
Abstract
Autistic children and young people are at increased risk of mental health difficulties, but often face barriers when seeking help from Child and Adolescent Mental Health Services. This study aimed to (1) explore the experiences of parents/carers seeking help from Child and Adolescent Mental Health Services for their autistic child’s mental health difficulties, and (2) gain parents’ perceptions of the accessibility of Child and Adolescent Mental Health Services for their child. A mixed-methods survey design was used. In total, 300 parents/carers took part from across the United Kingdom. Quantitative data were analysed using descriptive statistics, and qualitative data using qualitative content analysis. Findings demonstrated ongoing struggles that parents/carers faced when seeking help from Child and Adolescent Mental Health Services. Those who were referred reported a lack of reasonable adjustments and offers of ineffective or inappropriate therapies. Ultimately, parents felt their child’s mental health difficulties either did not improve or declined to the point of crisis. However, there was a recognition that some professionals were kind and compassionate. There is a need for a more neuro-inclusive and personalised approach in Child and Adolescent Mental Health Services. Further research, funding and training are urgently needed to ensure support is accessible, timely and effective for autistic young people.
Lay abstract
Autistic children and young people are more likely to experience mental health difficulties than neurotypical peers, but also face more barriers when seeking help from Child and Adolescent Mental Health Services. Findings highlight the need for a more neuroaffirmative approach from the professionals themselves, in the adjustments offered, and in the therapies provided. Barriers to Child and Adolescent Mental Health Services for autistic children and young people include diagnostic overshadowing (i.e. assuming mental health difficulties are part of autism), high thresholds for assessment and a lack of professional knowledge about autism and care pathways. Healthcare policies should ensure that all Child and Adolescent Mental Health Services professionals receive neuroaffirmative training and that resources/funding are provided for appropriate adjustments and early support. There is also a need for further research and funding to develop and evaluate effective neuroaffirmative therapeutic interventions.
Keywords
Introduction
Autism is a neuro-developmental difference in the way the brain develops, meaning that autistic people may process sensory information differently, have different cognitive profiles, and use different communication styles to neurotypical individuals. This influences how they communicate with, behave in, and experience the world. Autistic children and young people (CYP) experience a higher prevalence of co-occurring mental health problems, with around 70% of autistic CYP experiencing one mental health condition, compared to the national average of 12% (Simonoff et al., 2008). Similarly, autistic CYP are up to 28 times more likely to think about or attempt suicide than neurotypical CYP (Cusack et al., 2016) and are more likely to present at Emergency Departments or be admitted to hospital for suicidal crisis (Ashworth et al., 2022; Melvin et al., 2022). While there are multiple and complex factors contributing to the higher rates of mental health difficulties in autistic individuals, key issues are considered to be increased experiences of bullying/victimisation, feeling othered, differences in interacting with the world, misdiagnosis, social isolation or loneliness, societal stigma and a lack of effective support (Mind, 2024).
Consequently, autistic CYP are overrepresented in Child and Adolescent Mental Health Services (CAMHS) in the United Kingdom (Read & Schofield, 2010). In the United Kingdom, CAMHS is a service operated by the National Health Service (NHS) for CYP up to age 18 (although some support individuals aged up to 25), which is free at the point of use (private alternatives to CAMHS are available, but come with an associated cost). However, CAMHS waiting lists can be long and CYP declined appointments, due to both high levels of demand and the stipulated high thresholds of need. This is thought to be due to decades of under-investment and under-resourcing of the NHS as a whole, as well as CAMHS specifically, with only 8% of the mental health budget and less than 1% of the total NHS budget spent on CYP mental health (England & Mughal, 2019; NHS Confederation, 2024). CAMHS provides multiple services across four tiers, spanning early intervention to in-patient provision, involving a multi-disciplinary team. CAMHS offers support for a range of mental health difficulties, as well as assessments for neuro-developmental differences such as autism. CYP need to be referred to CAMHS for support, typically via their doctor or school, although parents/carers can also self-refer. CAMHS will then decide whether they are able to support the young person and, if so, will arrange a ‘first appointment’ to discuss needs and develop a care plan for future sessions.
Despite the overrepresentation of autistic CYP in CAMHS, strategies in the assessment of and intervention for CYP’s mental health needs do not typically take into account neuro-developmental differences, such as the potentially unique needs of autistic CYP, with little focus on the harms that can come with imposing neurotypical standards for all (Hanlon et al., 2022). Indeed, recent findings (Ashworth et al., 2023) indicated that CAMHS was not considered by parents to be accessible for many autistic CYP, and there are concerns that autistic CYP’s mental health needs are often overlooked in assessments, as symptoms are conflated with traits relating to their autism, a phenomenon known as diagnostic overshadowing (Pemovska et al., 2024). In addition, symptoms commonly associated with anxiety and depression, such as avoidance, loss of motivation and sleep disturbance, may not be expressed in the same way as in neurotypical individuals, and may be related to autistic-specific experiences such as autistic inertia and/or burnout (Hanlon et al., 2022). Reports also suggest that CAMHS staff frequently do not feel they have the knowledge or skills to identify and support mental ill health in autistic CYP, and therapists have highlighted concerns over a lack of training (Brookman-Frazee et al., 2012). Thus, autistic CYP experiencing mental ill health are often not assessed or supported effectively.
Recently, multiple national policies focusing on improving mental health outcomes for autistic individuals have been introduced (e.g. NHS England, 2019; Department of Health, & Department for Education, 2017; Department for Education, & Department of Health and Social Care, 2021; Department of Health and Social Care, 2023), as well as investments in researching and developing effective interventions. However, service models continue to focus on ‘impairments’ or deficits in autism, delivering interventions that respond to difficulties rather than building strengths (Hanlon et al., 2022). Such neuro-disorder approaches fail to address the impact of a hostile world on autistic well-being, and distract staff working with autistic CYP from adopting a neuro-inclusive framework of care (McGreevy et al., 2024).
To date, there is limited literature exploring the accessibility of CAMHS for autistic CYP. While studies have examined barriers and facilitators to attaining an autism diagnosis (Crane et al., 2016) and accessing psychological support for neurotypical children (e.g. Reardon et al., 2017), autistic adults (e.g. Camm-Crosbie et al., 2019) and autistic children in in-patient settings (e.g. Cervantes et al., 2019), there is a paucity of research garnering parents’ perceptions of the accessibility of CAMHS when seeking mental health support for their autistic child. To date, only one study (Read & Schofield, 2010) has examined parents’ perspectives of access to CAMHS for autistic CYP in the United Kingdom, and this was over a decade ago. Indeed, a recent meta-analysis of mental health provision for autistic CYP identified a lack of research relating to specialised care pathways, service-wide adaptations, and professionals’ knowledge (Pemovska et al., 2024). Thus, this study aimed to (1) explore the experiences of parents/carers seeking help from CAMHS for their autistic child’s mental health difficulties, and (2) gain parents’ perceptions of the accessibility of CAMHS support for their child and understand potential improvements.
