
Abstract
Previous research suggests that individuals with obsessive-compulsive disorder (OCD) lack confidence in their memories and experience intolerance of uncertainty regarding the completion of tasks, which fuels compulsive rituals. The current pilot study aimed to test a novel interpretive cognitive bias modification (CBM-I) training to attenuate maladaptive thinking styles related to memory distrust, intolerance of uncertainty, and perfectionism. A two-condition (CBM-I training: positive, control) repeated measures design was used to examine the effect of repeated CBM-I training. Participants diagnosed with OCD completed measures of interpretive biases, self-reported symptoms, and behavioral responses. Participants in both conditions interpreted novel ambiguous scenarios more adaptively and endorsed more adaptive OC-relevant beliefs following training. Findings were mixed for behavioral assessments of checking, uncertainty, and perfectionism. Although the small sample size and heterogeneity of the sample limits the conclusions that can be drawn, results highlight opportunities to improve experimental paradigms with better control conditions and idiographic stimuli.
Keywords
Introduction
Cognitive behavioral treatments for obsessive-compulsive disorder (OCD) are mostly effective in reducing symptoms (Abramowitz, Franklin, Zoellner, & DiBernardo, 2002). However, these interventions are neither accessible nor acceptable to all people requiring treatment and the development of new procedures is necessary (Kyrios, Hordern, & Fassnacht, 2015; Lee & Rees, 2011). In the current pilot study, we focused on negative interpretive biases associated with OCD; that is, the tendency to negatively interpret ambiguous stimuli (Butler & Mathews, 1983) in a manner consistent with maladaptive OC-relevant beliefs (Abramowitz, Nelson, Rygwall, & Khandker, 2007; Obsessive Compulsive Cognitions Working Group [OCCWG], 2003).
In OCD, repeated checking behavior is aimed at reducing the risk of perceived potential harm (Rachman, 2002). Dysfunctional assumptions and beliefs about memory and uncertainty contribute to the maintenance of checking compulsions (Muller & Roberts, 2005; Tolin, Abramowitz, Brigidi, & Foa, 2003) and are specific to the content of an individual’s obsessions and compulsions (van den Hout & Kindt, 2003; Woods, Vevea, Chambless, & Bayen, 2002). There is less research examining how they interact to affect interpretation of ambiguous stimuli (Clerkin & Teachman, 2011). For example, an individual who engages in compulsive checking may have beliefs about her memory that are activated by an ambiguous situation (e.g., a closed door that may or may not be locked): My memory is terrible, so I can’t be sure if I have remembered correctly, and I need to check again.
Intolerance of uncertainty, “beliefs about the necessity of being certain, about the capacity to cope with unpredictable change, and about adequate functioning in situations which are inherently ambiguous” (OCCWG, 1997, p. 678) may serve as an integral link between doubting, repeated checking, and memory distrust. The doubt associated with checking generates anxiety, which may be further heightened by inflated standards for certainty (Tolin et al., 2003; van den Hout & Kindt, 2003). Holaway, Heimberg, and Coles (2006) found that individuals with OCD have high levels of intolerance of uncertainty that are comparable to those with generalized anxiety disorder. The need for certainty and control in OCD may be fueled by maladaptive forms of perfectionism (Frost, Novara, & Rhéaume, 2002). Across different subtypes of OCD, compulsions often need to be performed perfectly in order to prevent feared outcomes (Chik, Whittal, & O’Neill, 2007; OCCWG, 1997). These maladaptive beliefs and associated biases are important targets of cognitive interventions. A novel cognitive training procedure shows some promise as an adjunctive intervention for attenuating the maladaptive interpretations of intrusions in OCD (e.g., Clerkin & Teachman, 2011; Williams & Grisham, 2013).
Cognitive bias modification for interpretation (CBM-I) is a novel, computerized approach that aims to target interpretive biases in a range of mental disorders. Mathews and Mackintosh (2000) demonstrated that the active interpretation of personally relevant emotional information can be modified by systematic and repeated presentation of positive or benign illustrations. They pioneered a methodology during which interpretations of three-sentence descriptions of ambiguous situations were trained by asking participants to read a completed sentence (on which the last word was varied between the conditions) or complete a final word fragment that disambiguated the fictional situation. Since their seminal study, different CBM-I procedures have been investigated as potential approaches to modifying maladaptive interpretive biases across a range of disorders (e.g., depression, Blackwell & Holmes, 2010; social anxiety, Salemink, van den Hout, & Kindt, 2009). In OCD, images may be recurrent, disruptive, and uncontrollable (Rachman, 2007). Given the relevance of imagery in the maintenance of a number of psychopathologies (for review, see Holmes & Mathews, 2010), the current study included an imagery induction prior to CBM-I for OC-relevant beliefs as a possible alternative method of reshaping threatening images (Holmes, Lang, & Shah, 2009).
