
Abstract
When discussed in the context of diagnosing or medicating children, psychiatrization is usually portrayed as a more or less monolithic top-down process, which, according to some, enables a child’s right to health, while for others is a form of child abuse. This article challenges these conceptualizations in two steps: First, it draws on available literature on psychiatrization (including its top-down and bottom-up operations, and its ideological and material aspects), and its relationship to various psy-practices, and wider processes of (bio) medicalization, psychologization and reification. Second, using two detailed vignettes from ethnographic research with children and youth in Poland, the article demonstrates that children and youth are not necessarily passive recipients of psychiatrization as they themselves navigate, appropriate, resist, and transform top-down influences. While one vignette details a child’s more or less open resistance to psychiatrization through their attention-deficit/hyperactivity disorder label, the other vignette shows young people embracing and positively identifying with bio and psy-knowledge in relation to depression. However, both vignettes show how children and youth make psychiatrization meaningful as it shapes their lifeworlds, with them sometimes becoming agents of psychiatrization themselves. Our data illustrate the nuances of psychiatrization of, with and by children, and we draw on this to complexify existing literature and framings of psychiatrization.
Introduction
It is increasingly common to see children’s poor mental health spoken about as an epidemic of rising diagnoses. Diverse and contradictory reasons are given for the increase in diagnoses, ranging from the development of more accurate diagnostic practices; increasing pressures on children linked to standardized testing; and structural issues, such as poverty, inequality, and globalization. Another reason given is the psychiatrization of young people–that is, that many societies of the global North but also some in the global South–are now more likely to frame children’s behaviour through the language of mental health, and through therapeutic, psychological and psychiatric discourses.
When discussed in the context of diagnosing or medicating children, psychiatrization is usually portrayed as a more or less monolithic top-down process, which, according to some, enables a child’s right to health, while to others is a form of child abuse (Burstow, 2017). Research into children’s accounts of psychiatrization serves to challenge both adult centric professionalized assumptions of acting in children’s ‘best interests’, as well as more critical sociological assumptions of the top-down medicalization of children’s lives (Brady, 2014; Mills, 2018: 250–251; Singh, 2011; Witeska-Młynarczyk, 2018, 2019). This makes children and young people’s mental health a ‘complex, controversial and contested terrain’ (Mills, 2018: 250).
In this article, we discuss the concept of psychiatrization through both reviewing available literature and thinking about this in relation to empirical examples from our own research. We discuss two detailed ethnographic vignettes of psychiatrization in Poland, to illustrate how children and youth are involved in psychiatrization in different ways – from blocking and resisting, to enabling, its circulation. These vignettes are used to flesh out and unpack the complexities, nuances and overall messiness of psychiatrization (something we argue is missing from much of the current literature).
Psychiatrization: preliminary definition and theoretical antecessors
Defining psychiatrization is notoriously complicated, as the term itself is used in various contexts with widely different meanings. Notions can range from involuntary commitment of individuals to psychiatric hospitals, to being used synonymously for pathologization or invoking a larger social transformation in analogy to medicalization. The Oxford dictionary defines psychiatrization as ‘the process of treating or analyzing something psychiatrically; description in psychiatric terms’, thus emphasizing non-material processes of interpreting or judging an individual or a phenomenon through a psychiatric lens. However, we would like to suggest a broader notion of psychiatrization, which includes both material (e.g. growth of psychiatric infrastructures, private or public research institutions, technological, pharmaceutical or biomedical companies) and ideological aspects (e.g. defining or labelling certain conditions or behaviours as mental disorders) and highlights expansion or growth as its core feature. Psychiatrization, as we understand it, refers to the expansion of psychiatry as institution, practices, and knowledge formation, resulting, for example, in an increasing number of individuals being diagnosed as mentally ill, the permeation of psy-knowledge within more and more areas of life, and the furthering of its impact on and its importance in society as a whole.
