
Abstract
Background:
Prescribing errors are a significant cause of preventable harm in healthcare, particularly in low- and middle-income countries where system-level safeguards are often lacking. However, data on their prevalence and predictors in Ghana’s primary healthcare facilities remain limited.
Objectives:
To determine the prevalence, types and predictors of prescribing errors in a primary-level health facility in a peri-urban municipality in Ghana.
Design:
Retrospective analytical cross-sectional study.
Methods:
We analysed data from the hospital’s pre-existing prescribing error incident reporting database, which contains errors identified by pharmacists and documented during routine care between June 2021 and June 2024. Prescribing errors were classified using a structured tool based on the National Coordinating Council for Medication Error Reporting and Prevention (NCC MERP) guidelines. Logistic regression analysis was conducted to identify predictors of prescribing errors, with statistical significance set at p < 0.05.
Results:
The prevalence of prescribing errors was 1.92% (95% CI: 1.71–2.13). The most common errors were frequency (27.8%), commission (26.2%) and dose errors (25.2%). Dose errors were more frequent among nurse prescribers (odds ratio (OR) = 3.02; p = 0.022) and less common in patients aged 41–65 years (OR = 0.24; p < 0.001). Commission errors were higher among doctors (OR = 2.79; p = 0.001), while frequency errors were less likely with doctors (OR = 0.28; p = 0.006). Incorrect drug selection occurred more often among nurse prescribers (OR = 6.35; p = 0.012) and non-insured patients (OR = 6.05; p = 0.006).
Conclusion:
Although prescribing errors were relatively infrequent, they were significantly influenced by prescriber type, patient age and health insurance status. These findings highlight the importance of continuous prescriber training, enhanced pharmacist participation in the medication-use process and the establishment of robust prescription monitoring systems to strengthen medication safety and optimize patient outcomes.
Plain language summary
This study looked at how often mistakes occur when healthcare providers write prescriptions and what factors contribute to these errors in a primary healthcare facility in Ghana. Prescribing errors can cause avoidable harm to patients, but information about them in Ghana’s healthcare system is limited. Researchers reviewed three years of prescription data (from June 2021 to June 2024) collected through the hospital’s error reporting system. These records included only errors that were identified and documented by pharmacists during routine work. Each error was grouped into types such as wrong dose, wrong drug, or wrong frequency, and statistical analysis was used to find out what factors made errors more likely. Out of all prescriptions reviewed, about 1.9% contained an error. The most common mistakes involved giving the wrong dose, the wrong drug, or the wrong frequency of use. Nurse prescribers were more likely to make dose and drug selection errors, while medical doctors were more likely to make commission errors (e.g., prescribing a medicine that was not needed). Patients without health insurance and those outside the middle-age group were also more likely to be affected by errors. Overall, prescribing errors were not very common, but they still pose safety risks that can be prevented. The study recommends regular training for prescribers, stronger involvement of pharmacists in checking prescriptions, and better systems to monitor and prevent medication errors in Ghana’s primary healthcare facilities.