Testing the premises of cognitive models of OCD, Clerkin and Teachman (2011) found that positive training (compared to control training) produced healthier interpretations of OC-relevant stimuli and reduced subsequent emotional vulnerability on a thought suppression stressor task. These results suggest that maladaptive processing associated with anxiety can be changed through CBM procedures (Clerkin & Teachman, 2011). Following from this study, Williams and Grisham (2013) and Beadel, Smyth, and Teachman (2013) replicated Clerkin and Teachman’s results on reductions in OC-relevant beliefs, although the results were inconsistent on OC stressor tasks. CBM training procedures may also enhance traditional cognitive behavioral treatments for OCD (Amir, Kuckertz, Najmi, & Conley, 2015; Salemink, Wolters, & de Haan, 2015).
Recent studies have examined the effect of CBM-I training procedures for specific belief domains related to OCD, including contamination (Whitton, Grisham, Henry, & Palada, 2013), responsibility (Grisham, Becker, Williams, Whitton, & Makkar, 2014), and control of thoughts (Clerkin, Magee, & Parsons, 2014). These studies showed an increase in OCD-specific adaptive interpretive biases following positive CBM-I training compared to control CBM-I training, although the results on behavioral tasks in response to training were inconsistent. Extending from this research, CBM-I training may be applied to target the related OCD belief domains of memory distrust (Alcolado & Radomsky, 2011), intolerance of uncertainty (Salkovskis, 1999), and perfectionism (Chik et al., 2007). Targeting these biases in OCD may clarify their downstream consequences on anxiety and compulsive behavior and provide more data regarding the potential of CBM-I as an adjunct to traditional OCD treatment.
Aims
Investigations targeting specific maladaptive interpretation biases in OCD may clarify the downstream consequences on anxiety and compulsive behaviors and thus their potential for meaningful change. In the current pilot study, we examined whether repeated sessions (one lab session, three home sessions) of positive CBM-I training (compared to control training) could attenuate maladaptive thinking styles related to memory distrust, intolerance of uncertainty, and perfectionism in a sample of participants meeting diagnostic criteria for OCD. Given the relevance of intrusive imagery to OCD (Rachman, 2007), we utilized an imagery induction prior to CBM-I to potentially bolster the effect of the training (as in Holmes et al., 2009; Mathews & Mackintosh, 2000).
Hypotheses
We predicted that participants in the positive training condition (compared to control training) would report more adaptive OC-relevant interpretation biases (related to memory distrust, intolerance of uncertainty, and perfectionism) following training (Amir et al., 2015; Clerkin & Teachman, 2011; Williams & Grisham, 2013). In addition, participants who report a greater tendency to use imagery in their everyday lives may endorse a greater change in interpretation bias following training. Based on the link between thoughts, beliefs, and behaviors in OCD (Rachman, 1997), we predicted that positive CBM-I training would be associated with reduced symptoms and decreased behavioral response to OCD-relevant stressors.
Method
Participants
Participants were recruited via community advertisements and previous participant databases. Participants indicating at least a moderate degree of checking were invited to participate in the study (reporting a score greater than 2 on at least three out of five questions on the Concerns about being Responsible for Harm, Injury, or Bad Luck subscale of the Dimensional Obsessive–Compulsive Scale; Abramowitz et al., 2010). All participants met diagnostic criteria for OCD according to a structured diagnostic interview administered by an advanced doctoral student in clinical psychology (Mini International Neuropsychiatric Interview [M.I.N.I.], Sheehan et al., 1998). Participants were excluded if they reported a current psychotic illness, current substance abuse, or current suicidal ideation. The final sample consisted of 30 participants (23 females, 7 males, mean age = 30.27, SD = 13.19, range 19–61). See Figure 1 for a summary of allocation and exclusions. Current comorbid diagnoses included major depressive disorder (N = 12), generalized anxiety disorder (N = 18), panic disorder (N = 10), agoraphobia (N = 4), social anxiety disorder (N = 7), post-traumatic stress disorder (N = 4), bulimia nervosa (N = 6), and binge eating disorder (N = 1).

CONSORT diagram.
Materials and measures
M.I.N.I.—English version 7.0.0 for DSM-5
The M.I.N.I. is a brief structured interview to assess diagnostic criteria for current and past major psychiatric disorders in DSM-5 and ICD-10 (Sheehan et al., 1998). Diagnosis based on the M.I.N.I. has a high concordance with the Structured Clinical Interview for DSM-III-R (Spitzer, Williams, & Gibbon, 1990) with fair to excellent Cohen’s κ scores (for OCD: κ = 0.63, sensitivity = 0.62, specificity = 0.98; Cohen, 1988; Lecrubier et al., 1997; Sheehan et al., 1997). This measure was administered by a graduate student in clinical psychology and supervised by a senior clinical psychologist.
