. The scale asks respondents to visualize a rising sun, and then rate the picture in their mind’s eye with regard to aspects such as clarity and vividness, on a 5-point Likert-type scale. Lower scores indicate greater imagery ability. Internal consistency in the present study was good (Cronbach’s α of .83).
The Positive and Negative Affect Schedule (PANAS; Watson, Clark, & Tellegen, 1988) assesses state affect by asking participants to rate their current feelings in relation to 10 positive mood adjectives (e.g., happy, proud; summed to create the positive affect subscale) and 10 negative mood adjectives (e.g., irritable, ashamed; summed to create the negative affect subscale). All items are rated on a 5-point Likert-type scale ranging from 1 = Very slightly or not at all to 5 = Extremely. This state version of the PANAS was administered at five time points, as described below in the procedure. Across the five time points, the PANAS subscales in the present study demonstrated excellent internal consistency for positive affect (Cronbach’s α ranging from .92 to .96) and acceptable to excellent internal consistency for negative affect (Cronbach’s α ranging from .77 to .90).
The Perception of Speech Performance (PSP; Rapee & Lim, 1992) questionnaire was used to measure participants’ negative perceptions of their own performance on the video-recorded speech task. The measure asks participants to rate how much each of 17 items (e.g., Had a clear voice; Appeared nervous) was true of them during the speech task, on a 5-point Likert-type scale from 0 = Not at all to 4 = Very much. Higher scores indicate more negative perceptions of speech performance. In this study, the scale demonstrated excellent internal consistency (Cronbach’s α of .91).
The Waterloo Images and Memories Interview (WIMI; Moscovitch et al., 2011) was used to assess participants’ mental images. Participants’ verbal descriptions of their images were audio-recorded and subsequently transcribed. A team of six coders was trained to divide each of the participant narratives into separate utterances or grammatical clauses and then classify the valence of every utterance as being positive, negative, or neutral. Coders were first trained to attain at least 80% agreement in categorizing details with an expert coder on a subset of eight narratives that were coded in common by all coders; subsequently, each coder worked independently to code a unique set of narratives.
Study procedure
Participants completed various measures at an initial session, including the SPIN and DASS. Additional measures that were not relevant to the present study were also administered in the initial session, as detailed in Moscovitch et al. (2018). 1 One week after the initial session, participants attended the training session. During the training session, participants were randomly assigned to one of two conditions: morphing or SC. Training was matched in duration across groups, with each lasting 15–20 min. Following the training session, participants were assigned homework in which they were expected to practice their strategy every day and record their practice online. Finally, they returned to the laboratory approximately 1 week after their initial training session to complete the speech task and associated ratings. Complete details of each procedural component are provided below, and a flowchart of the study procedure is presented in Figure 1.

Procedural flowchart. DASS-21 = Lovibond and Lovibond’s (1995) Depression, Anxiety and Stress Scale–Short Version, depression subscale; SPIN = Connor et al.’s (2000) Social Phobia Inventory; PANAS = Watson et al.’s (1988) Positive and Negative Affect Schedule; WIMI = Moscovitch et al.’s (2011) Waterloo Images and Memories Interview; PSP = Rapee and Lim’s (1992) Perception of Speech Performance scale; VVIQ = Reisberg et al.’s (2003) Vividness of Visual Imagery Questionnaire–short form.
Morphing
Participants in the morphing condition were instructed to bring a single negative image to mind and use your imagination in whatever creative way you would like to morph the aversive features of that image into more positive ones. For example, participants who imagined themselves behaving or appearing in ways that would hinder positive social connections or failing to make a good impression on others were encouraged to change the content of these images so that they saw themselves behaving and acting in specific ways consistent with the goal of forming positive social connections with others and making a desired social impression within the situation.
Participants were also encouraged to become attuned to the other people within their images. For example, if in their negative images they visualized other people appearing uninterested or unengaged in the social interaction, they were instructed to morph the images so that the positive version contained other people behaving and acting in specific ways suggestive of being engaged in the social encounter.
Although the instructions urged participants to make meaningful changes, rather than to morph merely perceptual aspects of the image that may have been external to the social situation itself (e.g., lighting in the room), any superficial changes that contributed to making the overall image more pleasant for the individual were permitted. Furthermore, participants were instructed that when the new positive image came to mind, they were to notice all of the possible details in that new image and to experience the new image as vividly as possible.
