
Abstract
An ever-growing number of transdiagnostic processes that maintain psychopathology across disorders have been identified. However, such processes are not consistently associated with psychological distress and symptoms. An understanding of what makes such processes pathological is required. One possibility is that individual differences in rigidity in the implementation of these processes determine the degree of psychopathology. The aim of this article is to examine the relationship between rigidity/flexibility and transdiagnostic maintenance processes. Initial searches were made for research examining relationships between 18 transdiagnostic processes and rigidity/flexibility. Relationships between rumination, perfectionism, impulsivity and compulsivity, and rigidity/flexibility were systemically reviewed; 50 studies met inclusion criteria. The majority of studies indicated that transdiagnostic cognitive and behavioral maintenance processes and rigidity were correlated, co-occurring, or predictive of each other. Findings are consistent with the hypothesis that it is inflexibility in the manner in which processes are employed that makes them pathologically problematic. However, further research is required to test and establish this.
Convergent evidence from genetic, neurophysiological, personality, and cognitive–behavioral research suggests that current diagnostic categories do not precisely specify the factors that cause and maintain psychopathology (Buckholtz & Meyer-Lindenberg, 2012; Morris & Cuthbert, 2012; Rössler, 2013). Numerous reviews have identified cognitive and behavioral processes that maintain psychopathology across disorders (Harvey, Watkins, Mansell, & Shafran, 2004; Nolen-Hoeksema & Watkins, 2011). These are termed transdiagnostic processes.
An important narrative review of the flexibility literature (Kashdan & Rottenberg, 2010) has made a strong case that it is the ability to flexibly adapt responses, in order to meet situational demands and personal goals, which could be the key contribution that flexibility makes to well-being. Yet, Kashdan and Rottenberg’s review did not systematically review research relating to the relationship between rigidity/flexibility and cognitive–behavioral processes. Furthermore, the authors suggested that additional work was necessary to integrate the different facets of flexibility. To indicate the difference between the studies reviewed in their review and the current review, only seven studies were included in reference list of both. Earlier reviews have also found it difficult to integrate the facets of rigidity (Chown, 1959; Schultz & Searleman, 2002). The current review offers a theoretical account of how the constructs of both rigidity and flexibility could be integrated. Our review is further informed by reviews that indicate that rigidity and flexibility are transdiagnostic processes (e.g., Robinson et al., 2006; Snyder, Miyake, & Hankin, 2015; van Holst, van den Brink, Veltman, & Goudriaan, 2010).
Although considerable research evidence is available for whether a particular cognitive–behavioral process is transdiagnostic or not, attempts to explain how such processes relate to each other are much less common. Further, there is increasing evidence that a number of transdiagnostic processes are associated with psychological distress only in certain contexts. We propose that the feature of these processes that is responsible for maintaining distress is the rigid or inflexible way that they are applied. We introduce perceptual control theory (PCT; Powers, 1973) as a framework to explain how and why rigidity may have this role. The first step in testing this proposal is to review broad neuropsychological, clinical, and personality research to establish whether measures of transdiagnostic processes are related to measures of rigidity and inflexibility. Showing correlations between rigidity/flexibility and transdiagnostic processes is a necessary but not sufficient step to establishing whether these processes, when applied rigidly, lead to psychopathology. The current review includes a number of studies examining correlational, predictive, and interaction relationships, using a variety of experimental paradigms and both clinical and nonclinical participants. These diverse methods of assessing rigidity and of transdiagnostic processes make it unlikely that correlations are purely based on circumstantial method variance of individual measures.
To introduce the review, we define transdiagnostic processes, rigidity, and flexibility. We then summarize the evidence that transdiagnostic processes are not consistently associated with psychological distress. Finally, we introduce an explanatory PCT framework. Figure 1 provides a diagrammatic overview of the hypothesized model presented within this article.
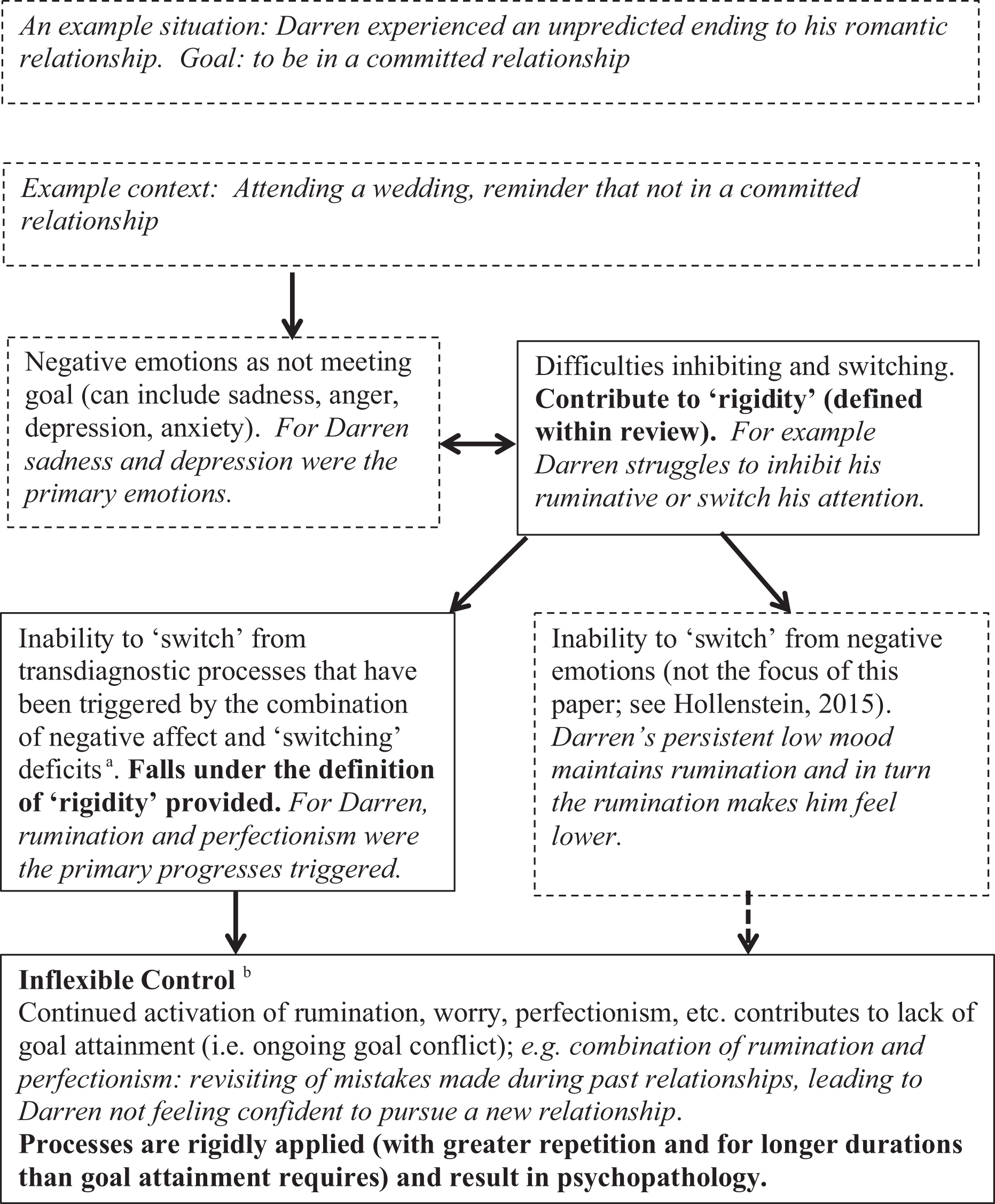
Overall model presented within the article, using an example. Notes. (1) Solid boxes indicate the relationships that this article primarily focuses upon. Dashed boxes provide overall context of the model. The example is italicized. (2) For the purpose of simplicity, feedback and bidirectional arrows are not used. But it is acknowledged that there will be additional feedback relationships as dynamic interactions involve constant feedback processes (Powers, 1973); for example, continued perfectionist rumination is likely to maintain negative affect (Di Schiena et al., 2012; Randles et al., 2010). aIt is recognized that inhibition deficits will also contribute to rigidity and inability to disengage from transdiagnostic processes. But (as discussed in the “The definition and measurement of rigidity and flexibility” section) it can be useful to separate these two constructs and the current review focuses more on switching. bThis construct is an aspect of arbitrary control (described in the account of PCT in the review introduction) but specifically focuses on instances where continued employment of a process prevents goal attainment and maintains internal conflict. PCT = perceptual control theory.
The definition of a transdiagnostic process
A cognitive or behavioral process is defined as “an aspect of cognition (e.g. attention, memory, thought, reasoning) or behavior (e.g. overt or subtle avoidance) that may contribute to the maintenance of a psychological disorder” (Harvey et al., 2004, p. 14). It is recognized that the terminology of “styles” could be used for some of the “processes” reviewed; for example, “ruminative response style” can be used to indicate the repetitive nature of this process (Nolen-Hoeksema & Morrow, 1991) and perfectionism can be described as a style or a process (Egan, Wade, & Shafran, 2011). However, the term process is preferred in order to focus on proximal and contextual factors that can affect a specific episode of any of the processes reviewed (Roberts, Watkins, & Wills, 2013). A transdiagnostic process is defined as a cognitive or behavioral process that contributes to the maintenance of symptoms of psychological distress across a wide range of psychological disorders.
The definition and measurement of rigidity and flexibility
Conceptualizing rigidity and flexibility has proved difficult (Chown, 1959; Kashdan & Rottenberg, 2010; Schultz & Searleman, 2002). We briefly review some key ways in which these constructs have been conceptualized. We then consider definitions based on the extant literature.
Within the neuropsychological and neurobiological literature, rigidity is often defined in terms of a difficulty in switching from one set way of responding to a different way of responding and can be synonymous with set/task-switching difficulties. Flexible cognitive control is comprised of a number of aspects including “…the inhibition of unwanted habitual or impulsive responses” and “the rapid updating and flexible switching of goals and behavioral dispositions…” (Goschke, 2014, p. 44). Therefore, flexibility encompasses both inhibiting inappropriate goals and switching tasks to respond to changing demands (Meiran, 2010; Miyake et al., 2000). Task-switching and inhibition can be conceptualized as relatively independent processes and some paradigms measure these specific components (Meiran, 2010; Whitmer & Gotlib, 2012). However, commonly theoretical accounts emphasize that the functions of switching and inhibition are highly interrelated (Koch, Gade, Schuch, & Philipp, 2010), with empirical data supporting this (Friedman & Miyake, 2004). 1 Therefore, it has been suggested that such executive functions (EFs) exhibit both unity and diversity, that is, different components correlate (suggestive of a common underlying process) but also show separability (diversity) (Miyake et al., 2000; Miyake & Friedman, 2012).
Factor-analytic methods have been used to extract common and specific aspects of executive functioning (Friedman et al., 2008; Miyake & Friedman, 2012). Switching and inhibition are correlated at the latent level, but this variance is accounted for a common EF factor (Friedman et al., 2008). Further, at the latent level, inhibition is fully accounted for the common EF factor. The common factor is hypothesized to be the ability to maintain task goals in working memory and use them to direct behavior (Miyake & Friedman, 2012). Importantly, research indicates that common EF and switching-specific components can show opposing patterns of correlations (Altamirano, Miyake, & Whitmer, 2010; Friedman, Miyake, Robinson, & Hewitt, 2011) and, therefore, indicate that switching and common EF should be considered as separate (albeit interrelated) processes. Snyder et al. (2015) provided a review of this area.