Padua Inventory–Washington State University Revision
The Padua Inventory–Washington State University Revision (PI-WSUR) is a 39-item self-report measure of the severity of obsessions and compulsions (Burns, Keortge, Formea, & Sternberger, 1996). It measures the degree of disturbance caused by a range of specified thoughts and behaviors and urges using a 5-point scale (e.g., “I have to do things several times before I think they are properly done”). The internal consistency of the total scale is excellent with α = .92 and was comparable in the current study with α = .93.
Obsessive Beliefs Questionnaire—44-item version
The Obsessive Beliefs Questionnaire (OBQ) is a 44-item self-report questionnaire that assesses the degree of beliefs associated with OCD along three dimensions: importance and control of thoughts, responsibility and threat estimation, and perfectionism/certainty (OCCWG, 2003; 2005). Participants are asked to rate each belief on a 7-point scale to describe how they think (e.g., “It is essential for me to consider all possible outcomes of a situation”). The scale has good to excellent internal consistency with α = .93 and comparable in the current study with α = .95.
Memory and Cognitive Confidence Scale
The Memory and Cognitive Confidence Scale (MACCS) is a 28-item self-report questionnaire that measures a range of beliefs about memory and related processes including concentration and attention, decision-making abilities, perfectionism, and confidence in one’s memory abilities (Nedeljkovic & Kyrios, 2007). Participants are asked to rate the extent to which they agree or disagree with statements on a 5-point scale (e.g., “I often doubt my memory for having completed tasks”). The internal consistency of the total scale is excellent with α = .92 and was comparable in the current study with α = .92.
Spontaneous Use of Imagery Scale
The Spontaneous Use of Imagery Scale (SUIS) is a 12-item measure of the tendency toward general imagery use (Reisberg, Pearson, & Kosslyn, 2003). Participants “indicate the degree to which each statement is appropriate to them” on a 5-point scale (e.g., “When I think about visiting a relative, I almost always have a clear mental picture of him or her”). The SUIS has good internal consistency with α = .76 (Nelis, Holmes, Griffith, & Raes, 2014; Reisberg et al., 2003) and was comparable in the current study with α = .82.
Recognition scenarios task
The recognition scenarios task (modified from Mathews & Mackintosh, 2000) was used to assess interpretation of novel ambiguous information pre- and post-training. This task has been validated by Salemink and van den Hout (2010). Pretraining, participants were presented with 10 scenario descriptions that were paired with a title, and remained ambiguous in terms of harmful consequences, memory confidence, or uncertainty. Following a filler task, participants were presented with the titles for each of the 10 scenarios and 4 emotionally valenced disambiguated scenario descriptions, 2 of which corresponded to potential positive or negative interpretations relating to checking, memory confidence, or uncertainty, or perfectionism (targets), and the other 2 corresponded to positive and negative distractors that described a slightly different event to the original (foils). See Table 1 for an example of this task.
Example recognition scenarios task.

Similarity ratings between the original and test scenarios were summed to create an overall score for each of the four categories (positive target, positive foil, negative target, and negative foil). Pre- and post-training overall Target Bias Index scores were calculated by subtracting similarity ratings for negative target items from similarity ratings for positive target items in order to indicate a positive (more adaptive) or negative (more maladaptive) bias across the scenario descriptions (Clerkin & Teachman, 2011). A similar procedure was used to calculate a Foil Bias Index score.
CBM-I task
The CBM-I task was based on the procedure originally used by Mathews and Mackintosh (2000) and modified by others (Clerkin & Teachman, 2011; Holmes et al., 2009; Williams & Grisham, 2013). Training items target interpretations of checking scenarios related to memory distrust, intolerance of uncertainty, and beliefs about the function of checking. Items were developed based on checking-relevant beliefs described in a large online pilot study and in previous laboratory studies including Clerkin and Teachman (2011) and Williams and Grisham (2013). Items were pilot-tested online with an unselected community sample and in two laboratory studies with analogue undergraduate samples who reported compulsive checking behaviors.
Thus, the training paradigm consisted of 40 scenarios, each presented twice (80 items total). The CBM-I training task was programmed using E-Prime software (Version 2.0.0.1; Psychology Software Tools Inc., Pittsburgh, USA) and was presented to participants on a desktop computer. The three home practice tasks for CBM-I training each consisted of a different selection of half the original items (20 scenarios, each presented twice, 40 items total). Most participants completed all three home practice tasks (Task 1 = 28/30, Task 2 = 27/30, Task 3 = 29/30). Removing these participants from the analyses did not change the pattern of results.
