
Abstract
The safety of medication use in primary care is an area of increasing concern for health systems internationally. Systematic reviews estimate that 3–4% of all unplanned hospital admissions are due to preventable drug-related morbidity, the majority of which have been attributed to shortcomings in the prescribing and monitoring stages of the medication use process. We define high-risk prescribing as medication prescription by professionals, for which there is evidence of significant risk of harm to patients, and which should therefore either be avoided or (if avoidance is not possible) closely monitored and regularly reviewed for continued appropriateness. Although prevalence estimates vary depending on the instrument used, cross-sectional studies conducted in primary care equivocally show that it is common and there is evidence that it can be reduced. Quality improvement strategies, such as clinical decision support, performance feedback and pharmacist-led interventions have been shown to be effective in reducing prescribing outcomes but evidence of improved patient outcomes remains limited. The increasing implementation of electronic medical records in primary care offer new opportunities to combine different strategies to improve medication safety in primary care and to integrate services provided by different stakeholders. In this review article, we describe the spectrum of high-risk medication use in primary care, review approaches to its measurement and summarize research into its prevalence. Based on previously developed interventions to change professional practice, we propose a systematic approach to improve the safety of medication use in primary care and highlight areas for future research.
Keywords
Background
Although licensing systems across the world are designed to ensure that medicinal products entering the market have a favourable risk–benefit balance, drugs frequently cause harm across all healthcare sectors, much of which is preventable. In primary care, the size of the problem is illustrated by systematic reviews which estimate that 3–4% of all unplanned hospital admissions are due to preventable drug-related morbidity [Howard et al. 2006]. In addition, hospital admissions are only the tip of the iceberg of drug-related harm and inconvenience to patients since many preventable adverse drug events (pADEs) are managed in primary care. One systematic review estimates that almost 7 pADEs occur per 100 outpatients annually, of which only a small proportion require hospital admission [Thomsen et al. 2007].
The medication use process in primary care comprises the consecutive stages of prescribing, dispensing, drug administration and medication monitoring, which are shared across a multidisciplinary team of professionals, informal carers and patients [Hepler and Segal, 2003]. While systematic reviews attribute the vast majority of pADEs in primary care in approximately equal parts to shortcomings in prescribing, patient nonadherence and monitoring [Howard et al. 2006; Thomsen et al. 2007], this review article focuses on prescribing and monitoring since these are more directly under professional control. We describe the spectrum of high-risk medication use in primary care, review approaches to its measurement and summarise research into its prevalence. Based on previously developed interventions to change professional practice, we propose a systematic approach to improve the safety of medication use in primary care and highlight areas for future research.
Definition of high-risk prescribing
A pADE has been defined by the United States Institute of Medicine as ‘any preventable injury due to medication’ [Bates et al. 1995]. The causes of pADEs are generally referred to as medication errors, which encompass ‘failures in the treatment process that lead to, or have the potential to lead to, harm to the patient’, including deficiencies in prescribing and monitoring [Aronson, 2009].
Prescribing medicines is an inherently risky and often complex task. Cribb and Barber define appropriate prescribing as ‘a balance between the right technical properties, what patients want and the greater good’ highlighting the potential for conflicts between the different rationales for prescribing [Cribb and Barber, 1997]. Labelling prescribing ‘inappropriate’ or ‘erroneous’ in cases where medication use violates a predefined rule can therefore be simplistic [Hepler and Segal, 2003]. For example, prescription of a nonsteroidal anti-inflammatory drug (NSAID) to a patient taking warfarin is clearly high risk, but will occasionally be appropriate. For a prescriber faced with a patient with active rheumatoid arthritis who has recently been anticoagulated for thromboembolic disease, coprescription may be the least bad choice. We define high-risk prescribing as medication prescription by professionals, for which there is evidence of significant risk of harm to patients, and which should therefore either be avoided or (if avoidance is not possible) closely monitored and regularly reviewed for continued appropriateness.