A key, comprehensive review included a meta-analysis of three measures of rigidity and presented a definition (Schultz & Searleman, 2002). Based on this, and more recent conceptualizations of task sets within neuropsychological literature (e.g., Meiran, Kessler, & Adi-Japha, 2008; Miyake & Friedman, 2012), we define rigidity as “the tendency to develop and perseverate in particular cognitive or behavioral patterns, and such patterns being continuously employed in situations where the pattern is no longer effective.” 2 For example, Rachel worries about her performance at work and tries to do her best to get her work perfect. She carries on perfecting work even when it means she does not meet a deadline in time. Rachel’s perfectionism enables her to produce work of a high standard, but she persists in perfecting her work even when this means that she does not meet a deadline and, therefore, is no longer working effectively.
A longstanding debate within rigidity literature is whether rigidity is a dispositional trait or a task-specific phenomenon observable under certain conditions (Chown, 1959; Schultz & Searleman, 2002; Stewin, 1983). In line with Schulz and Searleman (2002), the definition given incorporates both dispositional and context-specific explanations of rigidity. It is noted that for rigidity to be pathologically problematic, some degree of temporal stability is likely, even if this is also task and context dependent (Schultz & Searleman, 2002). For example, a parent worrying about their child’s education might help them clarify how best to support their child. However, if they keep worrying about this when they have put all the possible supports in place (a change in context that means that this no longer meets their goals), then this would be considered rigid. This is in line with a review of the literature that indicated that expression of a personality trait could vary as a function of context (Ferguson, Heckman, & Corr, 2011; Mischel & Shoda, 1995; Roberts, 2009), that is, even if rigidity was “trait like” (i.e., temporally stable), it would not manifest in all contexts. In a similar vein, it is also proposed that an individual could display rigidity in certain behavioral processes, but not in certain cognitive processes. To return to the example given earlier in this paragraph, of the parent worrying about their child’s education, the parent might not persistently and excessively worry about their own work or even about their child’s social relationships. This will be determined by the goals that are important to them; for example, they might value education more highly than their child having a lot of friends.
Following from the definition of rigidity given and with reference to the review by Kashdan and Rottenburg (2010), flexibility is defined as “despite an individual having formed a particular cognitive/behavioral pattern of responding to a specific situation they are able to disengage from this initial pattern if the initial pattern of responding is no longer effective for the specific situation.” For example, Mumtaz has recently lost her mother and is experiencing a lot of sadness. While she is at work, she suppresses thoughts of her mother and appreciates being able to focus on her work; however, when she speaks to friends and attends a support group, she appreciates being able to fully experience and express her sadness. She is able to disengage from suppression of sadness within situations where it is not effective. Although not specifically emphasized in this definition, the authors propose that effectiveness of a given pattern of responding for an individual in a specific situation is determined by the individual’s goals (Kashdan & Rottenburg, 2010). 3 This is discussed in more detail in the section introducing the PCT-informed conceptual framework.
Throughout the review, the terms rigidity and flexibility will be used. However, rigidity is considered synonymous with inflexibility. One of the difficulties in providing a consistent account of rigidity and flexibility is that flexibility can be considered interchangeable with switching abilities within the neuropsychological and neurobiological literature (e.g., Kehagia, Murray, & Robbins, 2010; Remijnse et al., 2013). However, flexibility in the clinical literature is often defined in terms of how effective a response is, that is, whether it involves switching from processes that are not in accordance with an individual’s values/goals and can also encompass persisting with processes that are consistent with individual’s goals. For example, the term is used in this way within acceptance and commitment therapy (ACT; Hayes, Strosahl, & Wilson, 1999) and relational frame theory (Hayes, Luoma, Bond, Masuda, & Lillis, 2006), some theoretical accounts of mindfulness (e.g., Shapiro, Carlson, Astin, & Freedman, 2006), and some CBT accounts (e.g., Dennis & Vander Wal, 2010). Although evidence suggests that effective switching results in greater flexibility (e.g., Snyder et al., 2015), there is a difference between the two conceptualizations described. This issue and a potential solution will be outlined within our conceptual account (the “An integrative PCT framework” section).
What is the relationship between rigidity and flexibility?
The authors’ conceptualization of rigidity and flexibility is that these constructs are on the same dimension and are not conceptually distinct; consequently, the definitions of rigidity and flexibility provided are “mirror images” of each other. Furthermore, the definitions provided emphasize the ability to switch when a pattern of responding is no longer effective.
This conceptualization that rigidity and flexibility are opposite poles of a continuum is not new. Theorists have suggested that the rigidity of thought and behavior seen in many psychological disorders indicates a lack of contextual sensitivity and flexibility (Kashdan & Rottenberg, 2010). Furthermore, in the neuropsychological literature, flexibility and rigidity are generally seen to relate in this way; for example, flexibility is often measured by high ability to switch tasks and rigidity is often measured as low switching ability (Dennis & Vander Wal, 2010; Geurts, Corbett, & Solomon, 2009).
However, some theorists have considered rigidity to be a multidimensional construct rather than a unidimensional construct, with flexibility at the other end (Steinmetz, Loarer, & Houssemand, 2011) and a distinction can be made between “cognitive” and “behavioral” rigidity (Schaie, Dutta, & Willis, 1991; Schultz & Searleman, 2002). It is noted that multidimensional conceptualizations of rigidity are common within the social and personality literature, but not in the neuropsychological literature. For example, Steinmetz et al. (2011) states Presently, it is generally accepted that rigidity should not be considered as a one-dimensional construct with flexibility on the one extreme and rigidity on the other. Rigidity is to be considered as multidimensional in nature with perseverative behaviors in a multitude of personal habits, cognitive sets, and attitudinal sets. (Schultz & Searleman, 2002; also Schaie, Dutta, & Willis, 1991, p. 86)
Further empirical work is required to clarify the exact relationship of these constructs. However, it is suggested that there is no conclusive evidence that rigidity and flexibility are not on a continuum. Even if rigidity is multidimensional, it is possible that each dimension is on a continuum; this could entail a continuum of rigid to flexible behavior, rigid to flexible cognitive control, and so on. Our theoretical rationale for this conclusion is provided in more detail in the section “An integrative PCT framework.”
Transdiagnostic processes are inconsistently related to psychological distress
To illustrate how transdiagnostic processes are established, we provide a summary of research pertaining to rumination and perfectionism, which are two of the processes focused upon in this review.
Rumination was established as a transdiagnostic maintenance process by Harvey et al. (2004), which reviewed the extant evidence to establish whether numerous cognitive and behavioral processes maintained psychopathology across Axis 1 disorders (including anxiety, mood, eating, psychotic, and substance-related disorders). Further reviews have provided additional support that rumination maintains psychopathology in all the disorder clusters aforementioned (Ehring & Watkins, 2008; Nolen-Hoeksema & Watkins, 2011; Watkins, 2015). In addition, rumination predicts the onset of multiple psychological disorders and symptoms, including depression, anxiety, binge eating, and substance abuse (see Watkins, 2015). Perfectionism was established as a transdiagnostic maintenance process for anxiety, mood, and eating disorders by a review in 2011 (Egan, Wade, et al., 2011); this review also indicated that perfectionism prospectively predicts eating disorders, depression, and bipolar disorder. More recent research supports this and indicates that perfectionism may predict anxiety symptoms (Mackinnon, Battista, Sherry, & Stewart, 2014; Mandel, Dunkley, & Moroz, 2015), although findings are mixed as to whether the relationship is prospective or concurrent (Gautreau, Sherry, Mushquash, & Stewart, 2015; Sherry, Richards, Sherry, & Stewart, 2014).
Table 1 provides a summary of transdiagnostic processes and research establishing their transdiagnostic status. (The research described within this table is based on previous reviews and, therefore, is determined by the extant evidence at the time of these reviews; a systematic review of empirical studies would be required to fully update the transdiagnostic status of different processes.) However, there is considerable evidence that transdiagnostic processes, whether behavioral or cognitive in nature, are not consistently associated with psychological distress. We briefly review examples of these in turn.
A list of selected transdiagnostic processes based on previous reviews of research evidence (see source section for the specific reviews used).

Notes. ASD = Acute stress disorder; BDD = Body dysmorphic disorder; GAD = General anxiety disorder; OCD = Obsessive compulsive disorder; PTSD = Post traumatic stress disorder.
All of the above processes have been defined in various ways, where major conceptual differences exist, then multiple definitions have been included. This table is provided as a summary of much more detailed reviews. Subtleties in the research regarding which diagnoses are related to which cognitive and behavioral processes cannot be fully captured (e.g., where results are mixed, it has been necessary to base the judgment to include a diagnosis on whether the majority of methodologically stronger studies support the relationship).
a All processes sourced from Harvey et al. (2004) met their criteria for a “definite transdiagnostic process.” A definite transdiagnostic process is one, whereby “the majority of evidence, which must be at least of moderate quality, indicates that the process is present in all of the disorders in which it has been investigated. As a minimum, the process must have been investigated in four or more disorders” (Harvey et al., 2004, p. 24).
b Egan et al. (2011) state: “For the purposes of this paper, we consider a transdiagnostic process not simply as one which occurs across different diagnoses but also one that is either a risk factor for the disorder or a maintaining mechanism” (p. 2).
c The final four sets of processes: intolerance of uncertainty, impulsivity, compulsivity, and executive and attentional control deficits have not been specifically reviewed using a definition and strategy similar to Harvey et al. (2004). Therefore, a number of reviews and papers are cited to support the claims (made by varied authors) that these are transdiagnostic processes.
Behavioral avoidance can refer to avoidance, or premature leaving, of fear-evoking situations (Harvey et al., 2004). Safety behaviors involve overt or covert behaviors to avoid a feared outcome (Salkovskis, 1991). Although there is considerable evidence that safety behaviors can maintain and exacerbate anxiety (Helbig-Lang & Petermann, 2010), there is increasing evidence that judicious 4 use of safety behaviors does not reduce the effectiveness of exposure therapy for anxiety and, in some instances, actually improves it (Deacon, Sy, Lickel, & Nelson, 2010; Hood, Antony, Koerner, & Monson, 2010; Milosevic & Radomsky, 2008; Rachman, Radomsky, & Shafran, 2008; Rachman, Shafran, Radomsky, & Zysk, 2011). In a recent review, it was suggested that a particular behavior can be more or less functional within a given situation (Helbig-Lang & Petermann, 2010); for example, preparing for a presentation might be functional, yet excessive preparation (commonly seen in social anxiety disorders) can be counterproductive.
Covert behaviors seem to show a similar pattern of findings. For example, emotional suppression is generally positively associated with psychopathology (Aldao, Nolen-Hoeksema, & Schweizer, 2010). However, emotional suppression can also be adaptive, such as choosing to suppress grief at work so that one can achieve the tasks of the day. Indeed, research shows that emotional suppression can predict reduced distress over time (Bonanno, Papa, Lalande, Westphal, & Coifman, 2004; Westphal, Seivert, & Bonanno, 2010). In the same studies, effective emotional expression, which is apparently opposite to emotion suppression, also predicted reduced distress (Bonanno et al., 2004; Westphal et al., 2010).
