
Abstract
The inference-based approach (IBA) is a cognitive account of the etiology and maintenance of obsessive-compulsive disorder (OCD). According to the IBA, individuals with OCD confuse an imagined possibility with an actual probability, which leads them to become immersed in their obsessions. To investigate the relationship between OCD and the cognitive factors proposed to add to immersion, we used the Choice Blindness Paradigm (CBP). This paradigm is an experimental reasoning task designed to induce confabulatory reasoning. Undergraduate participants with high levels of OCD symptoms (n = 29) were compared to those with low levels of OCD symptoms (n = 32) with respect to their performance on the CBP. Compared to low-OCD participants, the results indicated that high-OCD participants were more certain (one aspect of immersion) when reasoning about falsely occurring events. However, the cognitive factors proposed by the IBA to underpin immersion did not mediate the relationship between OCD status and certainty regarding false events. Replication and refinement of the current study will help to determine the significance of these cognitive factors in obsessions.
Obsessive-compulsive disorder (OCD) is often referred to as the disease of doubt (Janet, 1903) because obsessions are often expressed as doubts, such as “I might be contaminated” or “my door might be unlocked.” Individuals with OCD then utilize various compulsive behaviors, such as washing and checking, to alleviate the distress caused by the doubt. It is now known that individuals with OCD tend to experience doubt not only in relation to their OCD concerns, but also regarding their memory (Dar, 2004; Tolin et al., 2001), decision-making and concentration abilities (Nedeljkovic & Kyrios, 2007; Nedeljkovic, Moulding, Kyrios, & Doron, 2009), perception and senses (Aardema, O’Connor, & Emmelkamp, 2006; Hermans et al., 2008; van den Hout, Engelhard, de Boer, du Bois, & Dek, 2008; van den Hout et al., 2009), and internal states such as relaxation and muscle tension (Lazarov, Dar, Liberman, & Oded, 2012; Lazarov, Dar, Oded, & Liberman, 2010; Lazarov, Liberman, Hermesh, & Dar, 2014). Despite its fundamental role in OCD, little is known about how obsessional doubts are maintained despite there being substantial contradictory evidence available to the individual with OCD (Lazarov et al., 2012; O’Connor, Ecker, Lahoud, & Roberts, 2012).
The inference-based approach (IBA) is a cognitive model that attempts to address this limitation in our understanding of OCD (O’Connor et al., 2012). The central argument of this model is that these pathological doubts or imagined possibilities about reality are confused to be true via a state termed inferential confusion (Aardema et al., 2006; Aardema, O’Connor, Emmelkamp, Marchand, & Todorov, 2005; O’Connor & Robillard, 1995). This state of inferential confusion is characterized by the maladaptive reasoning devices proposed to be exclusive to OCD, which together enforce the credibility of and immersion into the obsessional doubt, such as “my car is unlocked.” These reasoning devices include apparently comparable events—viewing distinct independent events as comparable (e.g., “my friend’s brother thought he locked his car but found out that he didn’t”) and out of context facts—applying abstract facts without reference to the current context (e.g., “I’ve read about car doors mysteriously unlocking and swinging open”). For a detailed explanation of all the reasoning devices, see O’Connor, Ecker, Lahoud, & Roberts (2012).
The IBA suggests that individuals with OCD typically use one or more of these unusual or inappropriate reasoning devices to justify their doubts (O’Connor et al., 2012; O’Connor, Koszegi, Aardema, van Niekerk, & Taillon, 2009). This justification of doubt takes the form of an inductive narrative, which becomes the obsession (i.e., “my car might be unlocked. I’ve read about car doors mysteriously unlocking and swinging open. My friend’s brother thought he locked his car but found out that he didn’t. Therefore the car is unlocked”). These reasoning devices and inferential confusion lead the inductive narrative to become immersive and to take on obsessional qualities (i.e., increased frequency and distress), and is what sets it qualitatively apart from the content of obsessions observed in nonclinical populations (Julien, O’Connor, & Aardema, 2016). Compulsions then develop in response to the resulting distress by attempting to resolve the doubt.