Prior to the lab training, participants in both conditions were given an imagery induction task in which they were asked to imagine cutting a lemon (Holmes et al., 2009). Participants were given four sample descriptions and were asked to “imagine each event as happening to themselves” as the description unfolds while describing their mental image out loud. At the beginning of CBM-I training, participants were instructed to read the scenarios and imagine that they were actively involved in the situation and completed two practice scenarios. The first part of each description was presented for a maximum of 8 s (e.g., “Whilst you are out you think that you might have left the heater on at home…”), followed by the final part of the sentence which appeared on the screen for a maximum of 15 s and disambiguated the scenario description. In the positive condition, participants completed the word fragments to resolve the ambiguity of the scenario in an adaptive way (e.g., “but a f_re is unl_kely to start as it is beh_nd a guard’’). In the control condition, the fragments completed the scenario in a non-OC-relevant manner (e.g., “You wond_r what the time is as you are b_ginning to get tir_d”). The control items were based on a pilot study that found that scenarios that ended with an unrelated neutral statement did not change baseline interpretive biases (Black, Stech, & Grisham, 2014) and were employed in Black and Grisham (2016). The same letter fragment was missing from three words in the ending that disambiguated the scenario, to increase the likelihood that participants would read the complete phrase. One study examining CBM-I for social anxiety manipulated the number of letters missing from a single word and did not report a detrimental effect on the training outcome, except if the single word was missing three letters (Steinman & Teachman, 2015). Following half of the training items, participants were presented with a dichotomous comprehension question (e.g., “Would you be very worried if the heater wasn’t off?” [positive condition]), and Correct! or Incorrect! was displayed on the screen depending on the participant’s response.
Neutral images filler task
In order to provide a delay and neutral distraction between stimuli presentation and test on stimuli at two points during the experiment, participants were asked to rate the pleasantness and vividness of a series of neutral images taken from the International Affective Picture System (Lang, Bradley, & Cuthbert, 2005).
Post-training checking measure—noise blaster checking task
Following training, a noise blaster task was used to induce and assess repetitive checking. Participants were asked to use a decibel meter to measure the noise levels emitted by a competitive reaction time task and note them down on a prompt sheet. This task was based on the computerized sound recognition task and pill-sorting task employed by Ladouceur et al. (1995). The experimenter informed participants that the task in the current study was being pilot-tested for another experiment. She emphasized that it was important that the five different levels of noise blast were different from each other, and that none were loud enough to potentially damage a participant’s hearing (e.g., greater than approximately 80 decibels).
A web camera and screen capture recorded the noise blaster checking task, and a blind independent assessor viewed the videos to count checking behaviors based on indices employed by Reeves, Reynolds, Coker, and Wilson (2010) and Grisham, Becker, Williams, Whitton, and Makkar (2014). The following checking behaviors were coded: (1) looking at prompt sheet, (2) checking with decibel meter, (3) checking with headphones, (4) writing on prompt sheet, (5) moving back screen on task, (6) asking for reassurance, and (7) checking after final screen. A sum of these checking behaviors and the total time to complete the task were recorded.
Post-training uncertainty measure—probabilistic inferences task
Following training, participants were asked to complete a probabilistic inferences task (Garety, Hemsley, & Wessely, 1991), during which they were presented with two jars: one that contained 85 red beads and 15 blue beads, and the other that contained 85 blue beads and 15 red beads. Participants were told that they would be able to draw one bead at a time, rate their certainty, and make a final decision about which jar had been chosen. The sequence of beads drawn was randomly alternated between mainly red and blue as follows and was an “easy” level sequence:
R R R B R R R R R B B R R R R R R R R B or B B B R B B B B B R R B B B B B B B B R
Participants could continue drawing beads up to a maximum of 20, after which they were prompted to make a final decision. The task was presented via LiveCode (Version 5.5.1; Runtime Revolution Ltd., 1997). The task has been shown to provoke distress associated with uncertainty for anxious individuals (Jacoby, Abramowitz, Buck, & Fabricant, 2014). A monetary incentive of Australian $5 was included to introduce a “cost” to checking (Australian $0.20 was deducted for each check). To be consistent with Jacoby, Abramowitz, Buck, and Fabricant (2014), the dependent variables were number of checks, final certainty rating, and the accuracy of the final decision. As final certainty ratings may be confounded by the number of beads drawn, certainty rating for the first bead was also included.
Post-training perfectionism task—writing task
To measure perfectionism behaviors, the writing task used by Williams and Grisham (2013) was used in the current study. Participants were asked to write a summary of the tasks that they had completed in the study and were told that the experimenter wanted to find out about their perceptions of the study and to help with describing the study to future participants. As in Williams and Grisham, participants were only given 45 s to enter their response. Following this, participants were asked to rate their confidence in the accuracy of their information and were given the opportunity to add information to their initial response. The total time spent and number of words written during the second phase of the task were used as measures of perfectionism behaviors.