Further, a comprehensive review indicated that worry is not consistently associated with psychological distress (Watkins, 2008). Similarly, evidence from different research groups suggests that ruminative thinking has adaptive elements (Joormann, Dkane, & Gotlib, 2006; Treynor, Gonzalez, & Nolen-Hoeksema, 2003). In order to explain these findings, several authors have turned to accounts that refer to rigidity; for example, Watkins & Nolen-Hoeksema (2014) propose that one of the aspects that makes rumination pathological is when it becomes habitual and recognize that deficits in attentional control (including inhibition) could result in difficulties in interrupting habits. A seminal review of the role of self-focused attention in psychopathology proposed that it is the rigidity of self-focused attention that maintains distress across disorders (Ingram, 1990). More recently, it has been found that “mind wandering” (attention shifting from an activity toward unrelated inner thoughts and feelings) becomes maladaptive when it becomes a rigid pattern (Ottaviani, Shapiro, & Couyoumdjian, 2013).
Personality style research indicates similar patterns of findings and explanation. For example, perfectionism has been conceptualized as having both adaptive and maladaptive aspects, with evidence to support this distinction (Bergman, Nyland, & Burns, 2007; Bieling, Israeli, & Antony, 2004; Owens & Slade, 2008). However, attempts in clinical samples to differentiate between adaptive and maladaptive perfectionism have not fully supported a categorical distinction (Egan, Piek, Dyck, & Kane, 2011). It has been proposed that whether perfectionism is adaptive or could not be determined by the degree of perfectionism and whether this enables an individual to meet their goals in a given situation (Haase, Prapavessis, & Owens, 2013; Hamachek, 1978; Shafran, Cooper, & Fairburn, 2002). For example, studies indicate that individuals can experience both adaptive and maladaptive perfectionism depending on the domain (e.g., adaptive perfectionism at work, maladaptive regarding physical appearance) (Haase et al., 2013).
There are also more specific empirical findings to indicate that it is the rigid way that processes are applied that maintains distress. Several studies using a range of methodologies have found that people who use a mixture of different coping processes showed less anxiety and depression than those who showed rigid adherence to either problem or emotion-focused processes (Cheng, 2001; Cheng, Hui, & Lam, 2000). Furthermore, individual differences in flexibility of process use are associated with, and predictive of, adjustment in students exposed to trauma and/or stressors (Galatzer-Levy, Burton, & Bonanno, 2012). Even though certain transdiagnostic processes (such as rumination and emotion suppression) are generally associated with psychological distress compared to “adaptive” processes (such as acceptance, reappraisal, and problem-solving), it appears that there is another important difference—the “maladaptive” processes are applied with less variability (Aldao et al., 2010; Aldao & Nolen-Hoeksema, 2012). This suggests that it could be when these processes become more rigidly “default” that they become pathological.
It is important to note that some processes—but not all—are explicitly conceptualized in terms of rigidity and, therefore, are more likely to promote psychopathology. For example, intolerance of uncertainty is defined as a “tendency to react negatively on an emotional, cognitive, and behavioral level to uncertain situations” (Buhr & Dugas, 2009, p. 216). While uncertainty itself can be adaptive (Bar-Anan, Wilson, & Gilbert, 2009; Einstein, 2014), this definition emphasizes a negative reaction to the unpredictable events that will inevitably arise. Consequently, intolerance of uncertainty and intolerance of ambiguity have been conceptualized as aspects of rigidity (Fergus & Rowatt, 2014; Schultz & Searleman, 2002). 5 In such cases, these processes seem likely to lead negative outcomes (i.e., psychopathology, elevated distress). Further, commonly self-report measures of transdiagnostic processes include items that refer to processes being employed repeatedly and excessively. Our review examines whether defining transdiagnostic processes “in terms of” rigidity is appropriate, especially given the less consistent relationship with psychopathology in other domains (e.g., repetitive thinking, perfectionism, emotional suppression).
Overall, the evidence indicates that it is when certain processes are utilized rigidly that they become pathological. Yet, the studies reviewed above have commonly not used established measures of processes that can contribute to rigidity and flexibility (e.g., switching measures). Furthermore, it is necessary to understand how and why such processes are sometimes pathological, for example, so that pathological processes can be treated therapeutically.
An integrative PCT framework
It is important not merely to state that the rigid use of certain processes can result in distress and psychopathology, but to explain how and why this may be the case. Furthermore, a closely specified theoretical account can enable unique predictions. We use a self-regulatory macro-theory, 6 PCT, to provide such an explanation.
Control is a key tenet of PCT. It is seen as a fundamental process and refers to keeping a perception as close as possible to a desired goal (or internal reference; see Figure 2 for the closed “negative feedback” loop that is the basic unit of control within PCT). A full pathway round such as closed loop is necessary to implement the control of perception by behavior. The “reference” or goal refers to a broad range of “personal just rights,” from reference values for a good cup of tea (e.g., milky but strong) to reference values for being a good person (e.g., kind, honest, etc.). It is beyond the scope of this article to provide a detailed account of the evidence base for PCT (see Mansell & Carey, 2009; Marken & Mansell, 2013).
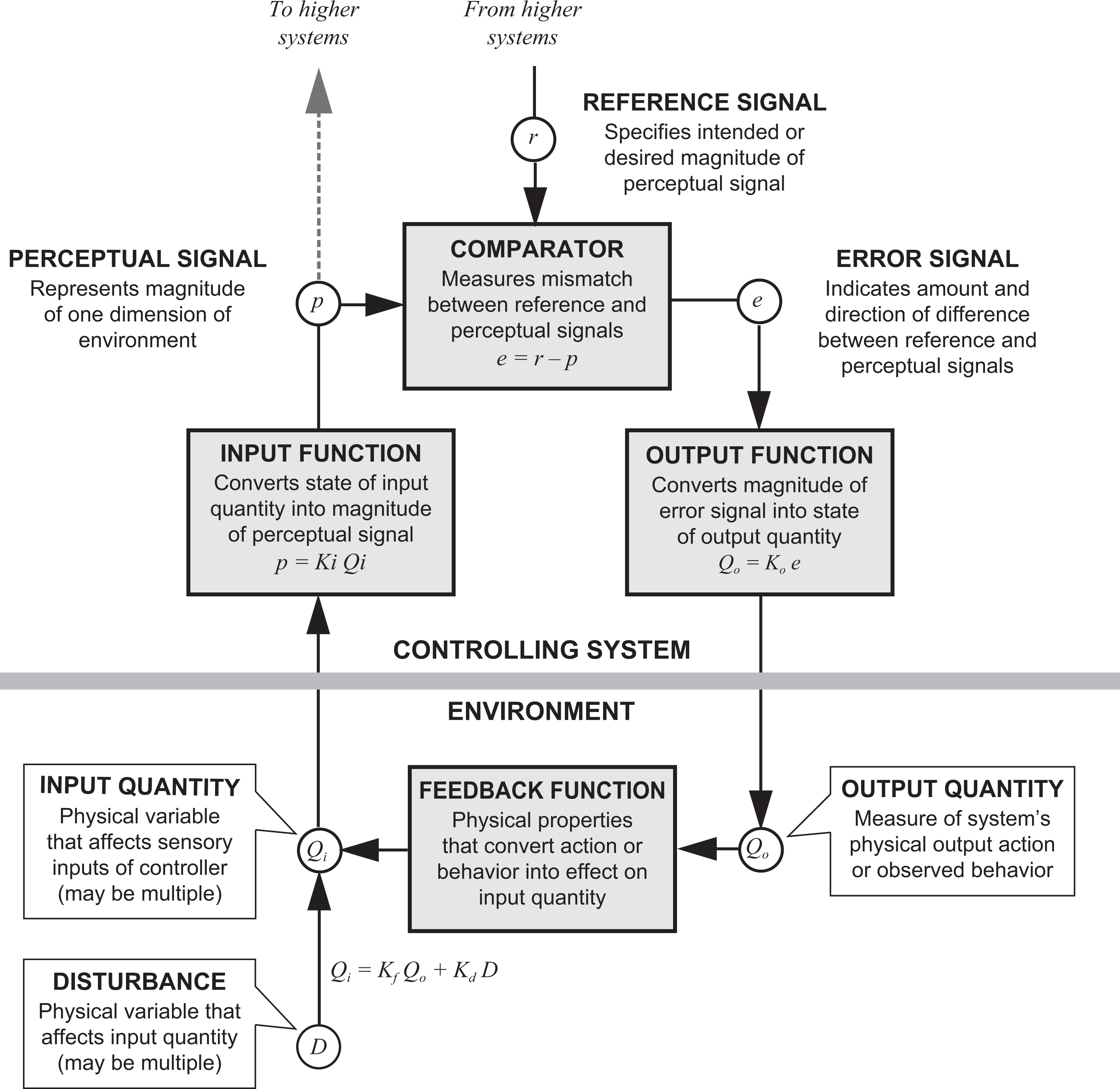
A model of the closed negative feedback loop described in PCT; definitions of key components are included within the diagram and a key is provided below (Redrawn by Dag Forssell from a diagram by William T. Powers). See Powers et al. (2011) for more details. Key: p = perceptual signal; r = reference signal; e = error signal; Qi = input quantity; Q0 = input quantity; D = disturbance; K in each case (Ki , Ko , Kf , Kd ) = a constant converting amount of input to amount of output at each of the indicated points in the loop. PCT = perceptual control theory.
PCT suggests that these internal references are organized hierarchically with higher levels specifying the references for the levels below. Higher level references refer to self-concept and other important references, such as “I want to be a safe” and “I want to be capable.” It is proposed that enduring higher level conflicts between goals undermines control and is associated with distress (Carey, Mansell, Tai, & Turkington, 2014), and this is supported by a recent systematic review of the literature (Kelly, Mansell, & Wood, 2015). For example, a person who has been assaulted in their neighborhood may experience anxiety and indecision about whether to leave the house because they strive to be capable and safe from harm.
A PCT account offers a distinct explanation of when and how particularly rigid forms of control (including habits and psychological processes) lead to distress, by maintaining the goal conflicts described above (Mansell, 2012). Such control is termed arbitrary control (Mansell, 2005; Powers, 1973). Arbitrary control refers to “attempts to make behavior conform to one set of goals without regard to other goals (and control systems) that may already be controlling that behavior” (Powers, 1973, p. 271). Figure 3(a) illustrates how conflict at higher levels of the control system can lead to rigid employment of transdiagnostic processes. It is generally a conscious choice to aim at a particular goal and sometimes this will involve implementing a particular transdiagnostic process, but it is unlikely that it is a volitional goal “to be rigid” or impair other goals. For example, the beginning of ruminative thinking can either arise spontaneously or through conscious choice (Hertel, 2004; Watkins & Nolen-Hoeksema, 2014), as rumination can be perceived to facilitate understanding a situation better or further goal pursuit in other ways (e.g., Kingston, Watkins, & O’Mahen, 2013; Moberly & Watkins, 2010; Watkins, 2004). For this thinking to interfere with goal progress, and therefore to be rigid, it will need to be continued; this can be a conscious or more automatic process (Watkins & Nolen-Hoeksema, 2014). However, the extent to which an individual is able to “switch from” rumination if they realize it is inconsistent with their goals will vary, as switching and inhibition deficits and low mood can contribute to difficulties disengaging (Koster, De Lissnyder, Derakshan, & De Raedt, 2011). So, in this example, the person is not choosing to be rigid, rather they are trying to reduce a behavior (rumination) that is not in line with their goals but are unable to effectively do so.