In Beeker et al. (in press), we conceive of psychiatrization as consisting of heterogeneous, not centrally controlled sub-processes, which are driven by different agents, for diverse and sometimes even contradicting motives (see Figure 1). Although many sub-processes might be initiated or perpetuated mainly by top-level-agents (e.g. the inclusion of new diagnoses into DSM-5), bottom-up processes seem to play a key role to further psychiatrization, especially in the consumer societies of the Global North. Examples of bottom-up-psychiatrization might be advocacy groups, awareness-campaigns, parents demanding diagnoses and treatment of learning and behavioural problems of their children or people searching for recognition of all kinds of subjective suffering through a diagnosis, which often is also a necessity to obtain financial and social support or to access treatment. This view on psychiatrization is also consistent with Foucault’s (2003) claim that ‘psychiatrization does not come from above, or not only from above’ (p. 295), and can be ‘requested, rather than imposed’ (p. 296). Developing this further, Rose (2007) shows how recent scientific developments permeate the everyday life of contemporary societies, envisioning psychiatrization as an ambivalent reshaping of life (Rose, 2007). For others, psychiatrization is seen as far less ambivalent. For example, Mad Studies and much mental health user and psychiatric survivor research, are forms of knowledge production from those ‘whose lives have collided with the powers of institutional psychiatry’ (Menzies et al., 2013: 14). In these approaches (themselves diverse), psychiatrization is a political act made possible through highly unequal power relations.
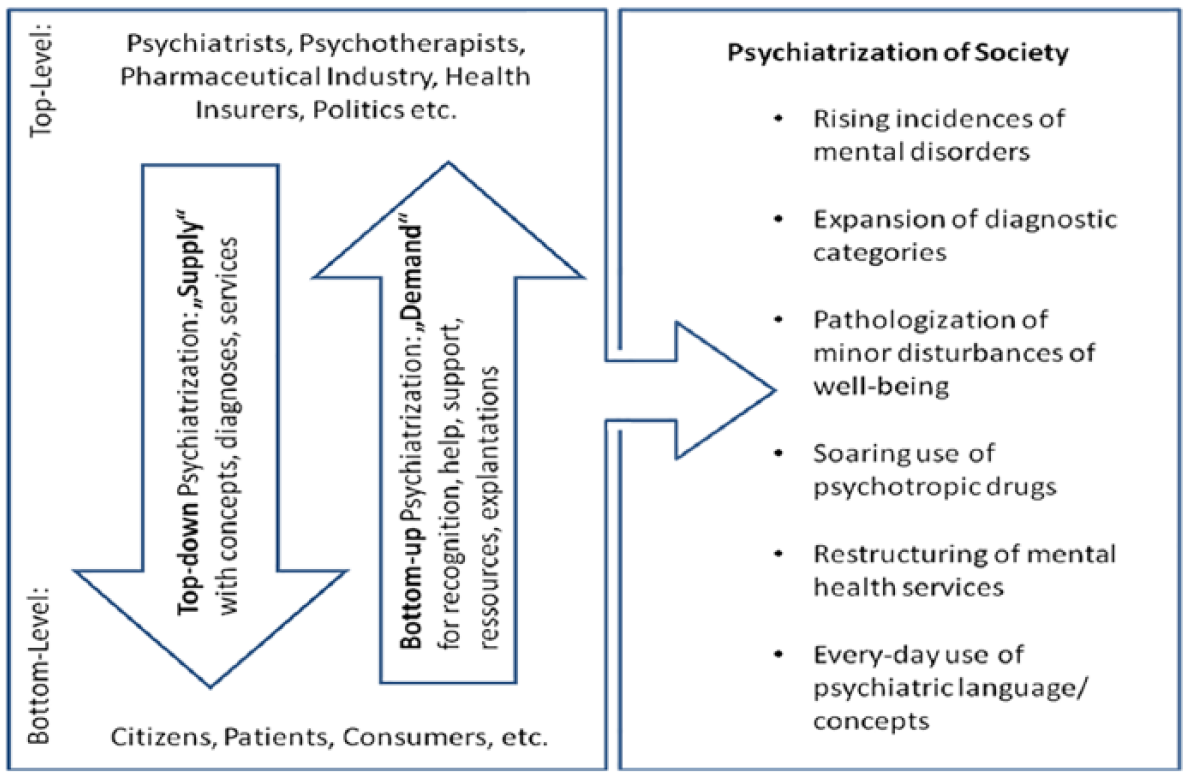
Psychiatrization of society (Beeker et al., in press).
