
Abstract
In this article, we focus on sex education in schools and not sex education in general, which has different audiences, purposes, aims and scope. Swedish sex education has had a reputation as being very liberal and sex-friendly, providing the most advanced information for primary- and secondary-school pupils and students from the mid-20th century onwards. When following the trajectory of sex education into the schooling system, from the start of the 20th century, it becomes clear that the teaching targeted gendered bodies associated with varying risks. Different actors involved in the process make different associations between health promotion, bodies and risk, and a key finding is that the state uses risk as a productive force when promoting sex education in school, while at the same time excluding knowledge about the visual anatomy of the clitoris and the glans, i.e., organs vital to the experiencing of sexual desire. Contemporary Swedish sex education remains a discourse that revolves around health promotion and risk, and the state guidelines (still) lack visual presentations of bodies with organs for desire. In this article, we trace how versions of health promotion have regulated and constrained children’s and young people’s sexuality.
Introduction
In this article, we analyse how health education has focused on promotional aspects through the various concepts that have been used to present Swedish school sex education, mainly in relation to curricula from the beginning of the 20th century until today. As we show below, sex education has been related to subjects like health education, women’s hygiene, biology education with health education, sexual hygiene, the biology of sexual life and hygiene, the biology of sexual life, ethics and hygiene, sexuality and relationship education, social life education, and sexuality, consent and relationships. Hence, we use health promotion as an all-encompassing concept covering different aspects of both hygiene and health in relation to school sex education. Today, “sexual and reproductive health” is a global rights discourse, and in this article, we provide an example of how it is entangled with sex education in schools. We argue that a path to focusing on health promotion as primarily a bodily matter associated with risk was laid out from the beginning and has produced a form of body politics of the state aimed at regulating children’s and young people’s sexuality.
In the history of school sex education, “hygiene” has been a prominent presence from the early 20th century onwards; for example, social hygiene or school hygiene promoting how increased standards of cleanliness were expected to support a healthier lifestyle in general, and in particular to avoid the spread of venereal diseases (Eberwein, 1999; Hampshire, 2005; Zimmerman, 2015). In the early 20th century, the American Social Hygiene Association (ASHA) was a driving force behind the establishment of sex education. It inspired many nation-states to take the “first steps to teach about sex in schools,” and in addition, to spread the topic “to overseas colonies and territories via missionaries as well as secular instructors” (Zimmerman, 2015: 15). ASHA and other actors based in America also disseminated sex education and hygiene on a global scale via a vast number of films and videos (Eberwein, 1999; Zimmerman, 2015). Today, we would not talk about hygiene, instead we would emphasize health promotion (World Health Organization (WHO), 2010), and, in this article, we trace today’s notions of health promotion in relation to sex education into the early 20th century’s concept of hygiene.
When reviewing the research, it becomes clear that the more comprehensive concept of “health” has materialized in varying aspects of sex education in school. Health has been used in relation to sex education as a policy instrument interconnected with a population policy generally aimed at regulating childbirth, and where different aspects of the role of state politics have been studied (Goh, 2024; Haerness Nordberg, 2013; Hampshire, 2005; Lišková et al., 2020; Talukdar et al., 2013; Zimmerman, 2015). References to “health” in sex education have also been regarded as a regulating element to encourage young people to take personal responsibility for their sexuality, meaning that they should regulate themselves according to majority societal norms (Gorzanelli and Knijnik, 2025; Ilpo and Yesilova, 2006). Maintaining “health” has been a way to convey the message that abstinence is the goal of sex education; in the United States, this has been referred to as a conservative neutrality shaping the curriculum (Howe, 1990). This is also known as ABC-education, which teaches about abstinence, being faithful, and using condoms, which became particularly strong at the start of the HIV epidemic in the 1980s and 1990s (Lindgren, 2025; Lesko et al., 2010).
