
Abstract
Over the past decades, reports from official authorities and the media have suggested that there is a ‘crisis’ in young people’s mental health. However, there is considerable uncertainty regarding how to interpret the data referred to in these alarming reports. The present article draws on ‘the minority voices’ of young people and theories developed by Ian Hacking to undertake a critical analysis of the conceptualisation of young people’s mental health. According to Hacking, systems of classifications formulate general truths about people and frame the suffering of individuals in specific ways. Classification changes people. However, young people are social actors who interact with classifications of their mental health and by doing so they could cause classifications to be redrawn. Hacking refers to these feedback effects as ‘looping effects’. Based on 51 interviews with 15-year-olds, this article explores how young people interact with psychiatric labels associated with their wellbeing such as anxiety and depression. We demonstrate how the participants gave new meaning to these psychiatric labels, devalued and gave nuance to them, and by doing so transformed them into cultural categories rather than diagnostic categories. We discuss the potential looping effects related to young people’s mental health and how the present findings can inform policy practice.
Introduction
Over the past decades, reports from governmental authorities, organisations and the media have portrayed young people as a homogeneous group who seem to be suffering from mental ill health to a higher extent over time. The reports of a crisis in young people’s mental health correspond poorly with the complexity seen in the research into young people’s wellbeing (Coppock, 2011; Morrow and Mayall, 2009; Wickström and Kvist Lindholm, 2019). Epidemiological survey studies show that young people report problems such as headaches, irritation, problems sleeping and feeling nervous while they continue to report high levels of wellbeing (Petersen et al., 2010). These dual narratives have presented a puzzle to scholars about how to interpret the statistics on young people’s mental health. A large-scale systematic review of the literature on trends in Swedish young people’s mental health 1945–2009 concludes that It is from this review not possible to verify or disprove the general perception of a sharply rising frequency of mental disorders among Swedish children and adolescents. (Petersen et al., 2010: 13)
The conclusion cited above establishes that the general perception of a sharply rising frequency of mental disorders is not verified in the epidemiological research. However, in addition, the conclusion illustrates a leap in reasoning in which various problems reported by young people in the surveys, in the systematic review, are framed and assessed on the basis of being indicative of mental disorders. It signifies how attempts to measure and interpret data about young people’s wellbeing draw on a medical model in which young people’s experiences of various problems are decontextualised and considered signs or symptoms of psychopathology (Graham, 2015; Kvist Lindholm, 2015; Liegghio et al., 2010, 2019; Wickström, 2018). The dual narratives seen in the epidemiological research and the specific way of framing young people’s various problems as symptoms of psychopathology suggest a need to analyse critically the construction of dominant understandings about youth mental health and what it does to young people. In this article, we draw on interviews with 15-year-olds to explore how young people interact with dominant discourses regarding their mental health and what consequences this specific way of framing young people’s mental health bring for young people.
Psychiatric labelling and framing of young people’s reported problems
The specific way of framing young people’s various problems as symptoms of psychopathology is underpinned by the processes of psychiatric labelling of various problems experienced by young people.