The spectrum of high-risk prescribing in primary care
In a systematic review of studies investigating the drugs most frequently implicated in preventable hospital admissions, four drug classes accounted for approximately 50% of preventable drug-related hospitalizations: antiplatelet drugs, NSAIDs, diuretics and anticoagulants. A further 21% of preventable admissions were attributed to other cardiovascular agents (beta blockers, angiotensin converting enzyme [ACE] inhibitors, angiotensin receptor blockers, cardiac glycosides), opioid analgesics and antidiabetic agents [Howard et al. 2006]. The bulk of preventable harm in terms of hospital admissions is therefore not due to drugs that should generally be avoided because the risk of harm usually exceeds expected benefits, but rather to therapeutic agents that are commonly used in primary care and have strong indications (the obvious exception being NSAIDs used as simple analgesics).
Table 1 summarizes common patterns of high-risk prescribing that have been implicated in preventable hospital admissions [Howard et al. 2003; Thomsen et al. 2007], demonstrating that preventable harm is often the consequence of not recognizing or taking insufficient account of patients’ needs at a time of particular vulnerability. The following types of preventable hospital admission can generally be distinguished (although they may overlap in individual patients): (1) continuing drugs that are not indicated or no longer indicated, (2) not using drugs that are indicated to prevent adverse drug reactions, (3) using drugs or drug doses that interact with existing medical conditions, (4) using drugs or drug doses that interact with existing drug therapy and (5) inconsistent monitoring.
Reported scenarios of high-risk use of drugs most frequently implicated in preventable drug related hospital admissions [Howard et al. 2003; Thomsen et al. 2007].
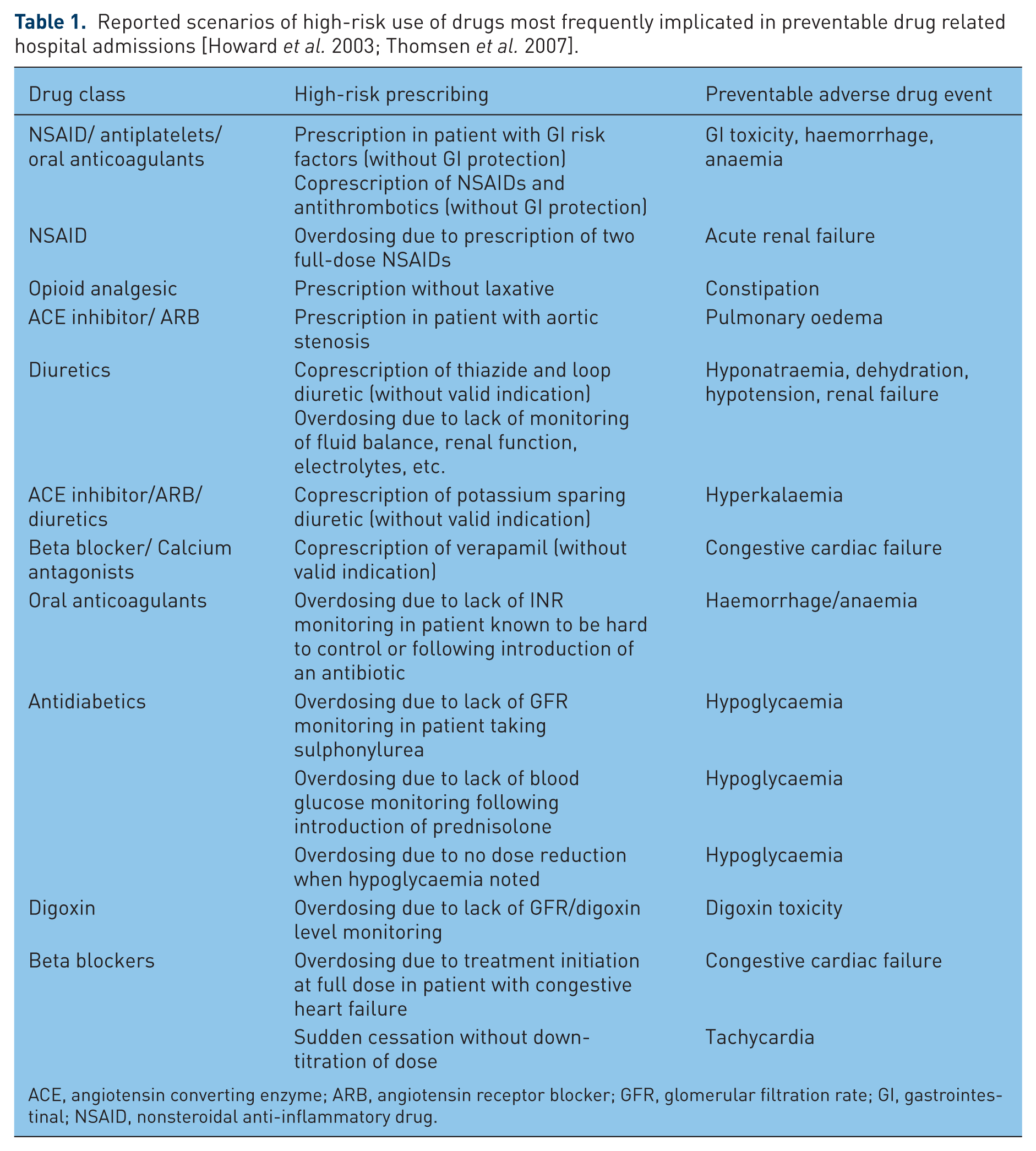
ACE, angiotensin converting enzyme; ARB, angiotensin receptor blocker; GFR, glomerular filtration rate; GI, gastrointestinal; NSAID, nonsteroidal anti-inflammatory drug.
