
Abstract
Background:
Rational prescribing optimizes medicine use, reduces costs, and improves patient outcomes. However, adherence to rational prescribing practices varies, particularly in low- and middle-income countries like Ghana, where healthcare systems differ across urban, peri-urban, and rural settings.
Objectives:
This study assessed adherence to WHO/INRUD prescribing indicators in public hospitals and determined each hospital’s Index of Rational Drug Prescribing (IRDP).
Design:
A retrospective descriptive study was conducted in 25 public hospitals across rural, peri-urban, and urban settings in the Ashanti Region of Ghana.
Methods:
Data from 5091 patient encounters were analyzed to assess prescribing indicators, including the average number of medicines per encounter, generic prescribing, adherence to the Essential Medicines List (EML), antibiotic use, and injection prescribing. IRDP scores were calculated, and geographic comparisons were performed using analysis of variance (ANOVA), with p < 0.05 considered statistically significant.
Results:
No hospital met the WHO target of <2 medicines per encounter (regional average: 3.63 ± 0.62). Generic prescribing averaged 72.26%, and EML adherence was 91.85%, with no hospital achieving 100%. Antibiotic prescribing exceeded the <30% target, averaging 60.84%. Injection use aligned best with WHO standards (average: 13.42%), with 22 of 25 hospitals meeting the <20% threshold. The regional IRDP was 3.67, with rural hospitals scoring lowest (3.63), followed by peri-urban (3.64) and urban hospitals (3.81). No significant geographic differences in IRDP scores were observed (p > 0.05).
Conclusion:
While injection use aligns with WHO standards, gaps remain in generic prescribing, antibiotic use, and EML adherence. Strengthening prescriber training, antimicrobial stewardship programs, and policy enforcement is essential to improving prescribing practices and patient outcomes in public hospitals in the Ashanti Region.
Plain language summary
Doctors and other healthcare providers must prescribe medicines in a way that is safe, effective, and affordable for patients. This study looked at how well hospitals in Ghana’s Ashanti Region follow international guidelines for good prescribing practices. Researchers collected data from 25 hospitals across rural, peri-urban, and urban areas, analyzing 5,091 patient records to assess key prescribing patterns.
The study found that, on average, patients received more medicines per visit than recommended, and the use of generic medicines (cheaper, equally effective alternatives) was lower than ideal. While most hospitals prescribed medicines from the approved Essential Medicines List, none fully met the 100% target. A major concern was the high use of antibiotics—double the recommended limit—raising the risk of antibiotic resistance. However, the use of injectable medicines was mostly appropriate, meeting international standards.
Overall, prescribing quality varied slightly between rural and urban hospitals, but the differences were not statistically significant. The study suggests that better training for prescribers, stricter policies, and improved access to essential medicines could help hospitals improve their prescribing practices, leading to better patient care.
Keywords
Introduction
The rational use of medicines (RUM) is critical for achieving optimal health outcomes by ensuring that patients receive appropriate medications tailored to their specific conditions. It requires prescribing the right drug, in the correct dosage, for the appropriate duration. 1 Rational prescribing enhances patient safety by minimizing adverse drug reactions, improving therapeutic efficacy, reducing antimicrobial resistance, and optimizing healthcare costs.1 –4 Conversely, irrational prescribing—characterized by over-prescribing, under-prescribing, or incorrect prescribing—poses significant risks to patients and healthcare systems alike. Over-prescribing, such as the misuse of antibiotics for viral infections, escalates healthcare costs and contributes to resistance, while under-prescribing can result in suboptimal treatment outcomes.5 –8 Factors such as gaps in physician knowledge, patient expectations, pharmaceutical marketing, and inadequate monitoring systems further exacerbate the problem.4,7,9
Globally, irrational prescribing remains a major challenge, with the WHO estimating that nearly 50% of medicines are prescribed, dispensed, or sold inappropriately. 1 A systematic review across Africa revealed troubling trends: the average number of medicines per patient encounter was 3.1, antibiotics were prescribed in 46.8% of cases, and injections in 25%. 10 These figures exceed WHO standards and highlight the urgent need for interventions, particularly in resource-limited settings.