Conceptually, psychiatrization (Coppock, 2002) overlaps with anteceding sociological theories of medicalization and biomedicalization, as well as with later work on psychologization and therapization. The first studies on medicalization were published in the late 1960s, where medicalization was understood as the process of defining and treating problems as medical that previously had been regarded as non-medical, resulting in the expansion of medical jurisdiction into new realms, and signalling a move from understanding deviance as ‘sickness’ rather than ‘badness’ (Conrad, 2007: 6). The concept of ‘biomedicalization’ further emphasizes the role of the bio- and life-sciences in shaping life in ‘technoscientifically enmeshed ways’ (Clarke et al., 2003: 162). Psychologization (Gordo Lopez and De Vos, 2010) and therapization (Ecclestone and Brunila, 2015), complement psychiatrization as ‘processes by which psy-knowledge becomes dispersed and globalised, making psychological vocabularies widely available for understanding ourselves and others’ (Klein and Mills, 2017: 1991).
A strong tendency towards the reification of psychiatric diagnosis by both professionals and lay people might further facilitate psychiatrization. Although it is seldomly linked to psychiatrization, reification (which literally means: to make a thing of) is acknowledged as a profound problem in psychiatry (Hyman, 2010). According to Hyman, reification may partly happen due to the mere act of naming behaviours, which might result in thinking we have thereby explained them. However, the rapid growth of neuroscience adds another layer to the way we conceptualize mental health and its possible treatments (Blum, 2011; Choudhury, 2010; Pickersgill and van Keulen, 2011), and also facilitates reification and psychiatrization. For instance, the generalization of small brain correlates erroneously suggest that all those classified with descriptive diagnoses like attention-deficit/hyperactivity disorder (ADHD) share certain (dysfunctional) brain attributes (Te Meerman, 2019), which can suggest constructs like ADHD or depression are like neurological conditions that need medical intervention. Conceptually, reification can be seen as a process that fulfils ideological aspects of psychiatrization, as it describes how abstract and difficult to define behaviours come to be seen as concrete entities of disorder. However, reification clearly also influences material aspects of psychiatrization if these entities become part and parcel of the (socio-economic) infrastructure, for example, as research programmes become based on these entities and reimbursement for care often requires a diagnosis in many countries.
Psychiatrization and children
In his analysis of the centrality of childhood to psychiatrization, Foucault (2003) explores how ‘childhood as a historical stage of development and a general form of behaviour becomes the principal instrument of psychiatrization’ (p. 304), while simultaneously ‘the position of the child is being redefined vis-à-vis psychiatric practice’ (p. 301). Drawing on Foucault’s work, a wide literature shows the central role-played by the psy-disciplines in the governance of childhood and children (Rose, 1998), through constructions of ‘normal’ development enacted widely but especially within education and health (Bendix Petersen and Millei, 2016; Harwood and Allan, 2014). Psychiatrization, then, is one thread of the wider psy-disciplining of childhood.
In 1979, Castel, Castel and Lovell pointed out that psychiatrization ‘is not a recent phenomenon’, and is particularly evident in the European and North-American 19th-century developments of individualized screening of ‘delinquent’ children–justified as more humane than criminalizing children, yet in this process ‘the whole life of the young delinquent came under investigation’ (Castel et al., 1979: 238).
More contemporary accounts of psychiatrization (though not usually named in this way) are situated within social science literature concerned with the mental health of children. Numerous academic works analyse the narratives of variously positioned actors involved in the practices of caring for children with psychiatric diagnoses – including mothers (Blum, 2015; Singh, 2004), teachers (Malacrida, 2004), and clinicians (Rafalovich, 2005). There is also a rich ethnographic literature of children’s mental health services (Davis, 2016; LeFrançois, 2008; Liegghio, 2016), auto-ethnography by professionals involved in psychiatrization (LeFrancois, 2013), and institutional ethnography of parents’ involvement in psychiatrization (Hande et al., 2016). Other literature focuses on the production of psy- and neuro-knowledge (Hollin and Pilnick, 2015), how this influences children’s encounters with psychiatry (Choudhury, 2010; Rapp, 2011), and how medical uncertainty is managed in various settings, including clinics (Buchbinder, 2015).
Children’s perspectives have been sought on a variety of mental health issues, and experiences of distress and of services (Mills, 2018; Singh, 2011). Much of this literature conceptualizes children as social actors, capable of representing themselves and their experiences, and as active research participants (LeFrançois, 2008; Witeska-Młynarczyk, 2019) or in some cases as co-researchers (Liegghio, 2016). Unsurprisingly, given the heterogeneity of children’s lives, this research shows multiple and sometimes conflicting experiences of psychiatrization. Some research documents top-down psychiatrization, where young people reported having little choice regarding treatment or participation in decision-making (LeFrançois, 2008) and marginalization stemming from the subordinate social statuses associated with being a child, and with having a mental health diagnosis (Liegghio, 2016). Other research shows different interactions with psychiatrization – that may be both helpful and unhelpful in different ways that are often contingent on context.