Keywords
Introduction
Prescribing medications is a core function of healthcare delivery, essential for disease management, symptom control and the achievement of positive health outcomes. When executed accurately and rationally, prescribing minimizes adverse drug events, optimizes treatment effectiveness and enhances the overall quality and safety of care. 1 Prescribing errors (PEs) are defined by Ferner and Aronson 2 as failures in the prescribing process that lead to or have the potential to lead to patient harm. Their burden is particularly pronounced in low- and middle-income countries (LMICs), where systemic resource constraints often exacerbate their impact.3–5
Globally, PEs account for a substantial proportion of all medication-related errors, with reported prevalence rates ranging from 25% to 50%, depending on the clinical setting and study methodology.4,6–8 These errors include incorrect drug selection, inappropriate dosing, omission of critical information or duplication of therapy, and have been linked to adverse drug reactions, treatment delays, increased hospital readmissions, avoidable healthcare costs and death.4,6,9–11 In high-income countries, studies have consistently reported high rates of omission errors and instruction-related mistakes in both outpatient and inpatient settings.12–14
The causes of prescribing errors are multifactorial, involving factors such as inadequate prescriber training, poor access to up-to-date treatment guidelines, workload pressures, reliance on handwritten prescriptions and limited interprofessional collaborations.3,4,15,16 The World Health Organization (WHO) estimates that medication-related harm accounts for nearly 50% of preventable harm in healthcare, with an annual global economic cost exceeding $42 billion. 17 In LMICs, additional contributors include the absence of clinical pharmacists, high patient-to-provider ratios and limited technological infrastructure, like electronic prescribing with decision-support tools. Despite these risks, underreporting remains widespread due to blame-oriented cultures, fear of punitive action and weak institutional systems for monitoring and learning from errors.8,16–18
In Ghana, existing studies on prescribing errors have primarily concentrated on secondary/tertiary hospitals, medication administration or broader aspects of medication safety.9,19–21 There is a notable dearth of research examining these issues in primary-level health facilities, where most patients seek initial care. This gap is particularly concerning given the diverse cadre of prescribers – physicians, physician assistants and nurses – who operate at this level, often with varying degrees of training, clinical experience and familiarity with prescribing guidelines.8,22 As a result, prescribing practices may be inconsistent and susceptible to error, particularly in high-volume, resource-constrained environments.
To address this critical gap, the aim of the present study was to determine the prevalence, types and predictors of prescribing errors in a primary-level health facility in a peri-urban municipality in Ghana. By identifying key predictors, this study aims to inform targeted interventions to improve prescribing practices. The findings are expected to guide context-specific strategies, ultimately contributing to enhanced medication safety and improved patient outcomes in Ghana and similar resource-limited settings.
Methods
This study adhered to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines (Supplemental Table 1). 23
Study design
This study employed a retrospective observational design using data from a pre-existing prescribing error reporting system. The analysis focused on pharmacist-verified prescribing errors documented between June 2021 and June 2024. Only errors formally reviewed and recorded by pharmacists were included to ensure data validity and to reflect discrepancies identified by qualified medication therapy experts.
Study setting
The study was conducted at a 165-bed primary-level Bekwai Municipal Hospital located in a peri-urban municipality approximately 40 km from Kumasi, Ghana. The hospital was selected for its high outpatient attendance, diverse prescriber workforce (including medical doctors, physician assistants, midwives and nurses), and the presence of an established electronic health record (EHR) system integrated with e-prescribing functionality.
Within this system, prescribers generate prescriptions electronically using international non-proprietary names, selecting drug, dose, frequency and duration from standardized dropdown menus. Each prescription undergoes verification by a pharmacist or pharmacy technician before dispensing. When a prescribing error is detected, the pharmacist intervenes by consulting the prescriber for correction, and the incident is documented in both the EHR and a manual intervention register.
The hospital serves approximately 80,000 outpatient visits annually and maintains an average inpatient bed occupancy rate of 60%. Its outpatient services include general consultations and specialized clinics such as dental, eye, ENT and chronic disease management (diabetes and hypertension).
In Ghana’s healthcare system, primary care refers to the first point of contact within the public tiered structure, typically delivered through health centres, polyclinics and district hospitals. These facilities manage common health problems such as malaria, respiratory infections, hypertension, antenatal care and childhood immunizations. While health centres and polyclinics are primarily staffed by non-physician clinicians (physician assistants and nurses), district hospitals, such as the study site, occupy a unique position – serving as both primary care providers for their communities and referral centres for lower-level facilities. 24 They operate under a mixed prescriber model involving doctors, physician assistants and nurses. Hence, although classified as primary care settings, district hospitals possess a more complex organizational structure than typical family practice clinics.