(a) Conflict at higher levels of the control system leading to rigid employment of transdiagnostic processes and lower level conflict. (b) Resolution of higher level conflict through awareness of the reference that is setting the conflicting goals. Note. The reference “To be myself” sets the references for “To be safe” and “To be normal.” Cognitively, this could be experienced as a realization that both “To be safe” and “To be normal” are valid goals of the self, and a balance can be achieved where both are met. The goals are the same as in Figure 2(a), and the individual is still worrying, but they have greater meta-flexibility (flexibility in meeting all their important goals).
Arbitrary control is more likely to lead to goal conflict and psychological distress, because if one goal is pursued over another, then the second goal will not be met (Brandtstädter & Renner, 1990; Kelly, Wood, & Mansell, 2012). For example, pursuing a goal of “work being perfect” by employing processes, such as repeatedly checking work produced, could become problematic without being able to flexibly balance this with other goals, such as “completing work within time limits.” Thus, rigid implementation of a goal (via a goal-relevant process) 7 is equivalent to pursuing a goal arbitrarily; when this process is implemented without current awareness of the conflict, it causes with other important goals. Such a conceptualization highlights the importance of (1) understanding the overall goal(s) an individual is trying to achieve and (2) establishing whether the transdiagnostic process that they are employing is in service of this goal(s).
There is recognition within the neuropsychological, clinical, and personality literatures that there is a “trade off” between stable goal maintenance and flexible goal adaptation in order for an individual to meet personally important goals (e.g., Brands, Stapert, Köhler, Wade, & van Heugten, 2015; Goschke, 2000; Herd, Hazy, Chatham, Brant, & Friedman, 2014). Although stable stimulus–task associations allow effective responding under equivalent conditions, they can interfere when a new response is required (Goschke, 2000). For example, as rumination can promote maintenance of a certain mindset (stability), it can be adaptive in tasks that require goal maintenance (Altamirano et al., 2010). The capacity to focus attention on one goal, and employ goal-related transdiagnostic processes, can be beneficial in some circumstances (e.g., Brands et al., 2015; Dunne, Coffey, Gallagher, & Desmond, 2014); however, not when this is at the ongoing expense of another important goal (Henselmans et al., 2011). This supports the suggestion that employment of transdiagnostic processes can be described as rigid when it impedes goal progress, as the same process can both facilitate and impede goal progress depending on the context.
PCT predicts a crucial role for awareness in order to reduce rigidity and promote flexibility. Within PCT, the change mechanism, known as reorganization, makes changes to the control system when a conflict between goals (or error) is detected (Powers, 1973). These changes occur at the point that awareness is directed within the control system. Thus, targeted awareness promotes flexibility, and such flexibility would entail acting in a way in which an individual is able to meet all of their important goals and would require awareness of these higher level goals (Morris, Mansell, & McEvoy, 2016).
Therefore, our PCT framework specifically predicts that it is vital to bring awareness to the higher level goals of the individual to establish whether continued employment of a particular process is flexible—is employment of this process in line with all the important goals of the individual? The importance of considering a broad range of goals has been recognized within the neuropsychological literature with a recent article, presenting a neural network model of individual differences in task-switching abilities, suggesting that their model could be enhanced by including an “outer loop” for meta-task goal maintenance (Herd et al., 2014, p. 22). They recognize that individuals have “trained” on range of tasks throughout their life and have goals outside of the current task. This suggests that an individual’s current important goals can influence whether they switch tasks. In line with this, the ability of an individual employ transdiagnostic processes to meet all of their important goals is described as meta-flexibility, in order to distinguish it from task-specific switching processes. The key implication of this term is that switching can be used in a flexible way (to support goal pursuit), but that switching will not always be flexible (will not always promote goal pursuit). Figure 3(b) illustrates how higher level conflict can be resolved through awareness of important goals, and how this can result in more flexible employment of transdiagnostic processes.
This meta-flexibility account is in accordance with the aforementioned conceptualization that there is a “trade off” between stable goal maintenance and flexible goal adaptation (e.g., Goschke, 2000). Both continuing with a task and switching to another task can be adaptive. It is also in accordance with self-regulatory theories, which emphasize the necessity of flexibility in order to meet important goals (Carver & Scheier, 1998; Powers, 1973). For example, both tenacious pursuit of goals and flexible goal adaptation have been shown to promote well-being in some situations and be detrimental to well-being in others (Henselmans et al., 2011; Wrosch, Scheier, & Miller, 2013). Initial evidence suggests that the degree of flexibility with which goals are tenaciously pursued moderates this relationship (Brandtstädter & Renner, 1990; Kelly et al., 2012).
Predictions that can be derived from this explanatory framework are that it is when employment of cognitive/behavioral processes promotes higher level goal conflict that such employment can truly be described as rigid and that people recover when awareness is brought to such higher level conflicts. A number of accounts, including PCT, suggest that “negative” emotions 8 arise in response to perceiving stimuli in order to prepare the individual for action and to meet a goal (Boudreaux & Ozer, 2013; Morris et al., 2016). It has been suggested and evidenced elsewhere that negatively valenced emotions arise and endure when progress toward a goal is impeded (Carver & Scheier, 1998, 2013; Powers, 2005, 2008). Furthermore, it is recognized that negative emotions in themselves can make it more difficult for an individual to achieve their goals and inhibit transdiagnostic processes and, therefore, can directly contribute to rigidity. As shown in Figure 1, the same switching and inhibition deficits that prevent switching from transdiagnostic processes can also prevent switching from and inhibition of negative emotions. For example, considerable evidence indicates inhibition deficits in those who are depressed and particularly difficulties disengaging from negative material and rigid, repetitive rumination (e.g., Joormann, Yoon, & Zetsche, 2007; Koster et al., 2011). However, it is beyond the scope of this review to fully explore the relationship between negative emotion and rigidity; where possible, findings are reported that control for negative affect. The vicious cycle of negative emotions and transdiagnostic processes is broken by opportunities and interventions that broaden the individual’s awareness of their conflicted goals and help them to balance these more flexibly (Alsawy, Mansell, Carey, McEvoy, & Tai, 2014). Direct attempts to test these will require further research, which we return to in the discussion.
A review of the constructive and unconstructive consequences of repetitive thought concluded that a control theory account was the only one that explicitly hypothesized that repetitive thinking could have constructive as well as unconstructive consequences and, therefore, provided the most robust account (Watkins, 2008). Further, a control theory framework has been used elsewhere to explain the contexts in which a process can be both constructive and unconstructive (Egan, Wade, et al., 2011; Mansell, 2012). For example, in order to develop a clearer understanding of the form of perfectionism that maintains psychopathology, Shafran et al. (2002) have suggested a conceptualization of clinical perfectionism. What underlies such pathological perfectionism is whether unobtainable personal goals are rigidly pursued, that is, goals that cannot be obtained and/or that strongly conflict with other important goals (Egan, Piek, et al., 2011). Our use of a PCT framework allows that certain cognitive and behavioral processes are conceptualized in terms of rigidity and, therefore, are more likely to cause conflict and psychopathology. However, given our explicit emphasis that such processes are rigid only when they promote conflict with an individual’s other important goals, a therapist (or researcher) is less likely to assume a particular process is always maladaptive.
Therefore, elaborated control theory accounts can provide a specification of cognitive/behavioral maintenance processes that explains why these can be inconsistently associated with psychopathology (Watkins, 2008). In summary, this specification is that effective self-regulation requires flexible coordination between different levels within the goal hierarchy in order to meet valued goals (Carver & Scheier, 1998; Powers, 1973; Watkins, 2008). This entails responding to the contextual demands of different circumstances, that is, the employment of the most appropriate level within the goal hierarchy to meet the current task demands and the employment of correspondingly appropriate cognitive/behavioral processes (Watkins, 2008). However, such accounts do not specify that difficulties in switching (or inhibiting previously relevant task set) could impede appropriate employment of transdiagnostic cognitive/behavioral processes. Consequently, the PCT-informed framework presented here (see Figure 1) proposes that high levels of cognitive flexibility enable an individual to employ a transdiagnostic process (e.g., worry, thought suppression) in a way that ameliorates against their distress and may even have benefits. More specifically for the purposes of the current review, our framework predicts an association between transdiagnostic processes and psychopathology as a consequence of the fact that the existing measures of such processes partly assess the rigidity with which they are applied. This view would be supported by the finding of consistent correlations between transdiagnostic processes and predefined measures of rigidity. This is the purpose of our systematic review.
Aims and hypotheses
As explained earlier, the aim of our review was to systematically examine the relationship between rigidity/flexibility and transdiagnostic processes that maintain psychopathology. We predicted that the majority of studies would find a correlational, or predictive, relationship between the measures of rigidity/flexibility and transdiagnostic processes. Correlational studies will provide evidence as to whether rigidity is commonly related to transdiagnostic processes. Of particular interest and support for the argument presented are studies that describe interaction effects (individuals who score highly on levels of rigidity and highly on levels of maintenance processes exhibit greater psychopathology) or that indicate that rigidity/flexibility predicts transdiagnostic processes.
Method
The methodology was informed by preferred reporting items for systematic reviews and meta-analyses (PRISMAs) statement (Moher, Liberati, Tetzlaff, & Altman, 2009; see Appendix A). A meta-analytic approach was considered, but it was concluded that this would not be methodologically sound as any aggregation would be difficult to interpret due to heterogeneity in the designs of included studies and measures used (Liberati et al., 2009). Reviewed studies have used decidedly different methodologies and participant groups, and using meta-analytic approaches in such circumstances can mask important differences in findings (Cooper, 2003; Hinshaw, 2009).
Included measures
All measures of rigidity and flexibility that were covered by our definitions were included. Measures of switching and inhibition of task set will be included within the review. Measures of inhibitory processes that promote goal maintenance will not be included within this review. The experimental, self-report, and interview paradigms included are detailed below.
The experimental paradigms that measured switching and inhibition of previous task set were affective shift task, internal shift task, set-shift task, cognitive set shift task (CatBat), task-switching paradigm, Wisconsin card sorting test (WCST; including advanced section), modified card sorting task, negative affective priming paradigm, modified Sternberg task, antisaccade task, trail making test (TMT), Delis–Kaplan EF system TMT, Brixton test, picture set test, haptic illusion task (perceptual shift), and probabilistic reversal-learning task (involves shifting as the stimulus that was previously correct became incorrect, and vice versa). Shifting tasks (including the WCST, picture set test, and Brixton test) involve changing response pattern when a task rule changes; for example, the WCST involves sorting cards according to a rule that participants must ascertain purely from feedback as to whether their selection is right or wrong, the rule changes every 10 cards, and so participants must change their response once the rule changes. The term “task-switching paradigms” is generally used for tasks that involve similar shifting processes but also allow specific measurement of different EFs that may affect performance. Notably, some of the older performance-based measures (e.g., the WCST) involve a number of neurocognitive processes, such as substantial working memory demands (e.g., Hampshire & Owen, 2006; Wildes, Forbes, & Marcus, 2014) and, therefore, should be interpreted with caution.
The self-report measures of flexibility were Acceptance and Action Questionnaire (AAQ)–II and the flexibility subscale of the O’Brien Multiphasic Narcissism Inventory (OMNI). The self-report measures of rigidity were Persistence, Perseveration and Perfectionism Questionnaire (perseveration subscale); Test of Behavioral Rigidity (TBR), Rigidity Questionnaire; and Behavior Rating Inventory of EF—Adult Version (shift subscale). The EATATE interview paradigm was used to measure rigidity (inflexibility and being bound by rules).