For example, a systematic review of 38 qualitative studies into the impact of psychiatric diagnosis on young people’s identity shows that diagnoses can be alienating and threatening to self-concept while also facilitating self-understanding and promoting acceptance (O’Connor et al., 2018). In relation to ADHD, research has found that for some children, diagnosis was stigmatizing and something to be kept secret, whereas others found it useful to excuse them of doing things they didn’t like (Singh, 2011). Brady (2014) found that a key part of children’s agency involved them coming to see themselves as mental health consumers, who ‘neither fully accept nor fully reject the medical definition of their experience but actively work to redefine the experience to make it meaningful to them’ (p. 223), partly motivated by a desire to exercise control in their lives.
Young people’s accounts of psychiatrization may challenge dominant adult-centred assumptions–both of acting in children’s ‘best interests’, as well as more critical sociological assumptions of the top down psychiatrization of children’s lives. Thus, instead of assuming the passivity of those being psychiatrized, psychiatrization (as Rose, 2007, argues regarding medicalization) can instead provide a starting point for analysis. The above research shows that children have nuanced understandings of their behaviour, distress and of psychiatrization; and may both resist and sometimes strategically enact psychiatrization.
In this discussion, we reflect upon ways in which young people get engaged in ‘zones of potential circulation’ (Lakoff, 2005: 63) of psy-knowledges and practices, and associated commercial interests. Zones of circulation include global diagnostic manuals, such as the Diagnostic and Statistical Manual of Mental Disorders (DSM), currently in its fifth edition (American Psychiatric Association (APA), 2013); the ways diagnostic manuals, as the primary ‘boss texts’ of psychiatry, are activated by different actors for different purposes (Hande et al., 2016: 87); how diagnostic criteria circulate to professionals and more widely, for example, through their inclusion in University textbooks (Te Meerman et al., 2017); and broader scale transnational flows of psy-knowledge (Bergey et al., 2018), including the power dynamics and coloniality that structure the circulation of psychiatric knowledge and practices in relation to children around the world (Béhague, 2018; Mills, 2014; Witeska-Młynarczyk, 2019).
Methodology
Building on, but differently from, more top-down framings of ‘psychiatrized childhoods’ and rights (LeFrançois and Coppock, 2014), this article draws on empirical data to demonstrate the messiness of psychiatrization in practice, and takes as a focus the ways that those involved in psychiatrization (especially children and adults involved in care) engage in the processes of its reification, including acts of resistance and creative transformation. We aim to flesh out the nuanced ways in which psychiatrization operates in the everyday lives of children and youth.
To do this, we provide two detailed vignettes from empirical research into how psy-knowledges shape young people’s lives and evoke different sets of practices, provoking various responses. We discuss two ethnographic vignettes which complexify discussions of psychiatrization and show how it can be ‘done to’ children, ‘with’ children or even ‘by’ children (Witeska-Młynarczyk, 2019). The vignettes are based on two research projects carried out by one of the authors in Poland.
In Poland, a post-socialist country with a long history of state-controlled healthcare, child and youth psychiatry remains weak and underfinanced, with a lack of professionally trained medics (approximately 430 specialists in the entire country). It is undergoing a process of redefinition (among others, the idea of community psychiatry is taking on significance). Along with the socio-political transition, since the 1990s, on the whole, the Polish healthcare system has undergone a massive and rapid privatization, pluralization of therapeutic practices available to the patient-client who takes on responsibility for choosing the right option, and for whom the healthcare choices are also indicative of social status and life success. The increase in psychiatric diagnoses has been coupled with growing availability of psy-knowledge among teachers, parents and children themselves. The promotion of mental health became a flagship theme for an ineffective and badly reformed Polish educational system taking an impetus coming from larger transnational networks of global mental health and economy of which Poland is a part. Still, due to rapid socio-economic and cultural transformations, Poland remains characterized by a distinctive “cultural disorientation” (Sztompka, 2003) that manifests in everyday life in the form of tensions between the new and progressive with traditional structures and values (including, conservative family and gender relations, traditional model of schooling, rigid doctor–patient relations and alike being challenged by more liberal values and pedagogies).