Content analysis of sex education has shown that “health” has been linked to biology, and that biology has become a driving explanatory model for societal change, rather than determining how norms and the social could drive change (Bolander, 2009, 2015; Haerness Nordberg, 2013; Svendsen, 2017; Talukdar et al., 2013). Such a biological discourse on sexuality presents sex as the agent that creates sexuality, rather than acknowledging that it is culture and society that create the conditions for what is perceived as a desirable sexuality (Svendsen, 2017). It has also been pointed out that positioning sex education within biology education is normative and makes certain sexualities particularly visible, as though “natural,” while other sexualities are excluded. This implies that sexuality not aimed at reproduction is illegitimate; if gendered bodies are used for purposes other than procreation, sexuality is deemed superfluous (Backman Prytz, 2024; Junkala, 2023; Planting-Bergloo, 2023; Svendsen, 2017). Additionally, in sex education, risks have been discussed in relation to negative perceptions of sexuality, which has resulted in an education that lacks the ability to engage in teaching about healthy sexuality and desire (Cameron-Lewis and Allen, 2012; Fine, 1988; Lamb et al. 2013; Sauerteig and Davidson, 2009).
In terms of the establishment of sex education in schools, Sweden stands out as one of the first countries in the world to introduce such teaching in primary school, with a national curriculum, as early as the 1940s. Already in the first decades of the 20th century, there was a consensus that society would benefit from introducing sex education to the broader population. Despite changes in society itself, our research has shown that up to the present day the prevailing idea has been that school-based sex education should address societal problems. Thanks to the affluence of archival sources and the possibility of tracking sex and health education over more than a century, Sweden provides a significant example of how sexuality has been regulated through state politics over time. The central question guiding the analysis is: What has been the role of health promotion in the Swedish state sex education discourse over the past hundred years and more?
Health promotion and risk enter education—boys in focus
In Sweden, education about health was part of the curriculum around the turn of the 20th century and framed differently in varying school forms. In state-run girls’ schools, health was already a subject in itself by 1885, and the same curriculum was supposed to regulate private girls’ schools (Statens normalskola för flickor, 1885; Kyle, 1972). In primary school, health was included by 1900 (Normalplan för undervisningen i folkskolor, 1900). State-run upper secondary schools and lower secondary schools included health education as part of the biology syllabus (Undervisningsplan för realskola och allmänna läroverk, 1906).
Regardless of the differences of how health was framed in the varying curricula, health was taught as part of knowledge about nature, specifically human nature and the human body. However, it was only in upper secondary and lower secondary schools mainly targeting boys that health education was associated with risks, thus giving it a clear health-promoting focus. In these schools, knowledge about the human body was supposed to include teaching about substances affecting the body; for example, the damaging effects of stimulants such as alcohol and tobacco as well as contagious diseases. The importance of adopting a healthy lifestyle was also something to be addressed.
Hence, in the early 20th century, health was singled out as important in school education and was associated with knowledge about the body. This was before sex education became related to health education, but health and risk started a narrative that would be re-enacted in relation to such education in other school forms later on in the 20th century. For example, health and risk were introduced into the curriculum for primary school in 1920 (Undervisningsplan för rikets folkskolor 1919, 1920). But our focus remains on the early 1900s as we examine how sex education evolved and became embedded in various health-education concepts, connected to a health-promotion perspective.
Women’s hygiene in civil society—and clitoris visualization
The female physicians who, at the turn of the 20th century, advocated for the establishment of sex education, especially in girls’ schools, regarded the curriculum’s health education as a resource. A specific topic of women’s hygiene was introduced as sex education mainly in private schools for girls, as part of the health education included in biology, zoology and anatomy. This early sex education was mainly coded as a women’s issue, female physicians and teachers were willing to take on such education and girls were the main target group (Thorsén, 2021). To support this education, one of the leading female physicians of the time, who was also one of the first female physicians, published the first anatomical images of the female genitals in Sweden in the late 19th century (Hammarberg, 2001), including naming and visualizing the clitoris (Widerström, 1903[1889]).