Methods
Design
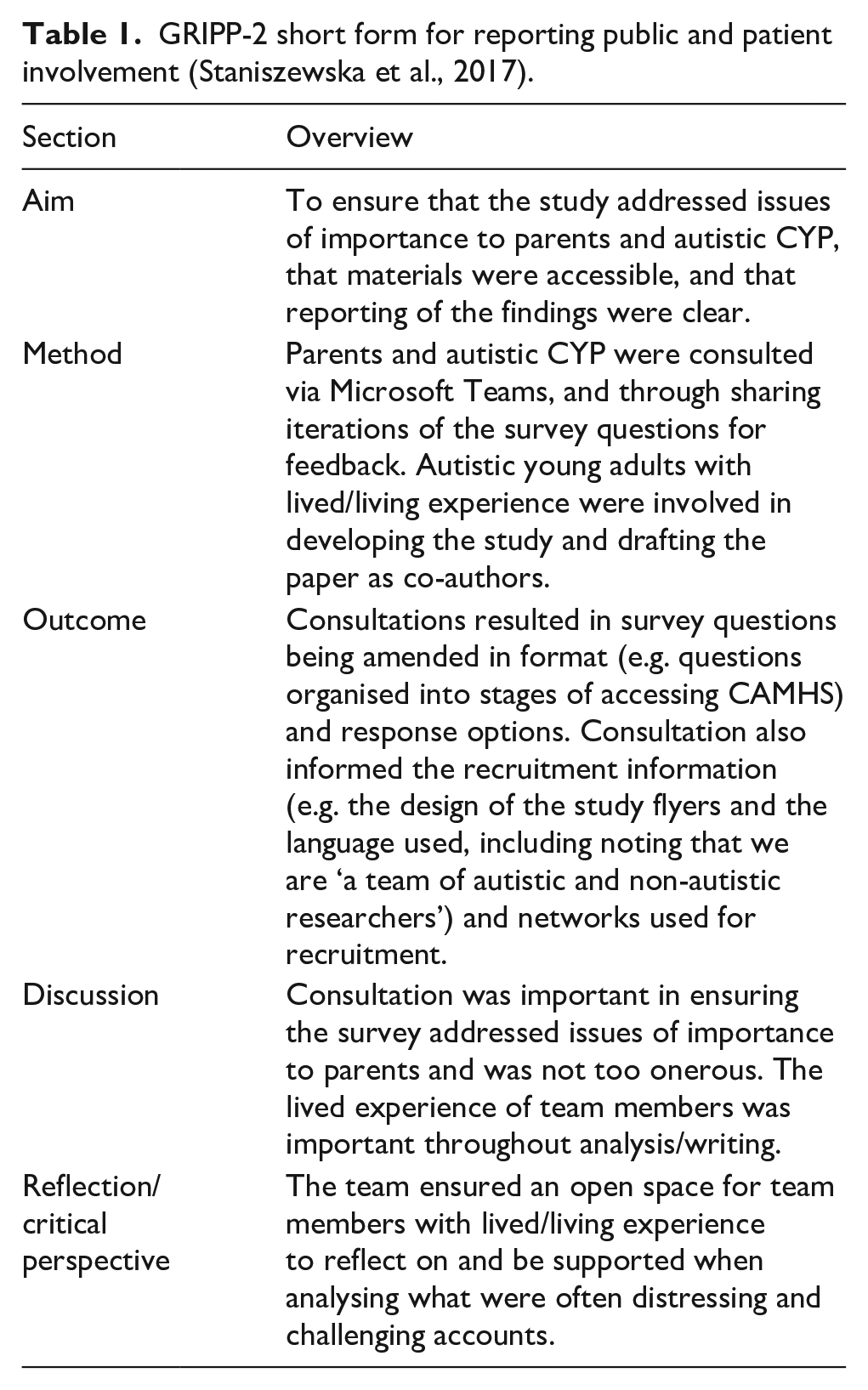
A mixed-methods concurrent exploratory design (QUALquan) (Creswell & Plano Clark, 2007) was used. The qualitative approach was dominant to allow participants to raise issues and share experiences of importance to them, while the quantitative element was considered supplementary, to provide further contextual information. Ethical approval was provided by Liverpool John Moores University’s Research Ethics Committee (ref:23/PSY/046). The team engaged in consultation with autistic adults and CYP, and parents of autistic children, to inform all stages of the study. This is reported according to the GRIPP-2 short form in Table 1.
GRIPP-2 short form for reporting public and patient involvement (Staniszewska et al., 2017).
Participants
Parent/carers were recruited using volunteer/opportunity sampling, via social media (e.g. Facebook support groups and using ‘hashtags’ on Twitter/X), and through the sharing of study materials via relevant organisations and networks (e.g. parent/carer forums). Parents were invited to take part if they lived in the United Kingdom and had an autistic child who had experienced mental health difficulties, for which they had sought professional help in the last 5 years.
In total, 300 parents/carers participated. The majority (87.7%; n = 263) lived in England. Their children were aged between 5 and 25 years (mean age = 13) and girls were the largest single group (48%; n = 144). In all, 84.7% (n = 253) also had another long-term health or neuro-developmental difference. Table 2 provides further detail.
Participant demographic detail.