Vignette 1 is from a research project on children’s experiences of ADHD in Poland carried out by one of the authors. The vignette focuses on ‘Steven’ and his family. The researcher worked with Steven using mainly participant observation and ethnographic interview, and also visited the family on a regular basis throughout 1 year and kept in touch with them for 8 months after the research was completed. The researcher conducted interviews with Steven’s parents and sister, with the teachers and headmaster in Steven’s school, with the psychologist, the pedagogue and the psychiatrist. Notes were taken during Steve’s mother’s consultations with a psychiatrist and in a psychological centre. The researcher also participated in a therapeutic group for boys with ADHD for which Steven showed up only once. Also, as a part of the research, Steven’s Mother (Monica) kept an ethnographic diary in which she described unfolding events, her emotions and reactions to various situations.
Vignette 2 is part of an Internet ethnography conducted by the same author in the Polish context. The researcher followed the Facebook (FB) profile of a group of young women who identify themselves as having had a successful fight with depression and call their group the Porcelain Angels. Over 6 months, the researcher tracked various appearances of the members of the group in the media and observed the awareness campaigns in which the group were engaged. The research was conducted according to the American Sociological Association (ASA) Ethical Guidelines of the Good Research Practice (Association of Social Anthropologists of the UK and the Commonwealth, 2011). All the data gathered in the first project were anonymised. The second research involved the analysis of the publicly available materials, and hence, it did not undergo the process of anonymization. The specific contexts and mental health landscape is integral to each vignette, and is discussed below.
Vignette 1
Psy-practices ‘of’ children
Steven
Steven lives in Malden, a medium-size city in Poland. He is 10 years old. His parents (Monica and Martin) are separated. In financial terms, the family’s situation is stable, and they can afford private medical consultations and a number of extracurricular activities. Apart from the difficulties caused by the separation of his parents, Steven also had to navigate multiple meanings of the ADHD label – itself embedded in discourses and practices of sanism 1 and ableism. 2
During the research Steven was attending his second and third school year. From each school, he was pushed away by the teaching staff. The complaints and pressures from the parents of his classmates played an important role too. Talking about school, Steven reported the disengaged teaching style and the hostile relations between the teachers and the pupils:
In the primary school, the pupils treat the teachers as the necessary evil. Also, that the teachers are like their biggest enemies, that they would not help them with anything. 3
A number of exclusionary practices were pointed at Steven who displayed challenging behaviours in the educational context. The peer group used the psychiatric categories to bully the boy. Steven described the school environment as full of tensions, verbal aggression and prejudices:
What was this conflict about?
I do not know. In general, they were calling me names all the time.
Was it a bigger group?
Yes, they were six or five.
Were they boys from your class?
Yes.
How would they call you?
For example ‘Take the brain tablets!’ and alike.
From the parent’s perspective, the school seemed disengaged from supporting a child with a diagnosis. Some of the teachers actively denied validity to this particular diagnostic category:
‘There is no ADHD’ – a history teacher says.
Does she say it to the parents?
She told it straight into our faces. Absolutely. The natural science teacher, she is about to retire, [. . .] in my opinion, she does not adhere to the recommendations [given by the psychological centre which diagnosed the child].
Such minute interactions portray a chaotic bundle of events which impact the way Steven positions himself towards the ADHD diagnosis and psy-practices performed by the adults. In his case, the ADHD diagnosis is a contested terrain (Witeska-Młynarczyk, 2018, 2019), a statement over which the adults fight. Since the 1990s, the local infrastructure in Malden was taking a new form shaped, among others, by transnational flows of knowledge, goods, and practices involving the increased professionalization of child and youth psychiatry and the encroachment of pharmaceutical companies on a newly freed market. The pharmaceutical companies, together with some of the psychiatrists and patient organizations, got intensively engaged in introducing knowledge about ADHD, diagnostic standards and standardized treatments to lay people – teachers, psychologists, pedagogues, parents and children themselves (Witeska-Młynarczyk, 2019). Steven was diagnosed at the age of 7 in a public psychological centre specializing in diagnosing ADHD. The diagnostic process was run by a psychologist and a pedagogue. Both the psychologist and the pedagogue were trained by a team of psychiatrists specializing in ADHD, who, basing on the DSM and the UK guidelines, worked out standardized tools and measuring scales in the Polish context. The diagnosis issued by the public psychological centre was legally binding for the school. This public psychological centre, quite typically, did not employ a psychiatrist. The staff working there perceived the psychiatrists as ‘mainly prescribing drugs’ and giving ‘10 minutes long consultations’ (Witeska-Młynarczyk, 2019). Steven was not referred to a psychiatrist until he was nine. Still, at that time, it was merely a suggestion on the part of the professionals who diagnosed the boy. He was first consulted by a psychiatrist at the age of 11. Monica, Steven’s Mother, purposefully refrained from medication for a long time, wanting to exhaust other methods, mainly behavioural plans. Yet, when Steven’s behaviours got very difficult for her, and when he was to fail in school, she decided to turn to the psychiatrist. She explained to me that she had wanted to try everything, so as not to regret that there had been an option and she had not tried it. In fact, during the psychiatric consultation about her son’s health, Monica was advised by the doctor to start her own pharmacotherapeutic treatment. When I accompanied Monica at her first visit to a child and youth psychiatrist the doctor was surprised that Steven was not present at the consultation. Monica tried to arrange the consultation away from a psychiatric hospital, in a place which ‘looks more like a psychological centre’. She did not want Steven to think he goes to the psychiatric hospital. Apart from referring Steven to a psychologist with whom the psychiatrist was cooperating, the boy was prescribed psychostimulants. A feeling of shame of being a psychiatric user was being transferred from the mother to the boy.