There is increasing empirical support for some components of the IBA model. Aardema, O’Connor, Emmelkamp, Marchand, & Todorov (2005) developed the Inferential Confusion Questionnaire (ICQ) to measure the construct of inferential confusion. This questionnaire includes the items that reflect two key reasoning devices, inverse inference and a distrust of the senses (e.g., “I am sometimes more convinced by what might be there than by what I actually see”). Higher scores on the ICQ indicate a greater degree of reliance on these reasoning devices and consequently an increased tendency to confuse imagined possibilities with reality (Aardema et al., 2005). Researchers in multiple studies have found a positive and significant association between scores on the ICQ and OCD symptoms, independent of scores measuring general distress and the maladaptive belief domains proposed by other cognitive models of OCD (Aardema et al., 2005; Aardema & Wu, 2011; Paradisis, Aardema, & Wu, 2015). Individuals with OCD also score higher on this measure compared to individuals with other anxiety disorders and nonclinical groups (Aardema et al., 2005). These results have been replicated with the expanded version of the ICQ (Aardema et al., 2010), which includes items to cover the other reasoning devices detailed above. Furthermore, treatment studies comparing the efficacy of cognitive behavioral therapy for OCD and the treatment based on the IBA model (inference-based treatment) have found that a decrease in inferential confusion scores was significantly associated with a decrease in OCD symptoms following both types of treatment (Del Borrello & O’Connor, 2014). Together, these studies support the relevance of inferential confusion in OCD.
Relative to the amount of evidence for an association between inferential confusion and OCD symptoms, there is little experimental evidence for one of the central predictions of the IBA model: that greater levels of inferential confusion lead to increased immersion in the inductive narrative for individuals with OCD. Recently, Aardema et al. (2014) presented preliminary evidence suggesting a positive relationship between OCD symptoms and generating an inductive narrative. They induced an unselected sample of community participants to produce confabulatory self-reports via the Choice Blindness Paradigm (CBP; Johansson, Hall, Sikstrom, & Olsson, 2005). This paradigm was originally developed to induce confabulatory reasoning by deceiving participants into justifying a choice they did not actually make. While there are various versions of this paradigm, they all follow a similar structure. That is, the experimenter first asks participants to make a choice between two items. The experimenter then swaps out the chosen item with the one that was rejected using a sleight-of-hand manipulation and then presents this item back to the participant. The experimenter then asks participants to provide reasons for their “choice.” Participants generally fail to notice that the presented choice is incongruent with their initial choice (Johansson et al., 2005; Johansson, Hall, Sikstrom, Tarning, & Lind, 2006) and provide justifications.
Using a pencil and paper version of the CBP, Aardema et al. (2014) found that those who confabulated on this task (i.e., failed to notice that their initial choice was swapped out) scored significantly higher on the obsessions subscale of the Vancouver Obsessional Compulsive Inventory than those who did not confabulate. This result could not be explained by participants wanting to present themselves favorably to the experimenter (i.e., social desirability). Aardema et al. (2014) first concluded that inductive narratives can be experimentally generated using the CBP. Since participants were reasoning about the events that did not occur (i.e., a choice they did not make), these reasons were analogous to the inductive narrative people with OCD develop to justify an imagined state of affairs about reality. Aardema et al. (2014) also concluded that an individual’s forming of an inductive narrative is associated with their level of OCD symptoms. The IBA proposes that the mechanism behind this association is inferential confusion, which is what leads the OCD inductive narrative to be more immersive (Julien et al., 2016). However, neither inferential confusion nor immersion in the inductive narrative was measured in the described study. As such, we currently do not have evidence supporting a link between inferential confusion and immersion in the inductive narrative. This important gap in the IBA literature is what the current study attempted to address.
Due to its emphasis on the imaginary nature of obsessions, the IBA has provided a conceptualization of OCD that is consistent with a continuum hypothesis between OCD and delusional disorders (e.g., schizotypal personality disorder; Aardema et al., 2005; Sobin et al., 2000). Individuals with these delusional disorders tend to be overly suspicious of reality and have odd or magical beliefs, which together may lead to an absorption in alternate realities (Aardema et al., 2005; Chmielewski & Watson, 2008). In line with the continuum hypothesis, individuals with OCD have been shown to demonstrate positive schizotypal symptoms (Chmielewski & Watson, 2008). OCD and delusional disorder groups also score comparably and significantly higher on inferential confusion compared to individuals with other anxiety disorders and nonclinical groups, suggesting that these disorders may also share cognitive processes (Aardema et al., 2005). If OCD is dimensionally related to delusional disorders, then it is possible that the factors related to delusional disorder may also contribute to immersion in the inductive narrative as well as inferential confusion. As such, we were additionally interested in exploring the relationship between OCD and the symptoms related to delusional disorders (i.e., schizotypal personality features and magical thinking).
Aims and hypotheses
Our primary aim was to test one of the central ideas of the IBA model which asserts that inductive narratives are especially immersive for individuals with OCD (Julien et al., 2016). To this end, we administered the original version of the CBP (Johansson et al., 2005) to have participants with low and high levels of OCD symptoms generate inductive narratives in justifying their choice for photographs depicting women’s faces. Some of these justifications were about the choices participants actually made (non-manipulated trials) while others were about “choices” they did not actually make (manipulated trials), which was accomplished using a simple sleight-of-hand manipulation. As described above, it was the inductive narratives justifying these imagined choices on manipulated trials that are likened to the OCD narrative individuals with OCD use to justify an imagined state of affairs about reality (Aardema et al., 2014).