Participants received one training trial and three practice trials. To assess participants’ adherence to instructions and facilitate participants’ learning of the new morphing strategy, the experimenter probed in between each of the practice trials what, specifically, participants had done within their mind to cope with the negative image. Corrective feedback was provided as needed at each trial.
Supportive counseling
Participants in the SC condition were simply asked open-ended questions encouraging them to share their experiences with mental imagery. For example, conversation prompts included, Tell me about your experiences with mental images in everyday life, How do such images make you feel when they come into your mind?, and What do you usually do when some unwanted mental image enters your mind? The experimenter was trained to listen actively and convey warmth, empathy, and a nonjudgmental attitude. No direct guidance, advice, or suggestions about adaptive coping were provided to SC participants.
Daily homework assignments
All participants were instructed to practice their coping strategy every day during the week between the training session and the speech task. A link to the daily homework task was emailed to participants every morning, and for every day that homework was completed, the participant received an additional entry into a draw that occurred at the conclusion of the study in which they could win one of four cash prizes. The experimenter guided participants through the required homework exercises at the end of the training session, providing instruction on how to complete them and answering any questions participants raised.
For participants in the morphing condition, homework involved recording a brief description of any anticipated anxiety-provoking social situation. Instructions encouraged participants to choose daily situations that varied as much as possible. Participants were asked to close their eyes and bring an image of their situation to mind, and once they had one in mind, to describe how they saw themselves and were feeling within the image through an open-ended text response question. Participants were then instructed to write about how they might apply their coping strategy to this particular image. Then, they listened to a 6-min audio clip that led them through three trials of applying the morphing strategy to this negative image. Afterward, participants were asked to describe what, specifically, they did in their mind to cope with their image through an open-ended text response question.
Participants completing their homework in the SC condition described any mental image that came to mind that day, and answered additional open-ended questions asking about the effects of the image on their behavior in social situations. Participants were also asked whether they perceived the image to be positive or negative, and which strategies, if any, they might use to help cope with this image. If participants reported not experiencing any mental images that day, they were asked to describe any social situations that they anticipate engaging in over the next 24 hr. They were then asked to answer open-ended questions about how they feel when the upcoming social situation comes to mind, how they think the social situation will go for them, and which coping strategies they might use, if any, to cope with the upcoming situation.
In total, homework completion took participants in both conditions about 10–15 min to complete per day. Examples of open-text responses for homework across the two conditions are presented in Table 1.
Examples of homework open-text responses across conditions.

Note. This table presents examples that represent the types of responses provided on the daily homework assignments. In the morphing condition, the prompt was based on what you remember about the imagery coping strategy taught to you in the in-lab session, please describe briefly how you might use that strategy on this new image. In the SC condition, the question was Which coping strategies, if any, might you try to use to help you with this mental image? SC = supportive counseling.
Social stress task
Upon arriving to the lab approximately 1 week after their training session, participants provided baseline ratings of positive and negative affect. Participants in both conditions were aware that they would be asked to engage in a social task during this session but were unaware of the exact nature of the task. After completing baseline measures of state negative and positive affect, participants were informed of the upcoming speech task and completed the second ratings of state affect. They were then instructed to imagine themselves in the upcoming speech task and to become aware of whether or not they experienced a mental image associated with the speech. If an image was endorsed, details about the images were collected using a modified version of the WIMI (WIMI Administration 1). If no image was endorsed, participants were asked to describe to the experimenter what was going through their mind as they anticipated the upcoming speech. Participants who did not report experiencing a mental image prior to the speech were excluded from analyses, as detailed below in the Results section.
After speaking with the experimenter about their images, participants provided third ratings of state affect and were given 1 min to use the coping strategy taught to them in the training session. For participants in the morphing condition, this consisted of closing their eyes and completing the strategy in silence for 1 min, whereas for the SC group, this consisted of a 1-min conversation with the experimenter about mental imagery experiences more generally and how image intrusions affect their social experiences in everyday life. All participants were asked whether or not their original image changed at the end of the 1-min period, and if it did, the modified version of the WIMI was readministered (WIMI Administration 2) in relation to the new image. If the image did not change, the participant went directly into the speech task.
Following the optional administration of the WIMI, depending on whether or not the image changed, all participants completed the 3-min speech task. For this task, participants were instructed to give a 3-min speech about themselves, introducing themselves to the camera as they would to a group of people who do not know them. They were informed that expert raters would later rate the quality of their speech and various other aspects of their performance.