Data source and sampling
A complete enumeration approach was adopted, capturing all prescriptions reviewed and verified by a pharmacist during the study period (June 2021–June 2024) if they met the inclusion criteria. As such, no formal sample size calculation or power analysis was conducted. Data were extracted from the hospital’s prescribing error database, which systematically records all pharmacist-identified and documented prescribing errors as part of routine clinical practice.
Each record in the database included relevant details such as prescriber category, patient demographics, therapeutic class of the medicine and the specific type of error identified. Data from both the EHR system and the manual prescription intervention register were cross-checked to ensure completeness and accuracy before analysis.
Inclusion and exclusion criteria
The study applied specific inclusion and exclusion criteria to ensure data accuracy and clinical relevance.
Inclusion criteria
All prescriptions that were reviewed and verified by a pharmacist between June 2021 and June 2024 were included in the analysis. In Ghana, prescriptions are generally issued by clinicians without pharmacist pre-approval, and due to the national shortage of pharmacists, many are dispensed directly by pharmacy technicians. Including only pharmacist-verified prescriptions ensured that all documented errors had undergone the highest available level of professional review, enhancing data validity and reliability.
In addition, only prescriptions containing at least one pharmacist-confirmed prescribing error were included. This criterion focused the analysis on verified errors that had been intercepted at the dispensing stage, representing a conservative estimate of errors most likely to reach patients under routine clinical conditions.
Exclusion criteria
Prescriptions that were reviewed solely by pharmacy technicians without pharmacist verification were excluded to avoid potential variability in error detection accuracy and to maintain consistency in error classification.
Similarly, records with incomplete or missing essential information, such as undocumented drug details or unspecified error types, were excluded to preserve data quality and ensure the robustness of statistical analyses.
Data tool
Data were extracted using a structured, pre-piloted data collection form. The form was designed to capture key variables, including patient demographics (age, sex, insurance status), clinical setting, prescriber type and all relevant prescription details (drug class, dose, frequency, duration, formulation). A dedicated section was used to record and classify each potential error based on the NCC MERP taxonomy, noting both the error type (e.g. dose, frequency) and its suspected cause.
Variables and measures
The variables assessed in this study were categorized into patient-level, prescription-level and prescriber-level factors. Patient-level variables included the patient’s age (in years), sex (male or female), health insurance status (insured or uninsured), the season during which the hospital visit occurred – categorized as the dry season (November to March) or the rainy (wet) season (April to October) – and the phase of hospitalization, either outpatient or inpatient. Prescription-level variables included the implicated drug and its corresponding therapeutic class, which were classified using the Anatomical Therapeutic Chemical (ATC) system. Prescriber-level variables captured the category of the prescriber, namely medical doctor, physician assistant or nurse/midwife.
Classification of prescribing errors
Prescribing errors were classified according to the ‘type of error’ category of the NCC MERP taxonomy. This involves categorizing errors based on their nature, such as wrong drug selection, omission error, incorrect dose, formulation error, incorrect frequency and incorrect duration. 25 The ‘stage’ and ‘outcome’ categories of the NCC MERP taxonomy were not applied, as the study was specifically focused on characterizing the nature of errors at the prescribing stage. Table 1 provides operational definitions and examples of each error type. 25
Definition of prescribing error types.

Data collection procedure
Written permission was obtained from hospital management prior to data collection. Data were collected from February 3 to March 10, 2025, using a structured abstraction tool developed based on the NCC MERP taxonomy of medication errors. The tool was pre-tested on 30 randomly selected records to ensure its reliability.
Prescribing errors identified and documented in the hospital’s pre-existing incident reporting database by pharmacists during routine care were extracted by research assistants. Data collection was conducted by three pharmacists, each with between 6 and 8 years of clinical experience in a hospital setting, who were trained in the study objectives, data collection tool, and the application of the NCC MERP taxonomy.