As such, our primary hypothesis was that participants with high levels of OCD symptoms, compared to participants with low levels of OCD symptoms, would generate inductive narratives on manipulated trials that would be more immersive. Following Johansson, Hall, Sikstrom, & Olsson (2005), immersion was operationalized by the number of lexical indices indicating emotion, specificity, and certainty. That is, immersed participants were expected to justify their choices with more emotional engagement, more detail, and more certainty. We did not expect any between-group differences in these lexical indices on non-manipulated trials. As an important extension to Aardema et al.’s (2014) study, our secondary hypothesis was that inferential confusion would significantly mediate the relationship between OCD group membership and the lexical indices used on manipulated trials. In line with the findings from previous studies, we additionally hypothesized that participants with high levels of OCD symptoms would score higher on self-report measures of inferential confusion, schizotypal features, and magical thinking.
Method
Participants
The current sample was recruited via the first year undergraduate psychology pool at the University of New South Wales who received course credit for their participation. As per course requirements, all enrolled students (N = 1,100) completed a battery of prescreening measures. Only individuals scoring in the top and bottom quartiles of the Obsessive-Compulsive Inventory–Revised (OCI-R; Foa et al., 2002), a measure of obsessive-compulsive (OC) symptom severity (outlined below), were eligible for participation. The top and bottom quartiles of scorers were categorized as high OCD and low OCD, respectively. This use of nonclinical analogue samples in OCD research has been shown to be appropriate in understanding OC-related phenomena (Abramowitz et al., 2014; Burns, Formea, Keortge, & Sternberger, 1995). The final sample consisted of 61 participants: 32 low-OCD participants (22 women, mean age = 20.28, SD = 4.94, range 17–44) and 29 high-OCD participants (17 women, mean age = 19.08, SD = 1.32, range 17–22). The mean score on the OCI-R for the high-OCD group (M = 34.97, SD = 7.34) was higher than the mean score for individuals diagnosed with OCD (M = 28.01, SD = 13.53) and was above the OCI-R clinical cutoff score of 21 (Foa et al., 2002). The mean score on the OCI-R for the low-OCD group (M = 4.97, SD = 2.31) was lower than the mean score for non-anxious individuals (M = 18.82, SD = 11.10; Foa et al., 2002).
Materials and measures
Illusory Beliefs Inventory (IBI)
The IBI is a 24-item self-report questionnaire that was used to measure the strength of beliefs in the domains relevant to magical thinking (i.e., magical beliefs, spirituality, internal state, and thought-action fusion; Kingdon, Egan, & Rees, 2012). Items are scored on a 1- to 5-point scale (where 1 = strongly disagree and 5 = strongly agree). Higher scores indicate a stronger belief in these domains. In a nonclinical sample, the IBI has been validated and has a high internal consistency of 0.93 (Kingdon et al., 2012). Internal consistency (assessed using Cronbach’s α) in the current sample was comparable at 0.88. The IBI has good convergent validity with other measures of magical ideation such as the Magical Ideation Scale (r = .64) and good discriminant validity with measures of rational beliefs (r = −.23). Kingdon, Egan, & Rees (2012) found that the general population scored higher on the IBI than a skeptical sample, indicating good divergent validity.
Inferential Confusion Questionnaire–Expanded Version (ICQ-EV)
The ICQ-EV is a 30-item self-report questionnaire that was used to measure the broad range of reasoning devices that characterize inferential confusion (including a distrust of the senses and inverse inference; e.g., “I often react to a scenario that might happen as if it is actually happening”; Aardema et al., 2010). Items are scored on a 1- to 6-point scale (where 1 = strongly disagree and 6 = strongly agree). Higher scores indicate an overreliance on maladaptive reasoning devices and an increased tendency to confuse imagination with reality. The ICQ-EV has been validated in clinical and nonclinical samples (Aardema et al., 2010), showing significant correlations with OCD symptoms when controlling for negative affect (r = .38–.68) and OCD beliefs domains (r = .40). The total scale has high internal consistencies ranging from 0.96 to 0.97 and was comparable to the current sample (Cronbach’s α = .97).
OCI-R
The OCI-R is an 18-item self-report questionnaire that was used to measure the severity of OCD symptoms experienced during the past month (Foa et al., 2002). Items are scored on a 0- to 4-point scale (where 0 = not at all and 4 = extremely). The OCI-R has high internal consistencies across varying samples, ranging from 0.81 to 0.93 (Foa et al., 2002). This was comparable to the internal consistency of scores obtained from the current sample during prescreening (Cronbach’s α = .95).