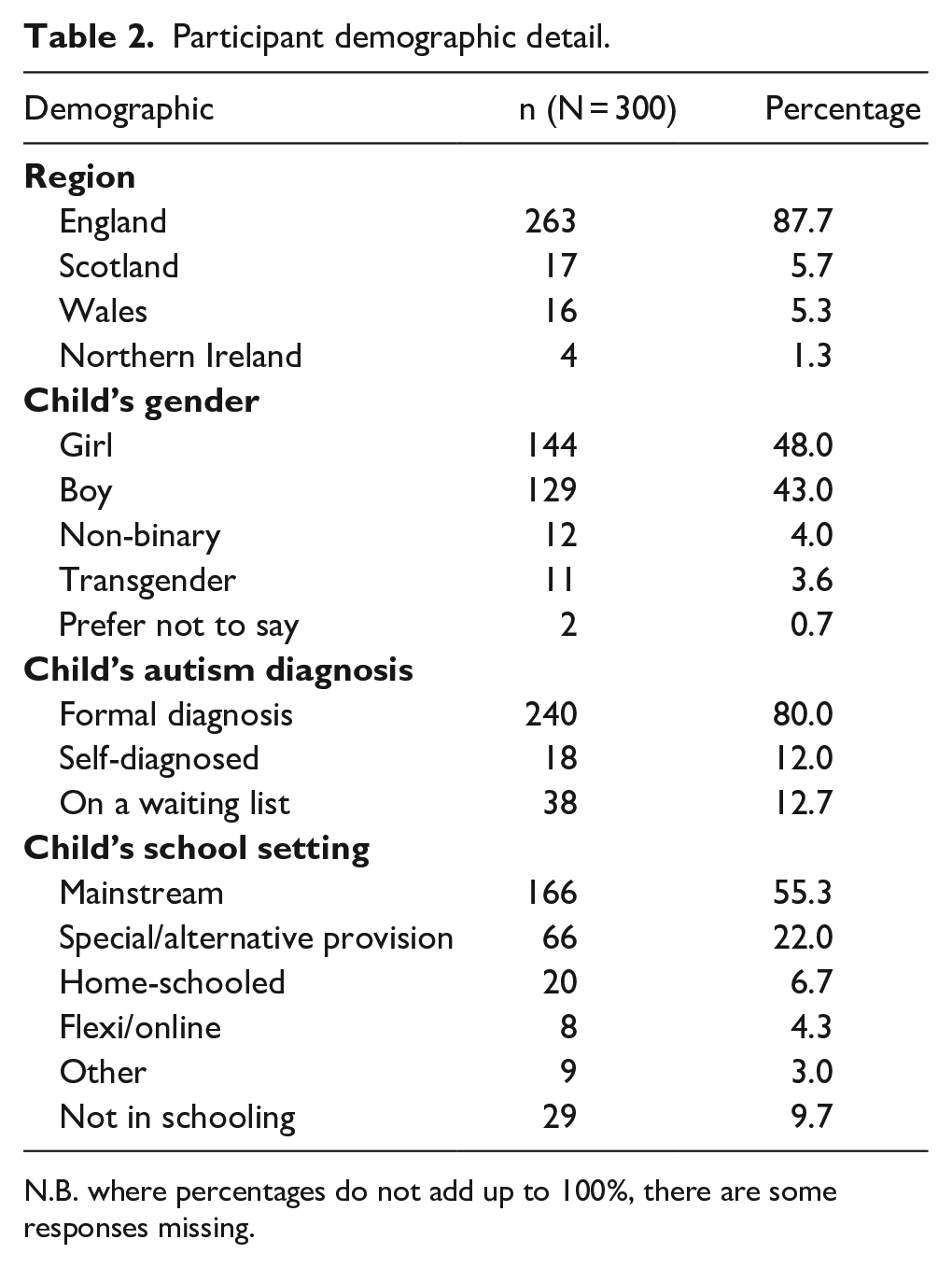
N.B. where percentages do not add up to 100%, there are some responses missing.
Data collection
A mixed-methods survey, dominated by exploratory qualitative questions, was developed for this study (Braun & Clarke, 2022). The survey was shared online via QuestionPro (https://eu.questionpro.com/) between June and October 2023. The survey included open and closed questions grouped into sections, each exploring a different point along the care pathway (e.g. seeking help, first appointment – see supplementary materials). Surveys began with opt-in consent and demographic questions, before exploring parents/carers’ experiences of seeking and accessing CAMHS support for their child.
Analysis
Descriptive statistical analyses of quantitative data were conducted in IBM SPSS v27 by one author (H.S.). Qualitative responses were extracted and collated in Microsoft Word, and were analysed using qualitative content analysis (Hsieh & Shannon, 2005) by three authors (E.A., C.H., and L.B.). Each author independently analysed qualitative data from one section of the survey (seeking help, support from CAMHS, after CAMHS). Qualitative data were read word-by-word to derive codes, which were subsequently labelled and developed into initial codes. All developed codes were then discussed and reviewed in a reflexive team meeting with the three analysts, whereby categories were created, discussed, and agreed. Codes were sorted into categories to organise and group them into meaningful clusters. The occurrence of codes was also counted and quantified where appropriate, to understand relative frequency of responses.
Reflexivity
In line with a reflexive approach, we acknowledge how our lived experiences and interests may have influenced our approach and interpretation. We have academic and professional experience from our work within the fields of health, psychology, counselling, and special educational needs and disability (SEND) provision, as well as personal experience. The team is made up of neurodivergent and neurotypical individuals, and parents of neurodivergent children. In line with a reflexive approach, we did not aim for ‘accurate’ or ‘reliable’ coding (Byrne, 2022) or the use of rigid coding frameworks when analysing the qualitative data. When discussing findings, the team reflected on the assumptions and expectations they brought to the work, as well as how their own experiences may have influenced their interpretations of the data.
Findings
Findings are presented below, grouped into parents’ experiences at each point of the care pathway. Relevant quantitative data are presented alongside the qualitative data. As some parents/carers did not answer every question, percentages are based on the total number of responses for each question. Overall, findings portray that CYP are reported by their parents/carers as accumulating trauma and experiencing worsening mental health along the care pathway, waiting for inevitable crisis. This summary of the findings, including barriers to accessibility at each point and the resultant impacts, is depicted in Figure 1.
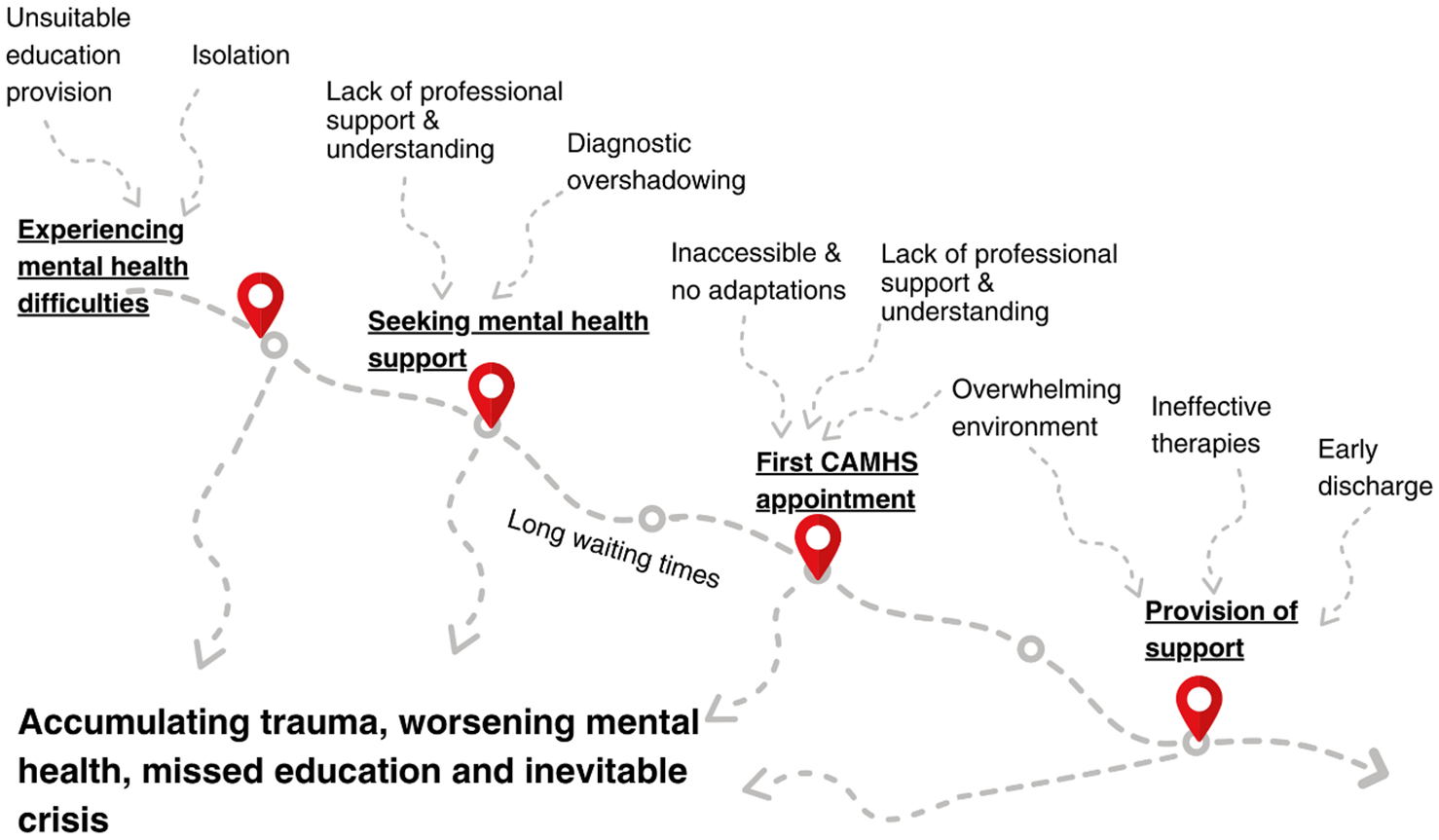
A summary of findings.