The image that participants reported having in mind immediately prior to the speech task was coded as their “latest image” and taken to be the best estimate of what the participant was holding in mind at the time of the speech task. The “latest” image could have been the participant’s original image that participants endorsed when first hearing about the speech (WIMI Administration 1), if the original image was reported not to have changed, or it could have been an updated version of the image, if the image had changed (WIMI Administration 2). This “latest” image was used as the predictor in analyses examining outcomes associated with holding different types of images in mind.
Immediately after the speech, participants completed the measure of state affect for the fourth time, along with a measure assessing their perceptions of their own speech performance. They were then given a 2-min rest period, to simply sit alone in the room and recover from the speech task. At the end of the rest period, participants provided the final (fifth) ratings of positive and negative affect, as well as the measure of vividness of visual imagery.
Results
Data preparation
Prior to analyses, the data were examined for univariate outliers, defined as SD = 3 above or below the mean. The positive details variable contained one univariate outlier with a value of 25.0, which was, therefore, winsorized to SD = 3 above the mean for positive image details (23.21). The negative image details variable also contained one univariate outlier, with a value of 26.0, which was winsorized to SD = 3 above the mean for negative image details (18.47). Post-speech positive affect, negative affect, and PSP variables did not contain any univariate outliers. Testing for multivariate outliers with a Mahalanobis’ distance of 20.46 as the critical value (df = 6; p = .001) indicated multivariate normality. Finally, one participant had incomplete data for computing the post-speech positive PANAS score, two participants had incomplete PANAS negative affect data, and one participant had incomplete PSP data. These participants were excluded from analyses investigating either positive affect, negative affect, or perceptions of speech performance, respectively, but were otherwise retained in analyses concerning other outcome variables. Means and SDs for all study variables are presented in Table 2.
Means and SDs of study variables.
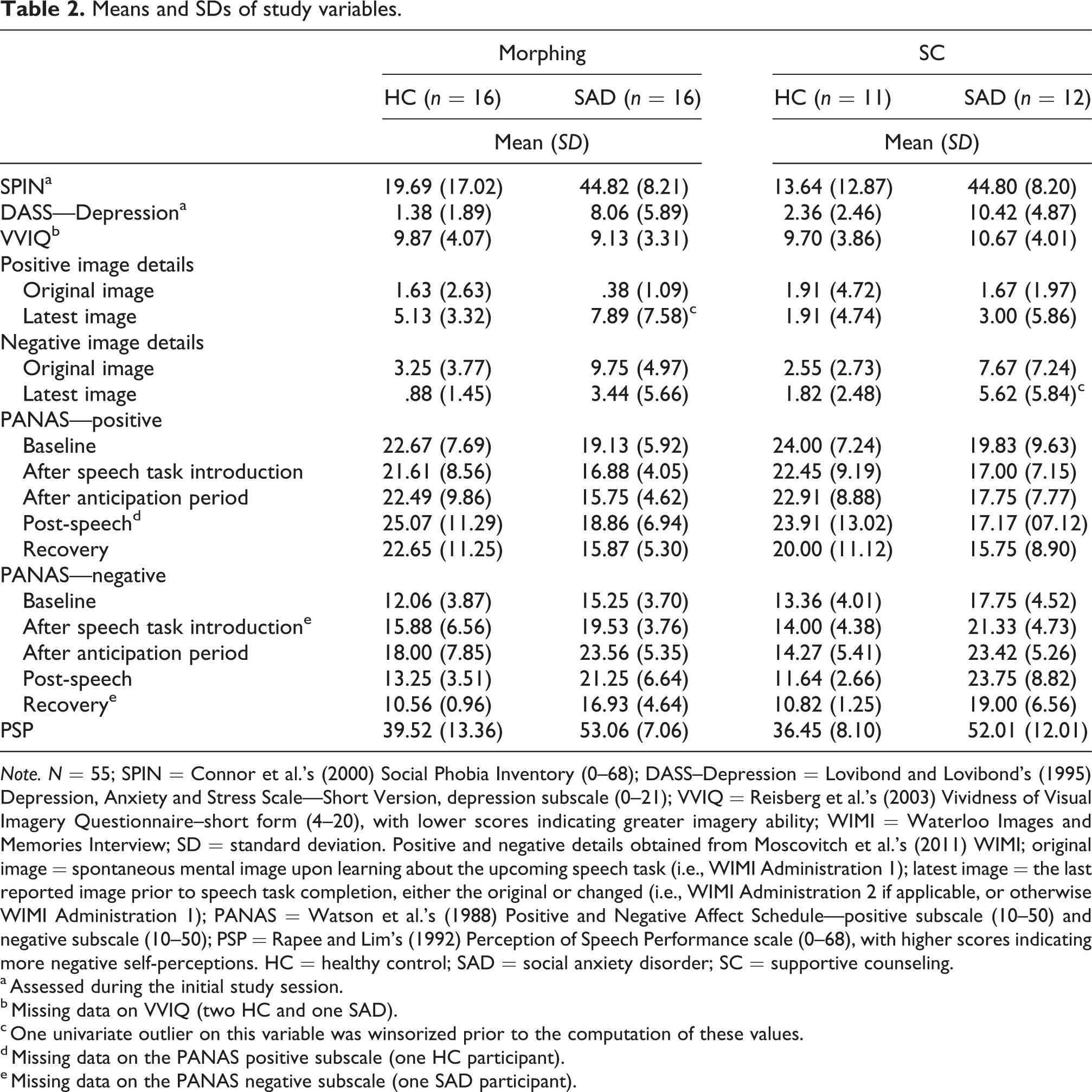
Note. N = 55; SPIN = Connor et al.’s (2000) Social Phobia Inventory (0–68); DASS–Depression = Lovibond and Lovibond’s (1995) Depression, Anxiety and Stress Scale—Short Version, depression subscale (0–21); VVIQ = Reisberg et al.’s (2003) Vividness of Visual Imagery Questionnaire–short form (4–20), with lower scores indicating greater imagery ability; WIMI = Waterloo Images and Memories Interview; SD = standard deviation. Positive and negative details obtained from Moscovitch et al.’s (2011) WIMI; original image = spontaneous mental image upon learning about the upcoming speech task (i.e., WIMI Administration 1); latest image = the last reported image prior to speech task completion, either the original or changed (i.e., WIMI Administration 2 if applicable, or otherwise WIMI Administration 1); PANAS = Watson et al.’s (1988) Positive and Negative Affect Schedule—positive subscale (10–50) and negative subscale (10–50); PSP = Rapee and Lim’s (1992) Perception of Speech Performance scale (0–68), with higher scores indicating more negative self-perceptions. HC = healthy control; SAD = social anxiety disorder; SC = supportive counseling.