To ensure the accurate identification and classification of PEs, a validation process was employed. All potential errors were independently reviewed by two clinical pharmacists, each with over 7 years of experience. Using the NCC MERP taxonomy as a standardized guide, they classified each PE. Any discrepancies between their initial classification were resolved through discussion to reach a final consensus.
Data management and statistical analysis
Data were first exported to Microsoft Excel for cleaning and validation. Records with missing values for key variables were excluded through listwise deletion, representing 4.6% of the 328 prescriptions containing documented errors (Figure 1). All statistical analyses were conducted using STATA version 17 (StataCorp LLC, College Station, TX, USA).
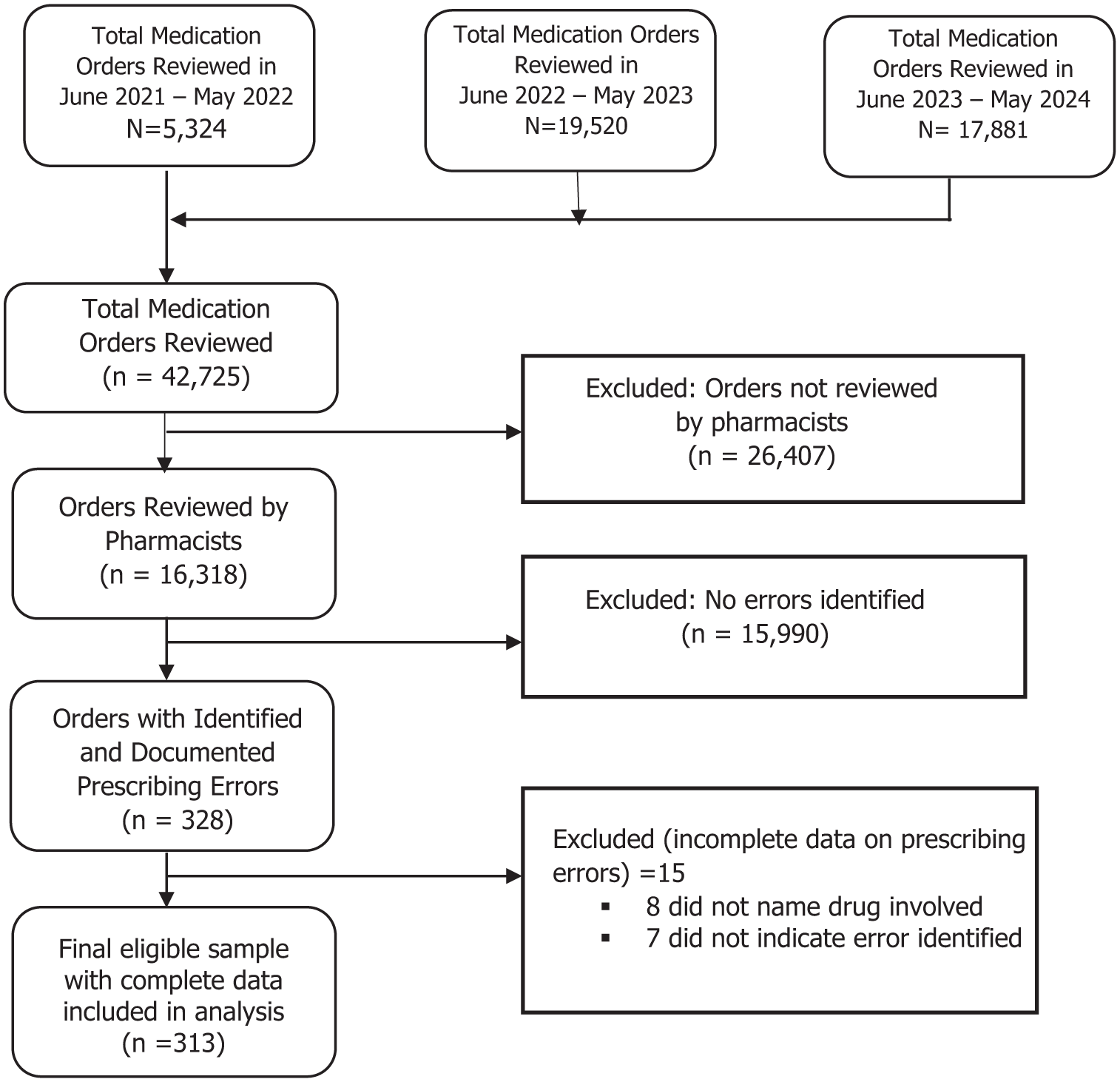
Prescription review and error inclusion process.