In Ghana, significant progress has been made in rational prescribing, particularly in increasing generic prescribing, improving adherence to the Essential Medicines List (EML), and reducing reliance on injections.11 –13 However, some challenges remain, especially regarding the overuse of antibiotics and the tendency to prescribe more medicines per patient encounter than recommended by WHO standards.12,14
While previous studies have provided valuable insights, their focus on single healthcare facilities limits the generalizability of their findings. A multi-facility study is needed to assess prescribing practices more broadly. This study addresses this gap by evaluating prescription indicators at outpatient departments in 25 public hospitals across the Ashanti Region of Ghana, covering rural, peri-urban, and urban settings. Specifically, the study aimed to assess adherence to World Health Organization/International Network for Rational Use of Drugs (WHO/INRUD) prescription indicators and determine each hospital’s Index of Rational Drug Prescribing (IRDP). By identifying key gaps and trends, the findings will inform targeted interventions to promote rational prescribing, enhance patient safety, and optimize healthcare delivery in Ghana and similar settings globally.
Materials and methods
Study design and setting
This retrospective descriptive study reviewed 5091 outpatient prescriptions from all 25 government district hospitals providing primary healthcare services in the Ashanti Region of Ghana. The data covered prescriptions issued between July 1, 2022, and June 30, 2023, ensuring a 1-year timeframe to account for seasonal variations in prescribing patterns.
A systematic sampling approach was used, with each hospital contributing between 194 and 216 prescriptions. This approach aligns with WHO guidelines 15 and ensures adequate representation of prescribing practices across facilities. The Ashanti Region, home to approximately 5.4 million 16 people across 43 districts, includes urban, peri-urban, and rural areas, providing a diverse setting for assessing prescribing patterns.
This study was designed and reported following the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines (Supplemental Table 1). 17
Sample size justification
While the WHO/INRUD guidelines recommend a minimum of 600 prescriptions for smaller-scale studies, a larger sample size was selected to enhance statistical power and improve the precision of estimates. The final sample of 5091 outpatient medication orders was determined based on data availability, ensuring sufficient representation across all hospitals. This expanded sample allowed for more robust subgroup analyses, reducing bias and improving the generalizability of findings.
Inclusion and exclusion criteria
Outpatient prescriptions containing at least one medication from public hospitals in the Ashanti Region were included in the study. However, prescriptions from specialized clinics, such as antenatal care, hypertension, diabetes, antiretroviral therapy, and tuberculosis clinics, were excluded to prevent bias from unique prescribing patterns. In addition, incomplete or illegible prescriptions were omitted to ensure data accuracy and reliability. Prescriptions that did not contain any medication were also excluded, as the study focused on medication use in outpatient care.
Index of Rational Drug Prescribing
The IRDP was used to assess adherence to RUM across hospitals. This composite index incorporates key prescribing indicators, including non-polypharmacy, safe injection use, adherence to the EML, rational antibiotic use, and generic prescribing. The indices for non-polypharmacy, safe injection use, and antibiotic prescribing were calculated by dividing the optimal value by the observed value, while adherence to the EML and generic prescribing were determined by dividing the observed value by the optimal value. An index score closer to 1 signifies better compliance with rational prescribing standards, whereas significantly lower scores indicate deviations from recommended practices. The overall IRDP was obtained by summing the five individual indices, with a maximum possible score of 5—higher values reflecting stronger adherence to WHO/INRUD prescription guidelines.18 –20
Data collection
A data collection tool adapted from the WHO manual for prescription indicator surveys 15 was used to extract relevant information. This included patient demographics, the number of medicines prescribed, the number of medicines prescribed by generic names, the number of medicines prescribed from the EML, the presence of an antibiotic, and the presence of an injection.
Antibiotic appropriateness was assessed using Ghana’s Standard Treatment Guidelines. 21 The tool was piloted at a non-study hospital using 60 prescriptions to refine its usability. Data collection occurred between August 10 and November 15, 2023, by practicing pharmacists who were members of the research team.