a Assessed during the initial study session.
b Missing data on VVIQ (two HC and one SAD).
c One univariate outlier on this variable was winsorized prior to the computation of these values.
d Missing data on the PANAS positive subscale (one HC participant).
e Missing data on the PANAS negative subscale (one SAD participant).
Equivalence of participant characteristics across conditions
Fifty-five individuals endorsed experiencing a mental image in anticipation of the impromptu speech task, leaving a total of 16 HC and 16 SAD participants in the morphing condition and 11 HC and 12 SAD participants in the control condition. Participants in the morphing and control conditions did not significantly differ in terms of social anxiety symptoms, t(53) = 0.46, p = .645, d = 0.13, or depressive symptoms, t(53) = 1.22, p = .228, d = 0.33, as assessed in the initial session, or in their reported vividness of visual imagery ability on the VVIQ 2 (t(50) = 0.690, p = .493, d = 0.19). Moreover, the valence of the coded details in the original image narratives (i.e., for the images that came to mind upon learning about the impromptu speech task) did not differ between the morphing and control conditions (positive details: t(53) = 1.04, p = .302, d = 0.27; negative details: t(53) = 0.82, p = .414, d = 0.22).
Homework completion
Across the morphing and SC conditions, participants completed homework an average of 3.87 (SD = 1.98) times between the two study sessions (morphing: M = 3.81, SD = 1.93; SC: M = 3.96, SD = 2.10). A diagnostic status by study condition univariate analysis of variance (ANOVA) on the number of days homework was completed revealed no main effects of either diagnostic status, F(1,51) = 1.22, p = .275, η2 p = .02, or study condition, F(1,51) = 0.05, p = 824, η2 p < .01, as well as no significant group by condition interaction, F(1,51) = 0.42, p = .520, η2 p < .01, suggesting that participants were similarly engaged in the homework tasks across conditions.
Image manipulation adherence
When asked to apply these skills prior to the speech task, most morphing participants were able to transform their negative image successfully into a more positive version of that image, with 87.5% of SAD and 75.0% of HC participants within this condition reporting that they successfully altered the perceptual features of their initial image to make it a more positive version of that image. Paired t-tests comparing the valence of participants’ original and updated image details within this condition showed that images were indeed changed such that new images contained significantly more positive details, t(25) = 5.58, p < .001, d = 1.09, and significantly fewer negative details, t(25) = 4.65, p < .001, d = 0.91, than the original images. Although not instructed to do so within the SC condition, three HC and five SAD participants reported that they spontaneously changed the perceptual features of their initial images prior to completion of the speech task.
