
Abstract
The increasing off-label use of medications needs a robust pharmacovigilance system. This is particularly crucial given the abundance of scientific data that can be harnessed to ensure a product’s safety. Our review focuses on the off-label use of local anesthetics, a common practice in topical and intracameral applications. However, the occurrence of mydriasis, as indicated in the monographs/summaries of product characteristics, is an unexpected adverse event. Our aim is to provide a comprehensive understanding of mydriasis caused by local anesthetics, both as an unexpected adverse event and as an off-label use, to reinforce the importance of pharmacovigilance practices. We conducted a comprehensive search in Medline/PubMed and Google Scholar from two distinct perspectives: examining the occurrence of mydriasis with the use of local anesthetic as an adverse event and as an off-label use. Our search yielded 14 articles that reported mydriasis as an unexpected adverse event with the use of anesthetics, with dental procedures being a significant contributor to this type of event. Also, we identified eight articles that explored the off-label use of local anesthetics to induce mydriasis, with the most common method of drug administration being intracameral injection. These findings underscore the importance of our research in understanding the unexpected adverse event of mydriasis and the potential for off-label use of local anesthetics. They also highlight the need for continued involvement and vigilance in this area, as our understanding of these phenomena continues to evolve and further investigation is crucial. The use of local anesthetics for mydriasis holds significant promise, particularly in ophthalmological surgeries. This approach could potentially mitigate the adverse events associated with conventional mydriatics, offering a more efficient and safer alternative. Furthermore, using a single medication for akinesia, anesthesia, and mydriasis could significantly enhance the efficiency and convenience of surgical procedures. On the other hand, it is crucial to extend the knowledge of the mydriasis-anesthesia association through risk minimization activities (e.g., the inclusion of monographs/summary of product characteristics) to communicate the risk of mydriasis with the use of local anesthetics.
Plain language summary
Why was the study done?
Unknown side effects of drugs can lead to undesired effects, but in some cases, they can lead to the discovery of beneficial effects that could significantly improve patient health.
What did the researchers do?
We searched the literature in Medline/PubMed and Google Scholar from two perspectives on the presence of mydriasis with the use of local anesthetic as an undesired and beneficial effect.
What did the researchers find?
This review has found several cases of undesired mydriasis caused by local anesthetics. However, it is essential to note that their beneficial use as mydriatic is also commonly observed in topical and intracameral applications, especially in ophthalmic surgeries.
What do the findings mean?
Although mydriasis could be considered an undesired event in some therapeutic interventions, this review considers the potential use of local anesthetics to induce mydriasis since it represents a promising new therapeutic indication that interests the medical community, particularly given their frequent use in ophthalmological surgeries.
Introduction
According to the information in the monograph/summary of product characteristics (SmPC), unexpected adverse events are inconsistent in nature, severity, or consequence.1,2 Since the monograph/SmPC is the document that provides information to health professionals, it must be updated periodically to avoid perpetuating outdated data that may result in adverse events, therapeutic failures, or unnecessary treatments. 3
The update of monograph/SmPC is initiated according to risk management, which aims to detect new risks related to drugs and consequently proceed to implement minimization activities, contributing to the continuous evaluation of the benefit–risk balance of drugs4,5; these data come from different sources, such as literature, clinical trials, spontaneous notifications, and pharmacovigilance studies. 6
Moreover, after administering a drug, the presence of some adverse events could have an unexpected beneficial effect on the patient’s health without having an approved indication for its use7–9; these unapproved beneficial effects result in off-label use of the drug since, for its approval as a new therapeutic indication, new information about the molecule must be submitted to demonstrate the safety and efficacy of the drug while maintaining a positive benefit–risk balance. 10
Off-label use is increasing, prompting efforts to fortify pharmacovigilance practices, and due to that, significant scientific data could be gathered, potentially leading to new therapeutic indications from adverse events that are typically considered unwanted.7,9
Despite mydriasis being an unexpected event according to their monographs/SmPCs of local anesthetics,11–13 several cases of mydriasis caused by local anesthetics in ophthalmological procedures have been described.14–16 Furthermore, since 1977, there have been signs of the mydriatic response of local anesthetics, 17 and currently, their off-label use is commonly observed in topical and intracameral applications.18–20 Therefore, the review aims to provide a comprehensive understanding of mydriasis caused by local anesthetics, both as an unexpected adverse event and off-label use, to reinforce the importance of pharmacovigilance practices.