Figure 1 illustrates how problems reported by young people in self-reporting surveys – that is, headache, stomach ache, back pain, irritation, feeling low, feeling dizzy, feeling nervous – are indexed and categorised in the summarising reports, and the systematic reviews of the literature report problems as symptoms of mental ill health, foremost symptoms of internal mental health problems and depressive symptoms (e.g. Merry et al., 2012; Petersen et al., 2010; Swedish Council on Health Technology Assessment (SBU), 2010). These labels are applied in the literature to describe young people’s wellbeing. However, the labels are also performative in the sense that they construct a framework of how to understand and respond to young people’s wellbeing in contemporary societies (Kvist Lindholm, 2015; Wickström & Zetterqvist Nelson, 2018; Wright, 2015; cf. Hacking, 2004). When various problems reported by young people are piled together and labelled as symptoms of depression and mental ill health, the problems are interpreted as indicative of pathology. Furthermore, within the field of public health, the psychiatric labels operate as diagnostic categories of illness and of illness risk. Based on the statistics, young people are defined as a group at risk and become a target group for psychoeducational programmes focusing on mental disorders such as anxiety and depression (e.g. Merry et al., 2012; SBU, 2010). The wide scale implementation of psychoeducational programmes in schools is presented as a form of ‘psychological immunisation’ against mental ill health in the population (Kvist Lindholm, 2015; Wright, 2015). However, it highlights the paradox that young people have to take part in interventions focusing on psychiatric diagnoses such as depression and anxiety, regardless of whether or not they have depression or anxiety (Kvist Lindholm and Zetterqvist Nelson 2015; Merry et al., 2012; Wickström 2013; cf. SBU, 2010). In this sense, young people’s lives undergo ‘psychiatrisation’, that is, a process by which areas of everyday human life come to be observed, understood and experienced through the language, theories, technologies, institutions and practices of ‘western’ biomedical psychiatry (Coppock, 2014; Liegghio et al., 2019).
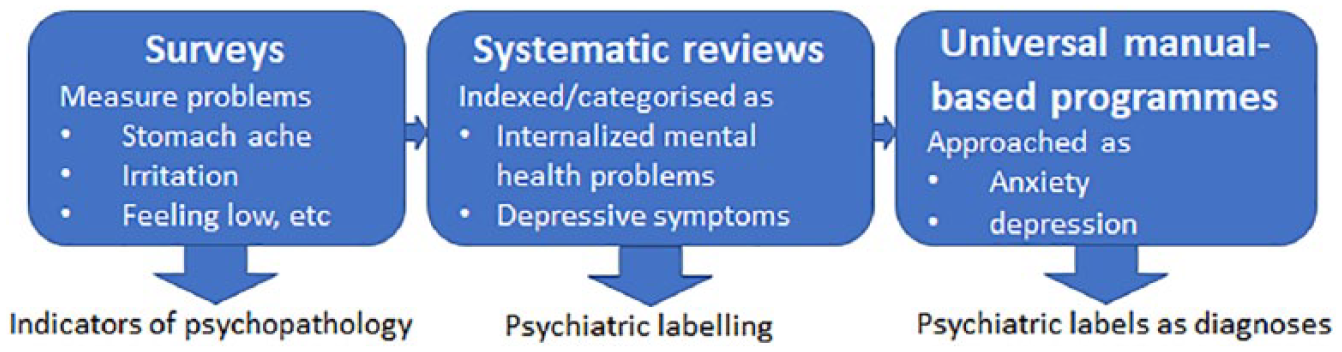
A system of classifying young people’s mental health.
The psychoeducational programmes being implemented in schools to deal with the apparent crisis in young people’s mental health are based on a psycho-centric problem definition in which the aetiology of mental health problems is positioned merely within the individual (Graham, 2015; Kvist Lindholm, 2015; Liegghio et al., 2010; Teghtsoonian, 2009; Wickström, 2018), that is, the programmes are based on ‘the perception that both the problem and solution lie inside the child’s head, despite considerable evidence of the contrary’ (Graham, 2015: 28). An example is the Depression in Swedish adolescence (DISA) programme being practised in schools in Sweden. The programme is based on the idea that an individual with depression has acquired a dysfunctional way of interpreting the world and the intervention is focused on helping young people restructure their depressive, negative/irrational thoughts into more positive and rational thoughts (DISA manual; Clarke et al. (1995 [2010]) (Rev edn): 3; cf. Beck et al., 1979). It signifies how contemporary discourses on young people’s mental health draw on a hollow individualism which has moved ‘the battleground inside our children’s heads’ – to mould the inner world of children – irrespective of external life conditions such as social class, family and school situation (Graham, 2015: 11, cf. Rose, 1999).