Negative and positive affect
To assess the impact of diagnostic status and study condition on affect within the social stress task session, with the expectation that affect would be more positive and less negative for individuals in the morphing condition, two repeated measures ANOVAs were conducted with diagnostic status and study condition entered as predictors, and positive affect and negative affect across the five measurement points within the follow-up session as the outcome variables. Diagnostic status significantly predicted positive affect, F(1,49) = 5.84, p = .019, η2 p = .11, such that HC participants tended to report more positive affect than SAD participants, and significantly predicted negative affect, F(1,49) = 38.92, p < .001, η2 p = .44, such that HC participants tended to report less negative affect than SAD participants. However, there was no main effect of condition on either positive affect, F(1,49) = 0.01, p = .908, η2 p < .01, or negative affect, F(1,49) = 0.18, p = .673, η2 p < .01. There was also no significant diagnostic status by study condition interaction for either positive, F(1,49) < 0.01, p = .976, η2 p < .01, or negative affect, F(1,49) = 2.21, p = .144, η2 p = .04.
There was also a significant main effect of time when predicting both positive affect, F(2.60, 127.62) = 4.60, p = .006, η2 p = .086, and negative affect, F(2.61, 130.13) = 18.64, p < .001, η2 p = .28, in these models 3 (for means and SDs, see Table 2). Although there were no significant two- or three-way interactions involving time in predicting positive affect (all ps > .250), there was a significant time by diagnostic status interaction (F(2.66, 130.13) = 6.07, p = .001, η2 p = .11) in predicting negative affect. The time by diagnostic status interaction was probed by dependent sample t-tests between time points, collapsed across study conditions, for HC and SAD participants separately. These analyses revealed that, although both HC and SAD participants experienced a significant increase in negative affect in anticipation of the speech task, HC participants experienced a decrease in negative affect from anticipation to post-speech, t(26) = 3.70, p = .001, d = 0.71, that was not observed in the SAD group, t(27) = 0.85, p = .405, d = 0.16. Both the HC, t(26) = 3.29, p = .003, d = 0.63, and SAD, t(26) = 4.77, p < .001, d = 0.92, groups reported a decrease in negative affect from post-speech to recovery.
Perceptions of speech performance
To examine the effects of group and condition on self-perception during the speech task, we ran a hierarchical linear regression analysis, with diagnostic status entered in Step 1, study condition added in Step 2, and the diagnosis by condition interaction term entered in Step 3, predicting post-speech perceptions of performance. Results showed that, as expected, diagnostic status significantly predicted positive perceptions, t(52) = 5.01, β = −.58, R 2 = .33, p < .001, d = 1.41, such that HC participants reported more positive perceptions. However, condition did not significantly predict PSP ratings above and beyond diagnostic status, ΔF(2, 51) < 1.0, ΔR 2 < .01, p = .493, nor was there a significant diagnostic status by condition interaction, ΔF(3, 50) < 1.0, ΔR 2 < .01, p = .741.
Ancillary analyses
In light of the unexpected findings that the morphing strategy in the present study was no more effective than SC, we conducted post hoc analyses in which we explored the potential benefits of holding positive image details in mind prior to speech task completion across both conditions (since both were equally effective in changing all outcome variables across time). The coded number of positive details and the number of negative details for each participant’s last reported image (either the original or changed image, depending on the participant, as explained in the Method section, above) served as predictor variables. In the morphing condition, the latest image was the original image for a total of six participants, and the latest image was a changed image for a total of 26 participants. Conversely, in the SC condition, 15 participants’ latest image was their original image and 8 participants’ latest image was a changed image. We opted to use the last reported image because that was the best available estimate of the mental image participants were experiencing prior to engaging in the speech task.