The clitoris was described as “a small sensitive organ” attached to other organs such as the small and large labia (Widerström, 1903[1889], p. 10). Naming and visualizing the clitoris was not general practice in medicine at the time, although Widerström was not unique in doing so. For example, the important Gray’s Anatomy (1901) also included the clitoris (Moore and Clarke, 1995). What was new was the introduction of the female genitals in the Swedish context and to make it available as educational material outside the medical field—and also to a young age group, schoolgirls. The main argument for doing this was that the female genitals, sexuality, reproduction and health are a natural aspect of the female body and that it was a right for every girl and woman to obtain such knowledge (Widerström, 1903[1889], 1905). To move the body, especially when in school, was what “the heart longed for,” and promoted health (Widerström, 1907). Hence, in this context of bodily knowledge as positive and a source for emancipation, the potential bodily risks associated with alcohol and tobacco use were not explicitly addressed, as they were in secondary schools for boys. However, other risks were mentioned, such as contracting venereal diseases or unwanted pregnancies. The argument was that women’s knowledge about their own bodies as sexual would serve as a form of protection from these risks (Widerström, 1903[1889]). As shown this far, sex education unfolded in a specific and gendered way in education for girls, closely connected to women and civil society.
Sexual hygiene in the state discourse—girls and sex education
When sex education was first presented for debate in the Swedish Parliament, that is, the state apparatuses, in 1908, it was in the context of a discussion about how to prevent the spread of venereal diseases. This was a male-only assembly excluding women. When measures to combat the spread of venereal diseases were discussed, school sex education was brought up as a possible solution; specifically, providing education in the form of sexual hygiene in primary school. Although the initiatives in girls’ schools in Sweden were mentioned, the main focus was on how male-produced knowledge from Germany could be used (Lindgren and Backman Prytz, 2024).
During this debate, it was mentioned that girls were more mature and capable of handling knowledge about sexual hygiene at an age when boys were regarded as too immature and incapable. For older boys it might be relevant, but for boys in primary school it was considered too early. The discussion ended with a voting procedure where the suggestion to implement sexual hygiene in primary school was defeated by (only) three votes. A strong argument for not taking these measures was that the state should not intervene in such private matters as sexual hygiene, and since the majority of children were in gender-mixed primary schools it was impossible to organize the lessons because girls and boys could not be educated together regarding this special topic (Lindgren and Backman Prytz, 2024).
In the state discourse, the term sexual hygiene continued to be used when talking about sex education. When municipal girls’ schools were organized at the demand of the government in the late 1920s, sexual hygiene was introduced into health education, including knowledge about the body (SFS, 1928: 426). As this shows, the practice of teaching sex education in private girls’ schools was extended into the state-initiated municipal girls’ schools, and in the process sex education changed from being women’s hygiene into the more male and state-connoted area of sexual hygiene. Women’s hygiene was never introduced into the curriculum, as sexual hygiene was.
Hence, a kind of re-gendering took place. The initial argument for the need to provide education in gendered knowledge, was replaced by a seemingly neutral and non-gendered term: sexual hygiene. However, this was also a gendered concept, because it was introduced into the political discourse by men, and in a context where it seemed like a deliberate choice not to use the terminology that was established at the time, which was women’s hygiene. This indicates that the male norm in the state was enough to overrule the already developed field of sexual knowledge promoted by women in civil society. Nevertheless, using sexual hygiene turned out to be a successful practice since it made sex education mandatory in girls’ schools. Via this reform, more girls gained access to sexual knowledge about the female body and reproduction.
The biology of sexual life and hygiene in upper secondary schools—boys and sex education
The next important reform to promote sex education occurred in the 1930s. This was to implement the biology of sexual life and hygiene into the curriculum for state-run higher schools such as upper-secondary schools, which were still mainly for boys. This new terminology had actually been presented ten years earlier in a referral from the National Board for Education. The school agency refused to comply with a suggestion to introduce sex education as mandatory in primary schools, but supported the idea of introducing it for students aged 14 to 15 and older, in order to fight the spread of venereal diseases (RA, Skolöverstyrelsen).