‘Making up people’ through the process of classification
The specific ways of conceptualising young people’s health reports and responding to the needs of young people outlined above could be understood as a system of classification. According to Ian Hacking, systems of classifications formulate general truths about people and bring specific ways of framing the suffering of the individual. He asked questions such as ‘Does the availability of a classification, a label, a word or phrase, open certain possibilities, or perhaps close off others?’ (Hacking, 2004: 285). Hacking pointed out that classifications may affect how people come to experience themselves. A classification of people ‘make up people’, he argued, since the classification may create new ways to be a person (Hacking, 1995). Hacking (1998) suggested that ‘scientific knowledge about ourselves – the mere belief system – changes how we think about ourselves, the possibilities that are open to us, the kinds of people that we take ourselves and our fellows to be’ (p. 10). However, when people interact with classifications, they may cause systems of classification to be modified in turn. Hacking referred to these feedback effects as ‘looping effects’. He suggested, ‘Classifying changes people, but the changed people cause classifications themselves to be redrawn’ (Hacking, 2004: 279). He argued that looping effects shape the evolution of what kinds of people can exist, as well as the evolution of scientific classifications. A relevant question to elaborate on is thus whether, and if so how, young people make use of the psychiatric labels in conversations about their wellbeing (cf. Zetterqvist Nelson, 2012).
The present article draws on interviews with 15-year-olds and theories of ‘making up people’ and ‘the looping effects of human kinds’ (Hacking, 1998, 2004) to open up a critical analysis of dominant understandings about youth mental health and contemporary discourse. Young people’s perspectives of their wellbeing represent a ‘minority knowledge’ that can help to widen majority discourses on young people’s mental health (Watson et al., 2012). An interest in young people’s perspectives about their wellbeing involves shifting focus to how they, as social actors, interact with dominant discourses regarding their mental health and take part in constructing their wellbeing. The aim of the present article is to explore how young people interact with psychiatric labels when talking about their wellbeing. We analyse how young people appropriate, reject and give new meaning to the psychiatric labels anxiety and depression and whether they develop ‘loping effects’ of these classifications.
The research framework
The empirical data informing this article are drawn from an ethnographic study of how young people make sense of psychological (ill) health.
The study focuses on 15-year-olds because large-scale epidemiological studies have reported a decrease in psychological wellbeing in this age group (e.g. Petersen et al., 2010). To form a broad sample of young people, the study was conducted in two schools with different socioeconomic catchment areas in Sweden. One of the schools is situated in a city centre, while the other is situated in a rural area. Initially, we established contact with the school principals who granted access and enabled us to contact the schoolteachers of three classes of ninth grade pupils. The teachers set aside time during school hours for us to inform students about the study, hand out information letters and consent forms, and inform them of the opportunity to withdraw from the study at any time. In total, 32 females and 9 males gave consent to participate in the study. The uneven distribution of males and females signifies the tendency seen in previous research for females to be more inclined to talk about their wellbeing and experienced problems than males.
The empirical data consist of 41 individual interviews and 10 group interviews with the 15-year olds. The study combines individual interviews with group interviews to provide participants with the opportunity to express more sensitive issues in the individual interviews and to discuss the questions together with their peers in the group interviews. The interviews were semi-structured and lasted 45–90 minutes. The interviews focused on what makes them feel well and what their health problems measured with the international survey Health Behaviour in School-aged Children (HBSC) represent in their daily lives. We also asked them what meaning they would give to concepts commonly applied in summarising reports on young people’s wellbeing. Various follow-up questions were posed to adapt the conversations to themes that the students stressed and talked about. The interviews were transcribed verbatim in Swedish and the excerpts were translated into English.