All those, non-biological factors, had a decisive influence upon Steven’s experience of psychiatrization, not only as being ‘done’ to him, but also, as something threatening his integrity. He acted towards the psy-practices as something he needed to defend himself from: From the fieldnotes: Yesterday, I got a phone call from Monica. She told me that Steven’s ‘oppositional defiant behaviours’ had escalated. We talked about pharmacotherapy. Monica had discovered that about half of the pills prescribed to Steven had found their way under the flower pot at the window still in his room. It is one of the examples when I see children actively negotiating, not only linguistically, the extent to which the psychiatric technology is allowed to enter their lives.
Apart from hiding the prescribed medication, he also rejected the idea of attending a group therapy for children with ADHD run by a psychologist and a pedagogue who diagnosed him. His resistance to psychiatrization seems to make him even more vulnerable, meaning, being exposed to further psy-practices ‘of’ and not ‘with’ (and standing in contrast to the second vignette, detailed below).
Vignette 2: Psy-practices ‘with’ and ‘by’ children
The Porcelain Angels (in Polish Porcelanowe Aniołki) We are teenagers, who, after a successful fight with depression, decided to speak out about this illness, combating the stereotypes. Depression can happen to any of us, including children, and this is no reason for shame.
4
It is with these words that a group of young girls who decided to set up an initiative named the Porcelain Angels introduce themselves on their FB page. One of their stated aims is to build up social awareness of the teen depression in Poland, among others, using social media but also, through active engagements in social campaigns. Explicit in the group’s statement of purpose is the popularization of the view that ‘the only effective method’ of treatment in chronic depression is psychotherapy combined with pharmacotherapy, and, when it is needed, with hospitalization. The narratives the Porcelain Angels popularize are constructed as narratives about successful biomedical treatment. Circulating in the media, was a story of Amelia, a teenage member of the Porcelain Angels, who got engaged in the larger awareness campaign sponsored by the Polish Ministry of Health titled ‘Cure depression’ (in Polish Wylecz depresję). Amelia is the main protagonist of one of the testimonial videos posted on the official website of the campaign. The video starts with the picture of restored family life – Amelia laughs, plays and talks with an adult male (presumably her father) and two younger children in a space which resembles a family apartment. In further frames, she explains her encounters with depression: ‘The symptoms of depression occurred in me in 2015. I was twelve’. In consecutive scenes, the girl describes the escalation of symptoms, including suicidal thoughts. Then, she brings in the description of the resolution: ‘Slowly, thanks to the help of the therapist, thanks to the help of the doctor, the help of the family and friends, I was persistently making those little steps ahead’ – she enumerates the people involved in her healing. The restitution narrative is strengthened by the visual material used. When Amelia says, ‘At that time, when I was depressed, I could not imagine that I could survive till the end of the day’ – in the background we see a wall with inscriptions written in blue ‘born to die’ and next to it, a new phrase, written in black, more visible – ‘born to live’. ‘Now, I have so many plans, so many things to do’ – she says and her smile accentuates the effective transformation.