Schizotypal Personality Questionnaire–Brief Version (SPQ-B)
The SPQ-B is a 22-item self-report questionnaire that was used to measure schizotypal personality features (e.g., odd beliefs and magical thinking; Raine & Benishay, 1995). Scoring is dichotomous (i.e., yes or no) and total scores range from 0 to 22. Higher scores indicate a greater level of schizotypal symptoms. The SPQ-B has an acceptable internal consistency of 0.76 for a nonclinical sample (Raine & Benishay, 1995) and was slightly higher for the current sample (Cronbach’s α = .85).
CBP
This is a task developed to reliably produce confabulatory self-reports (Johansson et al., 2005). There are a total of 15 trials and participants are asked to choose between two portraits for each trial. Three of these trials are manipulated trials where a sleight-of-hand manipulation is used to swap the portraits after participants have indicated their preference. Participants are then given back the decoy portrait and asked to provide reasons for their “choice.” No swap occurs on the 12 non-manipulated trials, in which participants are given back their chosen portrait and asked to justify why they chose it.
Photographs
The 15 portrait pairs (i.e., 30 portraits in total) used for the CBP were the Nottingham scans taken from the Stirling face database. The sizes of the portraits were 6.5 cm × 8 cm (length × height) and they were all black and white portraits of adult women. Portrait pairs were matched on age, ethnicity, and smile orientation.
Funnel debriefing procedure
Funnel debriefing was included to check for any suspicion regarding the CBP, particularly whether participants noticed the portraits being deliberately swapped. The experimenter asked three questions that gradually increased in specificity regarding the swap. The first question asked about the purpose of the experiment and the second question asked whether they felt that any part of the experiment was strange. For the third question, they were told that past experimenters have accidentally swapped the portraits on some trials of the CBP and then asked whether they thought a similar mistake had occurred in this experiment. Depending on their responses to these questions, participants were assigned a suspicion score ranging from 0 to 3 (where 0 = no suspicion and 3 = thought the experimenter deliberately swapped the cards).
Linguistic Inquiry and Word Count (LIWC)
The LIWC is a computer program that has an internal default dictionary which determines the words that should be counted in the target text files (Pennebaker, Boyd, Jordan, & Blackburn, 2015). This extensive dictionary is split into subgroups with words that tap into a particular domain (e.g., negative emotion words, achievement words). The latest version of the default dictionary is the LIWC2015. The LIWC output includes the percentage of words in the text that belongs to a subgroup. The LIWC has high external validity and reliability (Pennebaker et al., 2015). Of interest in the current study is the level of immersion (operationalized by lexical indices indicating emotion, specificity, and certainty) displayed by participants in their reasoning on the CBP.
Emotion dimension
Examples of emotion words from the LIWC2015 dictionary include “antagonistic,” “exhausting,” “heartbroken,” “optimal,” “stubborn,” and “warm.”
Specificity dimension
The amount of detail was operationalized as the total number of words used minus the number of filler words (e.g., “I mean,” “I don’t know,” and “you know”) and nonfluencies (e.g., “um,” “ah,” and “er”).
Certainty dimension
Examples of certainty words from the LIWC2015 dictionary include “absolutely,” “clearly,” “definitely,” and “undoubtedly.”
Procedure
All undergraduate students first completed the battery of prescreening measures, which included the OCI-R. Signups were processed via the SONA Experiment Management System that allowed the experimenter to restrict access to the current study based on students’ OCI-R scores. Upon entering the laboratory, eligible participants (see above) were seated at a table facing the experimenter and provided written consent. The experimenter then told them a cover story regarding the CBP and instructed them on the task. The aim of the cover story was to encourage participants to elaborate on their reasons for their choice of portrait. This was done by focusing their attention onto the portraits’ facial features to encourage them to base their reasons on these. They were told: We know that when people make choices, they can provide reasons for their choice that also distinguishes their choice from the other available options. I am interested in these reasons that people provide. Sometimes people are able to perceive certain personality characteristics based on facial features or make detailed judgments about how likeable the person is.
Following the CBP, participants completed the computerized versions of the ICQ-EV, IBI, and SPQ-B. Finally, participants went through the funnel debriefing procedure before being debriefed about the purpose of the study, thanked, and credited for their participation.
Results
Group characteristics
A χ2 test confirmed that the groups did not differ in regard to gender, χ2(1, N = 61) = .68, p = .41. Furthermore, a two-tailed independent samples t test was used to check for between-group age differences. The high-OCD group did not significantly differ from the low-OCD group in age, t(59) = −1.32, p = .19, Cohen’s d = .35.