First, a hierarchical linear regression predicting post-speech positive affect was conducted, with diagnosis, total number of positive image details, and total number of negative image details entered in Step 1, and interaction terms entered in Step 2. All continuous predictors were mean-centered prior to inclusion in regression analyses. In Step 1, results revealed significant main effects of diagnostic status (p = .007) and positive image details (p = .016), and no effect of negative image details on post-speech positive affect (p = .796). Overall, this model explained 20.5% of the variance in post-speech positive affect, F(3, 50) = 4.30, p = .009. The addition of interaction terms in Step 2 explained an additional 8.4% of the variance in post-speech positive affect, ΔF(2, 48) = 2.84, p = .068. In Step 2, diagnostic status remained a significant predictor, such that, overall, HC participants tended to experience more post-speech positive affect than SAD participants, t(48) = 2.35, β = .35, p = .023, d = 0.74. Additionally, there was a significant diagnosis by positive image details interaction, t(48) = 2.04, β = .29, p = .047. To probe the nature of the interaction, the effects of positive image details on post-speech positive affect were assessed at each level of diagnostic status. Linear regression results showed that positive image details significantly predicted post-speech positive affect within the HC group, F(1, 24) = 7.27, β = .48, p = .013, such that participants whose retrieved images contained more positive details just prior to engaging in a socially stressful task reported greater positive affect immediately after the task. However, there was no effect of positive image details observed within the SAD group, F(1, 26) = 2.36, β = .29, p = .137. Therefore, it appears that holding positive images in mind may be less beneficial for SAD participants than HC participants, as far as positive affect is concerned (see Figure 2).

Effects of positive image details on post-speech positive affect. HC = healthy control group, positive affect = 25.88 + 1.34 × number of positive details; SAD = social anxiety disorder group, positive affect = 17.89 + .28 × number of positive details; image details were obtained from participants’ last reported image prior to speech task completion.
We conducted similar hierarchical regression analyses with negative affect and perceived speech performance as the outcome variables. When negative affect was the outcome variable, Step 1 of the model was significant, F(3,51) = 12.13, R 2 = .42, p <.001, but the predictive utility of the model was not improved by the addition of interaction terms, ΔF(5,49) = 0.22, ΔR 2 < .01, p = .801. Although SAD participants generally tended to experience more negative affect than HC participants, t(51) = 5.62, β = −.66, p < .001, d = 1.67, there were no main effects of either positive (p = .839) or negative (p = .772) image details, or any significant interactions (ps > .500). When speech performance was the outcome variable, Step 1 was significant, F(3,50) = 10.01, R 2 = .38, p <.001, but the model did not benefit from the addition of interaction terms, ΔF(5,48) = 0.81, ΔR 2 = .02, p = .452. Although HC participants tended to rate their speech performance more favorably than SAD participants, t(50) = 5.25, β = −.64, p < .001, d = 1.38, again there were no significant effects of either positive (p = .076) or negative (p = .500) image details and no significant interactions (ps > .230) in predicting self-perceptions.
Discussion
The present experimental study was the first to evaluate the effectiveness of imagery morphing for social anxiety. Findings suggested that brief experiential training in the morphing strategy within the lab, followed by subsequent practice through daily homework assignments, effectively equipped participants across the social anxiety spectrum with the knowledge and skills required to alter the content and perceptual features of their negative mental images. Indeed, the majority of both SAD and HC participants were able to successfully morph initial negative images in relation to an impromptu speech task into more positive versions of those images. However, results also indicated that morphing was no more beneficial for participants than SC, at least in relation to measured changes in negative and positive affect and self-perception within the context of an in vivo social stress task conducted a week after initial training. Across conditions, homework adherence ratings were equivalent and indicative of similar levels of participant effort.
Although our data clearly show that it is possible to train people in imagery manipulation strategies aimed at increasing access to positive mental images, they do not provide precise insights into why imagery morphing was no more effective than SC. The data suggest that simply changing the perceptual features of a negative image in order to make it a more positive version of that image is not sufficient to produce meaningful changes in affect and self-perception over and above those that are produced by the nonspecific effects of empathy and support. Extrapolating from previous studies, it is possible that actively reappraising the meaning of a negative image may be critical for such changes to occur, particularly for emotionally vulnerable individuals such as those with SAD. Indeed, effective imagery-based interventions such as IR provide individuals with the necessary tools to challenge and modify the encapsulated meaning of their negative images vis-à-vis the probability and cost of negative social outcomes and how socially anxious individuals view themselves and others (Reimer & Moscovitch, 2015), supporting cognitive behavioral therapy (CBT) models which have long emphasized the need to challenge underlying beliefs associated with images and cognitions in order to bring about meaningful therapeutic change (Hackmann & Holmes, 2004).