As is visible in Amelia’s story, Porcelain Angels promote the model of healing that relies on recent biomedical, psychiatric and psychological knowledge and practice. The teenagers, fuelled by their parents, who also take an active part on FB, cooperate with the professionals – psychiatrists, psychologists, and the state officials. As they state on FB: ‘Basing on our own experiences and relying on the help of professionals, we inform the society about the reasons, effects, symptoms, the course and the treatment of depression’.
The activities of Porcelain Angles have their historical and political context. Polish child and youth psychiatry is openly recognized to be in crisis. The hospital wards are being closed. The young patients are being treated at the wards for adults. Media report cases of brutal violation of young patients. The proposed restructuring of the Polish psychiatry towards the community-based practice is in a very early and experimental phase. The excerpts from Amelia’s interview for the Polish weekly magazine Newsweek shall be interpreted in this context: ‘This hospital-stay really helped me. If it was not for the hospital, I would not recover. Cutting off from the reality, the constant support of the psychiatrist, these were the things I needed’. Her voice takes on a political meaning, it works towards building trust towards the institution of psychiatry.
Similarly, one of the fathers, who was actively involved in the Porcelain Angels, took part, along with a psychiatrist specializing in mental health of children and youth and a person involved, in the production of Cure Depression campaign, in a short morning TV show The question for breakfast (in Polish Pytanie na śniadanie), propagating a healthy lifestyle. He explained the mission of the group using a distinction between healthy and sick: ‘healthy children, those who got cured, help to those, who are depressed’. While speaking about his experiences as a father of a child diagnosed with depression, he referred to the present in the studio psychiatrist, stating that ‘the doctor would know best’. The psychiatrist’s voice summed up the meeting, stressing the authoritative position of the psychiatry: ‘Only the professional will be able to say if it is really an illness and how to treat it’. Many engagements of the Porcelain Angels presented on their FB page are meant to reinforce the psy-professionals–like the presence of the Porcelain Angels at the book launch of the text ‘Teen depression: How to recognize, understand and combat’ (Ambroziak et al., 2018) authored by a psychiatrist and two psychotherapists.
In March 2018, Amelia posted on the Porcelain Angels’ FB: A while ago, I attended a conference at the Ombudsman for Children (In Polish Rzecznik Praw Dziecka), which concerned the state of children and youth psychiatry. The situation is tragic. We have one specialist for one thousand patients. This thought is hunting me. It will not be easy to introduce changes to the system. It will be a long road. Now, we finally have to develop prevention, we have to make parents and teachers aware. We have to start speaking openly about psychiatric disorders and about how to prevent them and how to react.
Her words promise an active engagement in promotion of the biomedical model of treatment of young people diagnosed with depression.
Discussion
We draw on the vignettes above to show how children and youth can take very different stances towards psy-knowledge and practices in their lives, from more or less open resistance in the case of Steven, to embracement and positive identification as in the example of the Porcelain Angels. Challenging the assumption that children and youth are mere objects of psychiatrization with little room to mediate its effects, O’Connor et al. (2018) and Singh (2011) have shown that some children may actively enable some aspects of psychiatrization (diagnosis, medication etc.) as it can help them to negotiate their position at school, or find an explanatory framework for their so-called under-achievement, or their distress. The Porcelain Angels take this further, showing how children who might be conceived of as victims according to more top-down oriented theories of psychiatrization, may actively engage in spreading what could be called ‘orthodox biomedical’ psy-knowledge, including its reductionist neurobiological assumptions. Their initiative is an example of a configuration in which children and youth become spokespersons for psychiatrization, spreading the psychiatric vernacular (Behrouzan, 2016), psychiatric labels and specific ways of treatment. Ultimately, the Porcelain Angels appropriate psychiatrization in the very sense that they become vectors of psychiatrization themselves (with likely differing understandings of the larger political and economic psy-circulatory network).
Differently, some children may more actively obstruct the trajectories of psychiatrization. Through hiding pills, Steven blocks the circulation of psy-knowledges and practices, yet at the same time adult interpretations of his behaviour enable circulation. The effects are diverse: although he succeeds in defending what he perceives as his own integrity, his resistance to psychiatrization seems to make him even more vulnerable to psychiatrization as his behaviour can be interpreted as confirming the severity of his symptoms. That children’s’ resistance to psychiatrization may itself be psychiatrized illustrates differential and unequal power relations between psy-professionals and others, and between adults and children.