It should be noted that self-report and experimental paradigms might measure different aspects of the same construct. For example, self-report measures might reflect a “typical performance,” whereas experimental measures provide greater control and tap performance on a specific occasion(s) (Hofmann, Gawronski, Gschwendner, Le, & Schmitt, 2005). However, both types of study were included so that the relationships of interest could be examined in a comprehensive manner across methodologies. Furthermore, most available studies used a combination of self-report and experimental paradigms.
These measures are diverse and variable in their psychometric properties; for example, a number of these measures have not been cross-validated with other measures of rigidity and flexibility (Chown, 1959; Schultz & Searleman, 2002; Steinmetz et al., 2011). One measure with somewhat variable psychometric properties is the AAQ. The AAQ has a 16-item and a 9-item version, which have both predicted a wide range of outcomes (Bond et al., 2011; Hayes et al., 2006). However, the internal consistency has been low in a number of studies and the factor structure has been somewhat unstable (Bond et al., 2011). Recently, a 7-item AAQ-II has been developed and initial research has demonstrated sound factor structure and good reliability (Bond et al., 2011).
Data sources
Databases utilized in all searches were Embase (from 1974 to November 2014), MEDLINE (from 1946 to November 2014), and PsycINFO (from 1806 to November 2014). Restrictions imposed during searches were to identify studies that (a) were original peer-reviewed research articles, (b) used human participants, and (c) were written in English. For each study included in the review, manual searches of reference lists were conducted. One author was contacted to obtain additional data that were referred to in a study; they were unable to provide the information and the study was excluded.
Study selection
In order to identify the transdiagnostic processes to be included in this review, initial searches of reviews and relevant articles within this area were conducted (see Figure 4). A list of all processes identified in the book by Harvey et al. was compiled (Harvey et al., 2004). This book was the first attempt to review whether a number of cognitive and behavioral processes were common across a range of disorders. All processes they identified as transdiagnostic were included in the initial search terms. Given that this book was published in 2004, and in order to be as inclusive as possible, further transdiagnostic processes were included. Whether a process was considered to be transdiagnostic was determined by similar criteria to Harvey et al. (2004); that a process has been investigated in four or more disorders and the majority of evidence indicated that the process was present within all of these disorders. In addition, intolerance of ambiguity was included due to conceptual similarities with intolerance of uncertainty, despite being under-researched in clinical populations (Grenier et al., 2005). This resulted in a list of 18 processes: all-or-nothing/dichotomous thinking, selective attention/attentional bias, attentional avoidance, elective memory, interpretation reasoning bias, expectation reasoning bias, emotional reasoning bias, avoidance behavior, safety behavior, experiential avoidance, pessimistic attributional style, intolerance uncertainty, intolerance ambiguity, worry, rumination, impulsivity, compulsivity, and perfectionism. All processes that this review mentions in detail are included in Table 1.

Selection of studies.
From this list, a preliminary abstract search was run for each of these 18 processes AND rigidity and for each of these processes AND flexibility. If these two searches generated a total of five or more potentially relevant papers, based on the abstract only, then the style was kept in the review. A paper was deemed appropriate in this regard if it reported an empirical study regarding associations or causal relationships between a transdiagnostic process and measures of rigidity or flexibility in an Adult Axis 1 disorder sample. Appendix B provides full search terms across all searches.
Based on this process, the transdiagnostic processes searched were selective attention/attentional bias, dichotomous thinking, rumination, worry, perfectionism, intolerance of ambiguity, compulsivity, and impulsivity. The search strategy used was to run an abstract search for studies using one of these processes AND a search term related to rigidity or flexibility. The searches identified 2,682 citations (after de-duplication).
Relevant titles and abstracts were identified against the following prespecified inclusion and exclusion criteria. Articles were included that were written in English and that reported at least one empirical study regarding associations or causal relationships between specified processes and measures of rigidity or flexibility in an Adult Axis 1 disorder sample. Studies using analogue samples were also included when these measured subthreshold levels of transdiagnostic processes (e.g., high rumination). For example, correlational studies, studies investigating predictor variables, or prospective studies were included. Axis 1 disorders were focused upon in line with Harvey et al. (2004) and to keep the scope of the review manageable. Although Diagnostic and statistical manual of mental disorders (DSM-V) does not have axes, all the available research was conducted within previous versions of DSM (American Psychiatric Association, 1994).
Measures were included that measured rigidity/flexibility, and a relevant cognitive/behavioral process, experimentally or by self-report. Measures of switching were included, as were those that measured inhibition of previous task set, for example, difficulties inhibiting recently relevant information.
Citation searches were conducted on all papers included within the review, plus all examined full texts. Given the breadth of the search criteria in instances when an abstract was clearly not relevant, the full text was not searched; however, for all abstracts whereby potentially relevant tests, relationships or constructs were described that the full text was searched. For example, if an examination of cognitive flexibility was described, but it was not clear whether a relationship with a relevant process was examined, then the full text would be checked for relevance and for relevant citations.
Excluded were studies using nonhuman samples, samples of individuals with brain damage/organic brain impairment, samples of individuals with pervasive developmental disorder, samples of individuals with learning disability, child/adolescent samples (studies primarily with adults but which included data from participants aged 15 and over were included), and studies where participants were under the influence of drugs or alcohol. Appendix A provides an overview of the assessment of study quality.
Results
All tables report overall study design and the specific analysis/analyses used within the systematic review. Where partial eta squared (
Rumination
Eight studies found that rumination was associated with task-switching difficulties using a variety of experimental tasks (Altamirano et al., 2010; Brinker, Campisi, Gibbs, & Izzard, 2013; Davis & Nolen-Hoeksema, 2000; De Lissnyder, Koster, & De Raedt, 2012a; De Lissnyder, Koster, Goubert, et al., 2012b; Koster, De Lissnyder, & De Raedt, 2013) (see Table 2). However, one study found more mixed results on the WCST; depressive brooding was associated with categories completed, but not perseverative errors (Miranda, Valderrama, Tsypes, Gadol, & Gallagher, 2013). Five studies indicated that such switching difficulties in ruminators were more strongly related to difficulties inhibiting previously relevant task set than difficulties in switching task per se (De Lissnyder, Derakshan, De Raedt, & Koster, 2011; De Lissnyder, Koster, Derakshan, & De Raedt, 2010; Meiran, Diamond, Toder, & Nemets, 2011; Whitmer & Banich, 2007). The majority of these studies used the Ruminative Response Scale (RRS; long or short form) to measure rumination (Nolen-Hoeksema & Morrow, 1991; Treynor et al., 2003). 9 The pattern of results has been replicated in a clinical sample (Whitmer & Gotlib, 2012).
Characteristics of studies investigating rumination and rigidity/flexibility.

Notes. ANOVA = Analysis of variance; AST = affective shift task. BDI-II = Beck Depression Inventory-II. IST = internal shift task. MDD = major depressive disorder. RRS = Ruminative Responses Scale. RSQ = Response Styles Questionnaire; WCST = Wisconsin card sorting test. WCST-AS = Wisconsin card sorting test-advanced section. WM = working memory.
Two further studies indicate that rumination is associated with difficulties inhibiting previously relevant information (Owens & Derakshan, 2013; Zetsche & Joormann, 2011). In contrast, in one study, a rumination manipulation interfered with inhibitory processes in the dysphoric group only (Philippot & Brutoux, 2008). However, this study could not clearly differentiate between switching and inhibitory deficits and is also limited by a relatively small sample size (approximately 20 per group).
Emotional material may impact on the degree of impairment, with research suggesting that inhibitory deficits are particularly marked with regard to negative stimuli. Specifically, three studies indicated that depressive rumination predicted deficits in inhibiting negative information (De Lissnyder et al., 2010; Joormann & Gotlib, 2008) and in set-shifting (Koster et al., 2013). Further, Genet, Malooly, and Siemer (2013) found that deficits in affective flexibility predicted increased rumination, but this only applied when participants were switching away from negative material. However, one study has indicated that high ruminators demonstrated more impaired inhibition for both positive and negative words than low ruminators (controlling for depression) (Joormann, 2006).
Overall, findings of the 19 studies in this section suggested that deficits in switching were associated with, and maybe predictive of, ruminative thinking. This supports the hypothesis that rigidity is associated with rumination. In the majority of studies, associations between switching and rumination remained significant when depression was controlled for. A range of paradigms were used to measure switching and inhibition. Six experiments indicated that trait rumination had a greater impact on inhibiting previously relevant task set than non-inhibitory switching processes. Although much of the evidence is from analogue samples, and none of the studies utilized random sampling, there are three studies that report results from clinical populations (generally with depression). Effect sizes are variable from fairly small (r = .18) to large (r = .69).
Perfectionism
In five studies within clinical and nonclinical samples, perfectionism and rigidity were associated (Grilo, 2004; Leyro, Berenz, Brandt, Smits, & Zvolensky, 2012; Lindner, Fichter, & Quadflieg, 2014; Serpell, Waller, Fearon, & Meyer, 2009; Waller et al., 2012) (see Table 3). In two studies, some measures of rigidity and flexibility were correlated with or predictive of perfectionism, but this was not consistent (Tchanturia, Morris, et al., 2004; Wetterneck et al., 2011). In a sample of clients with Obsessive compulsive disorder (OCD), a significant correlation was found between the OMNI Flexibility and Frost Multidimensional Perfectionism Scale (FMPS) doubts about actions subscale; however, no other significant correlations between the FMPS and Flexibility subscale were found (Wetterneck et al., 2011). Childhood perfectionism in individuals with current anorexia, or in long-term recovery, was strongly predictive of performance on the trail making and Brixton tasks (Tchanturia, Anderluh, et al., 2004). However, childhood perfectionism was not predictive of rigidity on the other measures used, although this may reflect the measures, because these involved a range of perceptual, semantic, and other capabilities.
Characteristics of studies investigating perfectionism and rigidity/flexibility.