Descriptive statistics were used to summarize the data. Categorical variables (e.g. prescriber category, therapeutic class) were presented as frequencies and percentages, while continuous variables (e.g. patient age) were expressed as means with standard deviations (SD) or medians with interquartile ranges (IQR), depending on distribution.
Inter-rater reliability between the two independent clinical pharmacists who categorized PEs was assessed using Cohen’s Kappa coefficient. The strength of agreement was interpreted according to criteria commonly applied in medication error research as described by Forrey et al. 26
The overall prevalence of prescribing errors was calculated as the proportion of prescriptions containing at least one error, expressed as a percentage with 95% confidence intervals (CI). Each of the seven error types – dose, drug selection, commission, duration, formulation, frequency and omission – was analysed as a separate binary outcome variable (1 = error present, 0 = absent). Dummy variables were created following standard procedures. Model fit was assessed using pseudo R², and multicollinearity diagnostics were performed. Variables causing perfect prediction were excluded from regression models.
Univariate logistic regression models estimated odds ratios (ORs) and 95% CIs for associations between each error type and selected predictors: prescriber cadre, patient age group, sex, insurance status, hospitalization phase and season of attendance. Predictor selection was guided by prior literature, clinical relevance and data completeness. Subgroup analyses further explored variations in error distribution across prescriber categories, patient demographics, therapeutic classes, hospitalization phase and seasonal patterns. Statistical significance was set at p < 0.05.
Results
Characteristics of patients with prescribing errors
Out of 16,318 prescriptions reviewed, 313 contained at least one prescribing error. The median age of patients with erroneous prescriptions was 38 years (IQR: 23–59), with the highest prevalence observed among those aged 18–40 (32.3%) and 41–65 years (31.0%). Females were more frequently affected (59.1%), and most errors occurred in the outpatient settings (93.6%). Notably, a large majority (84.7%) of these errors involved patients with active health insurance (Table 2).
Characteristics of patients whose prescriptions had errors.

Prevalence and nature of prescribing errors
There was a high level of inter-rater agreement in classifying the types of prescribing errors (Cohen’s Kappa = 0.91, 95% CI: 0.87–0.94, p < 0.001), indicating near-perfect consistency. The overall prevalence of prescribing errors was 1.92% (95% CI: 1.71–2.13). Physician assistants were responsible for the majority of these errors, contributing to 78.0% of the total. All the errors recorded were classified under Category B of the medication error classification, indicating that although the error occurred, the medication did not reach the patient.
The three most common error types were incorrect frequency of administration (27.8%), commission errors (26.2%) and dose errors (25.2%; Figure 2). Anti-infective agents were the most frequently implicated drug class (43.8%), followed by cardiovascular agents (16.6%). The five individual medications most frequently associated with errors were co-amoxiclav (10.5%), atorvastatin (6.7%), metronidazole (5.4%), cetirizine (5.1%) and nifedipine (4.2%).

Distribution of types of prescribing errors identified at a primary care hospital.
Predictors of prescribing errors
The distribution of error types varied according to patient demographics, prescriber category and contextual factors (Table 3).
Bivariate logistic regression of predictors of prescription errors (by error type).

Bolded values indicate statistical significance.
CI, confidence interval; N/A, not assessed; OR, odds ratio; Ref., reference group.