The referral included a special comment about how concepts for sex education should be used. To use sexual hygiene and sex education as synonyms was considered a mistake. Instead, a new nomenclature was suggested: the biology of sexual life and hygiene. There was a need to differentiate what was meant by sexual hygiene by making it clear that it included both reproduction from a biological vantage point and an understanding of hygiene as a more societal and socially related phenomenon. This new terminology could make the education more focused on both of these aspects. The biological education ought to encompass three aspects related to gendered bodies: the anatomy of the genitals, the physiology of how the genitals function, and genital diseases as pathology. Hygiene, on the other hand, ought to include both ethical and medical aspects. It was argued that this new terminology made it more obvious that health was relevant in both the biological and the social realms. Ethics was different from biology, and both were needed (RA, Skolöverstyrelsen).
The new terminology was used in the revised curriculum for upper and lower secondary schools mainly enrolling boys, run by the state in the mid-1930s. The terminology was part of health education included in biology concerning the body, but framed in a new way. Anatomy was important, as well as menstruation, pollution and venereal diseases, in a context that conveyed messages about the desirability of the reproduction of the family and sexual abstinence. Heredity and racial biology might also be included. In addition, the education was expected to include teaching about how alcohol affects both the organs of the body and society at large by causing death, crime and accidents. Hence, in line with the argument made by the National Board for Education, both biological and societal aspects, here framed as risks, were to be taught. Moreover, the negative effects of alcohol, tobacco and drugs at the individual level as well as for the whole humankind were supposed to be included. It was also agreed that the role of coffee and tobacco should be included. For the study of the human body and health, all schools were expected to have collections of “skeletons and other models, anatomical embryonic specimens, and physiological apparatuses” available (Skolöverstyrelsen, 1939, p. 144, 150).
Thus, this new conceptualization of sex education entered secondary schools for boys in connection with bodily risks, as was already part of the health education included in biology, mentioned above. In addition, the biology of sexual life and hygiene was used in the curriculum in teacher training for primary school teachers (Lindgren and Backman Prytz, 2025b). This highlights how crucial the health promotion perspective was in education during this period.
The biology of sexual life and hygiene enters primary school—sex education for boys and girls
The biology of sexual life and hygiene was implemented in the curriculum for primary school in 1942, as part of teaching about nature. The content was formulated in exactly the same way as in the curriculum for secondary schools, as explained above. This meant that, although the students in primary schools were considerably younger than those in secondary schools, and primary school targeted all children, who were obliged to attend, the content of what the teachers were expected to teach was identical and concerned: anatomy, hormones, venereal diseases, reproduction, heredity, chastity and racial hygiene (Lindgren and Backman Prytz, 2021).
In parallel with this revision in primary school, “sex education,” as a specific concept in the context of the curriculum, was also implemented. Sex education should be taught within the subject area of local heritage knowledge, where knowledge about the body was handled. A “preparing sex education” module should be taught from the age of seven (Lindgren and Backman Prytz, 2021). The responsible Minister of Ecclesiastical Affairs made the decision and thereafter designated a new position at the National Board for Education to handle both school hygiene and sex education. A school physician got the job (Herlitz, 1961).
One difference from secondary schools was that primary schools were not expected to have collections of skeletons and similar materials, and girls and boys were usually in the same classes. According to the curriculum, and based on the idea that sex education was a particular topic to be taught, this education could be organized into homosocial groups. However, a female teacher could teach boys and a male teacher could teach girls, which was something new. Another important difference compared to secondary schools was that sex education in primary school was voluntary for both schools and teachers. In fact, the voluntary aspect was very important and triggered questions about how to interpret the material laid out in the curriculum, and whether it was mandatory or not (Lindgren and Backman Prytz, 2025a).
The Minister of Ecclesiastical Affairs also commissioned a government inquiry to provide a proposal about how the content could actually be taught in schools and how teachers could be supported. A group of teachers from various kinds of schools participated in the investigation, together with a bishop, and the school physician who had taken up the new post at the National Board for Education led the group. The results of the investigation were presented as suggestions for two sets of guidelines, one for teachers in primary school and one for teachers in “higher schools” (including lower- and upper secondary, and girls’ schools) (SOU, 1944: 41; SOU, 1946: 55). With these initiatives, sex education had become relevant for both boys and girls across school types as well as in primary schools encompassing pupils of varying ages, from 7 years upwards.