The analysis focused on how the young people made use of psychiatric concepts when talking about their wellbeing. First, we focused on content and meaning by asking questions such as ‘What do participants’ responses or texts tell us?’. All transcripts were searched through with a focus on the different ways the 15-year-olds made use of psychiatric concepts. We found that they commonly made use of the concept anxiety and sometimes depression. We identified the various situations when they themselves introduced these concepts and noted the situations in which we used the concepts in a question. We coded for recurrent themes of the meaning that participants gave to the concepts of anxiety and depression. We then shifted focus to analyse these concepts as discourse. Discourse refers to institutionalised patterns of knowledge that govern the formation of subjectivity. A focus on discourse involved asking questions such as ‘What is this discourse doing?’. Discourse analysis takes as its starting point that language is performative. When we describe an object for instance, we do not passively describe reality but bring the objects we describe into being (Willig, 2003). In this study, we focus on how young people use discursive resources and what it accomplishes (i.e. discursive psychology) (Willig, 2003). We analysed in what situations the young people made use of psychiatric labels, what meaning they gave to these psychiatric concepts, how they used them in different ways and what the use of labels accomplished. In this way, our aim was to explore how young people appropriated, rejected and gave new meaning to psychiatric labels and whether they accomplished what Hacking (2004) refers to as looping effects.
How young people appropriate and give new meaning to psychiatric concepts
The 15-year-olds being interviewed in the present study gave wellbeing the meaning of having friends and family they could rely on. They commonly made use of the psychiatric concept anxiety and sometimes depression when talking about their wellbeing. Mental health diagnoses such as anxiety and depression have been seen to carry a significant stigma, that is, a form of negative labelling, and there is a risk of being perceived or treated unfairly due to being judged as different from what is considered ideal or normal (Graham, 2015; Liegghio et al., 2010; Wright, 2015; cf. Goffmann, 1963). However, the young people commonly made use of the psychiatric concepts anxiety and depression in an unrestrained way, both in the individual interviews and in the group interviews. Their use of these psychiatric concepts could be seen to signify a normalising process of mental ill health, commonly understood as normalising the existence and acceptance of mental illness. In young people’s descriptions and accounts, anxiety was given various meanings such as having too much to do, being uncertain or aware that one might not succeed, or having to do things they did not really feel like doing. Depression was more commonly related to mental illness; however, both anxiety and depression were often used synonymously with feeling low. The young people made use of the psychiatric labels when talking about schoolwork, their futures and ideals of succeeding, as well as when they talked about conflicts and norms for acceptance in their peer groups. When they made use of the these psychiatric labels, they gave nuance to their meanings and rather than applying them as binary labels (feeling well, feeling ill) they applied them on a scale and introduced terms such as ‘anxiety anxiety’ to signify a higher level of suffering, whereas a singular anxiety could just apply to minor setbacks or things that annoy them. In the following, we will give examples of how they make use of the psychiatric labels anxiety and depression when talking about their school and conflicts in their peer groups. We will demonstrate how they gave nuance to, devalued and gave new meaning to these psychiatric labels, and by doing so transformed them into cultural categories rather than diagnostic categories.
Anxiety as connected to school and ideals of succeeding
The 15-year-olds made use of the psychiatric label anxiety when answering general questions about their wellbeing and what they would say affects how they are feeling. In the following, we see an example of this when Ella talks about her general wellbeing:
I have a very good life in some ways since my family is always there, I have a lot of friends and so on. But then I also have a less good life in the sense that I have a lot of performance pressure and anxiety connected to school.
The excerpt shows a recurrent pattern found in the interviews of young people often describing that they have a good level of wellbeing which they explained as the result of their social network of friends and family. At the same time, they gave examples of experiencing specific problems connected to school and related it to anxiety. As illustrated in the quote above, young people commonly associated anxiety with a pressure to perform well in school. When talking about anxiety, they sometimes referred to a wish to succeed and the ideal that they should be successful individuals who take responsibility for forming a prospering future for themselves:
You mention anxiety. What does anxiety mean, according to you?
Sort of, will I fail this test? Will I succeed? In the ninth grade, what school should I pick? What will my future look like if I choose this?