Methodology
For the literature review, a search was conducted in Medline/PubMed and Google Scholar from two viewpoints of the presence of mydriasis with the use of local anesthetic (adverse event and off-label use). Adverse events inclusion criteria: (1) case reports, (2) association anesthetic event. Off-label inclusion criteria included the following: (1) clinical trials, (2) mydriasis with local anesthetics; exclusion criteria included the following: (1) use concomitantly with known mydriatic drugs (e.g., alpha-adrenergic or anticholinergics).
This search was conducted independently by two investigators; then, the principal investigator collected and compared the information to ensure proper compliance with the inclusion and exclusion criteria mentioned before; in case of discrepancies between the two researchers, the principal investigator made the final decision. The keywords used for searching are as follows: adverse events (local anesthetic adverse event, local anesthetic mydriasis, local anesthetic anisocoria, local anesthetic eye, local anesthetic pupil size, local anesthetic iris); and off-label use (lidocaine + pupil, lignocaine + pupil, mydriasis local anesthetics, local anesthetics off-label, surgery local anesthetics). In total, 22 articles were retrieved (14 for adverse events and 8 for off-label use)
Local ophthalmic anesthetics
Most local anesthetics used clinically have a three-part chemical structure:
An aromatic ring (benzoic or para-aminobenzoic acid) corresponds to the lipophilic portion and is responsible for diffusion through the nerve membrane.
An intermediate connecting functional group that binds to the amino group via an ester or amide.
A hydrophilic amino group is essential in the water solubility of the molecule and, consequently, its biodistribution.
The molecules come in two forms: non-ionized (responsible for diffusion) and ionized (responsible for binding to the intracellular receptor of the neuron).21–24
According to the connecting functional group, anesthetics are classified into two types: ester type (cocaine, procaine, tetracaine, benzocaine) and amide type (lidocaine, mepivacaine, bupivacaine, ropivacaine). 22
Pharmacokinetic
Specific physiological and anatomical mechanisms prevent the absorption of ophthalmic drugs: (I) Physiological, such as tear turnover, nasolacrimal drainage, and blinking; (II) Anatomical, which are divided into static ones, such as the corneal epithelium, stroma, and blood–aqueous barriers, and dynamic ones, such as blood flow, lymphatic flow, and tear drainage. 25
The pharmacological effect of ophthalmic local anesthetics depends on three essential factors: pKa, lipid solubility, and melanin binding. 26
Ionized local anesthetics cannot cross the nerve membrane; therefore, the speed of their diffusion depends on the ionized/non-ionized ratio. Consequently, local anesthetics with high pKa (tetracaine pKa = 8.5) have a slower onset of anesthesia than those with low pKa (lidocaine pKa = 7.8).25–27 Factors that modify the physiological pH, such as inflammation or the use of other drugs, alter the action of local anesthetics. 26
Lipid solubility is a factor that also affects the biodistribution of local anesthetics because the corneal epithelium is lipophilic; therefore, drugs with high lipid solubility have a greater capacity to pass into the ocular structures.18,25,26
Finally, melanin in dark eyes is essential for its bioavailability due to local anesthetics binding to melanin, causing a minor but sustained effect compared to light eyes. 25
Pharmacodynamic
Local anesthetics interrupt the electrical impulse propagation of nerve axons by reversible binding of voltage-gated sodium channels across the neural membrane at the nodes of Ranvier (myelinated axons) and along the entire axon (unmyelinated axons).21–23,28 Therefore, the concentration to blockade the nerve impulse is lower in unmyelinated nerve fibers (type C), being able to cause complete analgesia without affecting motor and tactile function, named “differential block” (sequential blocking of sensory information).21,22,28
Many authors mention that channels other than sodium channels, such as potassium and calcium channels,21,29–31 are inhibited by local anesthetics. Even studies carried out by Hollmann et al. demonstrated the blockade of muscarinic M1 and M3 receptors by local anesthetics.32,33