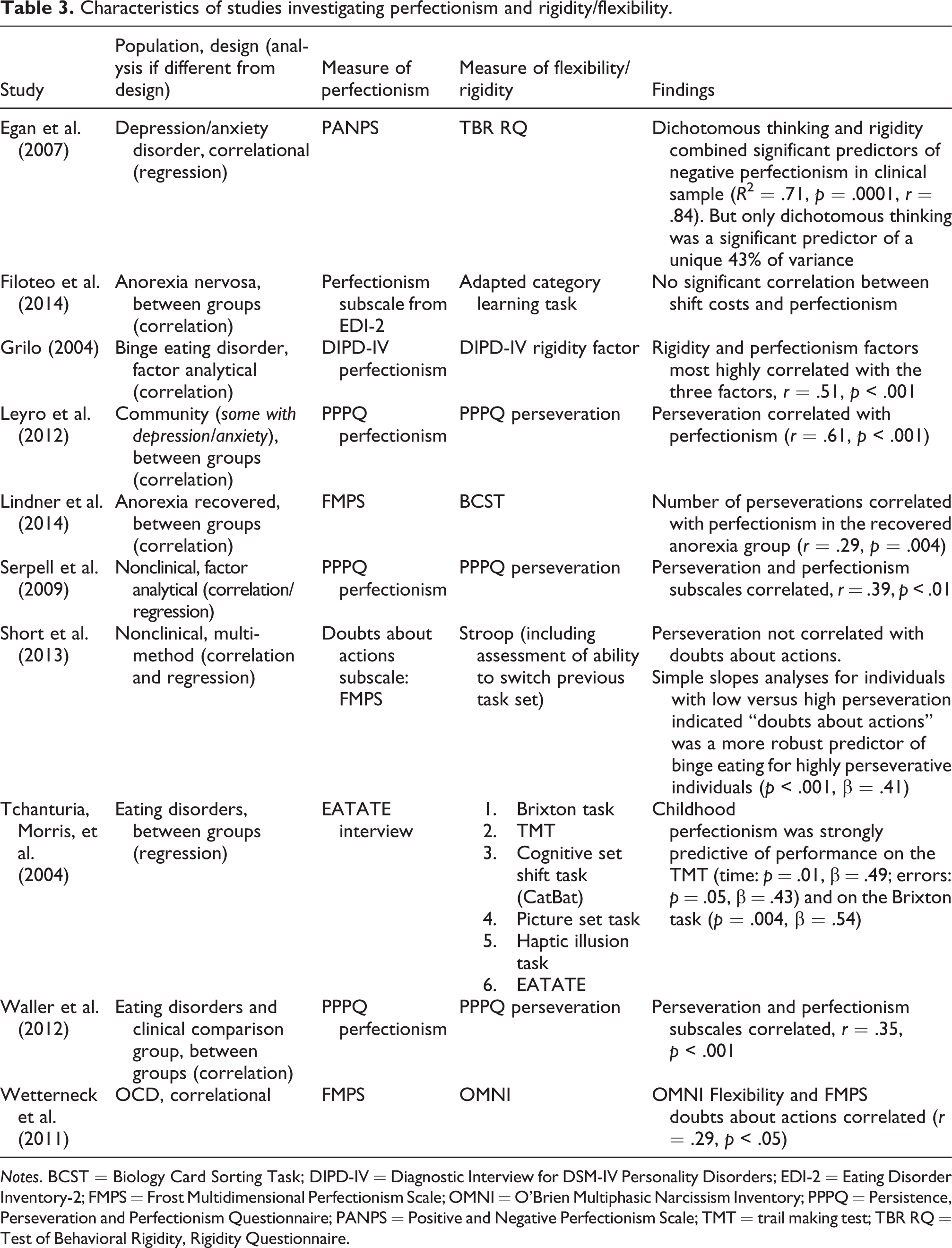
Notes. BCST = Biology Card Sorting Task; DIPD-IV = Diagnostic Interview for DSM-IV Personality Disorders; EDI-2 = Eating Disorder Inventory-2; FMPS = Frost Multidimensional Perfectionism Scale; OMNI = O’Brien Multiphasic Narcissism Inventory; PPPQ = Persistence, Perseveration and Perfectionism Questionnaire; PANPS = Positive and Negative Perfectionism Scale; TMT = trail making test; TBR RQ = Test of Behavioral Rigidity, Rigidity Questionnaire.
Overall, the research within these seven studies supports a relationship between rigidity and perfectionism. However, one study in a clinical sample found no correlation between shift costs and perfectionism (Filoteo et al., 2014). A further study in a clinical sample found that dichotomous thinking and rigidity (assessed by the TBR) combined were significant predictors of negative perfectionism, but only dichotomous thinking was a significant predictor of unique variance (Egan, Piek, Dyck, & Rees, 2007). However, the authors note that the TBR did not seem to adequately capture the clinical construct of rigidity.
Interestingly, Short, Mushquash, and Sherry (2013) found that while the FMPS doubts about action subscale was not correlated with perseveration on the Stroop task, there was an interaction between doubts about action and perseveration. Individuals who scored higher on perseveration and doubts about actions were more likely to engage in increased binge eating; thus these two styles together contributed to increased binging.
Overall, there is some evidence that rigidity and perfectionism are related. In a number of studies, measures of these two constructs were correlated (with r values of .39, .51, and .61). In one study, perfectionism predicted rigidity. However, the findings are preliminary and not totally consistent across measures. Insufficient studies have examined whether inhibition of task set or switching specific difficulties are more strongly associated with perfectionism. None of the studies utilized random sampling.
Compulsive behavior
In two student samples, perseveration/inflexibility was correlated with compulsive behaviors (Lawrence et al., 2006; Zohar, LaBuda, & Moschel-Ravid, 1995) (see Table 4). However, the magnitudes of the correlations were low. In another student sample, the AAQ-II was significantly positively correlated with Obsessive Compulsive Inventory–Revised washing subscale (Abramowitz, Lackey, & Wheaton, 2009). Given that it is stated in this study that the version of the AAQ-II used entails that higher scores indicate greater flexibility (less pathology), the direction of this correlation is surprising. However, it is also stated that AAQ-II is being used to measure experimental avoidance. Therefore, the findings must be interpreted with caution, because if the AAQ-II indicated greater experiential avoidance, then the correlation would be in the direction expected.
Characteristics of studies investigating compulsive behavior and rigidity/flexibility.
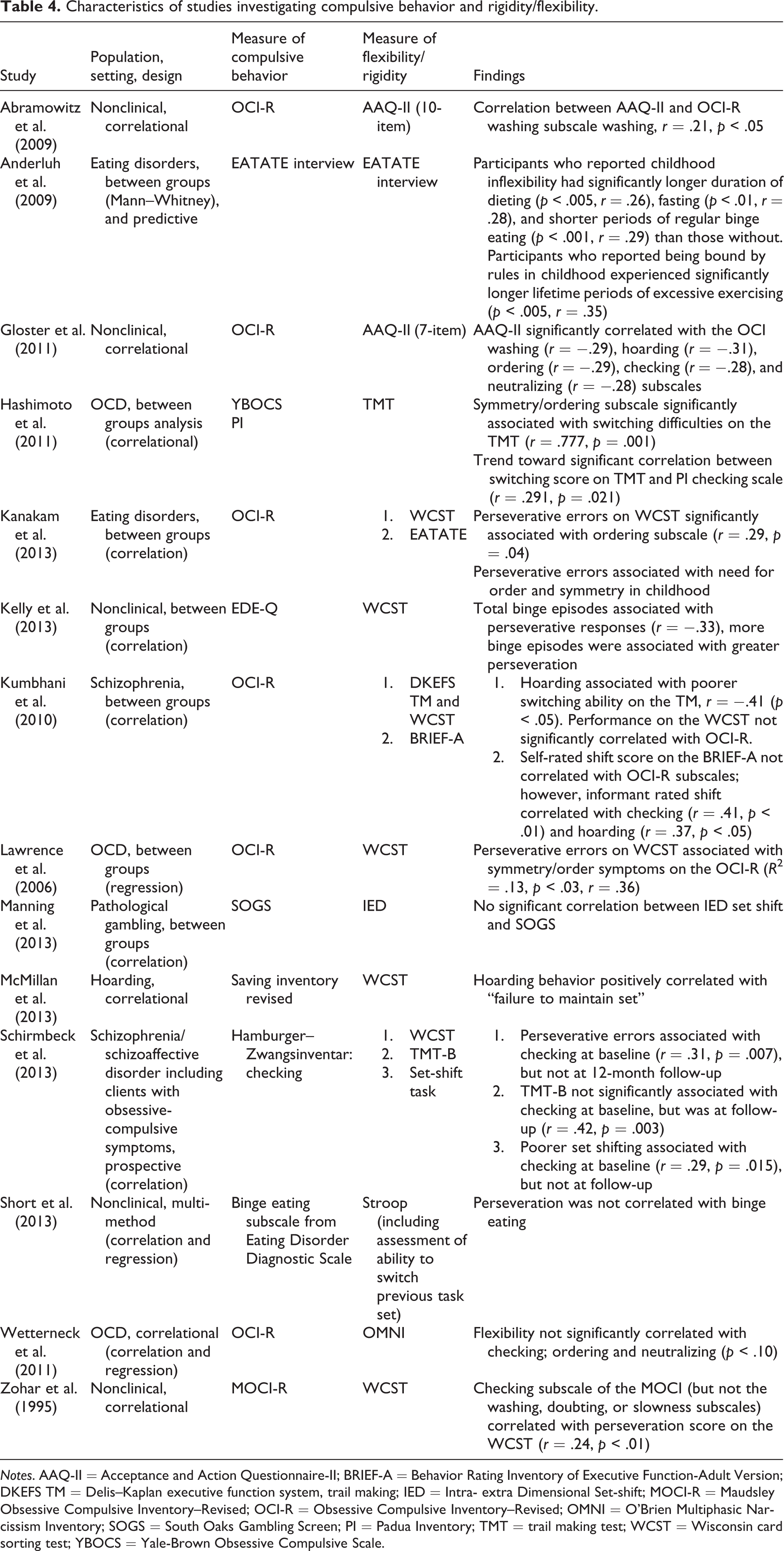
Notes. AAQ-II = Acceptance and Action Questionnaire-II; BRIEF-A = Behavior Rating Inventory of Executive Function-Adult Version; DKEFS TM = Delis–Kaplan executive function system, trail making; IED = Intra- extra Dimensional Set-shift; MOCI-R = Maudsley Obsessive Compulsive Inventory–Revised; OCI-R = Obsessive Compulsive Inventory–Revised; OMNI = O’Brien Multiphasic Narcissism Inventory; SOGS = South Oaks Gambling Screen; PI = Padua Inventory; TMT = trail making test; WCST = Wisconsin card sorting test; YBOCS = Yale-Brown Obsessive Compulsive Scale.
In three studies of clients with OCD, either checking or ordering behaviors were associated with greater rigidity (Hashimoto et al., 2011; Lawrence et al., 2006; Wetterneck et al., 2011). One study was methodologically limited as the sample size for the regression analysis was very low (n = 39), given the number of predictors (12) (Lawrence et al., 2006). In clients with compulsive hoarding, hoarding was associated with perseverative errors and hoarding severity correlated with failure to maintain set (McMillan, Rees, & Pestell, 2013). In addition, a study with clients with schizophrenia and OCD symptoms found that perseverative errors and poorer set-shifting were significantly associated with checking at baseline, but not at 12-month follow-up (Schirmbeck et al., 2013). Conversely, TMT-B was not significantly associated with checking at baseline but was at 12-month follow-up. The majority of these studies support the relationship between compulsive behavior and rigidity. This has been further replicated in a sample of clients with schizophrenia (with no history of OCD); hoarding was associated with poorer switching ability (Kumbhani, Roth, Kruck, Flashman, & McAllister, 2010).
Further three studies of individuals with eating disorders (or eating difficulties) supported the relationship between rigidity and compulsive behavior. A large study investigated the association between rigidity in childhood (indicated by inflexibility and rule-bound traits) and a number of compulsive behaviors (Anderluh, Tchanturia, Rabe-Hesketh, Collier, & Treasure, 2009). Participants who reported inflexibility in childhood had significantly longer duration of dieting and fasting and shorter duration of periods of regular binge eating than participants without this trait. A further study indicated that perseverative errors were significantly positively associated with ordering behaviors and need for order and symmetry in childhood (Kanakam, Raoult, Collier, & Treasure, 2013). In a nonclinical sample, the number of binge episodes was correlated with WCST perseverative errors (Kelly, Bulik, & Mazzeo, 2013).
As aforementioned, Short et al. (2013) found that individuals who scored higher on perseveration and doubts about actions were more likely to engage in increased binge eating; thus, these two processes together contributed to increased binging.
Overall studies provided evidence that compulsive behaviors were associated with rigidity. One study found that rigidity prospectively predicted a range of compulsive behaviors. Across all studies in this area, associations between rigidity/flexibility measures and compulsive behaviors were generally moderate to low. Additional research with clinical populations, which includes interaction terms, would be beneficial.