Given that negative imagery is often derived from autobiographical memories, the process of memory reconsolidation may also be relevant to our discussion of factors that help to promote effective image manipulations. Research has shown that new meaning about a feared stimulus can be incorporated into long-term memory when new information is presented during the critical window of memory reconsolidation and that information creates a mismatch between predicted and actual outcomes (i.e., prediction error; Ecker, 2015; Fernández, Pedreira, & Boccia, 2017). In other words, effective imagery coping strategies could ideally facilitate new learning by including elements that violate participants’ pessimistic expectancies about the likelihood and costs of negative outcomes. Furthermore, effective image manipulation may depend on eliciting higher levels of affective engagement, as outlined in emotional processing theory (Foa & Kozak, 1986); indeed, new learning appears to be facilitated by affective arousal, which has been posited as a core component of effective exposure to feared stimuli within CBT frameworks (e.g., Hope, Heimberg, Juster, & Turk, 2000; Wells & Papageorgiou, 1998).
The fact that meaningful changes in affect and self-perception did not follow from morphing negative mental representations into more positive ones, over and above SC alone, may be viewed as a potential challenge to the basic premise of Brewin’s (2006) competition retrieval hypothesis. According to Brewin’s influential hypothesis, increased access to positive mental self-representations is essential for therapeutic change, irrespective of whether the content of such representations is modified. In the present study, participants instructed to morph may have either changed superficial aspects of the image (e.g., light in the room) or more personally meaningful features of the image (e.g., an interaction partner’s reaction to what they are saying), but we did not record the specific nature of the changes that were made. Although we encouraged participants to make meaningful changes, we permitted them to make any kinds of changes they wished, including merely superficial or perceptual ones. It is possible that any positive changes to negative images—whether such changes are personally meaningful or merely perceptual/superficial—would only be expected to influence emotional outcomes and views of the self if such changes are perceived by participants as being authentic or believable. Unfortunately, we did not measure the authenticity or believability of participants’ image manipulations in the present study. It is also possible that morphing is only minimally effective as a single session intervention, with small initial effects that are no more powerful than those of SC but with potential to become cumulatively more effective over repeated practice and use.
Another explanation for the observed lack of differences between conditions is that morphing was not taught to participants in the present study in a way that allowed for its full benefits to become apparent in comparison to SC. For instance, although homework adherence in this study was generally good, the daily homework practice was administered by the use of an audio-recording and questionnaires presented online. It may be the case that effective practice of the morphing strategy requires a more structured environment, perhaps with feedback after each practice trial. There was also variability in homework completion among participants, in that participants had the option to either complete daily practice trials on the same image every day or to practice on a different image each day. We posit that structured, in vivo practice with a variety of different images could be more effective at enhancing the skillfulness and efficiency with which the morphing strategy can be applied in future anxiety-provoking situations.
It is also possible that the SC condition was more potent and effective than we expected, thus obscuring any benefits that morphing may have shown in comparison to a completely inert control condition. For instance, although the SC condition did not provide any training or suggestions for how to cope with negative mental images, it could have exerted effects similar to those of the morphing condition by fostering a positive participant–researcher alliance (Laska, Gurman, & Wampold, 2014) or via similar nonspecific therapeutic factors. The presence of such a positive interpersonal alliance, with experimenters who were specifically trained in skills of active listening and elements of supportive dialogue, may be especially important for the population assessed here (i.e., clinically socially anxious). These interactions could have served to directly impact mood because of the pleasant nature of the conversations or to improve affect and self-perceptions by providing direct evidence of social competence and acceptance within the session. Indeed, previous studies have also illustrated the beneficial effects of active control groups such as SC (Mohr et al., 2009; Werner-Seidler et al., 2018).
While the hypothesized differential benefits of morphing relative to SC were not supported, the findings of the current study did support hypotheses related to diagnostic status. Specifically, the results showed that, as expected, HC participants in general reported more positive affect and less negative affect than SAD participants and rated their speech performances more positively. Moreover, collapsed across the morphing and SC conditions, participants whose retrieved images contained more positive details prior to engagement in the speech task reported experiencing more positive affect following the task, but this was only true for HC participants, as a similar association was not observed within the SAD group. Interestingly, across both HC and SAD participants, positive image details did not contribute to decreases in negative affect or more favorable self-perceptions, suggesting a unique relationship between positive image details and positive affect, at least within healthy individuals. Surprisingly, the total number of negative image details, collapsed across study conditions, was not associated with positive affect, negative affect, or perceptions of performance regardless of diagnostic status.