Measurement and prevalence
The safety of medication use can generally be assessed using ‘implicit’ or ‘explicit’ approaches. ‘Implicit’ methods allow the assessor maximum flexibility to account for the clinical context within which prescribing and monitoring decisions take place, whereas ‘explicit’ methods assess medication use against prespecified rules. At the individual patient level, explicit ‘assessment criteria’ yield a dichotomous answer as to the presence or absence of high-risk prescribing while at population level, ‘prescribing indicators’ can be used to measure the percentage of vulnerable patients who are exposed. These distinctions are illustrated in Box 1 using the example of NSAID prescribing.
Illustration of the differences between implicit and explicit methods to assess medication use.
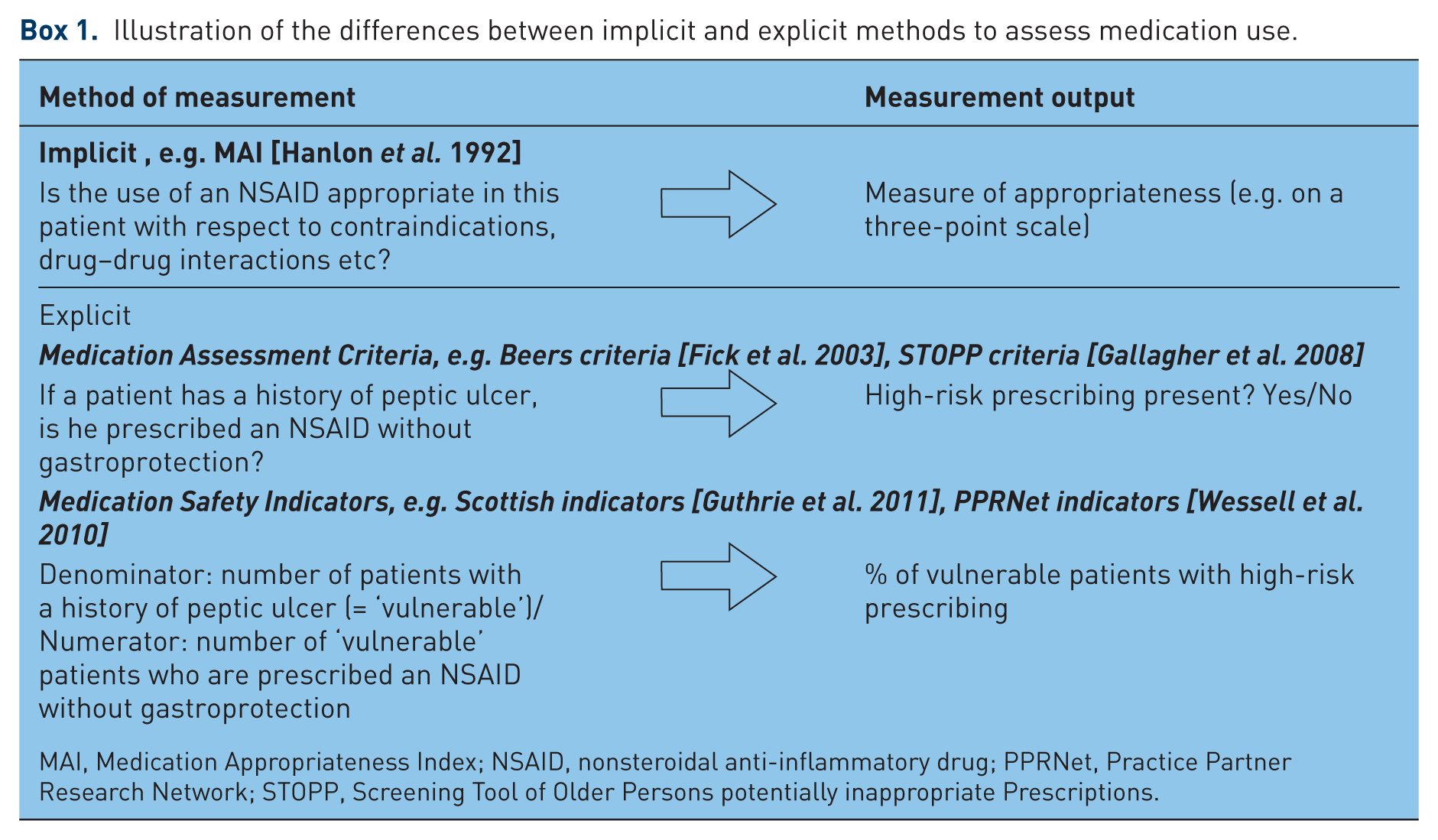
MAI, Medication Appropriateness Index; NSAID, nonsteroidal anti-inflammatory drug; PPRNet, Practice Partner Research Network; STOPP, Screening Tool of Older Persons potentially inappropriate Prescriptions.
Implicit measurement
The most prominent example of an implicit approach is the Medication Appropriateness Index (MAI), where each drug prescribed to a patient is assessed on a three-point scale (appropriate, marginally appropriate, inappropriate) in 10 domains: indication, effectiveness, dosage, directions, drug–drug interactions, drug-disease interactions, expense, practicality, duplication and duration [Hanlon et al. 1992]. A merit of implicit methods is that they allow the assessment of a wide range of therapeutic issues and to judge the appropriateness of prescribing. However, they depend heavily on the knowledge, experience and skills of the reviewer and are time consuming [Hanlon et al. 1992].
Explicit measurement