An overview of experiences
Figure 2 provides a visual overview of the pathways taken by CYP and their parents when seeking help. As can be seen, almost half of those who sought help (46%) were rejected for an assessment by CAMHS, and only a small proportion (9%) of parents felt that their child’s mental health improved as a result of their interaction with CAMHS.
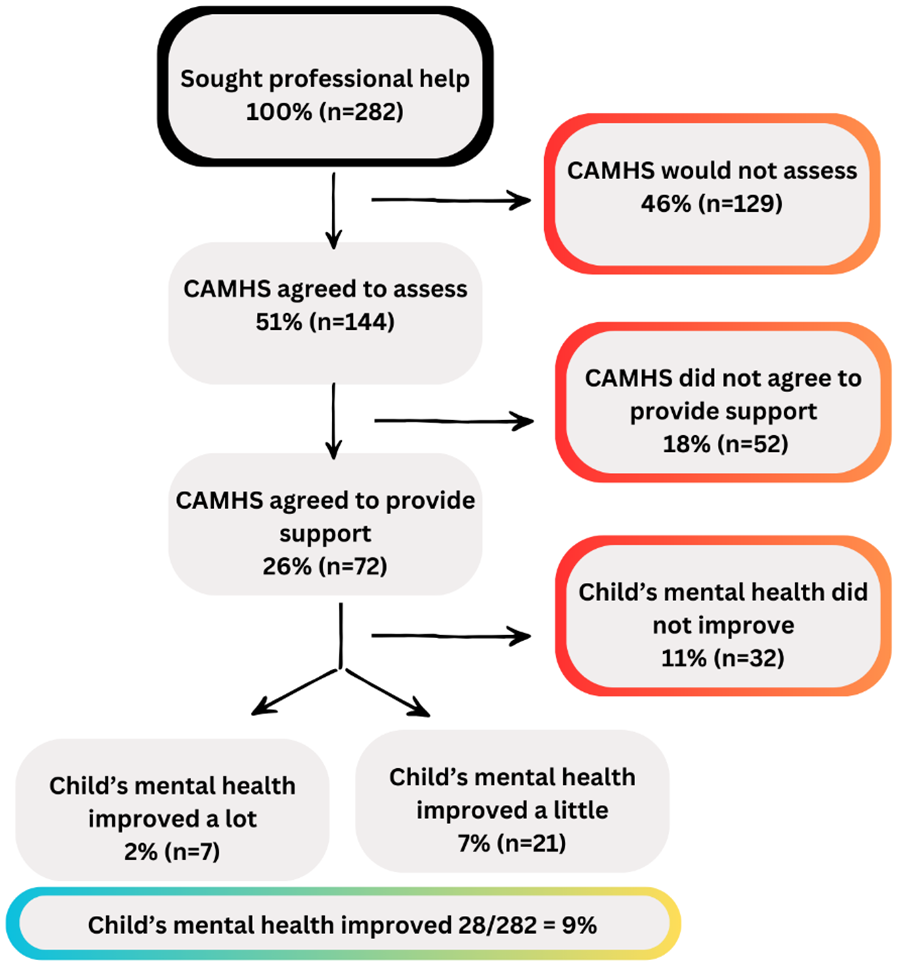
Flowchart of experiences on the care pathway.
Mental health difficulties leading to seeking help
Parents were asked to describe the mental health difficulties that first led to them seeking help for their child. Responses were coded and the number of code occurrences counted. The most frequently cited difficulty was anxiety (n = 154), followed by school-based anxiety or difficulties at school (n = 96), and suicide ideation (n = 83). Table 3 provides an overview of each response type.
Reasons for seeking help for mental health difficulties.