Dose errors, which accounted for 25.2% of all errors, were most common among younger patients. Specifically, children under 18 years and adults aged 18–40 years recorded the highest proportions, at 34.2% and 35.4%, respectively. These rates declined to 19.0% among those aged 41–65 years and 11.4% in patients aged 66 years and above. Prescriptions issued by nurses were significantly more likely to contain dose errors than those written by physician assistants (OR = 3.02; 95% CI 1.17–7.80; p = 0.022). Anti-infective agents were most frequently implicated in dose errors (45.6%), followed by cardiovascular and respiratory drugs, each contributing 10.1%.
Incorrect drug selection errors, although less frequent (3.2%), were more likely to occur in prescriptions for patients without health insurance. Uninsured patients had over six times the odds of receiving an incorrect drug compared to insured patients (OR = 6.05, 95% CI: 1.68–21.77; p = 0.006). Nurse prescribers were also significantly more likely than physician assistants to commit drug selection errors (OR = 6.35, 95% CI: 1.49–26.91; p = 0.012).
Commission errors, which involve the prescription of unnecessary medications, accounted for 26.2% of all prescribing errors. These were most prevalent among older adults. Patients aged 41–65 years and those aged 66 years or more had significantly higher odds of experiencing commission errors compared to younger patients (<18 years), with ORs of 5.15 and 5.87, respectively (p < 0.001). In addition, doctors were also more likely than physician assistants to commit commission errors (OR = 2.79, 95% CI: 1.49–5.25; p = 0.001). Interestingly, patients without insurance were significantly less likely to receive unnecessary medications (OR = 0.22, 95% CI: 0.08–0.63; p = 0.005).
Duration errors were more common in the inpatient setting, occurring in 15.4% of such cases compared to 5.6% outpatients. These errors were also more frequently recorded during the rainy season, with the difference reaching statistical significance (p = 0.031).
Formulation errors were rare, observed in only 1.9% of cases, but they showed a distinct demographic pattern. All formulation errors occurred in male patients (p = 0.003), and most (83.3%) were seen in patients under 18 years of age.
Frequency errors, the most common type of prescribing error, were slightly more prevalent among males (51.7%) compared to females (48.3%). However, this gender difference was statistically significant only at the bivariate level (p = 0.016). Medical doctors were significantly less likely to commit frequency errors than physician assistants (OR: 0.28; 95% CI: 0.12–0.70; p = 0.006).
Omission errors were significantly more likely among patients without health insurance (OR = 2.66; 95% CI: 1.03–6.85; p = 0.043). Although the elderly population (⩾66 years) accounted for the highest proportion of omission errors (43.5%), this difference was not statistically significant.
Discussion
This study examined the prevalence, types and predictors of prescribing errors in a primary-level hospital in a peri-urban municipality in Ghana. The overall prevalence of prescribing errors was 1.92%, which is significantly lower than rates reported in other settings: 8.8% in the United Kingdom, 27 8.5% in the outpatient department of a regional hospital in Ghana, 21 28.9% in Ethiopia 28 and a median of 54.7% in a systematic review of hospitals across Africa. 11
Several factors may account for the relatively low error rate observed in this study. First, pharmacists screened fewer than half of the total prescriptions issued, raising the possibility that additional errors may have gone undetected in the unscreened portion. Second, the health facility had implemented several safety-enhancing strategies, including adherence to standard treatment guidelines and the use of electronic prescribing systems – interventions that were absent in many of the comparator studies.29,30 These measures likely contribute to error reduction by improving prescription legibility, standardizing dosing and providing real-time alerts for potential drug interactions or contraindications. 31
Moreover, variations in the reported prevalence of prescribing errors across studies may be influenced by differences in error definitions, data collection methods, patient populations and healthcare settings. For example, an Ethiopian study 29 reported an average of 3.9 omission errors per prescription, by including a wide range of issues – from missing clinical information such as diagnosis and prescriber details to non-clinical issues such as spelling mistakes and illegibility. Similarly, studies from Nepal identified high omission error rates and poor adherence to WHO prescribing indicators, such as undocumented diagnoses and excessive polypharmacy. 30