Group differences on self-report questionnaires
A multivariate analysis of variance (MANOVA) simultaneously compared the groups on all questionnaire scores. Using Pillai’s trace, there was a significant main effect of group, F(4, 56) = 128.68, p < .001, η 2 p = .90. See Table 1 for means, standard deviations, and test statistics for group comparisons on each measure. Importantly, the prescreening procedure was successful such that the high-OCD group reported more OCD symptoms on the OCI-R than the low-OCD group, F(59) = 483.06, p < .001, partial η 2 p = .89. As predicted, the high-OCD group also reported significantly more inferential confusion, schizotypal personality features, and magical beliefs (p < .05).
Group means, standard deviations, and test statistics for questionnaire responses.
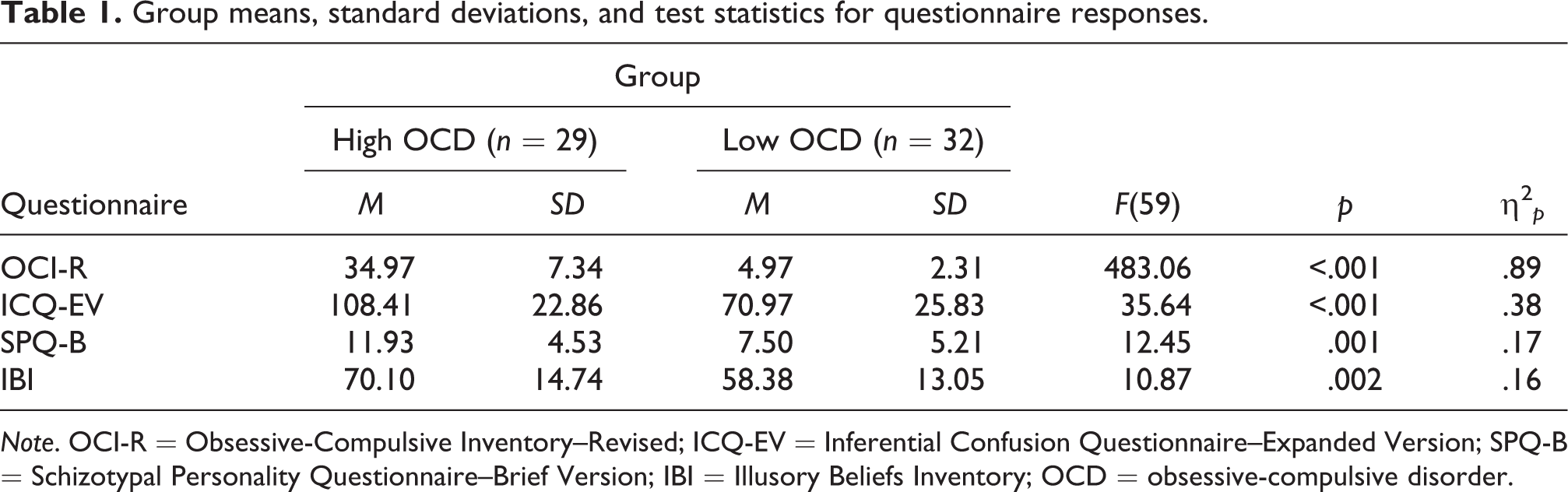
Note. OCI-R = Obsessive-Compulsive Inventory–Revised; ICQ-EV = Inferential Confusion Questionnaire–Expanded Version; SPQ-B = Schizotypal Personality Questionnaire–Brief Version; IBI = Illusory Beliefs Inventory; OCD = obsessive-compulsive disorder.
LIWC analyses
A χ2 test revealed that the groups did not significantly differ in terms of their suspicion (based on the funnel debriefing) on the CBP, χ2(3, N = 61) = .39, p = .94. Groups also did not differ in the number of participants who detected the swap (i.e., received a suspicion score of 3). Specifically, there was one detector in each group.
The LIWC output for each participant gives us the percentage of words in the text file that belongs to a particular lexical dimension. Percentages of words belonging to the emotion, specificity, and certainty dimensions were separately obtained for manipulated and non-manipulated trials. We also obtained the total number of words used by participants on each trial type to account for this potential confounding variable. That is, one group may exhibit more lexical indices of immersion simply because they have a tendency to use more words to justify their choices. We conducted a MANOVA to check if the groups differed on the total number of words used on each trial type (manipulated and non-manipulated). On manipulated trials, the high-OCD group used an average of 105.55 words (SD = 60.17) and the low-OCD group used an average of 137.03 words (SD = 68.66). On non-manipulated trials, the high-OCD group used an average of 114.69 words (SD = 46.83) and the low-OCD group used an average of 135.03 words (SD = 53.66). There was no significant main effect of group using Pillai’s trace, F(2, 58) = 1.77, p = .18, η 2 p = .06, suggesting that, averaging across trial type, the groups did not differ on the total number of words used.