In Anna’s account, anxiety is given the meaning of failing tests, trying to succeed and making the right choices for her future. The 15-year-olds thus gave anxiety the meaning of a pressure to succeed in school, but also related it to their future, a future they constructed as being dependent solely on themselves. Their accounts demonstrate a sense of far-reaching individual responsibility for succeeding and creating a good life on their own. The pressure they describe reproduces individualistic ideals and discourses characterising our contemporary western society to create a life of one’s own and discourses of ‘responsibilisation’ that direct individuals to become ‘enterprising selves’ who govern themselves in accordance with a ‘hollow individualism’ (Rose, 1999). The above quote could therefore be understood to illustrate how young people acknowledge prevailing values and norms about how to become a successful individual – passing tests in school and making the right choices for their future – and how they work on or invest in themselves in accordance. For some students the pressure to succeed, however, was put forward as an impossible task:
You are behind and sort of panic since there is too much to do. You don’t know how, there is too little time and so much to do and you have anxiety since you know you won’t make it.
This quote shows how anxiety is used as an expression for having problems in school and not managing the task of succeeding. However, Linnea’s account shifts focus to external circumstances, that is, the conditions that are formed for her to succeed. In Linnea’s description, anxiety is given the meaning of an unbearable school situation: ‘too much to do’ and ‘too little time’ and knowing ‘you won’t make it’. For students like Linnea, who have failed tests and do not always manage to meet standards, the pressure to succeed in school is thus constructed as an unbearable school situation.
The quotes above have illustrated various ways that the young people made use of the psychiatric concept anxiety when talking about their general wellbeing. In their accounts, anxiety represents a pressure to perform well, to succeed in school and to form a future for themselves. In this sense, young people reproduce ideals of forming ‘enterprising selves’, that is, a hollow individualism, but at the same time they relocate the focus to external factors such as the amount of work to do and the time and the possibilities given to succeed.
Anxiety as conflict and norms for acceptance
The young people in our study also made use of the psychiatric concept anxiety when they answered specific questions about their interpretation of health problems measured to indicate psychosomatic symptoms and mental health (headache, stomach ache, back pain, irritation, feeling low, feeling dizzy, feeling nervous):
to
Perhaps that you have got a little anxiety facing school or due to having argued with family or friends.
In the above quote, anxiety is used as an expression equivalent to feeling low and anxiety is associated with school and conflicts with family or friends. Since family and friends were referred to as the most important factors for feeling well, conflicting with family members and friends was constructed as having a negative impact on their wellbeing. Hannes’ account also illustrates a common way that young people applied the concept of anxiety, by adding an amplifying or diminishing word in front, such as ‘a little’ anxiety. The diminishing word accomplishes a decrease of gravity of what anxiety implies. Hence, in Hannes’ account, there is a scale of anxiety and he positions himself on the lower score of the scale. Another example of how the concept of anxiety was used by the young people when talking about the health problems measured in HBSC is shown in the next excerpt:
Why do you have a hard time falling asleep?
Stress and such stuff, sort of anxiety and so on.
You mention stress and anxiety. What causes it would you say?
I get stressed from school. That it becomes too much and . . . perhaps we have problems at home or perhaps I got into an argument with someone.
The way Kalle makes use of the concept anxiety shows another example of how anxiety was commonly expressed together with a word in front which changes the meaning of anxiety. In Kalle’s account, ‘sort of’ is used as a pre-word to anxiety. It implies anxiety is not a fixed category but something more fluent that can be diversified. In Kalle’s description of anxiety, the concept is given the meaning ‘stress and stuff’. In his elaborated explanation, the concept is related to ‘stress from school’ and how it becomes ‘too much’ when also facing ‘problems at home’ or getting ‘into an argument with someone’. Most students applied the concept anxiety when talking about a pressure that piles up at times when there are many exams at school or conflicts with peers and family members. In this sense, anxiety is used as an expression for temporary problems that come and go depending on their school situation and conflicts within their social relations. However, a few students made use of the concept anxiety as an expression for more severe social problems:
According to the social welfare office, my dad still has the rights to see me, so I must meet with him . . . I mean I get so much anxiety due to this.