Procedure
At the first session, after providing informed consent, participants completed the M.I.N.I. and baseline questionnaires: PI-WSUR, OBQ-44, MACCS, and SUIS. Following this, participants completed the pretraining recognition task. Then, the participants were randomly assigned to receive either positive or control CBM-I training (approximate completion time was 30 min) and the experimenter was blind to condition. Finally, the participants were given instructions about completing the three home practice CBM-I training tasks online (on Day 2, Day 4, and Day 6 after the lab training) and were sent an e-mail reminder on the morning of each task.
At the second session (1 week after the first session), participants completed the post-training recognition task. Participants then completed the behavioral tasks: noise blaster checking task, probabilistic inferences task, and writing task. Finally, they again completed questionnaire measures (PI-WSUR, OBQ-44, MACCS) and a funneled debrief to determine levels of suspicion.
Results
Participant characteristics
There were equal numbers of participants in each condition: positive (N = 15) and control (N = 15). There were no differences between the conditions on age, gender distribution, PI-WSUR total scores, or PI-WSUR checking subscale scores (all ps > .33). Participants in the control condition endorsed a greater preference for general imagery use on the SUIS compared to the positive condition, t(28) = −2.35, p = .03, d = .88. Given this difference, results including SUIS scores as a covariate are presented for all analyses. In any cases where these results differ from the results without including the SUIS, a footnote was added.
Comprehension accuracy during CBM-I training
Participants had a high degree of accuracy in answering comprehension questions during training (positive condition: M = 36.00/40, SD = 6.31; control condition: M = 35.40/40, SD = 2.75) and this did not differ between groups, t(28) = 0.34, p = .74, d = .13.
Interpretive bias ratings
Recognition ratings on the interpretive bias test taken pre- and post-training were compared using a repeated-measures analysis of variance (ANOVA). A bias index was calculated by subtracting negative ratings from positive ratings, so that a positive index score indicates a more positive bias. There was no difference between the conditions on positive target interpretive bias pretraining (positive condition: M = 4.13, SD = 5.25; control condition: 4.13; SD = 5.66). For target ratings, there was a significant main effect of time, F(1, 28) = 14.50, p = .001, η p 2 = .34, indicating that participants were endorsing a more adaptive bias following training. There was no Time × Condition interaction, F(1, 28) = 0.89, p = .36.
To test the hypothesis that participants’ imagery preference would moderate the effect of the CBM-I training on target bias, the PROCESS tool was used (Hayes & Preacher, 2014). The variable of interest was the change in target bias. The full model comprised SUIS score, experimental condition, and the interaction between SUIS and condition. This overall model was nonsignificant, R 2 = .394, F(3, 26) = 1.59, p = .21. Moreover, the R 2 change due to the interaction of SUIS and condition was nonsignificant, R 2 = .011, F(1, 26) = 0.560, p = .56. Thus, contrary to predictions, there was neither a main effect for participants’ preference for using imagery on the change in target bias nor did imagery preference moderate the effect of condition on target bias.
For foil ratings, there was a significant main effect of time, F(1, 28) = 7.01, p = .01, η p 2 = .20, indicating that participants were endorsing a more positive bias following training (reflecting greater overall positive interpretations of ambiguous scenarios). There was no Time × Condition interaction, F(1, 28) = 0.29, p = .59. Again, when SUIS scores were included as a moderator predicting foil bias at post, the R 2 change due to the interaction of SUIS and condition was nonsignificant, R 2 = .03, F(1, 25) = 1.31, p = .264.
Effect of CBM on self-reported psychopathology
See Table 2 for a summary of means on psychopathology self-report measures. A repeated-measures multivariate ANOVA (MANOVA) was used to examine the effect of CBM-I training on self-reported psychopathology including the SUIS as a covariate. The main effect of time was not significant, F(3, 25) = 0.79, p = .51, η p 2 = .09, 1 and there was no Time × Condition interaction, F(3, 25) = 0.81, p = .50, η p 2 = .09.
Pre- and post-training self-report psychopathology measures.

Note. Standard deviations are in brackets. PI-WSUR = Padua Inventory–Washington State University Revision; OBQ-44 = Obsessive Beliefs Questionnaire–44-item version; MACCS = Memory and Cognitive Confidence Scale.
Effect of CBM-I on checking task performance
See Table 3 for a summary of findings on the behavioral tasks. To examine the validity of these tasks in measuring OC-relevant behaviors, we conducted correlations between post-training self-report measures, post target bias, and observed responses on the behavioral tasks (see Table 4). Unsurprisingly, there were significant correlations between self-report measures of OCD symptoms and beliefs. In addition, positive target bias at post-training was significantly inversely correlated with self-reported OCD beliefs. Moreover, self-reported checking behaviors were significantly correlated with the number of beads drawn on the probabilistic inferences task, providing some support for the validity of this task. Finally, the amount of time spent on the perfectionism writing task was significantly correlated with the number of words written, but these behavioral measures did not correlate with self-report indices.
Results of behavioral tasks.

Note. Standard deviations are in brackets.
*p < .05.