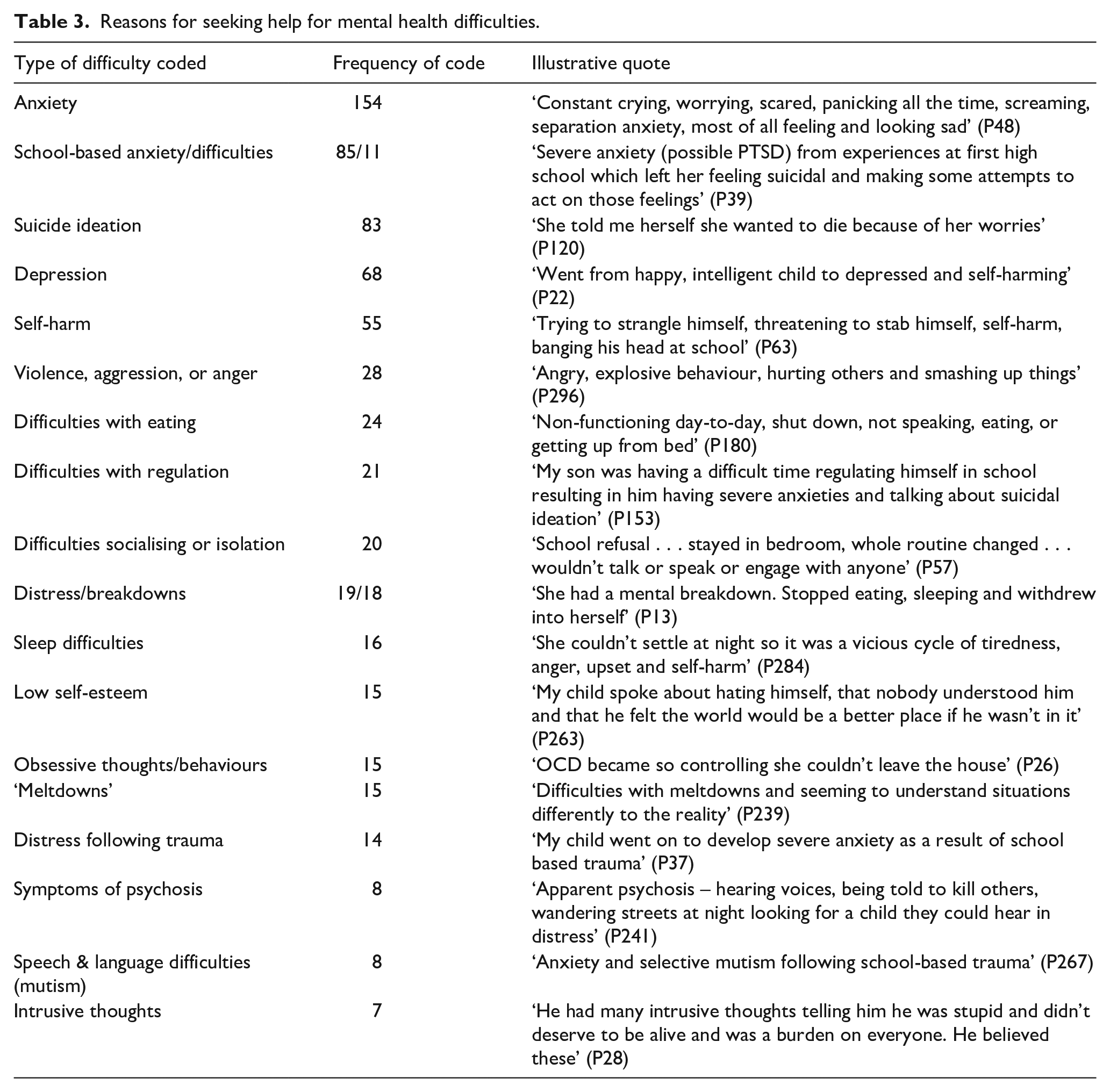
In all, 90% (n = 270) of parents reported that their autistic child’s ability to engage with their education had been affected by their mental health difficulties, and many reported that their child’s difficulties were due to attending schools which had outdated perceptions of autism or were unable to meet their needs. As a result, parents reported that their child attended school for an average of 2.7 days per week: ‘the focus is on forcing autistic children to adapt to schools designed for neurotypical children, which is impossible and results in avoidable mental health problems’ (P30).
Parents’ accounts described the mental health impact of attending an unsuitable education setting: ‘[schools have] an out of date understanding of autism. Better training for teachers and in-school professionals could prevent the need for some autistic children to access CAMHS’ (P194), with safety often a key issue: ‘we wouldn’t have a child with this level of anxiety if they had been able to access education in an environment that made them feel safe, understood, and was flexible to their individual needs’ (P62). The level of anxiety that school caused was often discussed: ‘intense anxiety, especially about attending school. Panic attacks, dangerous behaviour such as running into moving traffic to try to avoid going to school’ (P95), with one participant describing this in more detail:
The setting of school can be simply overwhelming to some autistic children (too busy, too many people, too loud, too bright, too many instructions, too many changes etc). School staff are not trained, equipped or resourced to understand how to meet the needs of an ND child. (P168)
Seeking mental health support
Parents were asked to indicate who they first spoke to about their child being referred to CAMHS for mental health difficulties. The majority (48.2%; n = 136) said they had first approached their General Practitioner (GP), followed by school/nursery (27.0%; n = 76), a paediatrician or hospital (11.0%; n = 31) and 7.8% (n = 22) said they self-referred.
In all, 56.6% (n = 158) felt their child received a referral when they needed it, 41.6% (n = 116) felt they did not, and the remainder stated they were not sure. Parents were asked to explain why they did not feel they received the referral when needed, stating issues with diagnostic overshadowing (‘it got rejected because ‘anxiety is part of autism’ (P37)), their child not being mentally unwell enough (‘only listened to when the self-harm and risk of suicide escalated. We had to be in crisis before we got any help. Kept being told that we didn’t meet threshold’ (P38)), long waiting times (‘school said they would wait forever, no point’ (P41)), poor communication between the school and GP (‘doctor said school should refer, school said doctor should refer’ (P64)) and schools refusing to refer (‘teachers thought there was no issue and my child was just naughty’ (P231)).
Of the parents whose child was referred to CAMHS, 50.0% (n = 144) said that CAMHS agreed to assess their child, 44.8% (n = 129) said they did not and 8.0% (n = 15) were not sure. Where CAMHS did not agree to assess their child, parents were asked to explain the stated reason and what happened next. Common responses included their child not meeting the threshold of need (‘I was told she doesn’t meet the criteria as she isn’t in crisis or harming herself’ (P103)), lack of clear pathways (‘they said he’s autistic and they don’t deal with autistic children’ (P105)), diagnostic overshadowing (‘assuming that autistic children should automatically be anxious as part of being autistic’ (P259)), blaming parenting style (‘was told to do parenting course and be stricter’ (P94)), that the service was not appropriate for an autistic child (‘they felt his ability to engage would not make any programme of work effective enough’ (P181)) or that no reason was given (‘refused initial referral but didn’t communicate this with anyone!’ (P69)). As a result, many were forced to seek private help: ‘if we had not gone privately, I don’t know where his life would have gone’ (P160).
For the children who were added to a waiting list for support, 48.9% (n = 68) of parents indicated that their child waited 0–6 months, 18.7% (n = 26) waited 7–12 months, 23% (n = 32) waited 1–2 years, and 11.5% (n = 16) waited more than 2 years. 4.3% (n = 6) of parents did not know. In all, 79.1% (n = 102) of parents said they were not offered any other NHS support while on the waiting list. While the number waiting 6 months for an appointment is broadly in line with national rates (48.8% waited 6 months vs 60% typically seen within 4.5 months), the proportion waiting more than 1 year is significantly higher (34.5% vs 4.6%), according to figures from the Royal College of Paediatrics and Child Health (RCPCH, 2023).
For those who were offered support, examples included GP follow-up appointments, parenting courses and online therapy programmes. Parents described the negative impacts of the long waiting lists without support, highlighting how their children’s mental health continued to worsen to the point of crisis: ‘you just sit on lists until things get so bad they have to help, or they’re too late and another young person loses their life when it could have been prevented’ (P84).
Attending the first CAMHS appointment for assessment
Parents whose child received a CAMHS referral (N = 144) were asked about their experiences of their first appointment for assessment.
In all, 66.2% (n = 88) reported that their child’s autism diagnosis was disclosed to the CAMHS professional, and 64.0% (n = 55) said that this was before the first appointment. Despite this, the majority of parents who had disclosed their child’s autism diagnosis (70.5%; n = 55) reported that no reasonable adjustments were made. The majority provided examples of a lack of reasonable adjustments to the environment: ‘not at all. Waiting room busy and noisy . . . bright lights and music’ (P111), and ‘not in any way which led to the meltdown. Nurse was late. Was left in a busy waiting area and no sensory equipment offered’ (P78).