Topical ophthalmic anesthetics primarily impact the corneal epithelium and stroma, and the drug that crosses the anterior chamber also anesthetizes the iris and ciliary body. However, the pharmacological effect is influenced by the amount of melanin since the duration of the effect may be different in pigmented and non-pigmented irises.27,34
The pupil
The pupil, whose diameter ranges between 2 and 9 mm, is conditioned by two opposite contractile elements, the iris sphincter muscle (constrictor) and the radial muscle (dilator), which are controlled by the autonomic nervous system through the parasympathetic (short ciliary nerves) and sympathetic (long ciliary nerves) derived from the ciliary ganglion located between the lateral rectus muscle and the orbital apex.35–38 This structure protects the retina against overexposure to light and provides a correct focus through accommodation jointly with changes in crystalline lens position.35,37,39 The retina can adjust to light exposure, but such adaptation is slower than that mediated through pupil contraction. 37
Mydriasis
The noradrenergic sympathetic system innervation acts through the excitatory 1α pupillary receptors. 36 The 1α adrenergic receptors are a G protein-coupled receptor associated with the Gq subunit, which activates phospholipase C (PLC) and hydrolyzes PIP2 to diacylglycerol (DAG) and inositol triphosphates (IP3), causing calcium release with subsequent contact of the radial muscle.36,40
This system is regulated by posterior hypothalamic nuclei spread through the cervical/thoracic spinal cord to the superior cervical sympathetic ganglion, moving through the ciliary ganglion without synapsing and innervating the eye through the long ciliary nerves.35,37,38 The regulation of the sympathetic system is complex and less understood than the parasympathetic since factors that modify the sympathoadrenal neurotransmission in the hypothalamus, that is, cognition, emotions, and pain, could cause mydriasis. 36
Myosis
The pupillary contraction at the molecular level is mediated by the muscarinic receptors, especially the M3 and M2. The M3 receptors are coupled to PLC, which generates IP3 and DAG, which cause calcium release, promoting the contraction of the sphincter iris muscle; on the other hand, the M2 receptor is negatively coupled to adenylate cyclase, causing the dilating effect of the sphincter iris muscles is not carried out.36,41
The intricate process of pupillary contraction is regulated by a subcortical reflex mechanism triggered by light and accommodation when viewing close objects. This reflex is mediated through the parasympathetic nervous system. 36
Light-mediated pupillary contraction involves the capture of photoreceptive impulses by the rods, cones, and ganglion cells; these impulses are then transmitted via the optic nerve to the pretectum of the midbrain and subsequently to the Edinger-Westphal (EW) nuclei, where the information is processed, afterward, the efferent neurons of the EW nuclei synapse with the neurons of the ciliary ganglion, which innervate the iris sphincter muscle through short ciliary nerves, leading to pupillary constriction.35–37,42,43
Pupillary contraction is also mediated by accommodation when observing nearby objects regulated by the retinal ganglion axons that excite the lateral geniculate body and subsequently distributed for the visual cortex; once analyzed by the latter, the efferent neurons provide excitatory to the EW nucleus, and from then on it produces the same excitatory effects as those mediated by light until reaching pupillary contrition. 36
Cases analysis
As an adverse event
During the review, 14 articles (26 patients) were found with mydriasis after the use of anesthetics in patients within an age range of 20–77 years (average 47.34 ± 19.24); dental procedures (6 patients) were most prevalent for this type of event, followed by blepharoplasty (4 patients) and photocoagulation (4 patients; Table 1)14–16,44–54; however, until now, this event has a status of “unexpected” according to the monograph/SmPC of different local anesthetics,11–13 despite its use as an off-label topical mydriatic.55,56
Mydriasis is an unexpected adverse event by the use of local anesthetics.