Correlations between post-training self-report measures, target bias, and behavioral task outcomes.
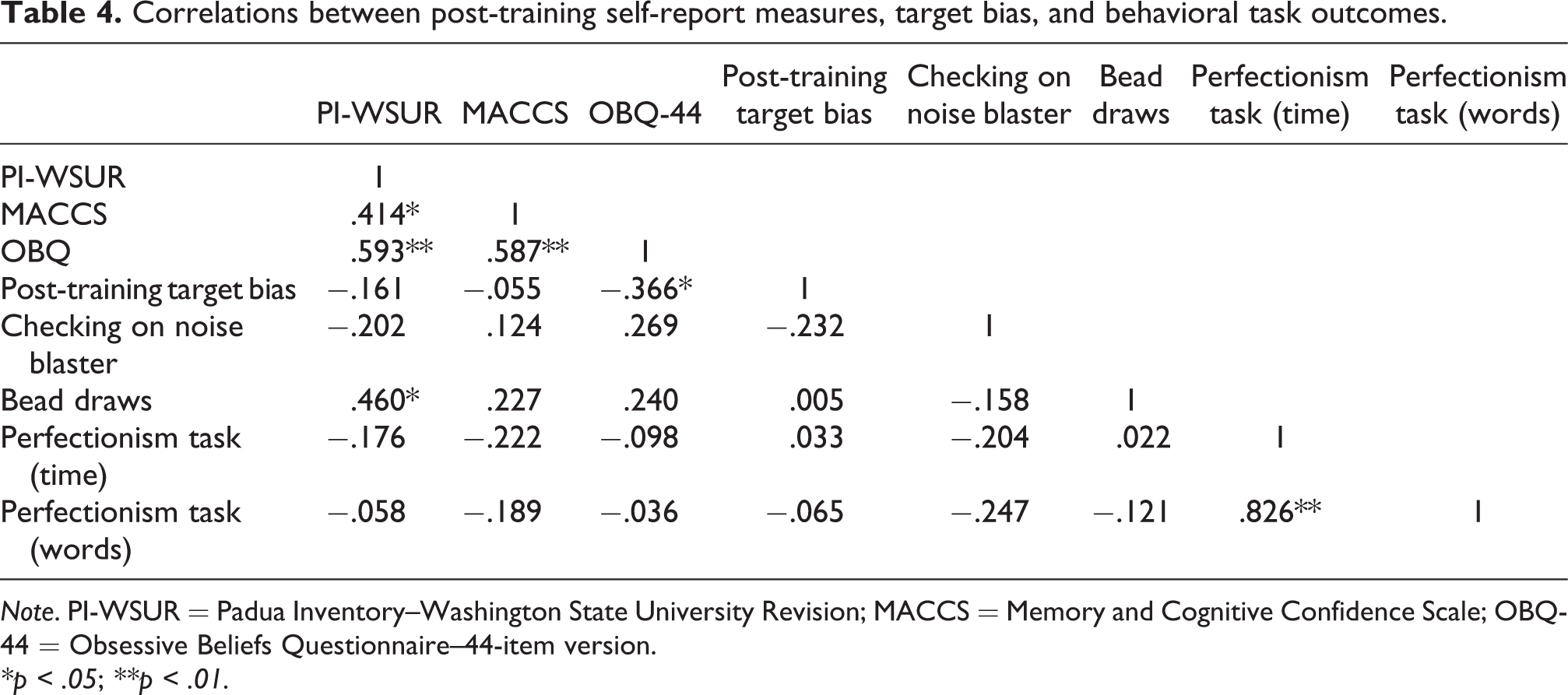
Note. PI-WSUR = Padua Inventory–Washington State University Revision; MACCS = Memory and Cognitive Confidence Scale; OBQ-44 = Obsessive Beliefs Questionnaire–44-item version.
*p < .05; **p < .01.
We examined the effects of CBM-I training on behavioral responses during the noise blaster checking task. Data were missing for one participant due to video recording error. MANOVA with condition as the between-subjects factor and SUIS as a covariate revealed no significant difference between the conditions on total checking time and total number of checking behaviors, F(1, 25) = 1.14, p = .34, η p 2 = .08.
To examine the effects of CBM-I training on the probabilistic inferences task we conducted, MANOVA with condition as the between-subjects factor, and the dependent variables consisting of the number of beads drawn (an index of how much information is required to make a decision) and certainty ratings and SUIS as a covariate. There was a significant difference between the conditions, F(1, 26) = 4.56, p = .02, η p 2 = .26. Participants in the positive condition drew significantly fewer beads than participants in the neutral condition, F(1, 28) = 7.35, p = .01, η p 2 = .21, although there was no difference between the conditions on final certainty ratings, F(1, 28) = 1.48, p = .23, η p 2 = .05.