Of those who indicated that some adjustments were made, many felt these were still ineffective: ‘they got out some sensory objects but only after she showed signs of distress in the waiting room’ (P194). However, a small minority of parents indicated positive adjustments: ‘lots of sensory toys and fidgets. The CAMHS lady was accepting my daughter wouldn’t look at her and kept jumping into a bean bag while talking’ (P256).
In all, 53.6% (n = 67) reported that their child did not feel ‘at all’ comfortable explaining their mental health difficulties to the CAMHS professional, 28.8% (n = 36) felt ‘a little bit’ comfortable and 12.8% (n = 16) felt ‘quite’ or ‘completely’ comfortable. The remainder did not know or said that their child could not engage. Parents/carers explained that their child did not feel comfortable with the reliance on verbal communication and the expectation for them to be able to understand and articulate their thoughts and feelings to someone they did not know: ‘my daughter struggles to talk to strangers and so I did all the talking away from her while she played’ (P184), ‘she finds it’s difficult to explain what she’s feeling and why’ (P74) and ‘as they are non-verbal it was difficult for them to communicate’ (P3). One parent summarised:
Expecting a 7-year-old to be able to talk about these topics on the phone is a massive ask especially for an anxious autistic child . . . they should have tried inviting the child into a room with toys/art materials and talked to them while they were playing/creating. (P81)
Many parents explained the negative impact of these often-difficult interactions, as in the following case: ‘very distressed and overwhelmed . . . My daughter was forced into a meltdown when the nurse asked around 50 direct questions on the first appointment despite me explaining she wouldn’t cope’ (P78). While the majority of the experiences were negative, there were a small number of positive comments relating to the kindness of the professionals, which helped to increase comfort: ‘the person was supportive and kind’ (P32) and ‘as it was the same person each time she built up trust to say what was needed’ (P93).
When asked to report how helpful the first CAMHS appointment was, 53.9% (n = 69) did not find the appointment helpful for their child, and 24.2% (n = 31) said their child could not engage. When asked why they did not find it helpful, parents indicated that they felt blamed for their child’s mental health difficulties: ‘basically blaming ASD and not parenting my child properly. Really insulting and did not engage well’ (P193), or that their child felt blamed, ‘she was made to feel bad for her worries, questioned a lot, and was embarrassed because she was made to feel silly for her worries’ (P120).
Some parents reported that the professionals did not recognise that their child was masking, 1 ‘they masked, all answers taken at face value when they were fawning’ 2 (P137), or have an appropriate level of knowledge about autism: ‘they didn’t assess him accurately and would not refer him. They did not seem to understand autism. They said his anxiety was because of his autism which is not only untrue, it is a damaging perception of autism’ (P43). Parents also felt that some professionals minimised their child’s difficulties or said they were not severe enough: ‘CAMHS told me my child had no enduring or significant mental health difficulties. After this appointment my child became very withdrawn and basically went into crisis about 10 days after the appointment’ (P81).
However, similar to above, there were a small minority of positive comments, which generally focused on the kindness of the professionals, and advice regarding an autism diagnosis: ‘they were the first professionals who understood and offered reassurance and advice. They also pointed out that she may be autistic’ (P184). Several also reported that they were advised to seek help elsewhere which, while not ideal, did help them ultimately receive the support their child needed: ‘being told off the record to go privately for therapy. And luckily we are in the financial position to be able to do this. Most are not’ (P160). Staff within CAMHS were also described by some parents as helping to identify environments which may be harmful to their child’s mental health: ‘they were the first professionals who actually identified the real problem and solution, which was school and its approach to autism inclusion. Everyone else had blamed our son for his anxiety’ (P30).
The provision or offer of further support from CAMHS
Parents who received an initial CAMHS appointment (N = 144) were asked whether CAMHS agreed to continue to provide support. In all, 55.0% (n = 72) reported CAMHS did agree to provide further support, 5.3% (n = 7) did not know and 39.7% (n = 52) reported CAMHS did not agree. For the parents who were not offered further support, they were asked why not and where they were signposted to instead. Common responses included that their child was not considered to be engaging enough, did not meet the threshold of need or were being discharged due to being autistic, for instance, ‘anxiety related to autism and discharged’ (P137), ‘just told I had to call back if got worse or call ambulance if needed’ (P89), and ‘they told me that she would not be able to access any of their services because she would be too anxious and upset to get to the meetings’ (P194). Regarding signposting, a large portion of responses stated being directed towards charitable services, as well as informative resources to assist in managing/coping: ‘was told to read a book’ (P197).
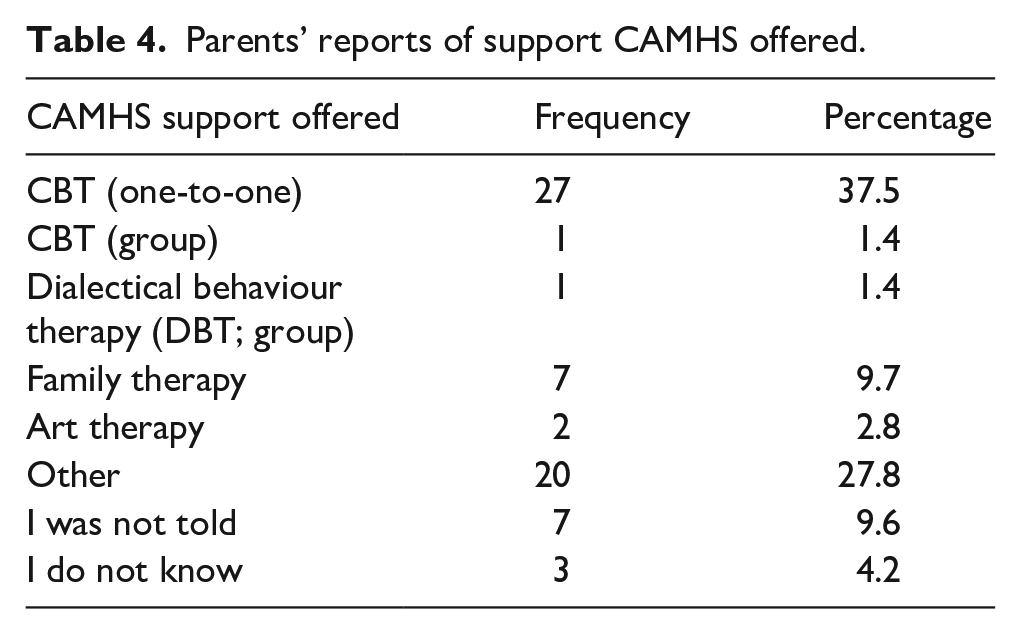
The majority of those provided with further support (39.7%; n = 27) were offered one-to-one cognitive behavioural therapy (CBT). Other support offered is listed in Table 4. Only 23.4% (n = 15) of parents thought that their child felt comfortable or able to partake the support that was offered. When asked to explain their answers, parents typically focused on the need for appropriate, neuroaffirmative therapies which would help their child engage and would not cause further harm or ‘force the child to mask further’ (P41): ‘would like to see access to therapies other than CBT and DBT! I would like to see a service which is neuroaffirmative and seems to understand the needs of autistic young people’ (P300). One parent explained:
CAMHS causing more harm by offering therapies which are inappropriate e.g. CBT, DBT, PBS – There needs to be safe spaces and trusted and trained adults where they can go to be themselves and therapies to let them express freely, not made to conform. (P63)
Parents’ reports of support CAMHS offered.