Study variables and data analysis
Prescription indicators were evaluated based on WHO/INRUD standards. These indicators include the following:
Average number of medicines per encounter.
Percentage of encounters with an antibiotic.
Percentage of encounters with an injection.
Percentage of medicines prescribed by generic names.
Percentage of medicines prescribed from the EML.
International Nonproprietary Names from the Ministry of Health EML were used to determine the percentage of generic and EML prescribing. 22 The prescription indicators evaluated in this study, along with their WHO/INRUD optimal values as reported by Ofori-Asenso 23 and their corresponding calculation formulae, are summarized in Table 1.
Prescription indicators and their optimal values for public hospitals in the Ashanti Region, Ghana.

EML, Essential Medicines List; INN, International Nonproprietary Name.
Data cleaning was performed using Microsoft Excel 2016, while statistical analysis was conducted with STATA version 17 (StataCorp, College Station, TX, USA). 24
Continuous variables were summarized using means with standard deviations or medians with interquartile ranges, depending on data distribution, while categorical variables were presented as counts and percentages. Hospitals were ranked based on their IRDP scores, and differences across urban, peri-urban, and rural locations were assessed using analysis of variance (ANOVA) tests. A significance level of p < 0.05 at a 95% confidence interval was applied for all comparisons.
Results
A total of 5091 patient encounters were sampled across 25 district hospitals in the region, with rural districts accounting for 2654 encounters (52.13%), peri-urban districts contributing 1633 encounters (32.08%), and urban districts reporting 804 encounters (15.79%). The average number of medicines prescribed per encounter in the region was 3.63 ± 0.62, with rural hospitals recording the highest average (3.89), followed by peri-urban hospitals (3.52) and urban hospitals exhibiting the lowest and most consistent prescribing patterns (3.23) as shown in Table 2. Hospital 17 recorded the lowest number of medicines per encounter (2.72 ± 1.16), while Hospital 6 had the highest (5.61 ± 1.54), with one-fifth of hospitals exceeding four medicines per encounter.