State guidelines propose abstaining from pleasure and desire—removing the clitoris and no glans
The governmental inquiry’s suggestions for teacher guidelines were soon to be published by the National Board for Education. They formed the first teacher guidelines for “sex education” issued by the state, published in 1945 for primary school and 1949 for higher schools (Skolöverstyrelsen, 1945, 1949). Both sets of guidelines included visualizations of both women’s and men’s genitals on four posters (SOU, 1944: 41; SOU, 1946: 55). The images had been discussed at several meetings and were regarded as important. Nevertheless, they were contested in the group finally presenting them; how the state guidelines should present female and male reproductive bodies (Lindgren & Backman Prytz, 2021).
Two of the posters presented female and male genitals in a drawing-like style (Figure 1(a) and (b)). Neither clitoris nor the glans was visualized, or named, in these posters.
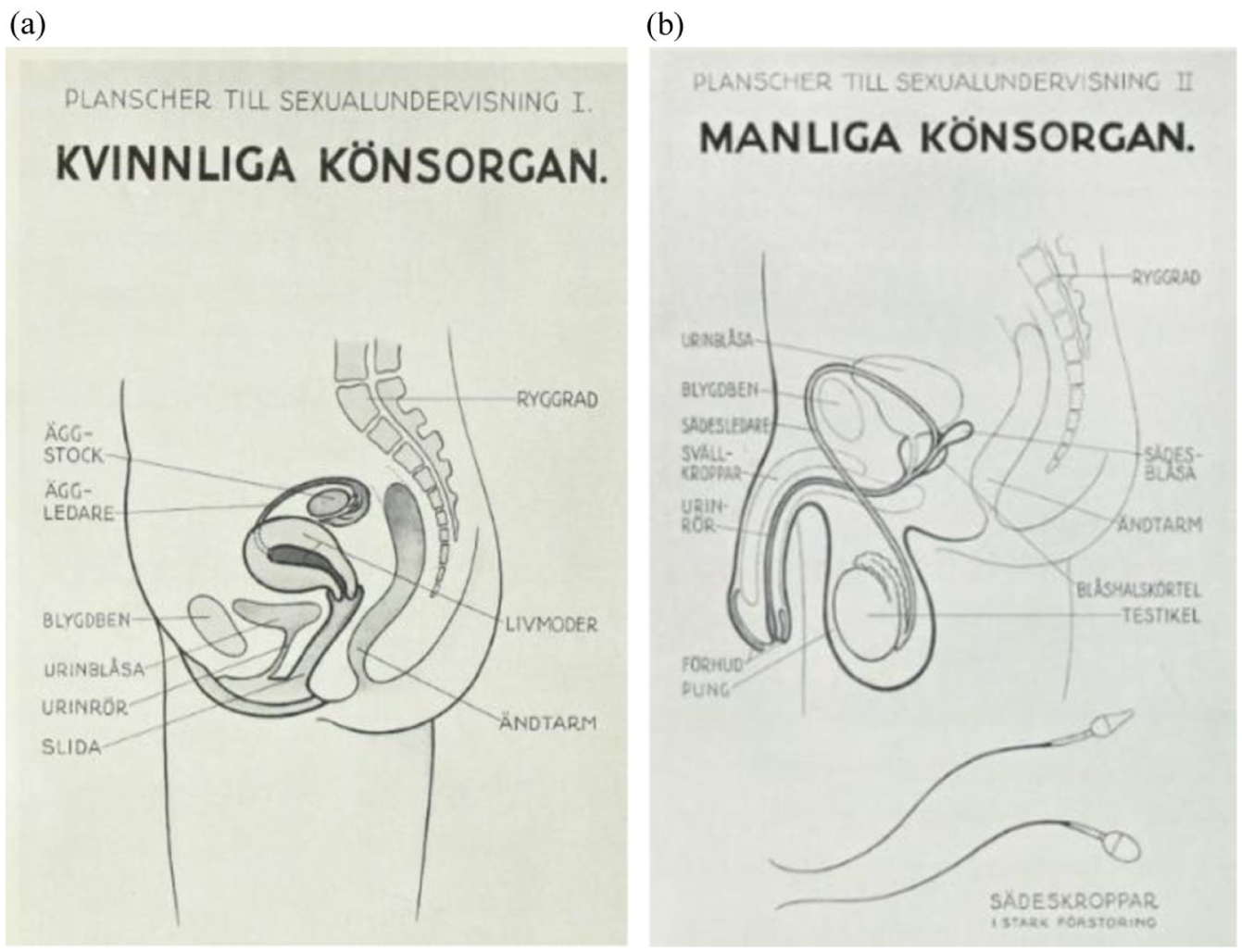
(a and b) Posters of the female and male genitals in the National Board of Education’s guidelines from 1946 and 1949 (first published in SOU, 1944: 41 and SOU, 1946: 55). These posters were reused in the new guide, Skolöverstyrelsen 1956, and in the English translation that was created at that time.
