
Abstract
Background:
Antibody–drug conjugates (ADCs), as a new type of targeted drug, have been widely used in breast cancer patients in recent years. However, while achieving better efficacy, its hepatotoxicity should not be ignored.
Objectives:
To clarify the incidence of hepatotoxicity associated with ADCs and compare the incidence of hepatotoxicity of ADCs with different drugs.
Design:
We performed a systematic review and meta-analysis to summarize the clinical trials and combined the data using meta-analysis.
Methods:
We searched the PubMed, Embase, and Web of Science databases up to March 12, 2023. The primary outcome was the incidence of ADC-related hepatotoxicity in breast cancer patients. The data were merged using Stata 17.0 software.
Results:
ADCs caused a high incidence of all grades of hepatotoxicity. Sacituzumab govitecan caused the highest incidence of all grades of alanine aminotransferase (ALT) elevation at 25.30% (95% confidence interval (CI): 19.29–31.82). Trastuzumab deruxtecan caused the highest incidence of all grades of aspartate aminotransferase (AST) elevation. The highest incidence of AST elevation was 31.89% (95% CI: 18.56–46.85). Conversely, trastuzumab emtansine caused the highest incidence of grade ⩾3 AST and ALT elevation (incidence rates were 3.95% (95% CI: 2.39–5.85) and 3.42% (95% CI: 1.95–5.24), respectively).
Conclusion:
Hepatotoxicity is an adverse reaction that cannot be ignored when ADCs are used for treating breast cancer. Moreover, clinicians should pay more attention to the assessment of patients’ liver function and monitoring of liver indices, particularly ALT and AST, when using ADCs.
Plain language summary
Why was this study conducted? In recent years, ADCs have increasingly been used as targeted agents in breast cancer patients. However, while they provide better efficacy, the hepatotoxicity they produce may affect drug usage and patient prognosis. What did the researchers do? The research team collected studies published before March 12, 2023, extracted relevant hepatotoxicity index results from those studies, regrouped them for analysis, and calculated the incidence of hepatotoxicity caused by ADCs. What did the researchers find? The incidence of hepatotoxicity caused by ADCs was generally high, with trastuzumab emtansine causing the highest incidence of severe hepatotoxicity. Trastuzumab deruxtecan, on the other hand, caused relatively little liver toxicity. What do these findings mean? Our findings suggest that clinicians should closely monitor liver function in breast cancer patients treated with ADCs and promptly assess the extent of liver injury in patients who develop abnormal liver function markers. Dose reduction or discontinuation should be considered when necessary.
Background
Breast cancer is one of the most common cancers in women worldwide and the leading cause of cancer deaths in women. 1 According to cancer data released by the World Health Organization, the number of new cases of breast cancer has surpassed that of lung cancer to become the most prevalent cancer worldwide. 2 Therefore, treatment of breast cancer has become a top priority. At present, antibody–drug conjugates (ADCs) are used for treating breast cancer after chemotherapy, targeted therapy, and immunotherapy. 3 Furthermore, ADCs are a new class of drugs that cannot be ignored in treating breast cancer. Numerous clinical trials have shown that ADCs can improve the progression-free survival (PFS) and overall survival (OS) of patients with breast cancer.4,5 Therefore, they are widely used in the treatment of breast cancer.
ADCs are antibody-coupled compounds consisting of three key components: antibodies, linkers, and small-molecule cytotoxic drugs. The targeting effect of ADCs is demonstrated by their ability to recognize highly expressed tumor cell surface antigens and bind with antigens to form ADC antigen complexes. These complexes are endocytosed by lattice proteins into the tumor cells releasing a cytotoxic load through lysosomal lysis, which damages DNA or tumor cell division and kills tumor cells. 6 Therefore, ADCs are often given the title of “precision killer.”
However, ADCs have been shown to cause toxic side effects while achieving better clinical efficacy.7,8 ADCs cause various toxic side effects, including interstitial pneumonia, hepatotoxicity, ophthalmic toxicity, and neurotoxicity.9,10 Among the various toxic side effects of ADCs, hepatotoxicity has received widespread attention because it may cause interruption of ADC treatment and worsen patients’ conditions. Currently, trastuzumab emtansine (T-DM1), among ADCs, has been reported to cause hepatotoxicity.11,12 However, the incidence of hepatotoxicity caused by other ADCs in breast cancer has not been reported. Furthermore, no study has systematically elucidated the incidence of hepatotoxicity caused by different ADCs in breast cancer.