Explicit approaches are narrower in scope and usually limited to identifying prescribing that is potentially inappropriate, but are more objective and less resource intensive. As a consequence, numerous explicit medication assessment tools have been developed over the last two decades [Beers et al. 1991; Naugler et al. 2000; Fick et al. 2003; Shrank et al. 2006, 2007; Basger et al. 2008; Gallagher et al. 2008; Avery and Rodgers, 2010; Wessell et al. 2010; Guthrie et al. 2011]. Our focus here is on instruments which have been applied in larger-scale studies to measure the prevalence of high-risk or otherwise undesirable medication use in primary care.
Beers criteria
The most cited explicit assessment method is the ‘Beers criteria’, first published in 1991 [Beers et al. 1991] and updated in 2003 [Fick et al. 2003]. The instrument identifies drugs or dosing regimes that should be avoided in the elderly, either in general (e.g. long-acting benzodiazepines), or under specific circumstances (e.g. anticholinergic drugs in people with chronic constipation). The Beers criteria can be assessed relatively easily in routine healthcare data and have been widely applied as a result. Prevalence studies conducted in primary care have reported that between 15% and 30% patients aged 65 years and over were prescribed at least one potentially inappropriate medication listed in the set [Willcox et al. 1994; Zhan et al. 2001; Ay et al. 2005; Simon et al. 2005; Van Der Hooft et al. 2005; De Wilde et al. 2007; Rajska-Neumann and Wieczorowska-Tobis, 2007; Ryan et al. 2009; Leikola et al. 2011]. The Beers criteria have been the gold standard for assessing medication use safety in the elderly for many years but have been criticized more recently because some of the drugs included have valid indications in older people and because of increasing evidence that most harm is caused by drugs which are not listed [Guthrie et al. 2011].