Prescription indicators across public hospitals in the Ashanti Region, Ghana.
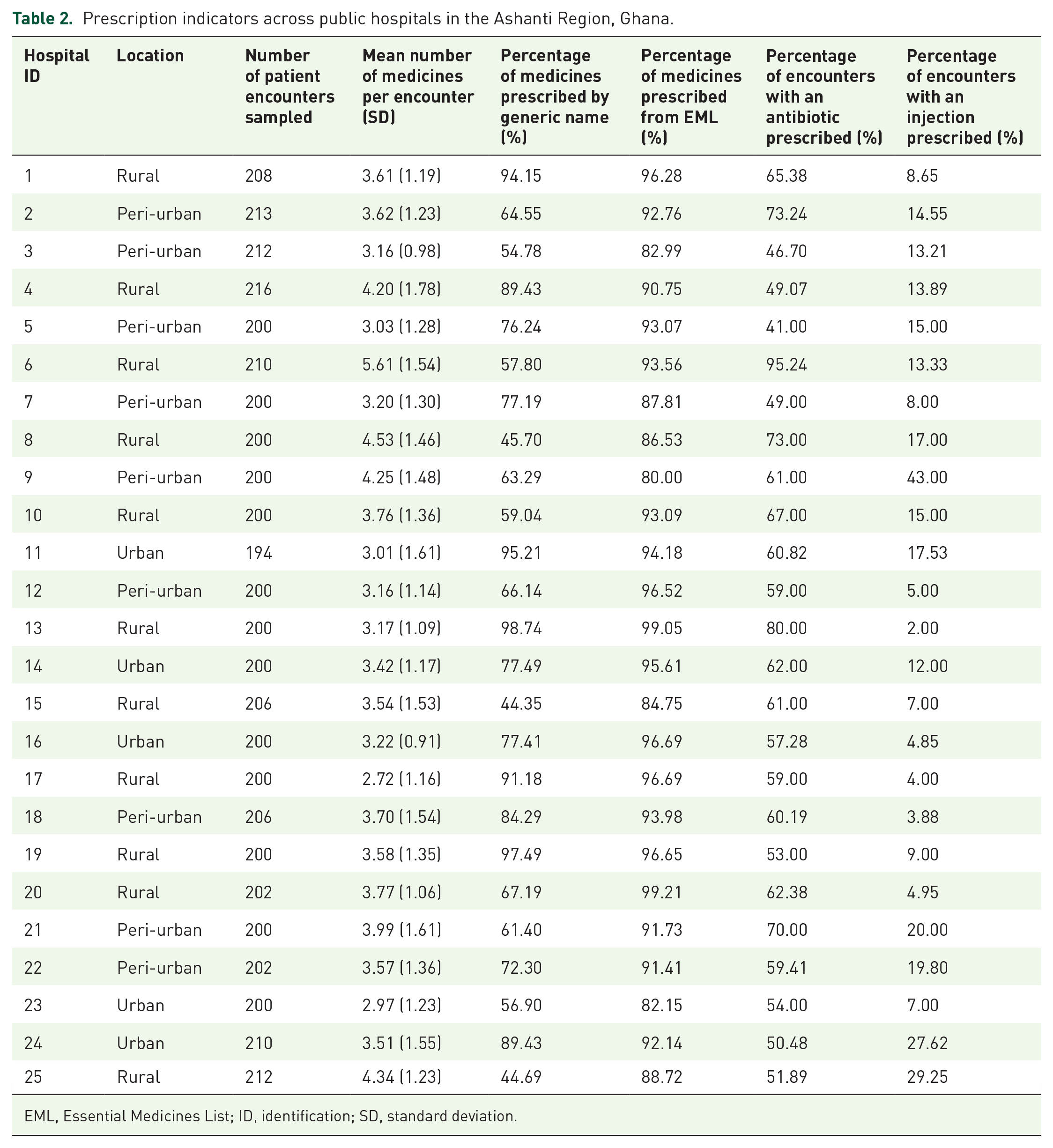
EML, Essential Medicines List; ID, identification; SD, standard deviation.
The average injection prescribing rate across public hospitals was 13.42%, falling within the WHO-recommended standard of <20%. While 80% of hospitals adhered to this guideline, 20% exceeded the threshold, with the highest rate recorded at 43.00%. By location, peri-urban hospitals had the highest injection prescribing rate (15.83%), followed by urban hospitals (13.80%) and rural hospitals (11.28%). By contrast, antibiotic prescribing rates were alarmingly high, with an average of 60.84% across the region—more than double the WHO-recommended standard of <30%. All hospitals exceeded this threshold, with rural hospitals having the highest rate (65.18%), followed by peri-urban hospitals (57.73%) and urban hospitals (56.92%).
Generic prescribing and adherence to the EML also fell short of WHO standards. The average generic prescribing rate was 72.26%, with no hospital meeting the 100% target. Urban hospitals had the highest rate (79.29%), followed by rural hospitals (71.80%) and peri-urban hospitals (68.91%). Similarly, adherence to the EML averaged 91.85%, with rural hospitals showing the highest compliance (93.21%), followed by urban hospitals (92.15%) and peri-urban hospitals (90.03%).
Hospital 17 achieved the highest IRDP score of 4.12 out of 5, excelling across all indices, closely followed by Hospitals 5 and 19 with scores of 4.08 and 4.07, respectively (Table 3). Most hospitals performed well in rational injection prescribing, with an index of 1.00, but generic prescribing showed considerable variation, ranging from 0.44 to 0.99. Low-performing hospitals, such as Hospitals 25, 9, and 8, had IRDP scores below 3.20, struggling particularly with polypharmacy and rational antibiotic use. On average, the regional IRDP score was 3.67 ± 0.34, with rural hospitals attaining the lowest score (3.63 ± 0.39), followed by peri-urban hospitals (3.64 ± 0.35), while urban hospitals performed best, averaging 3.81 ± 0.17. However, ANOVA results revealed no statistically significant differences in IRDP scores across rural, peri-urban, and urban locations (F = 0.531, p = 0.595).