Impulsivity
The results of studies in this domain were somewhat mixed. Three studies in substance-dependent clients or nonclinical samples found that impulsivity was associated with rigidity (Ersche, Roiser, Robbins, & Sahakian, 2008; Fernandez-Serrano, Perales, Moreno-Lopez, Perez-Garcia, & Verdejo-Garcia, 2012; Van den Broek & Bradshaw, 1993) (see Table 5). However, Salgado et al. (2009) found no significant correlations between the WCST and the measures of impulsivity in an alcohol-dependent group. Another study found that higher impulsivity was associated with greater rigidity but failed to reach significance (Sweitzer, Allen, & Kaut, 2008); group numbers were fairly low at 17–21 per group.
Characteristics of studies investigating impulsivity and rigidity/flexibility.
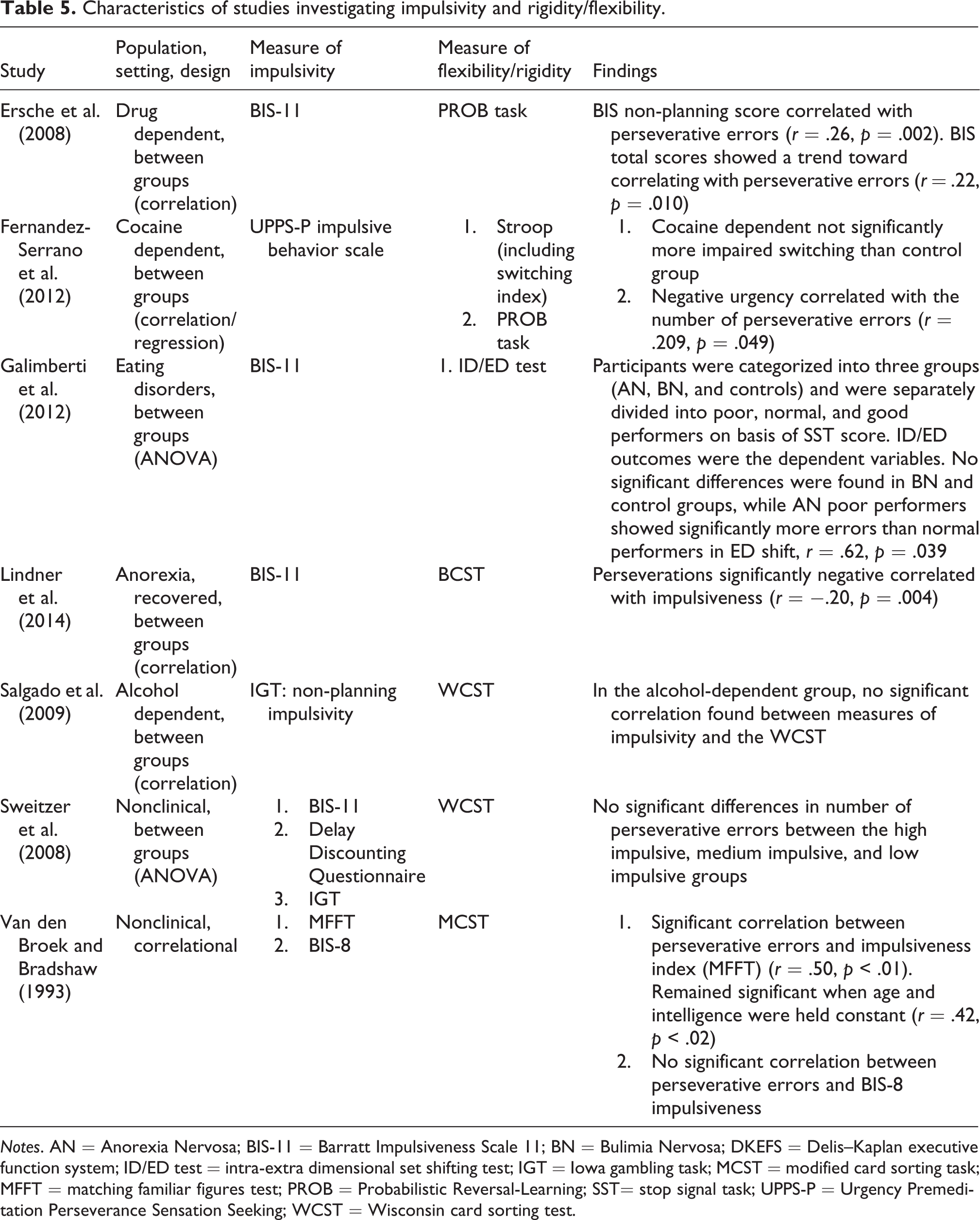
Notes. AN = Anorexia Nervosa; BIS-11 = Barratt Impulsiveness Scale 11; BN = Bulimia Nervosa; DKEFS = Delis–Kaplan executive function system; ID/ED test = intra-extra dimensional set shifting test; IGT = Iowa gambling task; MCST = modified card sorting task; MFFT = matching familiar figures test; PROB = Probabilistic Reversal-Learning; SST= stop signal task; UPPS-P = Urgency Premeditation Perseverance Sensation Seeking; WCST = Wisconsin card sorting test.
Perseverations were significantly negative correlated with impulsiveness in recovered anorexic individuals and controls (Lindner et al., 2014). This was supported by a further study, in which impulsive anorexic clients showed significantly more shift errors than “normal performers” (Galimberti, Martoni, Cavallini, Erzegovesi, & Bellodi, 2012). However, the sample size for this analysis was very low.
Overall, the studies with clinical samples have generally found that impulsivity is associated with rigidity (with r values of .21–.50). Studies using analogue samples provide additional, albeit limited, support that rigidity and impulsivity are associated. Again, the methodological quality of a number of studies is limited, including small sample sizes and lack of random sampling. Fewer studies in this domain used the newer and more precise switching paradigms. For example, few studies used paradigms that could discriminate between difficulties in inhibiting previously relevant task set and difficulties in switching per se. In summary, only a limited number of studies have investigated the relationship between impulsivity and rigidity; however, where both of these are present, they have generally been found to correlate.
Other studies: Selective attention and worry
This section reports the results of two studies: one regarding attentional bias and one worry. Deveney and Deldin (2006) indicated that individuals with major depressive disorder (MDD) performed more poorly than controls on an affective flexibility task when stimuli were negative; one can infer from this that the degree of flexibility was influence by attentional bias.
A study using combination of different measurement paradigms found that cortisol reactivity and task-switching costs interacted to predict worry, but higher task-switching costs alone did not predict worry (Robinson, Ode, & Hilmert, 2011).
Clearly, there is insufficient to be able to draw any conclusions in these domains; however, the study on attentional bias supports earlier studies that found that emotionally salient material could result in greater impairments in switching and inhibition. It would have been useful if these studies examined whether rumination or worry moderated this relationship.
Discussion
In the areas covered by this review, the majority of studies have found a relationship between measures of rigidity and processes that can maintain pathology. Measures of rigidity were correlated with, predictive of (or predicted by), the processes examined. However, whether a significant relationship was found varied somewhat depending on the measures used. Relationships were nearly always in the expected direction, that is, greater rigidity was correlated with, or predictive of, greater levels of the transdiagnostic process (or greater levels of the process were more predictive of rigidity). The majority of studies used switching paradigms to measure levels of rigidity, but rigidity was also used to refer to a broader range of paradigms (e.g., inhibition and self-report measures) (Joormann, Levens, & Gotlib, 2011; Tchanturia, Morris, et al., 2004; Whitmer & Banich, 2007).
This relationship was most consistently significant with regard to rumination and perfectionism. The majority of the 19 studies investigating rumination utilized between groups or correlational designs and nonclinical populations; however, there were two prospective studies. Overall, findings suggested that deficits in inhibition and switching were associated with, and maybe predictive of, ruminative thinking. In the majority of studies, associations between switching and rumination remained significant when depression was controlled for. Different experimental paradigms were used to measure switching and inhibition, but rumination was primarily measured through a limited number of self-report measures. A range of effect sizes were reported, from fairly small to fairly large, but the majority of studies reported medium effect sizes. In the area of perfectionism and rigidity, 9 of the 10 studies reported correlational relationships between the two constructs, using a range of measures. Effect sizes were mostly medium to large.
In the other areas, covered (impulsivity and compulsivity) effect sizes, or the consistency of findings, were lower. The majority of studies found a relationship in the direction expected (with a range of effect sizes). The studies of impulsivity and compulsivity rarely used the more precise switching paradigms, which could contribute to somewhat mixed results.
Does rigid application of transdiagnostic processes contribute to greater psychopathology?
Overall, correlational or predictive relationships were demonstrated and findings point to a statistical overlap between rigidity and maintenance processes, but for measures to be tapping into a single construct, a high correlation value of above .8 would be expected (Evans, 1996). This suggests that while the measures overlap (potentially due to features of rigidity within the measures of maintenance processes themselves), they also include components that may not contribute to the shared variance.
One possibility is our proposal that only a rigid application of these processes contributes to greater psychopathology. The shared variance could represent the common rigidity and the unique variance could represent process-specific factors. However, because impairments in EF are transdiagnostic, correlations between these and the other transdiagnostic processes reviewed could be because both of these are associated with psychopathology. The assessment of symptoms that constitute psychopathology will pick up on the observable or reportable signs of the very processes that are being assessed (e.g., worry, perseverative compulsion). Although not fully addressing this issue, a number of the studies reviewed have included control groups or participants who are not experiencing psychological distress. Furthermore, some studies control for low mood, worry, and other symptoms that could explain some of the variance. In spite of this, the most reliable way to test whether transdiagnostic processes in conjunction with rigidity contribute to psychological distress would be to examine whether the interaction between a transdiagnostic process and rigidity predicts the maintenance and exacerbation of symptoms of psychopathology over time, when controlling for psychopathology at baseline. The authors are not aware of any such studies and this would be a useful area for future research.
If rigidity of application is a key factor in whether maintenance processes are problematic, then it would be expected that individuals who score high on levels of rigidity (or low on levels of flexibility) and high on levels of maintenance processes would be at greater risk of psychopathology. One study demonstrated that the interaction between perfectionism and perseveration contributed to increased binge eating, while perseveration alone did not (Short et al., 2013). Another study (not included within the systematic review) found that inhibition moderated the relationship between impulsiveness and binging/bulimic symptoms, but inhibition alone was not correlated with impulsiveness (Robinson, Pearce, Engel, & Wonderlich, 2009). This study did not measure the inhibition of task-set but indicates that the use of interaction terms could contribute to an understanding of how rigidity and transdiagnostic processes relate. These studies support the hypothesis that transdiagnostic processes in combination with switching/inhibition difficulties are predictive of psychopathology.
Four prospective studies have supported the related hypothesis that inhibition of task set and switching deficits have a causal role in inflexible employment of transdiagnostic processes (e.g., Joormann & Gotlib, 2008). Impaired inhibition predicted Time 2 rumination scores (controlling for rumination and depressive symptoms at Time 1) (Zetsche & Joormann, 2011). Impaired switching at Time 1 moderated the association between stress and increased rumination during a later stressful period (De Lissnyder, Koster, Goubert, et al., 2012). Further, perseverative errors on the WCST predicted suicidal ideation at 2–3 year follow-up, and ruminative brooding mediated the relationship between perseverative errors and suicidal ideation (Miranda et al., 2013). A large study (97 clients with eating disorders) found that participants who reported childhood inflexibility had significantly longer duration of dieting and fasting and shorter duration of periods of regular binge eating than those without; participants who reported being bound by rules in childhood experienced significantly longer lifetime periods of excessive exercising (Anderluh et al., 2009). This study used a self-report measure of inflexibility, and it is interesting that childhood inflexibility was particularly associated with high levels of compulsive dieting and fasting in adulthood, but with shorter duration of regular periods of binge eating. Given that perfectionism has been found to interact with perseveration to predict increased binge eating, this area requires further research (Short et al., 2013). Additional longitudinal studies are required. Overall, these studies provide some support for the model presented in Figure 1. However, they are clearly limited in number, and directions for future research are discussed in more detail toward the end of this section.