STOPP criteria
The Screening Tool of Older Persons potentially inappropriate Prescriptions (STOPP) consists of 68 medication assessment criteria, which cover a broader spectrum of safety issues than the Beers set [Gallagher et al. 2008]. STOPP not only targets drugs that should be avoided in the elderly but also considers high-risk drug–drug and drug–disease interactions and omissions of risk-mitigating agents. The clinical relevance of the STOPP criteria has been demonstrated in a recently published study, in which the instrument outperformed the updated Beers criteria in predicting the presence of pADEs that were sufficiently serious to contribute to hospital admission [Hamilton et al. 2011]. High-risk prescribing according to STOPP was found to be common in a cross-sectional study of 1329 patients from three GP practices in Ireland, where approximately 1 in 5 (22%) patients aged 65 or older living at home had received one or more high-risk prescriptions in the previous 6 months [Ryan et al. 2009]. Limitations of STOPP include that it exclusively focuses on the elderly, although vulnerability to drug-related harm, such as renal impairment or peptic ulcer, is not uncommon among younger patients. In addition, many items in STOPP rely on information that is rarely consistently recorded in electronic healthcare databases, which is a barrier to routine or large-scale application.
PPRNet indicators
The relative lack of relevant tools to measure high-risk medication use from electronic medical records (EMRs) has led researchers from the Practice Partner Research Network (PPRNet) in the US to develop a new instrument for use in primary care [Wessell et al. 2010]. The PPRNet tool consists of 30 medication safety indicators grouped into five categories (see below). The instrument was applied in a cross-sectional study including all patients aged over 18 years from 20 family practices in 17 US states (n = 52,246). Across all indicators, 61% of all patients met at least one indicator definition of being vulnerable because of their age, pre-existing disease, coprescription or being on treatment that requires laboratory monitoring [Wessell et al. 2010]. ‘Potentially inappropriate prescribing’ and apparent shortcomings in ‘monitoring/preventing potential ADEs’ each affected approximately 25% of patients identified as vulnerable in each category. The rate of ‘potentially inappropriate dosing’ (16%) and ‘potential drug–disease interactions’ (14%) was lower and was lowest for ‘potential drug–drug interactions’ (2%).
Scottish indicators of high-risk prescribing
Guided by similar motivations to the PPRNet researchers, we have recently completed a study to develop a set of medication safety indicators that can be operationalized within EMRs, using a modified RAND panel [Fitch et al. 2003] of general practitioners and primary care pharmacists [Dreischulte et al. 2012]. A subset of 15 indicators targeting high-risk prescribing of NSAIDs, warfarin, antipsychotic drugs, methotrexate and drugs that can aggravate heart failure was applied in a cross-sectional population database analysis of 1.76 million patients registered with 315 Scottish general practices in 2007 [Guthrie et al. 2011]. There were 7.9% of registered patients who met at least one indicator definition of being vulnerable and 13.9% of these patients had received at least one high-risk prescription in the previous year.
Although the estimated prevalence depends on the indicator set used, it is clear that high-risk prescribing in primary care is common. In addition, the data presented here is likely to substantially underestimate its prevalence, since even instruments comprising a reasonably large number of indicators [Fick et al. 2003; Gallagher et al. 2008; Wessell et al. 2010] cannot comprehensively cover the spectrum of medication safety. While it is important to note that only a fraction of patients affected by high-risk medication use will ultimately be injured, avoiding high-risk medication use where possible, and regularly reviewing such prescribing if it is judged to be essential, is a prerequisite to averting preventable harm. In our study of 315 general practices in Scotland, rates of high-risk prescribing varied approximately fourfold between practices after case mix adjustment [Guthrie et al. 2011], suggesting considerable scope for reducing such prescribing.
Quality improvement approaches
Root causes of preventable drug-related harm
There is relatively little research into the root causes of preventable drug-related harm. Nevertheless, a qualitative study conducted in 2004 provides useful insights into the weaknesses of medication use systems in UK primary care, which were associated with 18 common causes of preventable drug-related hospital admission [Howard et al. 2007]. In all of these cases, preventable patient harm was the consequence of active failures at multiple stages of the medication use process, including prescribing, dispensing, administration, monitoring and help seeking by patients. High-risk prescribing was most commonly caused by knowledge gaps about patients’ medical and medication histories and insufficient pharmacotherapeutic knowledge of prescribers. Potential defence mechanisms against harm were frequently undermined by inadequacies in the design of computerized decision support systems (CDSSs), lack of access to relevant patient information by community pharmacists and communication problems between all stakeholders (GPs, hospital specialists, community pharmacists and patients). Workload pressures exacerbated these problems at all stages.