Here, anxiety is used as an expression for deeper ongoing family problems regulated by the social welfare office. Similar to other interviewees, Amanda uses an amplifying word in front of anxiety that suggests there is a scale of anxiety. However, she positions herself towards the upper end of the scale. In Amanda’s account, getting ‘so much anxiety’ is the result of a situation in which she is forced to meet with her father although not wanting to. In her account, the problem represents external factors. What is at stake in her account is the loss of control and of not having a say in the situation. The young people applied anxiety to several deep ongoing relational problems. 1 A common denominator in their accounts is how they referred to having to deal with problematic situations that were out of their control but had a severely negative impact on their wellbeing.
In the young people’s descriptions of how conflicts with family and peers were related to them experiencing feeling low, problems sleeping, headaches and so on, they related these issues to how they constantly had to manage norms for acceptance within the peer group and argued it gave rise to anxiety:
Stress and anxiety are words that we often use. ‘I’m so stressed’ and ‘I have so much anxiety over this’ we commonly say.
/. . . /
You mentioned anxiety, what is it that causes anxiety would you say?
Lots of things, but sort of you’re afraid what people might think.
There are so many ideals that you should . . . you sort of must be a certain way.
You must be a certain way to be accepted (kind, good looking, funny, not too keen). Otherwise you will be excluded.
This excerpt from the group interviews illustrates how young people apply the concept of anxiety as an expression for the constant pressure they feel to acknowledge and adjust to prevailing ideals and norms to be accepted within their peer groups. In Hanna’s and Stina’s accounts, anxiety represents situations in which they have to adjust to ideals that they ‘must be a certain way’, ‘kind, good looking, funny, not too keen’ or otherwise risk being ‘excluded’.
To sum up, all the excerpts above have highlighted how the young people made use of the psychiatric label anxiety when talking about their wellbeing. Within their descriptions and accounts, anxiety was applied as a concept representing everyday life experiences of conflicts, including when feeling judged due to norms for acceptance and when going through tough periods of exams and making important choices for their future, as well as handling more severe problems which some of the young people were facing at school and in their social lives but had no control over.
When using the psychiatric label of anxiety, the young people take part in what could be understood as a normalising process of mental ill health and psychiatric discourses in lay people’s talk (Coppock, 2011). However, they do not use these psychiatric labels as diagnostic categories, nor do they reproduce the psycho-centric problem definition which permeates psychoeducational programmes for anxiety and depression being implemented on a wide scale in schools in Sweden, as in many other countries. Several sociological scholars (i.e. Graham, 2015; Liegghio et al., 2010) have critiqued the psycho-centric problem definition as it is applied in contemporary discourses of young people’s mental health – that is, locating the aetiology of mental health problems within the individual and moving the battlefield within young people’s heads – since it ignores the social and structural determinants of health. Against this background, an interesting aspect of the analysis was how the 15-year-olds applied the psychiatric label anxiety to make use of the label as a cultural category and by doing so accomplished looping effects in lay people’s talk. However, the programmes practised as universal interventions in school are based on clinical definitions of mental disorders (Kvist Lindholm, 2015; Kvist Lindholm and Zetterqvist Nelson 2015; Wickström 2013). The clinical definition of anxiety suggests that anxiety involves an excessive worrying, that is, adopting a psycho-centric problem definition which moves the battleground inside young people’s heads (Graham, 2015; Liegghio et al., 2010). In the young people’s descriptions and accounts of anxiety, however, anxiety was not constructed as irrational or inevitably excessive worrying, but as a reaction to a pressure to perform in school and to manage routines within their peer groups and family lives. Hereby, the 15-year-olds relocate the focus of anxiety to external factors such as their school situation, their social relations with peers and family, and ideals and norms of contemporary society and local peer groups. In this way, they de-pathologise the state of anxiety. Hence, the young people take part in a normalising process of using psychiatric concepts in everyday talk, but also accomplish a ‘looping effect’ in lay people’s talk in which the meaning of anxiety is re-focused to social and structural dimensions of the context in which their experienced problems arise. In the next section, we will discuss looping effects accomplished when young people start devaluating and redrawing the psychiatric diagnoses anxiety and depression.