Indices of rational drug prescribing and performance rankings across 25 hospitals in the Ashanti Region, Ghana.

IRDP score: The IRDP is the sum of all indices, representing overall rational prescribing performance. Ranking: Higher IRDP scores indicate better prescribing practices, with Rank 1st representing the best performance. If two hospitals have the same IRDP score, the next rank will skip one position to account for the tie.
EML, Essential Medicines List; ID, identification; IRDP, Index of Rational Drug Prescribing.
Discussion
The prescribing indicators assessed in this study provide critical insights into medication use practices in public hospitals across rural, peri-urban, and urban settings in the Ashanti Region of Ghana. The findings reveal several areas requiring improvement to align with optimal standards for rational medicine use. The average number of medicines prescribed per patient encounter of 3.63 ± 0.62 is comparable to the 3.7 14 reported in the Greater Accra region of Ghana but higher than the 1.99 reported in Tanzania 25 and the 0.98–2.5 range observed in Ethiopia. 26 However, it is lower than the 4.01 11 recorded in the Eastern region of Ghana and the 4.37 reported in Sierra Leone. 27 The higher prevalence of polypharmacy in rural hospitals may reflect limited access to prescribing references and training in rational prescribing, prompting broader prescribing practices, while urban hospitals’ lower rates could be attributed to better adherence to guidelines and access to well-trained professionals. These findings underscore the need for targeted interventions to address polypharmacy through the establishment or strengthening of drug and therapeutic committees within the hospitals, particularly in rural settings.
The average generic prescribing rate was 72.26%, falling short of the WHO target of 100%. Among facility types, urban hospitals had the highest rate (79.29%), followed by rural hospitals (71.80%) and peri-urban hospitals (68.91%). This rate is higher than the 68% 10 reported in a systematic review of the WHO African Region and the 62.6% 14 observed in the Greater Accra region of Ghana. However, it remains lower than the 99.4% 28 recorded in Ethiopia and the 84.4% 25 reported in Tanzania. This variability may reflect differences in prescriber preferences, training, and awareness of the cost-saving benefits of generic medicines, as reported in a study in Taiwan. 29 Similarly, adherence to the EML averaged 91.85%, falling short of the optimal 100%. Rural hospitals demonstrated the highest compliance (93.21%), followed by urban hospitals (92.15%) and peri-urban hospitals (90.03%). While this rate exceeds the 88% reported for the WHO African Region, 10 it remains lower than the 99.8% 28 observed in Ethiopia and the 97.6% 25 recorded in Tanzania. These findings highlight the need for stronger policies, improved availability of essential medicines, and stricter enforcement of prescribing standards.
Antibiotic prescribing rates were alarmingly high, averaging 60.84% across the region—more than double the WHO-recommended target of <30%. Rural hospitals had the highest average rate (65.18%), followed by peri-urban hospitals (57.73%) and urban hospitals (56.92%). This rate exceeds the 51.6% 25 observed in Tanzania, the 32.2% 30 reported in Saudi Arabia, and the 46.8% 10 recorded in a systematic review of the WHO African Region. However, it remains lower than the 86.4% observed in Ethiopia. 28 The high rate of antibiotic prescribing in rural hospitals observed in this study aligns with findings from rural China, 31 where doctors frequently prescribed antibiotics for viral acute upper respiratory infections, despite these conditions typically not requiring them. Similarly, a study from the United States 32 found that rural doctors were more likely to inappropriately prescribe antibiotics for urinary tract infections in women.
The over-reliance on antibiotics in rural settings raises significant concerns about antimicrobial resistance. This trend may stem from diagnostic uncertainties due to a lack of laboratory resources to confirm infections, insufficient training among prescribers to explore alternative causes of fever, or limited access to non-antibiotic treatment options.31,32 To address these gaps, capacity-building initiatives are essential. These include routine training for prescribers on rational medicine use, strengthening Drug and Therapeutics Committee (DTC) activities for stricter monitoring, and implementing antibiotic stewardship programs.4,9,33 Such measures could improve adherence to rational prescribing practices and mitigate the risks associated with antibiotic overuse.