Compared to the visualization and naming in the images used for teaching women’s hygiene it could be argued that clitoris had been removed from visual sex education knowledge when the state took command of the discourse. There were comments at the time about this failure to visualize the clitoris. In a referral to the government inquiry, the Swedish Association for Sexuality Education (RFSU) pointed out that the clitoris was absent from the posters (Lindgren and Backman Prytz, 2025b). We have not found any comments about how the male genitals were presented. However, we want to point out that both the main female and male organ for feeling and acting pleasure and desire were excluded from the anatomy posters published by the state.
The clitoris was also excluded from the proposed teacher guideline texts, where the focus was on the internal female reproductive organs, and the vagina was presented as a connection between the inner and outer organs. The role of the vagina was to “open outwards,” indicating it as a simultaneously passive and welcoming organ (SOU, 1944: 41, p. 47; SOU, 1946: 55, p. 68). For the boys, the external genitalia were the focus of the text; however, the glans was only mentioned as part of the penis, with neither its anatomical complexity nor its function to arouse feelings of pleasure or desire being described. What was said was that the penis “had a task to fulfil, to transfer sperm to the woman’s genitals” and in order to be able to accomplish this the penis had “to be able to become stiff, and that can be accomplished by being filled with blood.” The activity was referred to as a “transfer known as intercourse” (SOU, 1944: 41, p. 49; SOU, 1946: 55, p. 69). Students in higher schools were given some more information about what happens during intercourse: “when the penis in an erect state is inserted into the vagina, through friction against its wall ejaculation is induced” (SOU, 1946: 55, p. 78).
In this way, organs and cells were presented as “gendered agents” (Svendsen, 2017: 145) in a particular way. In comparison, the male organs stood out as more agentive than those of the female, who was expected to be open and welcoming. However, perhaps most striking is the way in which neither agent was ascribed desire or pleasure and, even though the male was more active, his was also a tamed agency. To perform and fulfil a task, and to be able to do so, implied that this was serious business and not something to be done just for pleasure. The penis was inserted and accomplished something thanks to friction, as though the penis was driven by forces outside the man’s own will or control. Moreover, his reproductive organ was just an instrument for a “transference” to occur. Indirectly, however, other messages were also conveyed. The male sperm were visualized as both large and in motion, indicating that they were active gendered agents in relation to the genitals. Egg cells were absent from the female genitals—while just one egg was depicted on a poster about the ovaries. These visual strategies clearly supported the notion that men are more important than women in reproduction.
In the proposed teacher guidelines, the focus was noticeably on sexuality as an act of heterosexual procreation, without any connotations of pleasure or desire. The goal in sex education, to encourage abstinence before marriage, was thus also promoted via visual and text-based descriptions of the bodily organs involved in sexual acts. It was clear that both male and female sexuality should be restricted in order to minimize the risks potentially connected to young people’s sex lives—unwanted pregnancies and the spread of venereal diseases. Having said this, we would also like to highlight the fact that teachers were supposed to actually talk to their students about these “intimate” issues, which in itself can be interpreted as a new and bold form of education (Lindgren and Backman Prytz, 2021). A few years later, the National Board for Education acknowledged teachers and thanked them for taking on the burden of teaching.