We also examined the effects of CBM-I training on responses to the perfectionism writing task with MANOVA with condition as the between-subjects factor and the dependent variables consisting of participants’ confidence ratings of their description at Phase 1, the amount of time spent completing the description at Phase 2, and the total number of words written at Phase 2. Overall, there was no significant difference between the conditions, F(1, 25) = 1.01, p = .40, η p 2 = .11.
Discussion
In the current pilot study, repeated sessions of CBM-I targeting maladaptive beliefs about memory, uncertainty, and perfectionism were administered. The results show that interpretive biases may be changed following both positive and control training, although there were no changes on self-report measures when imagery preferences were included as a covariate. Those in the positive training condition drew fewer beads on an uncertainty task, but there were no differences on any other behavioral indices. It is possible that participants’ imagery preference in the current study influenced the findings, but there was insufficient power to adequately test this hypothesis. Given that this was an initial pilot study, we examined only differences between the conditions and did not test the potential mediating role of change in target bias to self-report and behavioral measures. Our modest sample size would limit any conclusions that could be drawn from this type of analysis (Fritz & Mackinnon, 2007). However, it would be important for future, larger scale CBM-I studies to use mediation to test potential mechanisms, as noted in Beadel et al. (2013). These results indicate that the training delivered in the current study may not be strong enough to induce a clinically significant change in biases for participants experiencing clinical levels of OCD symptoms.
Consistent with findings in other CBM investigations (Beard, 2011; Black & Grisham, 2016), both the positive and control training conditions reported increased positive biases following training. Given that a neutral control CBM-I training condition was employed as the comparison, it is likely that this condition also had a positive effect for participants meeting criteria for OCD and endorsing a clinical level of negative OC beliefs. Anecdotally, a number of participants reported on debriefing that they found that the neutral scenario endings conveyed to them that their potentially negative beliefs were unimportant or nonthreatening. Future studies should compare alternative non-CBM control conditions (e.g., reading about OCD, relaxation training, controlled breathing) to determine potential placebo effects of CBM-I training. Those with a greater preference for using imagery also endorsed more positive interpretive biases following training, and possibly facilitated by imaginal exposure to ambiguous OC-relevant scenarios (Clarke et al., 2013). A study which administered CBM training in addition to treatment-as-usual suggested that changes in biases may have been due to cognitive restructuring techniques employed in therapy rather than CBM-I training (Salemink et al., 2015). It is possible that other, nonspecific features of the current study may have facilitated an increase in positive bias (e.g., imaginal exposure to OC-relevant scenarios, familiarity with training scenarios, receiving positive attention from the experimenter, discussing OCD during the diagnostic interview). Future studies may also assess “online interpretations” through probe scenarios during the training in order to detect possible differences between immediate and delayed maladaptive interpretations (Clerkin & Teachman, 2011; Salemink et al., 2015).
There were no significant changes on self-report measures following CBM-I training. This may be due to the brevity of the training or the heterogeneity of symptoms reported by participants. This may reflect the challenge of producing clinically meaningful change for a number of participants who had experienced OC symptoms for an extended period of time. Future studies may consider different symptom assessments or a longer window between training and follow-up to increase the likelihood of detecting differences on self-report measures. It is possible that there was insufficient time or inadequate dose for transfer of biases to symptom levels and associated beliefs (Clerkin & Teachman, 2011; Menne-Lothmann et al., 2014).
Although participants’ everyday imagery preference scores did not moderate the effect of training on interpretative bias, future studies may directly measure participants’ immediate engagement with the training through vividness ratings or include OC-relevant images to further investigate the role of imagery in CBM-I training (Salemink et al., 2015). Future studies may examine other possible moderators of engagement with the training (e.g., relevance of training scenarios, length of the training, delivery method, rewards, etc.). The participant sample in the current study was not treatment-seeking so this may have compromised their engagement with the task (c.f. Amir et al., 2015). Although the current study successfully facilitated a small change in interpretive biases, enhancing engagement with future CBM-I training programs may enhance outcomes.
A selection of behavioral tasks was used in order to assess possible differences in behavior between the two conditions: a noise blaster checking task (responsibility and harm), a probabilistic inferences task (intolerance of uncertainty), and a writing task (perfectionism). The positive condition drew fewer beads on the probabilistic inferences task compared to the control condition, and participants in the positive condition spent marginally more time completing the writing task. However, there were no differences between the conditions on the noise blaster checking task or other indices on the writing task. These results need to be interpreted with caution given that the parallel change in interpretive biases was not observed. Further, the coding of behaviors on these tasks could be improved by refining the limits of functional and dysfunctional behavior in OCD. The system used in the current study may have led to an overestimate of checking behavior (e.g., any “check” was counted in the noise blaster checking task, although this was the same for all participants and allowed for comparison between groups). A link between maladaptive biases and compulsive behavior may be expected based on cognitive behavioral models of OCD (e.g., Rachman, 1997), but further work is warranted to determine the possible moderating role of CBM-I on compulsive behavior. The positive correlation between self-reported checking symptoms and the number of bead draws on the probabilistic inferences task is encouraging as a test of convergent validity. However, future studies may examine the most effective way to measure potential behavioral change: either standardized tasks that are not clearly linked to individual obsessions and compulsions (as in the present study) or idiographic tasks that focus on individual clinical presentations.