Parents were asked whether they felt their child’s contact with CAMHS improved their mental health. In all, 51.6% (n = 32) felt that their child’s mental health did not improve ‘at all’, 33.9% (n = 21) felt that it improved ‘a little’, 6.5% (n = 4) felt that it improved ‘quite a lot’ and 4.8% (n = 3) felt that it improved ‘very much’. Finally, parents were asked what the most positive thing had been; comments mostly focused on the professionals themselves, describing them as ‘kind people’ (P23), and parents explaining ‘it felt like they wanted to support us’ (P188). However, there were very few positive comments generally (‘nothing, only medication has kept my son alive’ (P286)).
Improving mental health support
The final questions asked parents what support they would like to see for autistic CYP to help their mental health, both generally and when accessing CAMHS. The majority focused on the benefits of early, preventive interventions to help autistic CYP thrive before mental health difficulties develop: ‘the length of time or delays in getting support in place means that trauma is inevitable. With effective, efficient scaffolding those ND children are less likely to spiral into mental health crisis’ (P168). This early intervention would include improved post-diagnostic support: ‘there is nothing post-diagnosis which is awful . . . there should be a separate mental health/autism team who support families once diagnosed!! . . . we are left with a few agencies who provide short term, like counselling or signposting!!’ (P165). Many of the parents also identified the importance of fostering a sense of belonging and community as a protective factor: ‘we wouldn’t have a child with this level of anxiety if they had met peers who were similar to them . . . They’d feel less lonely and their anxiety would be reduced. They’d be more independent and have improved self-esteem’ (P62).
Several parents reported that the harm caused to many autistic CYP in accessing education in unsuitable settings could be mitigated by improving staff training, flexible safe spaces, and increased alternative provision: ‘schools need to be much more aware, flexible and understanding of needs and there have to be autism specialists in every secondary school’ (P241). Several parents also identified the need for interventions to be delivered by dedicated mental health provision for autistic CYP: ‘an ongoing drop-in service for autistic kids only with practitioners trained in evidence-based therapies proven to be supportive of the autistic neurotype’ (P213), and the need for all professionals working with autistic CYP to be up-to-date in neuroaffirmative approaches:
CAMHS need to understand what autism means, and use a neuro-affirming approach. They should stop using the basic approach to anxiety which is to assume it is illogical and use exposure therapies. Instead they should investigate whether the anxiety is perfectly logical – for example a stressful sensory environment. (P80) An understanding that autistic children present their mental health problems differently and are as entitled to universal, targeted and specialist mental health support, just like others are. Then support, advise, assessment and interventions that are neurodevelopmental trauma-informed, autism-appropriate, and neuro-affirmative. (P37)
Discussion
This study addresses gaps in understanding around the experiences of parents seeking help from CAMHS for their autistic child. Findings highlight the health inequalities experienced by this group, who are already at increased risk of experiencing mental ill health and suicidality. While this study was focused on UK CAMHS settings, findings still offer important insights for other healthcare systems internationally. A summary of the issues identified, along with associated considerations and recommendations for practice, is provided in Table 5; however, key points are also discussed below.
Summary of key issues and associated recommendations.
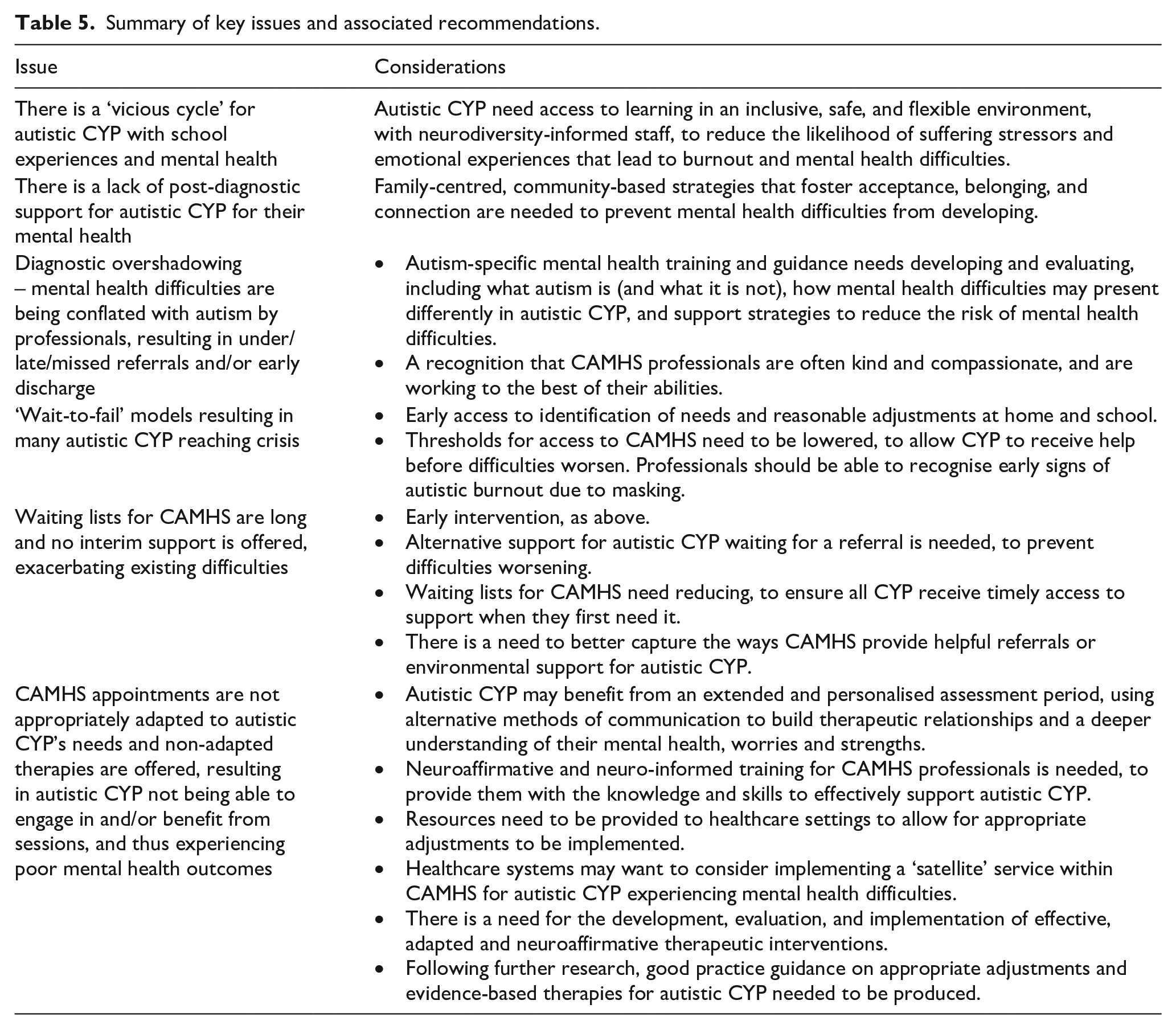
Findings demonstrated the ongoing struggles that parents faced when seeking help from CAMHS. Many of their children were either not referred to CAMHS to begin with or were rejected without an assessment, often due to issues relating to diagnostic overshadowing, a high threshold for assessment or a lack of professional knowledge about autism and care pathways. Those who were referred reported a lack of reasonable adjustments and offers of ineffective therapies, leaving CYP feeling uncomfortable, unable to engage, and thus not benefitting from the service. Ultimately, parents felt their child’s mental health difficulties either did not improve or declined to the point of crisis, felt blamed by clinicians and reported an overall lack of support. Consequently, parents expressed a need for a more neuroaffirmative approach in CAMHS, from the professionals themselves, in the adjustments offered and in the therapies provided (i.e. approaches that recognise the need to personalise strategies for different sensory and communication profiles, and that recognise minority stress and adversity as well as strengths of autistic individuals). Worryingly, the findings closely align with those from Read and Scofield (2010), conducted almost 15 years ago, suggesting that little may have changed regarding access to CAMHS for autistic CYP.