Group differences on lexical indices of immersion
We conducted a MANOVA to simultaneously compare the groups on the three lexical indices of immersion (emotion, specificity, and certainty) for each trial type (manipulated and non-manipulated). To adjust for inflation of the type I error rate due to multiple planned comparisons, we applied a Bonferroni correction to our critical p value (.05) by dividing it by the number of planned comparisons (k = 6). Given this, our modified critical p value was .008. See Tables 2 and 3 for group means, standard deviations, and test statistics for LIWC output (lexical indices of immersion and word count) on manipulated and non-manipulated trials, respectively. We found some support for our primary hypothesis, such that the high-OCD group used a higher percentage of certainty words on manipulated trials compared to the low-OCD group, F(59) = 7.80, p = .007, η 2 p = .12. No other comparisons were significant.
Group means and standard deviations for LIWC output on manipulated trials.

Note. Bonferroni-corrected critical p value = .008. OCD = obsessive-compulsive disorder.
Group means and standard deviations for LIWC output on non-manipulated trials.

Note. Bonferroni-corrected critical p value = .008. OCD = obsessive-compulsive disorder.
Mediation analyses
A mediation (indirect effects) model using the PROCESS script for SPSS version 25.0 (Hayes, 2013) examined our secondary hypothesis of whether the severity of OCD symptoms (i.e., OCD group membership) positively predicted the percentage of words indicative of certainty, emotion, and specificity on manipulated trials and if these relationships were mediated by inferential confusion. As smaller samples are prone to violating the assumptions of normality required by mediation models, the sampling distribution of indirect effects was bootstrapped 10,000 times to provide nonparametric estimates of these sampling distributions (see Preacher & Hayes, 2004; Williams & MacKinnon, 2008). In bootstrapping analysis, significant indirect effects (p < .05, two-tailed) are indicated by 95% bias-corrected and accelerated confidence intervals (CI) that do not include the value of 0. According to the recommendations by Fritz and MacKinnon (2007), single-mediator models with bias-corrected bootstrapping and medium effect sizes (β coefficient = .39) for each pathway in the model require a sample size of 71 for 0.80 power in detecting mediation. Since the current sample size was slightly lower than is recommended for this type of analysis, any conclusions drawn about mediation should be interpreted with caution. Separate mediation models were conducted with scores on the ICQ-EV as the mediator and the percentage of certainty, emotion, and specificity words on manipulated trials as the dependent variables. These models are presented in Figures 1, 2, and 3.

Mediation model with the percentage of certainty words used on manipulated trials as the outcome variable and Inferential Confusion Questionnaire–Expanded Version (ICQ-EV) scores as the mediator. Numbers represent unstandardized β coefficients. Group is coded 0 = low OCD, 1 = high OCD. *p < .05. **p < .01. ***p < .001. OCD: obsessive-compulsive disorder.