These differential effects of positive image details on the positive affect of HC versus SAD participants, as well as the surprising null effects of negative image details on outcomes, could be explained by unique methodological features of our study. Most prior research on the benefits of holding in mind positive images during a speech task has been conducted with analogue undergraduate samples of socially anxious and non-anxious participants (e.g., Stopa & Jenkins, 2007; Vassilopoulos, 2005). Our findings suggest that the positive effects of holding positive images in mind may diminish at levels of social anxiety above a clinical threshold. On the other hand, calculating image valence by summing verbally reported objectively positive and negative image details gathered through the WIMI is unique to this study and therefore likely also offers unique insights. It may be that the quantitative tally of negative image details is not an accurate representation of how distressing an image is for the affected individual, as certain types of negative details may contribute more to affective experiences and self-perceptions than others, perhaps depending on how personally meaningful they are, the ways that such details are interpreted, and how much they impact affective arousal. Likewise, transitioning from a negative to a positive image may confer more benefit for healthy individuals who perhaps find the task less taxing, as described in more detail below.
Because SAD participants’ initial mental images contained significantly more negative details than HC participants’ initial images, they may have had to work harder to make them positive and the resulting images may have, therefore, been less believable and in turn impactful. For instance, because HC participants had less negative details to begin with, it is also possible that they were primarily targeting mildly negative or neutral image details and making them more positive, whereas SAD participants were tasked with targeting highly negative details and attempting to make them less negative. Because appraising one’s negative images as accurate self-representations is likely to fuel their detrimental impact (Moscovitch et al., 2013), the negative images of those with SAD might have been more tenacious and resistant to the incorporation of positive details than were images of HC participants.
Potential differences in self-beliefs tied to distorted and negative mental images could have also contributed to how SAD versus HC participants approached the imagery manipulation tasks. Indeed, socially anxious individuals tend to have mental images that are personally meaningful and viewed as representing core flaws about themselves (Clark & Wells, 1995), whereas the same might not be true of non-anxious individuals. To this end, the types of details that were targeted by the two groups could have differed in the extent to which they were viewed by participants as being realistically changeable (e.g., changing a frowning face to a smiling face in the crowd vs. changing a critically unattractive projection of the self into more positive self-portrayal within the image).
In addition to methodological features already discussed above, there were several other limitations of this study which must be considered when interpreting the findings and which could help to guide potentially fruitful avenues for future research. For example, the impromptu speech task was highly stressful for many socially anxious individuals, and it is possible that the speech was simply too anxiety-provoking to allow for the use of the morphing strategy to be implemented effectively, especially since training and practice were completed in the absence of any social stress. Future research might examine the effects of morphing on coping with negative image intrusions during more mildly or moderately stressful social situations. Furthermore, it is possible that certain participant attitudes or common factors critical to intervention success have not been assessed here and thus cloud our conclusions. We, therefore, recommend that future research using similar paradigms assess common factors such as therapeutic alliance and levels of motivation, in order to obtain a deeper understanding of factors contributing to coping strategy effectiveness across conditions. Conclusions that can be drawn from these findings are also limited by the fact that we did not assess participant perceptions of their positive images. Therefore, it is unclear to what extent the meaning attributed to a mental image is likely to be critical to its power to exert an emotional effect. It remains possible that morphing was not an effective coping strategy because it did not personally resonate with the participants. Moreover, this study did not assess how subjectively positive or negative the participants’ images were. It is possible that diagnostic status predicted outcomes, whereas condition did not, because HC and SAD participants interpreted similar types of objective image details in discrepant ways. Such divergent appraisals of identical details would not be captured in our paradigm, which made use of independent raters coding the objective valence of image details. Finally, an important limitation of the present study was its relatively small sample size. Within the context of the small sample size, however, we focused on the interpretation of effect sizes, which did not suggest that larger samples would have changed the observed pattern of findings or the conclusions drawn from such findings.
In sum, the current study explored the possibility of training individuals with SAD to use an imagery morphing strategy to improve access to positive mental images within anxiety-provoking social contexts in which negative images intrude. While results indicated that participants could be trained to morph their negative mental images into more positive ones, simply conjuring up positive images in the absence of imagery reappraisal may not improve people’s abilities for coping with social stress, at least in comparison to SC. Future research should explore the facets of positive imagery that are likely to facilitate coping benefits for socially anxious individuals within challenging social contexts.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was undertaken thanks to funding awarded to the third author from the Canada Research Chairs Program, the Social Sciences and Humanities Research Council of Canada, and the Canadian Institutes of Health Research.