Other children may neither fully facilitate nor obstruct psychiatrization but instead, as found by Brady (2014), ‘actively work to redefine the experience to make it meaningful to them’ (p. 223). Here, we can’t ignore the centrality of the psy in the contemporary modes of truth-telling, meaning-making, organization, practice, and subject formation and the way these form the possibilities for being a young person or a child (Bendix Petersen and Millei, 2016). These complex discourses and practices intersect and generate the lifeworlds of children, and thus require closer reading of the specific constellations in which both diagnostic instruments, drugs, various therapies, physical spaces, new technologies, beliefs and motifs are at play.
Although children and youth may have agency within psychiatrization processes to a surprisingly high degree, their actions are embedded in networks of relationships and power relations. The Porcelain Angels, for instance, have strong parental support in their self-psychiatrization and on their mission. Differently, the comportment of Steven’s environment appears more ambiguous, making him move on contested terrain: While Steven’s teachers question the validity of ADHD in order to justify a return to more punitive behaviour management, Steven’s parents are actively involved in the psychiatrization of their child (through their support of the ADHD label) as a way to access support for him. Steven’s experience thus illustrates that psychiatrization can be enacted and contested for different reasons by different actors in varied contexts, underlining its complexity and ‘messiness’.
The vignettes also challenge any simple distinction of top-down and bottom-up psychiatrization. One might be tempted to see the Porcelain Angels as a prime example of bottom-up-psychiatrization. However, they clearly identify with and are shaped by circulations of bio-psychiatric knowledge which can be traced back to statements of experts and opinion-leaders in psychiatry. Their activism thus can be seen as reiteration of the biomedical perspective on depression, including its reification as biological, and culminating in the acknowledgement that psychiatrists are the only true experts in this domain. Bottom-up psychiatrization here is inspired or even induced, supported and partly maintained by top-level agents, as its inclusion in the Polish government funded campaign ‘Cure Depression’ also shows.
To add complexity, the Porcelain Angels may also illustrate that top-level agents may encourage and mobilize bottom-up psychiatrization. This top-down supported bottom-up mobilization might be especially powerful, if it mimics, or names itself as a, social justice movement, for example, by appropriating the rhetoric of antidiscrimination or to present itself as a form of scientific enlightenment. This links to patient and parent advocacy groups as key agents of psychiatrization (Hande et al., 2016).
Also, Steven’s example complexifies the understanding of psychiatrization by blurring the lines between top-down and bottom-up processes. His case involves psychologists and pedagogues, who had both been trained by a team of psychiatrists specializing in ADHD, who drew upon the DSM and UK guidelines to develop standardized tools and measuring scales for use in Poland. That the resulting diagnosis led to extra support which was legally binding for the school demonstrates the immense power of DSM criteria, and the ways diagnostic ‘boss texts’ are activated by different actors, sometimes to enable support and care (Hande et al., 2016).
It is also important to draw attention to the contributions of other non-psychiatrists and non-professionals engaged in processes and practices that expand and circulate psychiatric ways of knowing. Here, psychiatrization essentially operates through the doings of an intermediate category of agents such as teachers, who may enact and appropriate psychiatrization in unique ways (Barker and Mills, 2017) or peer groups (Witeska-Młynarczyk, 2019). Thus, psychiatrization of and with children appears to be ‘messy’ in that it involves numerous bundles of situated psy-practices based on medical, psychiatric, neurological, psychological and pedagogical knowledges and economies.
Despite psychiatrization’s ‘messiness’ on many levels, top-down-processes such as including ADHD and other disorders in the DSM still have a fundamental influence in shaping psychiatrization processes by defining their ideological framework. However, Te Meerman et al.’s (2017) analysis of textbooks shows how the psy-knowledge used to scientifically justify the definitions in the DSM may be transferred or spread in very different ways. This heterogeneity also mirrors heterogeneity within psychiatry itself (i.e. rivalling branches), which further complexifies our understanding of psychiatrization by pointing to the fact that there is no such thing as a monolithic ‘psychiatry’.
Possible questions for more detailed research focusing on the psychiatrization of, with, and by children might be: how exactly it resembles or differs from psychiatrization of adults and of the further zones of circulation of psychiatrization, including tracing key actors and interests (financial, individual, and social). An important part of this future research agenda is to explore children’s agency (including how it is enabled and limited), and not to shy away from the complexities and messiness of psychiatrization of, with and by children.
Footnotes
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research was conducted by Anna Witeska-Młynarczyk and it was financed by the National Science Centre (Narodowe Centrum Nauki) in the FUGA scheme (grant number: 2015/16/S/HS3/00150).