Study methodology also plays a crucial role in the observed variation. Research using direct observation or chart review tends to report higher error rates than studies relying on retrospective reviews or voluntary incident reporting. 32 Furthermore, prescribing errors are more commonly reported among vulnerable populations, such as children and the elderly, due to their complex dosing requirements and comorbidities.33,34 The level of care also influences error rates; tertiary and teaching hospitals, where cases are often more complex, tend to report higher prescribing error rates compared to primary-level facilities, such as the one in this study. 17
The majority of prescribing errors in the present study were committed by physician assistants, which aligns with their central role as frontline prescribers in many Ghanaian primary care facilities. 35 Their high involvement in routine prescribing activities makes their contribution to the total error burden statistically prominent, though not necessarily reflective of higher individual error propensity. Interestingly, nurses and doctors, while accounting for a smaller proportion of total prescriptions, had significantly higher odds of committing specific types of errors, particularly dose and commission errors, respectively. This underscores the importance of targeting prescriber-specific educational and quality assurance interventions that are tailored to practice patterns and clinical responsibilities.
In the current study, anti-infective and cardiovascular drugs were the most frequently implicated classes in prescribing errors, a finding consistent with previous research reporting antimicrobials as the most common drug category involved, with errors including failure to assess patient allergy status, incorrect dosing or renal function adjustments and inappropriate drug selection.28,36 Cardiovascular medications – such as anticoagulants (e.g. warfarin), digoxin, beta-blockers and others – were also prominent, contributing to approximately 16% of errors in some hospital-based studies, often due to inappropriate dosing, drug–drug interactions and inadequate monitoring, all of which pose significant clinical risks given these agents’ narrow therapeutic windows and complex pharmacokinetics.28,34 This pattern highlights the need for careful prescribing practices, allergy checks, dose adjustments and monitoring, especially with these high-risk drug classes.
Patient demographics, particularly age, were significantly associated with prescribing errors in this study, with children experiencing a disproportionately higher burden – especially related to dosing and formulation errors.33,37,38 This finding aligns with existing literature, which consistently identifies paediatric patients as particularly vulnerable due to the complexities of individualized, weight-based dosing and the use of various medication formulations.29,39 Evidence suggests that potentially harmful errors occur up to three times more frequently in children than in adults, with the youngest patients being most at risk.29,40 Common issues include 10-fold dosing errors and incorrect formulation selection. Contributing factors include the need for complex dose calculations and limited paediatric prescribing experience among healthcare providers.33,41 To mitigate these risks, targeted training and mentorship by experienced paediatricians are recommended to enhance prescribing safety in children. 41 In addition, the observed male predominance in formulation errors may reflect underlying disparities in diagnostic and treatment access or sociocultural influences on healthcare-seeking behaviour; however, this warrants further qualitative investigation.
This study found a significant association between insurance status and the occurrence of specific types of prescribing errors. Uninsured patients were more likely to experience omission errors, while commission errors were less frequent in this group. These findings align with existing literature that highlights the impact of socioeconomic factors – particularly insurance status – on medication safety. 42
Uninsured individuals often encounter barriers such as fragmented care, limited access to follow-up services and financial constraints. These challenges can result in incomplete medication histories and less thorough prescribing practices, increasing the risk of omissions and incorrect drug selection. Conversely, the lower prevalence of commission errors – defined as prescribing unnecessary or inappropriate medications – among uninsured patients may reflect more cautious or restricted prescribing driven by cost considerations or limited drug availability.