Devaluating and nuancing the psychiatric diagnoses anxiety and depression
When we noted that the young people made use of a psychiatric label, we asked them to give a further description of what they meant by the concepts. In some cases, they described applying such labels to trivial issues:
Me and my friends we use it just for example, ‘[When] I can’t find the shoehorn I get anxiety’.
This quote highlights how the seriousness of the psychiatric label anxiety is devaluated. The same phenomenon was seen when the young people talked about the psychiatric concept depression:
Being depressed is not such a heavy word anymore because it is used so much.
yes, I think ‘to be a little depressed’ is the same thing as being a bit low.
yes today, that’s what it means.
When Philip develops Oscar’s account that depression is not a heavy word anymore, he makes use of the qualifiers ‘a little’ and ‘a bit’, suggesting being a little depressed is the same thing as being a bit low. Their way of applying words in front of the psychiatric label confirms the looping effect in lay people’s talk seen in previous excerpts. When the interviewees applied the psychiatric labels this way they accomplished a looping effect which involves constructing the concepts not as binary diagnostic categories but as dynamic categories, and they accomplish a devaluation of the gravity of the psychiatric label. Anxiety and depression hereby stop being categories for suffering and instead become concepts one could apply to express oneself about trivial issues and strains in one’s life.
When we asked follow-up questions about these devaluations of the psychiatric labels, they started reflecting of the risks associated with the normalising process of psychiatric concepts:
I don’t think it’s good. That we almost normalise these things because then it feels like depression and anxiety become something people just blurt out and just use, when in fact it is something really serious.
This quote shows how Emma described a normalising process of the psychiatric labels, but not in a positive way such as normalising the existence and acceptance of mental illness, but rather as something hiding the seriousness of these issues. The young people sometimes compared the issues they would label as anxiety and depression with the clinical diagnosis of a disorder. An example is seen below when Klara compares her issues to someone suffering from what she categorises as ‘real’ anxiety:
Even if I’m irritated or feel low, I can’t say that I’ve got anxiety because there are still people with real anxiety /. . . / I have anxiety but I don’t have real anxiety sort of.
In Klara’s account, there is a difference between having anxiety and having real anxiety. The students commonly made such a distinction between ‘anxiety’ and ‘real anxiety’ or differently expressed between ‘being a little depressed’ and having ‘a real depression’. Hereby they coin new ways of applying the psychiatric labels in which the gravity of the problem it applies to is lessened, making these useful concepts to apply to everyday experiences rather than clinical diagnoses of a mental illness. Their accounts illustrate an awareness that they perhaps use the concepts in a new way – applying them not as diagnostic categories but as categories applicable to less severe issues not necessarily involving suffering or ill health. Their way of giving nuance to the meaning of psychiatric labels and applying them as fluent categories, rather than binary diagnostic categories, accomplishes a looping effect that devaluates the seriousness of the psychiatric label. Furthermore, they show that anxiety and depression are dynamic cultural categories in lay people’s talk that can mean different things depending on how the concepts are applied and depending on what problems they are used as an expression of. To sum up, the psychiatric labels are used as dynamic categories that could apply to a wide range of problems ranging from unbearable school and family situations to trivial issues and strains in one’s life.