More state initiatives—manifesting sex education as a concern for the state
In addition to proposing and publishing teacher guidelines, the state also took other measures to increase its role in relation to school sex education, and thereby take even greater responsibility for health promotion through education. Hundreds of further education courses for teachers in all levels of school were organized in different parts of the nation by the state school agency in collaboration with the regional school inspectors. These consisted of 2- to 4-day courses on topics related to the different concepts used in the curricula for the different school levels: sexual hygiene, sex education and the biology of sexual life and hygiene. Courses in school hygiene also included sex education. In particular, courses targeting teachers in primary schools comprised “exemplary lessons,” simulating a classroom teacher-led sex education lesson with participating pupils (Lindgren and Backman Prytz, 2021).
These exemplary classes were held in front of the teachers attending the course, and taught them how to tackle the teaching of “intimate” knowledge. The courses contained lectures about anatomy, sexual risks and student problems. The lecturers were mainly male physicians, but teachers also participated as lecturers to some extent, and particularly as leaders of the exemplary lessons (Lindgren and Backman Prytz, 2021). Civil society actors offering similar courses were actively excluded from the state-run courses by the school agency (Lennerhed, 2002). Via sex education initiatives revolving around health promotion, the body and risk, the state made itself visible at several levels of schooling within the diverse Swedish education system.
Downplaying health promotion in sex education
During the educational reforms of the 1960s and 1970s, there was no significant interest in sex education, even though the subject was linked to a new area of knowledge; social studies, which was considered important for democratic development. However, an extensive governmental investigation into sex education started during the 1960s and was presented in the 1970s. The goal of encouraging students to abstain from sex was abolished and sex education was presented as “sex and social life education,” and the new teacher guidelines were entitled “social life education” (Skolöverstyrelsen, 1977). In fact, the investigators were critical of including sex education in health education, because this promoted the idea that sexuality is associated with risks. They also explicitly stated that sex education ought not to be related to alcohol, drugs or tobacco, since such a context highlighted risk factors, which was not a good foundation for sex education adapted to what students needed and were asking for. The investigators sided with the student perspective and proposed a form of sex education adapted to that (Lindgren and Backman Prytz, 2025b).
However, the government chose to take “a middle way” (Lennerhed, 2009), and not include education about intercourse for the youngest students (aged 7–9), or education about contraceptives for 9- to 12-year-olds, as proposed by the investigation. Thus, although the state discourse on sex education changed during this time, the changes were not as extensive as the investigators wanted. In the curriculum, sex and social life education was related to alcohol and drugs.
A revival of health promotion and risk—sexuality and relationship education
During the 1980s and 1990s, probably due to the AIDS epidemic, health promotion again became a significant focus. With the 1990s came a resurgence in sex education, now referred to as in-depth social life education, where HIV/AIDS was included. However, the concept never entered the curriculum, where sex and social life education prevailed. School principals were given responsibility for sex education, and the topic was related to issues such as alcohol, tobacco and drugs – essentially in conjunction with education regarding bodily risks (Lindgren, 2025). The new reference material of the 1990s, in contrast, emphasized health promotion as a crucial aspect of sex education and efforts were made to incorporate a more positive perspective on sexuality into the curriculum, also via health (Skolverket, 1995). A government report, presented at an international conference on population policy and health, stated that the transmission of sexually transmitted diseases among the young had decreased, as had the number of unwanted abortions (SOU, 1994: 37). The report stressed a significant link between school sex education and reproductive health, a trend that has since become evident in government health policy.
When the Swedish National Agency for Education was tasked by the government in the late 1990s to review how well schools had fulfilled their objectives, the focus was aligned with three areas: i) bullying, ii) tobacco, alcohol and drugs, and iii) sex education (Skolverket, 2000). Hence, after one hundred years, sex education continued to be accompanied by an emphasis on health risks related to the body. Hence, the health-promotion perspective in education became even more prominent. The major School Commission of 2015, however, showed little interest in sex education. In the final report, sex education was mentioned only once, alongside the education on alcohol, tobacco and narcotics provided by student health services.