Limitations and future directions
OCD is a heterogeneous disorder (Melli & Chiorri, 2012), with symptoms occurring across multiple domains (Stasik, Naragon-Gainey, Chmielewski, & Watson, 2012). Due to practical constraints with recruiting an overall sufficient number of participants in the current study, future studies may aim to recruit participants who experience the particular beliefs targeted in the current study as a part of their primary symptom presentation. Beliefs about memory, intolerance of uncertainty, and perfectionism are likely to cut across dimensions of OCD (Myers, Fisher, & Wells, 2008; OCCWG, 2003), but are unlikely to be the primary concern for all individuals with OCD. Alternatively, tailored CBM-I training programs may gather information from potential participants and utilize this to develop idiographic training items (as in Amir et al., 2015).
Our sample size was small, although it is comparable to other studies investigating experimental paradigms in clinical OCD samples (e.g., Amir et al., 2015; Salemink et al., 2015). Larger randomized controlled trials in clinical samples, such as that proposed by Williams, Pajak, O’Moore, Andrews, and Grisham (2014), are likely to yield interesting results in the development of intervention-type CBM-I paradigms for maladaptive beliefs in OCD. Further, the online tasks were completed outside the laboratory to allow for generalization to different contexts and facilitate administration of repeat training sessions. However, this may have contributed to the inconsistent findings in the present study and controlled laboratory experiments may be necessary to clarify outcomes. The need for treatment innovation in OCD persists, and CBM-I remains a candidate for enhancing existing treatments, but high-quality, low-bias studies are necessary (Cristea, Kok, & Cuijpers, 2015). It is low cost, accessible, and is less stressful than exposure and response prevention (Salemink et al., 2015).
General commentaries and reviews of CBM-I highlight potential limitations with this procedure and translation to a clinical intervention (e.g., Cristea et al., 2015). Demand characteristics possibly lead to participants responding in a manner to please the experimenter rather than in a way that reflects true responding. In a meta-analysis, Cristea, Kok, and Cuijpers (2015) suggested that there may be exaggerated hype about the results of CBM training programs due to publication bias for significant results. As the CBM literature continues to progress, it will be important to avoid “teaching to the test” by seeking to confirm and replicate the results of previous studies and choosing outcome measures that may be sensitive to the specific changes that CBM-I programs are trying to facilitate. With this in mind, it is important to note that CBM research is still relatively young, and that early pilot investigations such as those undertaken in the current study are instrumental in the development of novel interventions.
Conclusions
The findings of our pilot study suggest that further basic science and translational studies are required to determine whether CBM-I training may be utilized to induce more adaptive interpretive bias. The results also provide useful information about potential mechanisms of action in CBM-I training given that there were relatively few differences between the positive and neutral control conditions. Although individual imagery preference did not moderate change in target bias in the current study, the potential influence of individual imagery preference on the outcome of CBM-I training should be considered as an important future research direction given the role of intrusive imagery in OCD (see Holmes & Mathews, 2005). Moreover, consistent with previous CBM-I studies (Koster & Bernstein, 2015; Williams & Grisham, 2013), changes in interpretive bias did not translate to clear changes in self-reported psychopathology or behavioral performance, necessitating improvements to the measurement of transfer of CBM-I training effects.
The results of the current study and recent meta-analyses (e.g., Cristea et al., 2015) may suggest that CBM training procedures may be less promising than indicated by earlier findings. These results provide useful information about the potential of specifically targeted CBM-I procedures to modify maladaptive biases. Future research is warranted in order to examine whether CBM-I training effectively modifies biases in OCD and whether other approaches to targeting maladaptive thinking in OCD are necessary. Several reviews have called for additional research to improve existing procedures and test their limits (e.g., Fox, Mackintosh, & Holmes, 2014; Koster & Bernstein, 2015). Despite initial findings, recent results, including those of this study, suggest that CBM training in its current form may not be powerful enough as a stand-alone intervention to produce clinically meaningful change. Future studies may further examine whether CBM is better utilized to enhance outcomes when it is integrated into a traditional cognitive behavioral treatment program for OCD (e.g., Amir et al., 2015; Salemink et al., 2015).
Footnotes
Acknowledgment
The authors wish to thank several anonymous reviewers who provided helpful suggestions on earlier versions of this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by an Australian Postgraduate Award of the Australian Federal Government awarded to Melissa J. Black and an Australian Research Council Future Fellowship FT140100207 awarded to Jessica R. Grisham.