Mediation model with the percentage of emotion words used on manipulated trials as the outcome variable and Inferential Confusion Questionnaire–Expanded Version (ICQ-EV) scores as the mediator. Numbers represent unstandardized β coefficients. Group is coded 0 = low OCD, 1 = high OCD. *p < .05. **p < .01. ***p < .001. OCD: obsessive-compulsive disorder.
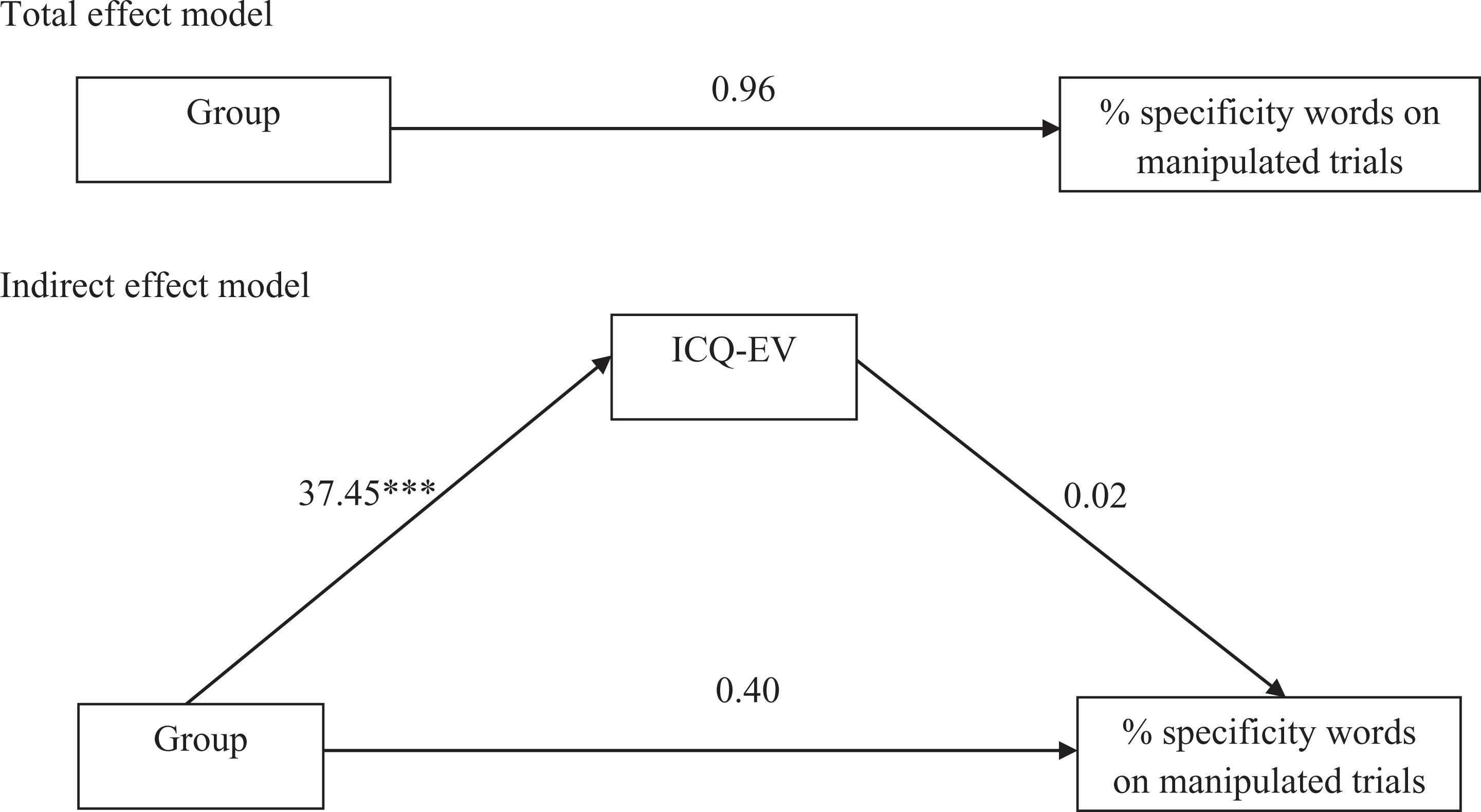
Mediation model with the percentage of specificity words used on manipulated trials as the outcome variable and Inferential Confusion Questionnaire–Expanded Version (ICQ-EV) scores as the mediator. Numbers represent unstandardized β coefficients. Group is coded 0 = low OCD, 1 = high OCD. *p < .05. **p < .01. ***p < .001.OCD: obsessive-compulsive disorder.
Unstandardized indirect effect β coefficients and 95% CI are reported in this section. The indirect effect of the OCD group on the percentage of certainty words used on manipulated trials via inferential confusion scores was negative (indirect effect β coefficient = −.06) and not statistically different from 0 (95% CI [−0.47, 0.22]). The indirect effect of the OCD group on the percentage of emotion words used on manipulated trials via inferential confusion scores was negative (indirect effect β coefficient = −1.05) and not statistically different from 0 (95% CI [−2.91, 0.53]). The indirect effect of the OCD group on the percentage of specificity words used on manipulated trials via inferential confusion scores was positive (indirect effect β coefficient = .56) and not statistically different from 0 (95% CI [−0.52, 1.69]).
Discussion
The current study investigated the differences in the degree of immersion in experimentally generated narratives between groups reporting low and high levels of OCD symptoms. Our primary hypothesis, that the high-OCD group would generate more immersive inductive narratives justifying their choices on the CBP compared to the low-OCD group (evidenced by a greater proportion of lexical indices indicative of immersion) on manipulated trials, was partially supported. Specifically, the high-OCD group justified choices they did not actually make with more certainty in their language compared to the low-OCD group, but did not differ in how detailed and emotional their language was. As inductive narratives justifying imagined choices on manipulated trials were likened to the OCD narrative individuals with OCD use to justify an imagined state of affairs about reality (Aardema et al., 2014), our findings were somewhat consistent with what the IBA model would predict (Julien et al., 2016).
Contrary to our secondary hypothesis, inferential confusion did not mediate the relationship between the levels of OCD symptoms and immersion in inductive narratives on manipulated trials. Together, these findings suggest that while this cognitive factor may be elevated and relevant in individuals with OCD, the mechanism by which it influences the OCD narrative is unclear. At least in the current study, we were unable to provide support for the IBA assertion that inferential confusion predicts greater immersion in the OCD narrative.