Injection use was the only indicator that demonstrated notable success, with an average prescribing rate of 13.42%, which falls within the WHO-recommended standard of less than 20%. Peri-urban hospitals recorded the highest rate (15.83%), followed by urban hospitals (13.80%) and rural hospitals (11.28%). This rate is comparable to a study in Ethiopia, which also reported 13.4%, 28 but is higher than the 2% 30 recorded in Saudi Arabia and the 8.3% 14 observed in the Greater Accra region of Ghana. However, it is lower than the 25% 10 reported in a systematic review of the WHO African Region. While 80% of hospitals adhered to this guideline, 20% exceeded the threshold, with rates as high as 43.00%. This overuse may reflect patient preferences, prescriber habits, or insufficient enforcement of guidelines. Despite this, the overall adherence to rational injection prescribing highlights the effectiveness of guidelines in this area.
The overall IRDP for the region was 3.67 ± 0.34. This figure fell short of findings from a similar study in Saudi Arabia 30 where the IRDP ranged from 3.71 to 5.0. However, the region’s performance was better than a study in Tanzania, 25 which reported an IRDP range of 2.81–2.90, though lower than an Eritrean study 34 with a range of 4.18–4.49. On average, rural hospitals had the lowest IRDP score (3.63 ± 0.39), followed by peri-urban hospitals (3.64 ± 0.35), while urban hospitals recorded the highest score (3.81 ± 0.17). Despite these differences, ANOVA test results showed no statistically significant variations in IRDP scores across locations. This suggests that the observed disparities may stem from systemic challenges rather than geographic factors, indicating that location did not have a substantial impact on performance.
Study limitations
This study’s descriptive design limits its ability to assess prescribing trends or establish causality over time. In addition, its focus on public hospitals may not fully represent prescribing practices in private healthcare facilities. These limitations highlight the need for further research to provide a more comprehensive understanding and strengthen efforts to improve rational medicine use.
Conclusion
While injection use met WHO standards, challenges persist with polypharmacy, generic prescribing, adherence to EML, and excessive antibiotic use—particularly in rural hospitals. The high reliance on antibiotics emphasizes the need for enhanced prescriber training, antimicrobial stewardship, and stricter enforcement of prescribing guidelines.
Although urban hospitals demonstrated higher IRDP scores, systemic factors likely contribute to prescribing disparities. Strengthening DTCs, improving healthcare provider training, and ensuring a stable supply of essential medicines are critical steps toward aligning prescribing practices with global standards. Hospitals with suboptimal performance could benefit from peer learning and mentorship programs with better-performing facilities.
In addition, public education campaigns are essential to address patient expectations for antibiotics and injections, which often drive inappropriate prescribing. Finally, investing in diagnostic resources—especially in rural and peri-urban hospitals—will support evidence-based prescribing and help curb unnecessary antibiotic use.
Supplemental Material
sj-docx-1-taw-10.1177_20420986251346321 – Supplemental material for Adherence to WHO/INRUD prescription indicators in public hospitals: evidence from the Ashanti Region, Ghana
Supplemental material, sj-docx-1-taw-10.1177_20420986251346321 for Adherence to WHO/INRUD prescription indicators in public hospitals: evidence from the Ashanti Region, Ghana by Richard Delali Agbeko Djochie, Rita Owusu-Donkor, Elizabeth Modupe d’Almeida, Francis Kwadwo Gyamfi Akwah, Emmanuel Kyeremateng, Samuel Opoku-Afriyie, Cecilia Akosua Tabiri, Francis Kyei-Frimpong, Samuel Dwomoh, Francis Fordjour and Jonathan Boakye-Yiadom in Therapeutic Advances in Drug Safety
Footnotes
Acknowledgements
The authors are grateful to the Regional Director of Health and the managers of the participating hospitals for their support in conducting this study.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.