Therefore, we conducted a comprehensive review and meta-analysis of ADC-related hepatotoxicity in breast cancer to compare the incidence of hepatotoxicity among different ADCs by integrating data from clinical trials.
Methods
Our report follows the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 13 statement for preferred reporting of meta-analyses and systematic evaluations.
Search strategy and nerfing criteria
We systematically searched English language literature on ADCs for breast cancer in the PubMed, Embase, and Web of Science databases up to March 12, 2023. We searched each of the four ADCs separately, T-DM1 drugs using the following search terms “Ado-Trastuzumab Emtansine,” “Kadcyla,” “huN901-DM1,” “Trastuzumab-DM1 Conjugate,” “Trastuzumab-DM1,” and other T-DM1 related subject terms with “Breast Neoplasm,” “Breast Tumors,” “Breast Cancer,” “Mammary Cancer,” “Breast Carcinoma,” and other breast cancer-related subject terms combination search. The T-Dxd drug was searched using the following search terms “trastuzumab deruxtecan,” “DS-8201a,” “DS-8201,” and “T-Dxd” in combination with breast cancer. SG drugs were searched using the following search terms “sacituzumab govitecan,” “IMMU-132,” and “HRS7-SN38” in combination with breast cancer. The RC-48 drug was searched using the following search terms “disitamab vedotin,” “RC48,” “RC-48,” and “Aidixi” in combination with breast cancer. Furthermore, the protocol for this systematic review and meta-analysis was registered with the International Prospective Register of Systematic Reviews (PROSPERO CRD42023460361). In case of duplicate publications, articles providing the most detailed data were included in the meta-analysis. The studies that met the following criteria were included: (1) clinical trials, (2) studies that included ADC-treated patients with breast cancer, and (3) studies on subjects receiving therapy with ADC. The exclusion criteria were as follows: (1) retrospective studies, case reports, meta-analyses, and reviews; (2) studies that did not mention indicators related to ADC hepatotoxicity (i.e., alanine aminotransferase (ALT), aspartate aminotransferase (AST), alkaline phosphatase (ALP), blood bilirubin, and gamma-glutamyl transferase (GGT)); (3) studies with a sample size fewer than 30 cases; and (4) duplicate studies. The literature search was performed according to the PRISMA statement. This study was an analysis of published and publicly available data and therefore did not require ethical approval from an institutional review board.
Data extraction
Two authors (Ping Yang and Hengheng Zhang) extracted data separately from the included studies using standardized forms. In case of disagreement, arbitration was performed by a third author (Yi Zhao). We extracted the following data and study characteristics for the included studies using an Excel spreadsheet: first author, year of publication, study name, drug, trial phase, number of patients in the safety analysis, and number of elevated ALT, AST, ALP, blood bilirubin, and GGT in all grades and grade ⩾3. The extracted data were further integrated and analyzed by Stata 17.0 software (StataCorp, College Station, TX, USA).
Study objective
The primary outcome is the incidence of all grades of ALT, AST, ALP, blood bilirubin, and GGT elevation in patients with breast cancer due to the use of ADCs. The secondary outcomes were the incidence of grade ⩾3 ALT, AST, ALP, blood bilirubin, and GGT elevations and the incidence of ALT and AST elevations caused by different drugs.
Data analysis
The randomized and nonrandomized controlled studies included herein were assessed using the Cochrane Risk of Bias Worker (RoB version 2.0) and MINORS criteria, respectively. We statistically analyzed the data using Stata version 17.0. The weight of each study in the analysis depended on the sample size of individual studies based on the total number of patients, and the proportion of patients enrolled in each study was calculated. Forest plots were used to visualize the incidence of each study, and 95% confidence intervals (CIs) were calculated using the binomial method. I 2 statistic and p value were used to estimate study heterogeneity. The larger the I 2 , the greater the heterogeneity. We considered I 2 > 50% or p < 0.1 to imply substantial heterogeneity, which was calculated using a random effects model. Conversely, a fixed-effects model was used. Publication bias was assessed by funnel plots and Egger’s test.