Finally, we were able to replicate the findings from previous studies showing that individuals with high levels of OCD symptoms self-reported greater levels of inferential confusion, schizotypal features, and magical thinking compared to individuals with low levels of OCD symptoms (Kingdon et al., 2012). These results also provide some support for the continuum hypothesis between OCD and delusional disorders (Aardema et al., 2005; Chmielewski & Watson, 2008). Indeed, individuals with clinically significant levels of OCD demonstrate mild to severe schizotypal features (Sobin et al., 2000) and future research could elaborate on the role of these features in OCD. One possibility could be that schizotypal features (e.g., odd or magical beliefs) lead to an absorption in alternate realities (Aardema et al., 2014; Aardema et al., 2005; Chmielewski & Watson, 2008). Therefore, we would expect that schizotypy mediates the relationship between the levels of OCD symptoms and immersion in the inductive narrative on manipulated trials. Future replications of the current study with more power for mediation analyses could investigate this hypothesis. Another possibility may be that schizotypal features contribute to increased rigidity of obsessive beliefs and thus poorer insight into the irrationality of an individual’s OCD symptoms (Paradisis et al., 2015), both of which are related to poorer responsiveness to traditional cognitive behavioral therapy for OCD (Foa, Abramowitz, Franklin, & Kozak, 1999). As such, the presence of schizotypal features in an individual with OCD may suggest the clinical utility of an IBA.
Limitations and future directions
It is possible that support for our hypotheses was precluded by the practical limitations present in the current study. In addition to the small sample size, shortcomings of the LIWC dictionary and the CBP may explain why there were no significant between-group differences on all the lexical indices of immersion. Johansson et al. (2005) proposed that a person immersed in their choice will justify it with more emotional engagement, detail, and certainty compared to an indifferent person. As such, we used the LIWC in the current study to count the number of words used by participants to justify their choices that are reflective of these dimensions (Pennebaker et al., 2015). However, there is little research into whether these dimensions are reflective of actual immersion. Unfortunately, the default LIWC dictionary does not have a single lexical dimension for words reflecting immersive thinking. However, the LIWC gives users the option to generate such a dimension themselves. One could first ask individuals who met diagnostic criteria for OCD to describe the thoughts or events that were experienced as highly immersive. Words that commonly appear across these idiosyncratic reports could then be compiled into a list of words indicative of immersion. Thus as an extension of the current study, the LIWC can count how many words from this custom list appear in participants’ verbal reports to form a more ecologically valid index of immersion in OCD.
It is also possible that participants were indifferent about choosing between female portraits because this decision was quite removed from their everyday concerns. As such, an argument could be made that the high-OCD group did not display more immersive confabulatory reasoning compared to the low-OCD group because their idiosyncratic OC-related concerns and anxiety were not activated. Future replications of the current study could overcome this limitation by changing the stimuli in the CBP to provoke obsessional anxiety such as using stimuli from the Maudsley Obsessive-Compulsive Stimuli Set (MOCSS), clinically validated materials that can reliably provoke different kinds of symptom-specific anxiety in OCD (Mataix-Cols, Lawrence, Wooderson, Speckens, & Phillips, 2009). For example, the MOCSS provokes anxiety in OCD patients with checking fears (i.e., checking subtype), with checking-specific audio instructions (i.e., “imagine that you are not sure whether you switched off or locked the following objects and it is impossible for you to go back and check”), and with pictures of objects that typically provoke anxiety in patients of this subtype (e.g., stove, cooker, and purse).
The CBP can thus adopt elements of the MOCSS to provoke idiosyncratic obsessional anxiety. For example, instead of asking participants to choose between photographs of faces, the experimenter presents them with two pictures of different stoves from the MOCSS and asks them to choose the one they would check to see if it was switched off. As with the current study, the experimenter swaps the pictures after a choice is made on manipulated trials and asks participants to justify why they chose the decoy picture. Although we have emphasized the importance of addressing the heterogeneity of OCD in future replications of the current study, the IBA model predicts an association between inferential confusion and immersion in the confabulated narrative irrespective of the obsessional content (e.g., contamination, symmetry, and harm; Aardema et al., 2005). Nonetheless, future studies with larger samples may be able to examine whether inferential confusion is more strongly associated with any particular OCD symptom dimensions.
Conclusions
The current study was the first attempt in investigating the relationship between inferential confusion and immersion in obsessions in OCD using experimentally generated reasoning data and the quantification of qualitative information. Given that this was a novel experimental approach to testing the predictions made by the IBA model, we have provided important suggestions for future studies to improve on the experimental design to further clarify the role of inferential confusion in OCD. As a burgeoning amount of questionnaire research (including our findings) highlights the relevance of reasoning devices in OCD, the current study serves as an example to go beyond questionnaire research and to investigate these processes using novel experimental approaches.
Footnotes
Author contributions
Shiu F. Wong and Jessica R. Grisham made significant contributions to the conception of the study. Shiu F. Wong designed and conducted the research, analyzed the data, interpreted and drafted the results, and prepared the manuscript. Jessica R. Grisham contributed to the design of the research, interpretation of the results, and to the writing of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.