Discussion
Previous research has shown that dominant discourses of young people’s mental health transform young people’s experienced problems into symptoms of psychopathology and suggest a ‘crisis’ when in fact, the majority of young people report good mental health (Coppock, 2011; cf. Petersen et al., 2010). Through the processes of indexing and categorising young people’s health reports, the wide range of problems reported by young people are narrowed down to psychiatric labels. Furthermore, the large-scale implementation of programmes focusing on psychiatric diagnoses such as depression and anxiety risk adding to individualising and pathologising effects of psychiatric labels. Graham argues that the programmes ‘reinforce the perception that both the problem and solution lie inside the child’s head, despite considerable evidence of the contrary’ (Graham, 2015: 28). Hence, diagnostic labels pose a significant risk for neglecting broader social and structural determinants of health. An important finding in the present study is that young people themselves appropriate psychiatric labels such as anxiety and depression when talking about their wellbeing and as such could be seen to take part in reproducing dominant discourses of a crisis in young people’s mental health. However, as highlighted above, when analysing how they apply these psychiatric labels, they accomplish looping effects in lay people’s talk that could be seen to cause systems of classification of anxiety and depression to be modified in turn (Hacking, 2004). Hence, when lay people use psychiatric labels in a new way, and change their meaning, the precondition changes. While the young people in the present study reproduced a psychiatric discourse as well as a ‘hollow individualism’ in some sense, they do position these issues in a wider social and structural context, that is, they point to the importance of social and structural determinants of health in understanding and responding to young people’s mental health. Furthermore, they accomplish looping effects that give nuance to the meaning and the gravity of psychiatric labels, detaching these classification categories from their clinical origin. Rather than reproducing a sense that the battleground is inside young people’s heads (Graham, 2015), they locate the battleground in their social and structural context of managing school, their social relations, and norms and ideals of society and their peer groups.
The way that young people change the meaning of the psychiatric labels involves appropriating the psychiatric label, without adopting the psychocentric-problem definition involved in the clinical definitions of anxiety and depression. Hereby, they accomplish a looping effect since they change ‘what kinds of people can exist’ under the labels of anxiety and depression. However, while they use the labels in a new way, they do not accomplish a looping effect in the clinical diagnoses of anxiety and depression applied in the programmes offered to young people in school. The present study sheds light on the importance of acknowledging this discrepancy. The young people make use of psychiatric concepts which originally were applied to signify mental illness. If young people’s transformations and devaluations of these psychiatric categorisations are not understood by the adult world, the looping effect is not brought to light. There is thus an overarching risk that when young people appropriate psychiatric labels as a means to express themselves about various types of problems, these psychiatric labels are interpreted by the adult world as diagnostic labels signifying a rise in mental ill health. Policy and practice might jump to conclusions that young people are in need of interventions to deal with the clinical diagnoses of anxiety and depression, thereby focusing programmes on diminishing excessive and irrational worrying, rather than acknowledging the complexity of social and structural determinants of health.
The ways that young people make use of these psychiatric labels as categories for everyday issues and strains in their lives could be argued to resonate with how the diagnostic and statistical manual (The Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-V)) for mental illness has been argued to expand these psychiatric diagnostic categories and by doing so reconfigure what is considered normal (Conrad, 2007). However, an important difference to be noted here is that while the DSM expands anxiety and depression as psychiatric definitions of illness, the young people detach these labels from pathology and apply them as cultural categories. In this sense, psychiatric labels stop being categories for suffering and start being cultural categories applicable to dealing with the ups and downs of life.
The results highlight an issue commonly overlooked in the quantitative research studying prevalence and time trends of mental ill health among young people. Epidemiological research is careful to standardise instruments and questions applied to measure wellbeing and to maintain professional classifications in order to accomplish valid interpretations. However, they tend to overlook the fact that societies do not stay the same. Societies change, and lay people’s discourses change with them. When measuring trends of wellbeing, we would argue that, to acknowledge discursive changes, ‘looping effects’ become essential.
Footnotes
Ethical approval
The research procedures have been approved by the Regional Ethical Review Board in Linköping, Sweden (Reg. No. 2017/171-31).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors received financial support for the research from the Swedish Research Council for Health, Working Life and Welfare (Reg. No. 2016-00129) and the Swedish Research Council (Reg. No. 2016-00784).