The mechanism proposed in most articles with mydriasis is focused on the ciliary ganglion; these support various author hypotheses since anesthetics provoke blockage in the nerve cells or have a neurotoxic effect in neurons that innervate the ciliary ganglion or since the lesion produced is very similar to a tonic Adie’s pupil with pupillary dilation, poor reaction to light, loss of accommodation, and positive denervation.14–16,44,46,47,49–52,54
However, some authors are not very sure that local anesthetics could be the cause of mydriasis, for example, D’Souza et al. mention that although they propose the mechanism of mydriasis mediated by anesthetics, they believe that the effect is caused by epinephrine entering the eyeball through the nasolacrimal duct 52 ; or the case of Kappen and Cols, where it is hypothesized that it could be related to other factors, such as surgery or postoperative ocular coverage. 15
Off-label use
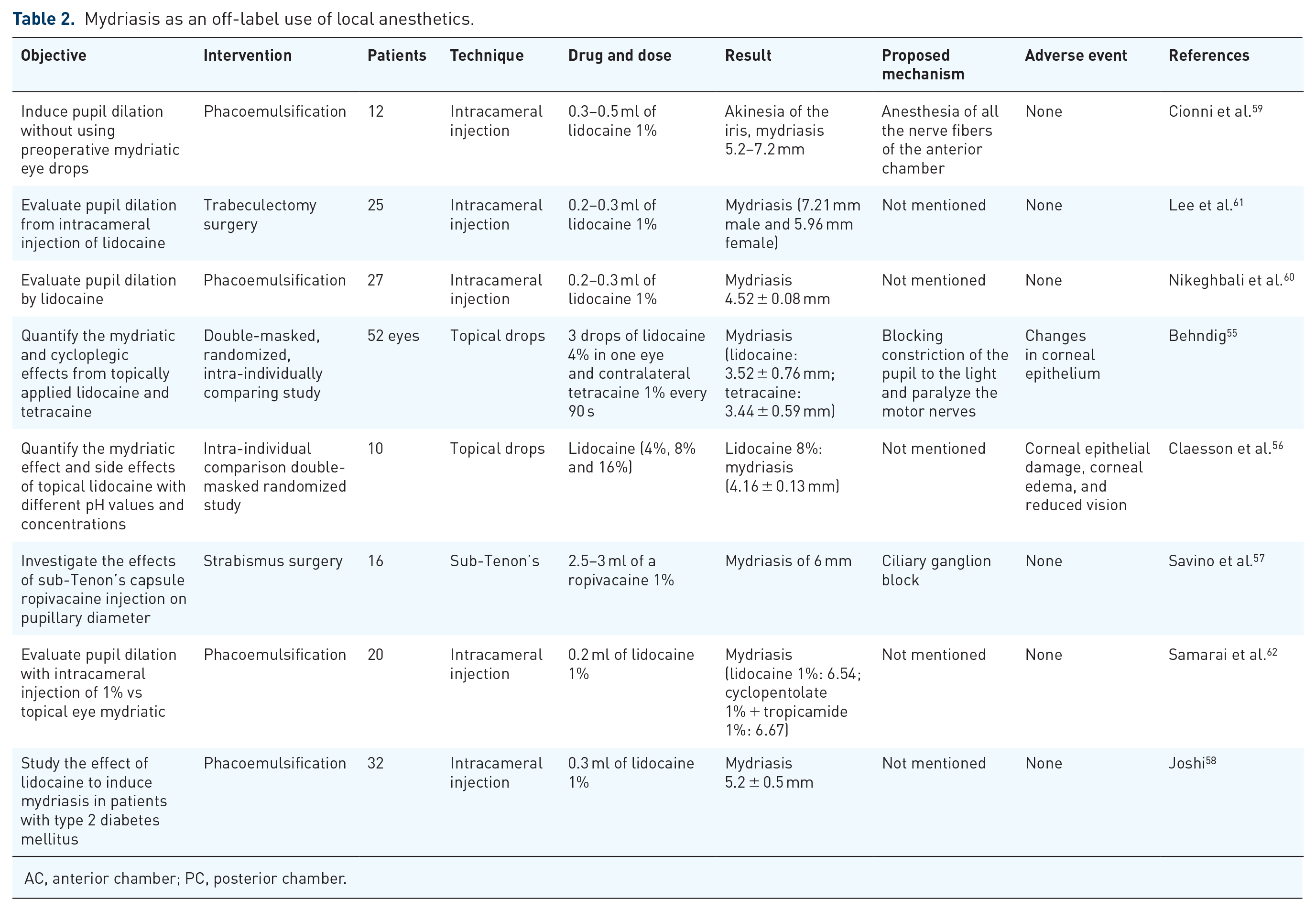
During the literature review, 8 articles (168 patients) in which local anesthetics were used to induce mydriasis were identified. The most frequent drug administration was by intracameral injection (5 articles), topical drops (2 articles), and one sub-tenon administration (Table 2).56–62 Two of them presented adverse events; (1) Claesson et al. mention the presence of corneal epithelial damage and corneal edema, but this occurred at high doses of lidocaine (16% used six times), and they concluded no adverse events occurred at the dose in which lidocaine presents the maximum mydriasis 56 ; and (2) Behndig mentioned the presence of adverse effects on the corneal epithelium; however, they concluded that is entirely reversible and are not clinically significant even at large doses. 55
Mydriasis as an off-label use of local anesthetics.