Previously tested interventions
There is a large body of research examining changing professional practice to improve the quality of care, much of which has been systematically reviewed [Jamtvedt et al. 2006; O’Brien et al. 2007]. Strategies which have been successfully applied to improve medication use processes include the following:
CDSSs, particularly when integrated into clinician’s workflow, and when alerts are system-activated rather than relying on user activation [Garg et al. 2005; Kawamoto et al. 2005]. A systematic review of CDSS studies focusing specifically on improving prescribing and monitoring [Pearson et al. 2009] found that alerts were most consistently effective when they targeted the initiation of high-risk drugs rather than stopping existing treatments. For example, in a study of 107 Canadian primary care physicians, CDSS significantly reduced new high-risk prescriptions (NSAIDs, benzodiazepines, tricyclic antidepressants) but had no impact on stopping long-term use of hypnotics [Tamblyn et al. 2003]. CDSS were also found to be effective in reminding clinicians to conduct laboratory tests for monitoring long-term treatments, such as warfarin [Demakis et al. 2000].
Feedback of performance data particularly when baseline performance is low and when feedback is more ‘intensive’ by targeting individuals, being verbal or prolonged, or when delivered by senior staff [Jamtvedt et al. 2006]. Feedback, often in combination with educational outreach, has been shown to reduce high-risk NSAID prescribing [Pit et al. 2007], excessive use of opioids and other regulated analgesics [Anderson et al. 1996], and hypnotics in the elderly [Smith et al. 1998].
Pharmacist-led interventions targeted at patients and/or prescribers [Royal et al. 2006; Nkansah et al. 2010]. Multidisciplinary models involving pharmacists in primary care or outpatient settings have been shown to be successful in improving a wide range of endpoints relevant to medication safety, including reduction in therapeutic duplication and cessation of treatments no longer needed [Nkansah et al. 2010], composites of high-risk prescribing and monitoring [Avery and Rodgers, 2010], reductions in medications implicated in falls [Zermansky et al. 2006] and overall improvement in medication appropriateness [Hanlon et al. 1996].
Overall, it is important to note that the effectiveness of these three types of intervention varies between studies, and few have been shown to improve patient as opposed to prescribing outcomes [Royal et al. 2006; Holland et al. 2007; Nkansah et al. 2010]. This may in part be attributable to the fact that many trials to date have used outcome measures that are insufficiently sensitive to improvements in medication use (e.g. quality of life or all-cause rather than drug-related hospitalization)[Royal et al. 2006]. However, in view of the complexity of the medication use system in primary care [Howard et al. 2007], it may also reflect the limitations of approaches that target specific aspects of a single process, such as prescribing.
Proposal for an integrated system to improve medication safety
The high disease burden associated with high-risk prescribing, the large numbers of patients affected, and the fact that shortcomings in the primary care infrastructure are an important underlying cause, call for a more systematic approach to improving medication safety. The increasing use of EMRs in primary care offer new opportunities to integrate complementary defence mechanisms against preventable ADEs from high-risk prescribing or monitoring deficiencies. EMRs can be exploited: (1) to implement CDSS alerts that prompt prescribers to explicitly consider patient vulnerability at the time of decision making; (2) to systematically identify patients who have received high-risk prescriptions or are due monitoring tests for targeted review and follow up; and (3) to provide timely and continuous performance feedback to monitor prescribing patterns and identify those in need of improvement. Although these three approaches have strong face validity, a number of challenges and uncertainties remain with respect to their specific design and implementation.
Challenges for implementation and future research
Decision support
A commonly reported problem in existing CDSSs is that highly important alerts are often ignored, because practitioners are desensitized by multiple alerts of minimal clinical relevance (alert fatigue). A US study from 2009 found that physicians ignored >90% of alerts with little association with the severity of the alert [Isaac et al. 2009]. The authors conclude that the ‘systems and the computers that are supposed to make physicians’ lives better are actually torturing them’ [Isaac et al. 2009]. The ability to customize alerts to the preferences of users may therefore be crucial in this respect, but requires careful selection of prompts that should always be considered because of potentially serious consequences [Sheikh et al. 2011]. A further problem is that alerts often only trigger when a drug is newly prescribed, meaning that prescribers will not explicitly be alerted to situations where continued prescribing becomes high risk due to changes in clinical circumstances [Guthrie et al. 2011].