Which theoretical frameworks may account for the findings of the review?
These findings are consistent with the PCT explanatory framework proposed, but it was not possible to fully examine specific predictions of the theory based on the available data. Rigid employment of transdiagnostic processes can be problematic because this is more likely to lead to goal conflict; if one goal is pursued over another, then the second goal will not be met (Kelly et al., 2012). As aforementioned, when a particular process is employed in pursuit of a specific goal, it would only become problematic if this process impedes the achievement of another important goal. Therefore, when processes are applied rigidly, that is, repetitively and possibly with limited volitional control, they are more likely to impede goal awareness and attainment (Morris et al., 2016; Teachman, Joormann, Steinman, & Gotlib, 2012).
Specifically, a PCT account would predict that transdiagnostic processes are associated with distress when they maintain conflict between higher level goals. Goal conflict is associated with certain transdiagnostic processes (e.g., rumination and perfectionism), but it is not always specified/examined whether these processes are being applied particularly rigidly or whether higher level conflicts are particularly detrimental (Boudreaux & Ozer, 2013; Emmons, King, & Sheldon, 1993; Martin, Shrira, & Startup, 2004; Mushquash & Sherry, 2012). Overall, this area requires more research, including examination of the relationship between higher level goal conflict, a range of (rigidly applied) transdiagnostic processes, and psychological distress. There are several methods of assessing goal conflict available, which vary in their capacity to assess conflict between higher level goals (see Kelly et al., 2015, for a review). For example, Varese, Mansell, and Tai (2017) used a modified version of the goal task (Dickson & MacLeod, 2004) with additional questions to enable participants to access important superordinate (higher level) goals that related to voices. Ratings of goal interference and facilitation derived from the strivings instrumentality matrix (Emmons & King, 1988) were used to assess higher level goals and their degree of conflict. Yet to date, such assessments of goal conflict have not be included in studies to test whether a transdiagnostic process and cognitive rigidity interact to maintain higher level goal conflict, which in turn mediates the maintenance of psychological distress.
Related to this, measures of switching and inhibition can be used to experimentally indicate rigidity. However, as previously described and indicated in Figure 1, according to our theoretical account, whether a transdiagnostic process is truly being employed rigidly is determined by whether it conflicts with an individual’s goals. Paradigms described in the previous paragraph can be used to measure goal conflict. The paradigm used by Varese et al. (2017) could be adapted so that participants are asked specific questions about why they are using a particular process, and the same procedure could be used to ask about general goals that are important to participants. For example, the internal switch task could be administered to participants with MDD, levels of rumination could be measured with the Response Styles Questionnaire, then the paradigm to enable identification of higher level goals could be used to (1) identify goals related to rumination (e.g., is rumination perceived to help understand problems or perceived to be unhelpful) and (2) overall goals (e.g., overall important life goals, such as being a good parent, getting into a relationship). It would be predicted that the degree of conflict between goals related to rumination and overall goals would mediate levels of depression (higher conflict associated with higher depression). Further, that those with negative appraisals of rumination (as unhelpful) would demonstrate higher switching and inhibition difficulties, because they would not believe that rumination helped them achieve their goals.
The finding that impaired inhibition of previously relevant task set is associated with rumination is consistent with Koster et al.’s (2011) useful “impaired disengagement hypothesis” of depressive rumination. However, it is suggested that this micro-theory is consistent with the broader PCT explanation, as the “impaired disengagement hypothesis” emphasizes how ruminative thought is problematic when it conflicts with an individual’s self-view. For example, self-criticism or negative self-referential thinking commonly undermines the goals of positive self-regard. Further, the account states that, while the internal conflict signal will often promote disengagement from rumination, it is when individuals do not disengage that rumination increases symptoms and can negatively affect functioning (Rawal, Park, & Williams, 2010; Watkins & Moulds, 2005). In line with studies reviewed that indicated valence-specific biases (De Lissnyder et al., 2010; De Lissnyder, Koster, Goubert, et al., 2012; Genet et al., 2013), this account suggests that negative mood may increase the chances of impaired disengagement from rumination (Koster et al., 2011). In accordance with PCT, the “impaired disengagement hypothesis” explains that it is only when rumination causes conflict, and this processing endures, that rumination is pathologically problematic (Nolen-Hoeksema, Wisco, & Lyubomirsky, 2008). Considering this broader explanation suggests that “impaired disengagement” due to impaired inhibition (and impaired attentional control) may promote rumination in a range of disorders, as ruminative thinking is not limited to depressive disorders (e.g., social anxiety disorder, borderline personality disorder, eating disorders) (Baer, Peters, Eisenlohr-Moul, Geiger, & Sauer, 2012; Hofmann, 2007; McEvoy, Watson, Watkins, & Nathan, 2013).
The outcomes of the current review are also broadly consistent with ACT (Hayes et al., 1999). However, these findings do not clearly support the specific tenets of ACT. Psychological inflexibility in ACT “entails the rigid dominance of psychological re-actions over chosen values and contingencies in guiding action; this often occurs when people fuse with evaluative and self-descriptive thoughts and attempt to avoid experiencing unwanted internal events” (Bond et al., 2011, p. 678). Flexibility entails higher levels of acceptance and value-based processes (Hayes et al., 2006) and inflexibility entails lower levels of such processes, including higher levels of experiential avoidance (Bond et al., 2011; Hayes et al., 2006). Support for this account could have been strengthened if a greater number of studies examined the relationship between experiential avoidance and measures that can indicate rigidity. The focus of the current review upon rigidity and flexibility as commonly defined in the psychological, neuropsychological, and neurobiological literature meant that acceptance and value-based processes were not specifically reviewed and, therefore, it is possible that relevant supportive research was missed.
Limitations of the current review
It is necessary to consider limitations of the systematic review strategy used here. Although a broad range of inclusive search terms was used, the authors did not include nonacademic publications or findings of conference abstracts that were not reported in a peer-reviewed journal. Therefore, the review is unable to assess the extent to which publication bias could have affected the findings reported. Furthermore, the systematic study selection was carried out by one author, which could limit objectivity.
The evidence base reported in the current review is preliminary. Measurement issues (e.g., variable psychometric properties, conflation of neuropsychological processes) limit the available literature. Further, this review is deliberately inclusive of a broad range of measures with varying time frames; for example, task-switching paradigms measure processes on the timescale of seconds, whereas mixing costs measure on the timescale of minutes, and self-report can measure various timescales (Meiran, personal communication). Although this is appropriate to the broad hypotheses of the review, it is highly recommended that researchers developing this topic use a more nuanced approach. It is recommended that researchers use more than one rigidity paradigm in order to measure general flexibility rather than task-specific processes (Meiran, 2010; Snyder et al., 2015) and chose paradigms that specifically measure different aspects of executive functioning. A range of EF can be impaired in certain client groups, but it is still important to establish whether this is the case and not to conflate impairments arising from different EFs (Snyder, 2013; Snyder, Kaiser, Warren, & Heller, 2014). Dynamic paradigms, such as ecological momentary assessment, can be useful as these are able to examine within-individual adaptations to different contexts (Kashdan & Rottenberg, 2010). It is also noted that the current review does not examine neurobiological research and so cannot comment on whether the cognitive processes described arise from common, or distinct, neural mechanisms (Snyder et al., 2015).
It is important that future studies consider factors that have been found be related to levels of rigidity in a number of studies. The majority of studies reviewed considered the potential impact of age or gender on switching abilities and some considered the potential impact of intelligence (Friedman et al., 2006; Schultz & Searleman, 2002; Tchanturia, Anderluh, et al., 2004). Apart from the studies on rumination (or with clients with depression), few studies considered the impact of mood (Dreisbach & Goschke, 2004; Marien, Aarts, & Custers, 2012; Meeten & Davey, 2011). Furthermore, very few studies considered the potential effect of state anxiety (Eysenck & Derakshan, 2011; Plessow, Fischer, Kirschbaum, & Goschke, 2011). Limited research has investigated whether switching/inhibition difficulties are a potential causal risk factor for developing psychopathology or a consequence of psychopathology (Snyder et al., 2015).
Summary of recommendations for future research
Studies that examine whether individuals who score highly on both rigidity and maintenance styles are at greater risk of psychopathology than those who score highly on one or the other. In addition, studies that examine whether the interaction between a transdiagnostic process and rigidity predicts the maintenance and exacerbation of symptoms of psychopathology over time, when controlling for psychopathology at baseline. Research examining whether the impact of rigidly applied processes is mediated by goal conflict, as indicated by our use of a PCT framework. Further research examining whether rigidity is a potential causal risk factor for developing psychopathology or a consequence of psychopathology. Further research examining how rigidity interacts with internal (e.g., mood) and external context (e.g., situational demands), as well as transdiagnostic processes.
Conclusion
With increasing identification of transdiagnostic processes, it seems important to consider what mechanisms these processes may have in common, in order to contribute to a parsimonious explanation of psychopathology. The majority of studies indicated that measures of rigidity/flexibility and maintenance processes were correlated, co-occurring, or predictive of each other. Possible explanations for this were considered, but data were insufficient to draw any definite conclusions. Further studies with interaction terms are required in order to establish whether maintenance processes in combination with rigidity are particularly predictive of psychopathology.
Footnotes
Authors’ note
The manuscript was written while both authors were affiliated with the University of Manchester. It was primarily written while the first author was in receipt a North West Doctoral Training College, Economic Social Research Council, CASE Studentship Award. Initial work on the manuscript commenced while the first author was employed by Manchester Mental Health and Social Care Trust.
Acknowledgments
The authors would like to thank two reviewers of a previous version of the review and also Dr Julia Hose (consultant psychiatrist), Dr Elizabeth Murphy (clinical psychologist), Dr Rebecca Kelly (clinical psychologist), and Professor Alex Wood for their very insightful and helpful comments. The first author is now employed by the University of Salford.
Declaration of Conflict of Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Notes
Appendix A
The recommendations in the PRISMA statement for reporting the flow of information through the different phases were followed (Liberati et al., 2009; Moher et al., 2009). The PRISMA statement includes a 27-item checklist of items to include in systematic reviews, which includes items related to all sections of the review (abstract, introduction, etc.) (Moher et al., 2009). Of the 27 items recommended, 22 items were incorporated into the review, as relevant to the focus of the review. For example, the introduction described the rationale for the review in the context of what is already known. The items, or elements of items, that were not incorporated were generally (with one exception) excluded because they were not relevant to either the focus or the methodological design of the review; for example, it was not relevant to include the details of which interventions were included, as the review does not examine intervention studies. Items that were not included were number five, which pertained to protocol registration, as the protocol was not registered and is detailed within the current review rather than elsewhere. Items 15 and 22 were not included as they relate to analyzing risk of bias across studies and the authors are not aware of any methods of doing this without first conducting a meta-analysis. Items 16 and 23 pertain to additional analyses and were not reported, as it was not appropriate to do sensitivity, subgroup, or meta-regression analyses because the review was not a meta-analysis.