
Abstract
Lesson
A systemic inflammatory response causing multi-organ failure and requiring multiple amputations was refractory to all treatments except Anakinra, and the cause remains unclear.
Case report
Investigation results.

Discussion
This patient presented with SIRS and progressive necrotizing vasculitis of unknown cause. Fifty percent of vasculitis cases are idiopathic, but 15–20% are secondary to infection, 15–20% associated with inflammatory disease, 10% due to a drug reaction and 5% associated with malignancy. 1 Infectious causes were deemed unlikely as extensive cultures showed no growth. A drug reaction was considered as she was exposed to multiple drugs including Clarithromycin, Teicoplanin, Ciprofloxacin, Clindamycin, Rifampicin and Paracetamol which have all been reported to cause vasculitis. 2 Heparin is also known to cause skin necrosis and both subcutaneous and IV routes have been implicated with varying severity; however, the ischaemia is thought to be caused by platelet aggregation and thrombosis rather than a vasculitis.3,4
Yamaguchi criteria for diagnosis of adult Still’s disease. 6
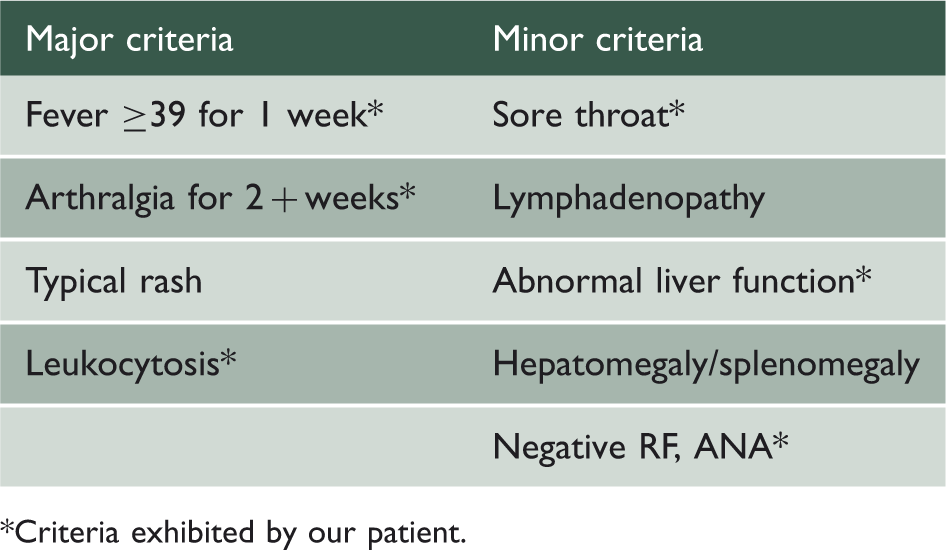
Criteria exhibited by our patient.
Only one case report links this condition with vasculitis; a 43-year-old male with adult Still’s disease was found to have leukocytoclastic vasculitis on skin biopsy. His condition improved with corticosteroids. 7 Similarly, only one report describes amputation associated with adult Still’s disease; a 23-year-old woman developed disseminated intravascular coagulation (DIC) leading to autoamputation of the distal phalanges of two fingers. She also responded to corticosteroids. 8
Takayasu’s arteritis usually affects women of Asian origin aged 20–40. There is
granulomatous inflammation of the aorta and major branches leading to stenosis, thrombosis
and aneurysms and it can be associated with fever, arthralgia and malaise.
9
Diagnosis criteria from the
American College of Rheumatology requires three of the following six criteria to be met:
Age ≤40. Claudication of extremities. Decreased pulsation in one/both brachial arteries. 10 mmHg difference in systolic blood pressure between arms. Bruits over subclavian artery or abdominal aorta. Angiographic narrowing of aorta, primary branches or large arteries in upper
or lower extremities.
10
Our patient met criteria one, two, three and six. Many reports describe skin lesions in association with Takayasu’s arteritis, especially pyoderma gangrenosum, livedo reticularis and erythema nodosum. One report describes a previously fit woman with leg claudication which progressed to gangrene requiring amputation. She was diagnosed with Takayasu’s arteritis following angiogram. 9
Conclusion
Our patient developed a rapidly deteriorating inflammatory and necrotic condition, which failed to respond to all treatments until the initiation of Anakinra prompted a swift response. Her symptoms were consistent with many disease states making treatment complex, and although a drug reaction and systemic inflammatory diseases have been considered these remain diagnoses of exclusion. Without any conclusive diagnostic test, the cause of her catastrophic condition remains unclear leaving both the patient and her physicians uncertain as to why Anakinra worked and whether she is now cured or if she is at risk of recurrence of her symptoms.