Seasonal variation appeared to influence prescribing practices, with a higher frequency of errors observed during the rainy season in the bivariate analysis. However, this association did not remain statistically significant in the logistic regression model. The initial trend may reflect increased patient volumes and heightened clinical workload during the rainy season, which can contribute to time constraints and reduced attention to detail. Although not independently predictive, this seasonal pattern highlights the need for resilient health systems and sustained quality improvement efforts, particularly during periods of increased service demand.
All identified prescribing errors were classified as Category B under the NCC MERP Index, indicating that the errors were intercepted before reaching the patient. While this is reassuring and reflects an active safety net within the dispensing process, it underscores a reactive rather than preventive approach to medication safety. The ultimate objective should be to minimize the occurrence of errors at the point of prescribing, thereby reducing reliance on downstream interception.
Relying solely on pharmacy staff to identify and correct prescribing errors is neither sustainable nor fool proof – particularly in high-volume or resource-constrained healthcare settings where staff are frequently overburdened. This was evident in the current study, where fewer than half of all prescriptions were screened by pharmacists due to workload limitations. These findings underscore the urgent need for proactive interventions, including routine training for prescribers and the integration of clinical pharmacists into the prescribing workflow. Clinical pharmacists are specifically trained to conduct real-time medication reviews, support prescribers in selecting appropriate therapies and promote evidence-based prescribing practices. Their involvement as part of multidisciplinary care teams can significantly reduce medication errors at the point of prescribing, thereby enhancing patient safety.
Limitations
This study was based on prescribing errors intercepted and verified by pharmacists at the dispensing stage. As such, it captures only errors identified during pharmacist review and does not include prescriptions dispensed solely by pharmacy technicians, which may have contained undetected errors. Consequently, the findings represent the intercepted error rate – a conservative estimate that likely underrepresents the overall prevalence of prescribing errors within the healthcare system.
In addition, the study did not evaluate the clinical severity, underlying causes, or potential patient harm associated with the identified errors. This limits the ability to stratify errors by clinical significance or to directly guide risk-based interventions. Furthermore, the study did not include a formal sample size analysis, as all available data within the study period were used. This may limit the generalizability of the findings. Finally, as the data were obtained from a single peri-urban primary care facility, caution should be exercised when generalizing these findings to other healthcare settings, particularly tertiary or specialized institutions.
Conclusion
Although prescribing errors in this study were relatively infrequent, they remain clinically important and are influenced by patient-, prescriber- and system-level factors. Enhancing prescribing accuracy and patient safety will require targeted interventions such as structured prescriber training, implementation of clinical decision support tools and the integration of clinical pharmacists into routine workflows for continuous prescription auditing. Particular attention should be given to high-risk groups, including children, the elderly and uninsured patients. Furthermore, strengthening antimicrobial stewardship and institutionalizing regular prescription review processes are critical for advancing medication safety within primary care settings.
Supplemental Material
sj-docx-1-taw-10.1177_20420986251414590 – Supplemental material for Prevalence and predictors of prescribing errors in a primary care setting in Ghana
Supplemental material, sj-docx-1-taw-10.1177_20420986251414590 for Prevalence and predictors of prescribing errors in a primary care setting in Ghana by Richard Delali Agbeko Djochie, Jonathan Boakye-Yiadom, Adwoa Oforiwaa Kwakye, Kwaku Gyamfi Oppong, Ivan Eduku Mozu, Constance Caroline Cobbold and Robert Peter Biney in Therapeutic Advances in Drug Safety
Footnotes
Acknowledgements
The authors sincerely thank the Directorate of Research, Innovation and Consultancy (DRIC) of the University of Cape Coast for organizing the manuscript writing workshop, which significantly contributed to the successful completion of this study. We are especially grateful to Professor Kwaku Oppong Asante and Professor Emmanuel Nii-Boye Quarshie of the University of Ghana, whose expert guidance and mentorship during the workshop were instrumental in shaping the development and refinement of this manuscript. We also express our appreciation to the management of the hospital for granting access to the data used in this study.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.