Systematic follow up of patients at risk of adverse events
Even with optimal implementation, patients may still slip through the system of alerts that are triggered at the time of decision making. EMRs can be used to facilitate systematic identification, regular review and monitoring of patients to identify where such treatments are necessary or have been issued by mistake. For example, dual antiplatelet treatment with aspirin and clopidogrel is strongly indicated after myocardial infarction or stent implementation but at least doubles the risk of bleeding compared with aspirin alone [Delaney et al. 2007]. Regularly searching EMRs for patients where treatment duration is longer than recommended will ensure that patients do not inadvertently continue a medication that is no longer indicated. In addition, a systematic approach to identifying patients for review may also allow distributing the associated workload across the multidisciplinary team. ‘For example, although high-risk prescribing is currently not a UK Quality and Outcomes Framework (QOF) topic, QOF financial incentives have stimulated practices to identify patients who are not treated according to evidence-based practice standards in order to improve their care, and this has significantly been achieved by the greater involvement of practice nurses in delivering systematic chronic disease management’ [Grant et al. 2009]. Pharmacists might play a similarly important role in reviewing high-risk prescribing.
Collaboration in medication management, and in particular a greater role for pharmacists in primary care, have long been advocated [The Scottish Government, 2010; Bond et al. 2000; Roth et al. 2009]. However, shared access to relevant patient information and adequate funding are prerequisites for more effective collaboration [Howard et al. 2007]. In addition, better integration of services provided by doctors and pharmacists is likely to also rely on overcoming the more tacit interprofessional barriers [Hughes and McCann, 2003; Howard et al. 2007] and on providing pharmacists with the necessary skills to function in a professional role that is still new to many [Howard et al. 2007; Krskaj and Avery, 2007; Salter et al. 2007].
Performance feedback
Decision support alerts can be complemented by routine feedback of prescribing safety data in order to monitor the performance of the medication use system as a whole. For example, indicator scores (percentage of vulnerable patients affected by high-risk prescribing) can be compared with internal or external benchmarks in order to identify variations in prescribing that need further investigation. However, most reported audit and feedback interventions are one off rather than sustained, and performance feedback is often limited to a small number of indicators [Pit et al. 2007; Avery and Rodgers, 2010], which are only likely to address a fraction of the wide spectrum of high-risk medication use. Although EMRs make it feasible to assess medication use against a wider range of assessment criteria, more research will be required to test different ways of data feedback that do not overwhelm practitioners [Guthrie et al. 2005]. Composite performance scores can make data presentation more efficient, but are often not sufficiently specific to guide the selection of actionable targets for improvement [Hysong et al. 2006; Guthrie, 2008].
In view of the plethora of potentially unsafe medication use practices it is clear that decision support alerts, criteria used to target patients for review and indicators used in performance feedback will require prioritization by clinical relevance. However, this is often undermined by a lack of primary evidence about the degree of harm. For example, the risks of many drug–drug interactions, such as coprescribing of NSAIDs with ACE inhibitors and diuretics (the ‘triple whammy’ [Loboz and Shenfield, 2005]), are not well quantified, and the evidence to support many monitoring recommendations is very limited. The growth of large, linkable electronic databases should allow more systematic study of the risks of prescribing in primary care in the future.
Conclusions
Despite major differences in measurement instruments, high-risk prescribing in primary care has been shown to be common, consistent with a lack of focus on medication safety in the past. Aging populations and the associated increase in the prevalence of multimorbidity and polypharmacy is likely to further exacerbate the problem of preventable drug-related morbidity. It is time for concerted efforts to improve the safety of medication use in primary care, which is likely to require multifaceted approaches across the entire spectrum of prescribing and monitoring processes.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors, but during the writing of this paper, TD was funded by Scottish Government Chief Scientist Office Applied Research Programme (grant number 07/02). The funder had no role in writing the paper.
Conflict of interest statement
The authors have no conflicts of interest to declare.