AC, anterior chamber; PC, posterior chamber.
In addition to its high-security profile, the literature review emphasizes the benefits of local anesthetics for use as a mydriatic, such as:
II. Few systemic adverse events. 59
III. Its use causes akinesia (retrobulbar and peribulbar administration), anesthesia, and mydriasis without the need for other medications and consequently reduces intraoperative discomfort.57,58,60
IV. It avoids severe cardiovascular effects, particularly in people with hypertension, cardiovascular diseases, and children.56,59,60
V. Unlike topical mydriatics, they do not cause additional inflammation and prevent endothelial cell loss, so their use is recommended in patients with chronic pathologies such as “Guttata.” 59
VI. Greater light tolerance, especially when using a microscope light during surgery. 59
VII. A decrease in the presence of superficial punctate keratopathy. 59
Hypothesis
Based on the literature search, three hypotheses about mydriasis caused by local anesthetics can be summarized: efferent nerve anesthesia, afferent nerve anesthesia, and ciliary ganglion anesthesia.
Efferent nerves anesthesia
Akinesia has been observed in peribulbar and retrobulbar anesthesia, suggesting blockage of efferent nerves,63–68 analogically it could provoke the iris muscle blockage. However, there needs to be more information to confirm this hypothesis because most of this type of anesthesia does not present mydriasis.16,63–70 Therefore, the blockage of efferent neurons could be caused intraocularly, according to studies carried out by May et al. and Shelton et al., which mention the existence of a large number of non-myelinated neurons within the eyeball,71,72 making them more prone to local anesthetics,21,28,73 triggering the blockade of the efferent neurons from both the adrenergic (sympathetic) pathway derived from the cervical ganglion as well as the acetylcholine (parasympathetic) pathway mediated by the EW nucleus (Figure 1).

Mydriasis as an off-label use of local anesthetics.
Afferent nerves anesthesia
While no information currently supports the optic nerve anesthesia hypothesis, several investigations have shown that optic nerve anesthesia indicates neuronal damage.63,64,68,74 The loss of myelination inside the eye could block nerve impulses,21,28,71–73 thereby preventing the afferent transmission of information and preventing light-mediated and accommodation contraction. However, the low bioavailability in the posterior chamber and in the ganglion cells may be a limitation in this hypothesis 75 (Figure 1).
Ciliary ganglion anesthesia
There is support in the literature for the anesthesia of the preganglionic sympathetic neuron since, as can be seen in Figure 1, it is the only one that contains a preganglionic neuron type B,36,41,76 and has poorly myelinated fibers, 76 which would be susceptible to blockage by the administration of local anesthetics, obstructing the transmission of the acetylcholine (parasympathetic) impulse that is responsible for the contraction of the circular muscle, causing mydriasis (Figure 1). Furthermore, Peñarrosa et al. mention that intraoral anesthetics and, therefore, those used in maxillary surgery produce mydriasis due to the proximity of the ciliary ganglion with the sphenomaxillary space 54 ; and this could explain the many adverse events in this type of surgery, such as those mentioned in Table 1.
Conclusion
The mydriatic effect of topical anesthetics is currently recognized, although their use is off-label. Clinical results have been promising, mainly because these drugs are commonly used in ophthalmological surgeries. Their application could help avoid the adverse events associated with traditional mydriatics, induce rapid pupillary dilation to minimize surgical time, facilitate the recovery of pupillary size as early as the first postoperative day, and enhance the patient experience. Importantly, using a single medication for akinesia, anesthesia, and mydriasis makes this approach an efficient option, ensuring a more comfortable experience for patients undergoing surgery. However, further research is necessary to evaluate topical anesthetics’ efficacy, safety, and appropriateness for mydriasis as a new therapeutic application. In addition, it is essential to reach a consensus among experts regarding the proposal of this drug for clinical practice.
Besides, pharmaceutical companies must enhance the medical community’s understanding of the association between mydriasis and anesthesia through risk minimization efforts. This could include disseminating information such as monographs or a SmPC to communicate the risks of mydriasis associated with local anesthetics, especially given the described mechanism of mydriasis and the consistently demonstrated relationship between the drug and this adverse drug reaction.
Footnotes
Acknowledgements
The authors thank Alejandra Sánchez Rios, MD, and Ricardo Osvaldo Jauregui Franco, MD, for their assistance writing the medical manuscript.