Health and honour-based violence—sexuality, consent and relationships
In 2021, the government decided that sex education would be referred to as “sexuality, consent and relationships,” and that it should promote students’ health and well-being. This encompassed “many questions about health” and the area was part of schools’ “health-promoting work” (Regeringen, 2021, p. 57). Consequently, the term social life education, introduced in the 1970s, was abandoned in favor of consent and relationships. Today, this approach to this area of knowledge is justified on the Swedish National Agency for Education’s website by referring to the need to provide students with knowledge about sexual and reproductive health. Furthermore, in subjects such as biology for grades 1 to 9, there are components related to “body and health,” while the later grades cover human reproduction, sexually transmitted diseases and contraceptives. This shows that the health education of the early 20th century continues to resonate within the sex education discourse.
However, in the 2020s, in addition to the old risks associated with sexually transmitted diseases, new health risks are also identified; primarily sexual violence, honour-related violence issues and a consideration of the (lack of) consent. Boys are identified as perpetrators and girls as victims, with the goals stated as: “more boys will understand the difference between consent and assault. And fewer girls will be subjected to sexual harassment and violations, both in school and later in life” (Riksdagen, 2021, p. 125). This represents a different approach to discussing risks compared to the previous discourse surrounding alcohol, tobacco and drugs. However, it continues to focus on bodily risks. Similarly to the approach during the early 20th century, distinctions between girls and boys are still highlighted.
Moreover, it is argued that school sex education is essential when implementing sexual rights and sexual health via the state’s action plan to improve the health of the population between 2023 and 2033 (Folkhälsomyndigheten, 2025). Health promotion is thus given a prominent role. Addressing school sex education in the state’s action plan is new, even though school sex education has been of interest to state politics before. For example, government investigations and strategies for preventing unwanted pregnancies and abortions have commonly referred to school sex education as a tool to implement new policies. This was the case in the 1930s, 1950s, 1990s, 2000s, and 2010s. In fact, these so-called abortion committees have been among the most active players in the state sex education discourse promoting high-quality school sex education (Lindgren and Backman Prytz, 2025b).
Conclusion: Continuity and change
In a study focusing on health education in South Australia from the 1880s until the 1990s, sex education is described as an outcome of health education in the 1960s and 1970s, as a way to counteract young people’s sexual liberation. Sex education continued to be reformed in relation to health education during the AIDS epidemic in the 1980s, promoting more varied and inclusive education supporting health (Gorzanelli and Knijnik, 2025). In this article, by taking our starting point in sex education, we have shown that a health-promoting discourse was prevalent in Sweden from the turn of the 20th century. The discourse also differed from that of South Australia in the 1960s and 1970s, trying to resist what was at the time a strong focus on health promotion in population policy. What happened in relation to the outbreak of the AIDS epidemic was also different in Sweden, and more similar to developments in the United States, with a focus on abstinence and using condoms (Howe, 1990; Lesko et al., 2010; Lindgren, 2025).
As argued in this article, despite several attempts, Swedish school sex education has struggled to renew itself. Perhaps this has been due to the fact that it is an interdisciplinary field of knowledge lacking a clear connection to any specific academic discipline; instead, it has been actors connected to state politics who have taken on the role of ensuring that this area exists and also that it undergoes change (Lindgren and Backman Prytz, 2025b). Sex education has provided a way for the state to make itself visible and relevant by actualizing health and risk issues in relation to children and young people. The health-promotion aspects of sex education have always been at the forefront and this has been a consistent theme from the early 20th century to the present day, with only one exception, during the 1960s and 1970s. This is in line with previous research indicating that sex education has served as a policy instrument to encourage young people to regulate themselves according to majority societal norms where sexuality is associated with risk, as outlined in the introduction. Our contribution is to acknowledge the productive nature of these aspects over more than a century.
Opinions about what is required in order to achieve and maintain positive healthy lifestyles have varied but, as an overarching area related to sexuality, one can still be struck by the strong continuity in how the state discourse on sex education has addressed this topic. Through its focus on health promotion and sex education, this article has provided examples of how in addition to health and risk, gender has been actualized in order to regulate sexuality in the history of Swedish school sex education and how that history is still more present than we often wish to acknowledge.
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the The Swedish Research Council [Ref: 2018-05311].
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.