While limited evidence from parents’ or children’s perspectives exist, a recent report (Smith, 2024) suggested that autistic CYP felt the support they received from CAMHS often centred around identifying symptoms and deficits rather than addressing the root causes of problems, that anxiety and autism are considered by professionals to be synonymous, that CAMHS should offer appropriate and effective therapies and that there needs to be a greater understanding of autism within services. Additional evidence exists highlighting how parents feel blamed by professionals for their autistic child’s mental health difficulties (Jackson et al., 2020). More generally, a systematic review of barriers and facilitators of healthcare access for autistic CYP (Babalola et al., 2024) identified many similar issues to those reported here.
Results from this study highlight clear implications for policy and practice, as well as future research directions, in order to better meet the needs of autistic CYP in CAMHS and reduce the likelihood of further harm. Findings suggest that CAMHS professionals may want to help and be willing to implement support, but may be limited by a lack of knowledge and resources. Indeed, one of the only clear positives highlighted by parents was the kindness, compassion and validation provided by some staff. Thus, there is a need for further training among professionals, and an evaluation of that training, to ensure all have a clear understanding of what autism is (and what it is not), how mental health difficulties might present in autistic CYP and reasonable adjustments that could be implemented. This training should be developed with autistic CYP, ensuring their voices are heard. However, in order for professionals to make these adjustments, resources and funding need to be provided for their implementation. This is particularly pertinent given the current NHS Long Term Plan (NHS England, 2019), which outlines the NHS’ plans to improve its understanding of the needs of autistic people, including providing healthcare staff with training on supporting autistic people and ensuring they make reasonable adjustments.
In addition, to be able to meaningfully reduce mental health difficulties in autistic CYP, further research is needed into the appropriateness and effectiveness of therapies. There is a mounting evidence base suggesting that therapies such as CBT and DBT are not effective for autistic individuals (especially when not adapted), with potential explanations including the reliance on cognitive schemas that may be alien or unnatural to autistic people, alexithymia (difficulty recognising or describing emotions) being common in autistic individuals and cognitive processing differences (Spain et al., 2023). However, there is currently little robust evidence regarding the utility of adapted/alternative therapies for autistic populations. This information could be used to inform the development of guidelines for clinicians; the National Autistic Society (2021) recently shared a practical guide which may be a useful starting point. Finally, there is a wider issue within CAMHS generally, whereby thresholds for assessment are too high and waiting lists are too long, resulting in a reactive ‘wait-to-fail’ model (Dvorsky et al., 2014) and CYP reaching crisis point (Grimm et al., 2022). While this is not specific to autistic CYP, it can disproportionately negatively impact this group who are already vulnerable to health inequalities. Thus, there is a need for more funding and service improvements to enable earlier intervention, rather than waiting for difficulties to escalate (Edbrooke-Childs & Deighton, 2020).
Limitations
This study has several limitations that need to be considered. First, parents/carers in this study self-selected and, as such, may not be representative of the entire population. Indeed, the parents who were more engaged with support services and online communities were more likely to have been targeted. It is also possible that those who had a more positive experience may not have felt the need to participate. Second, as the survey was online, some parents/carers may not have had access to the necessary technology; thus, it is possible that the families who are most isolated were not reached. Third, this study only captured the views of parents/carers, and not CYP themselves, meaning that some vital experiences may have been missed. Fourth, data were collected shortly after the COVID-19 pandemic, which may have influenced reported appointment waiting times. However, as participants were asked to share experiences of seeking help at any point in the last 5 years, the role of the pandemic cannot be accurately ascertained.
Conclusion
Findings from this study highlight the ongoing struggles that parents face when seeking help from CAMHS for their autistic child’s mental health difficulties. Many children were not able to access CAMHS due to issues relating to diagnostic overshadowing, a high threshold for assessment, long waiting lists and a lack of professional knowledge about autism. While CAMHS is already facing difficulties meeting demand generally, these issues are amplified for autistic CYP, a group who face disproportionate health inequalities and are more likely to experience mental ill health. Parents expressed a need for a more neuroaffirmative approach in CAMHS, as well as more effective and informed support from schools. Further research, funding and training are urgently needed to ensure mental health support is accessible, timely and effective for autistic CYP.
Supplemental Material
sj-pdf-1-aut-10.1177_13623613251335715 – Supplemental material for ‘Accumulating harm and waiting for crisis’: Parents’ perspectives of accessing Child and Adolescent Mental Health Services for their autistic child experiencing mental health difficulties
Supplemental material, sj-pdf-1-aut-10.1177_13623613251335715 for ‘Accumulating harm and waiting for crisis’: Parents’ perspectives of accessing Child and Adolescent Mental Health Services for their autistic child experiencing mental health difficulties by Emma Ashworth, Lucy Bray, Claire Hanlon, Harvey Stanway, Georgia Pavlopoulou, David Moore, Bethany Donaghy, Elizabeth Coen and Ellen Firth in Autism
Footnotes
Acknowledgements
The authors would like to thank all of the parents/carers who have shared their views, experiences and time with us. They would also like to thank the parent advisors and young people we consulted to help design the study.
Author contributions
Data availability statement
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Ethics approval
Ethical approval was provided by the authors’ institutional Research Ethics Committee (ref: 23/PSY/046). Informed opt-in consent was sought from all participants prior to data collection.
Supplemental material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.