Quality assessment
Because this study included both randomized and nonrandomized controlled studies, it was evaluated separately using the Cochrane Risk of Bias Tool (RoB version 2.0) 14 and the MINORS scale. 15 The Cochrane Risk of Bias Tool includes six aspects: selection bias, implementation bias, measurement bias, follow-up bias, reporting bias, and other biases. The results of the evaluation were plotted on a risk of bias diagram using Revman version 5.3. The MINORS scale consists of 12 evaluation indicators, each of which is scored from 0 to 2, with 0 indicating that no information was reported, 1 indicating that the information was reported but was insufficient, and 2 indicating that the information was reported and sufficient information was provided.
Results
Study selection and characterization
We retrieved 5684 articles from the databases (Figure 1). After removing duplicate records, 1186 unique titles and abstracts were reviewed for relevancy. By reading the titles and abstracts, 1136 articles were not relevant to our study, and 50 articles were screened for possible suitability. Finally, 6685 patients from 25 trials were included in our study. Three trials reported two treatment groups with different regimens, thereby yielding 28 independent study cohorts from 25 trials for analysis (Table 1). The included studies included 12 randomized controlled trials and 13 single-arm clinical trials. These studies included T-DM1 (n = 17),16–32 T-Dxd (n = 5),33–37 and SG (n = 3),38–40 with T-Dxd and T-DM1 sharing the same trial. Furthermore, 21 studies reported elevated ALT, of which only 1 study examined all grades because data on grade ⩾3 elevations were not mentioned. In all, 20 studies reported elevated AST, of which only one study examined all grades because data on grade ⩾3 elevations were not mentioned. Four studies reported elevated ALP. Four studies reported elevated blood bilirubin, of which one study examined only grade ⩾3 elevations because data on all grades of elevations were not mentioned. Four studies reported elevated GGT, of which only one study examined all grades because data on grade ⩾3 elevations were not mentioned. RC-48 was not evaluated in this study because hepatotoxicity was not reported in the available studies.

Flow diagram of included studies.
Number of antibody–drug conjugate-related hepatotoxicity in all studies included in this meta-analysis.

Includes the number of patients treated in antibody–drug conjugate arms but does not include patients treated in the control arms without antibody–drug conjugate.
The number of hepatotoxicity contains the number of ALT and AST.
ALT, alanine aminotransferase; AST, aspartate aminotransferase; AT-DM1, trastuzumab emtansine; SG, sacituzumab govitecan; T-DXd, trastuzumab deruxtecan.
Incidence of ALT elevation caused by ADCs in breast cancer
The overall incidence of all grades of ALT elevation caused by ADCs was 21.53% (95% CI: 16.09–27.50; Figure 2(a)). The incidence of all grades of ALT elevations caused by T-DM1, T-Dxd, and SG was 20.88% (95% CI: 14.65–27.86; Figure 3(a)), 19.96% (95% CI: 14.90–25.52; Figure 4(a)), and 25.30% (95% CI: 19.29–31.82; Figure 5(a)), respectively. The incidence of grade ⩾3 ALT elevation caused by ADCs was 2.68% (95% CI: 1.54–4.06; Figure 2(b)) and that caused by T-DM1 was 3.42% (95% CI: 1.95–5.24; Figure 3(b)). T-Dxd caused grade ⩾3 ALT elevations in 0.30 (95% CI: 0.00–2.08; Figure 4(b)), and SG caused grade ⩾3 ALT elevations in 1.50% (95% CI: 0.10–3.98; Figure 5(b)). Among all grades, SG caused the highest incidence of ALT elevation, whereas among grade ⩾3 ALT elevations, T-DM1 caused the highest incidence of ALT elevation.

Forest plot of the incidence of ALT elevation in ADCs in breast cancer patients. (a) Incidence of all grades of ALT elevation in ADCs in the treatment of breast cancer and (b) incidence of grade 3–5 of ALT elevation during ADCs in the treatment of breast cancer.

Forest plot of the incidence of ALT elevation in T-DM1 in breast cancer patients. (a) Incidence of all grades of ALT elevation in T-DM1 in the treatment of breast cancer and (b) incidence of grade 3–5 of ALT elevation during T-DM1 in the treatment of breast cancer.
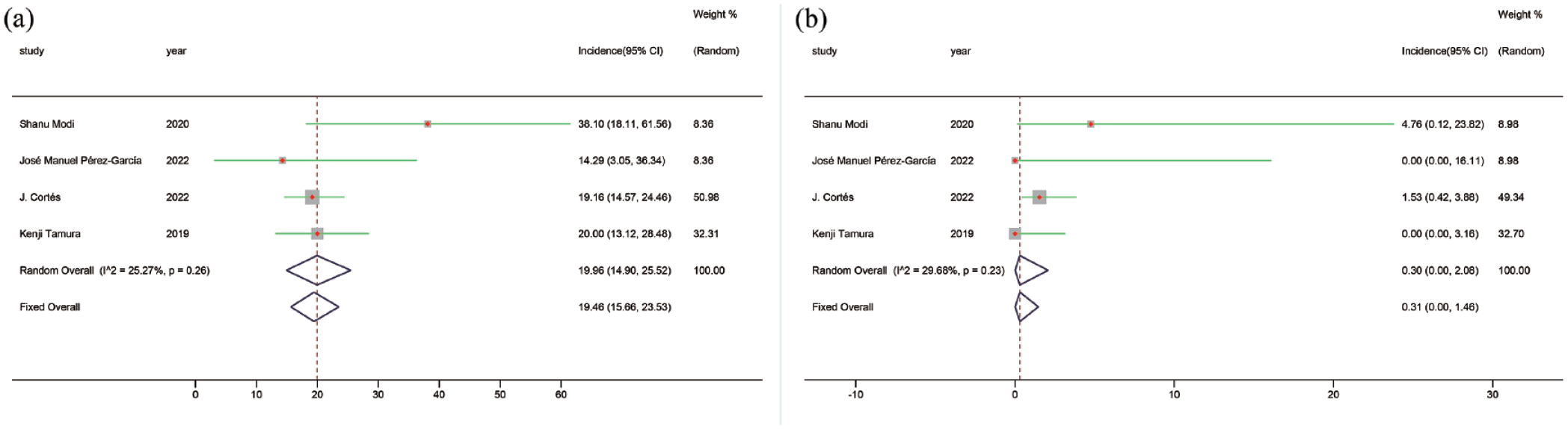
Forest plot of the incidence of ALT elevation in T-Dxd in breast cancer patients. (a) Incidence of all grades of ALT elevation in T-Dxd in the treatment of breast cancer and (b) incidence of grade 3–5 of ALT elevation during T-Dxd in the treatment of breast cancer.

Forest plot of the incidence of ALT elevation in SG in breast cancer patients. (a) Incidence of all grades of ALT elevation in SG in the treatment of breast cancer and (b) incidence of grade 3–5 of ALT elevation during SG in the treatment of breast cancer.
Incidence of AST elevation caused by ADCs in breast cancer
The overall incidence of all grades of AST elevation caused by ADCs was 24.17% (95% CI: 17.58–31.43; Figure 6(a)). The incidence of all grades of AST elevation caused by T-DM1 was 24.17% (95% CI: 17.58–31.43; Figure 7(a)). The incidence of all grades of AST elevation caused by T-Dxd was 31.89% (95% CI: 18.56–46.85; Figure 8(a)), and the incidence of all grades of AST elevation caused by SG was 20.19% (95% CI: 14.69–26.29; Figure 9(a)). The overall incidence of grade ⩾3 AST elevation caused by ADCs was 3.27% (95% CI: 2.06–4.69; Figure 6(b)), and the incidence of grade ⩾3 AST elevation caused by T-DM1 was 3.95 (95% CI: 2.39–5.85; Figure 7(b)). The incidence of grade ⩾3 AST elevation caused by T-Dxd was 1.76 (95% CI: 0.00–6.86; Figure 8(b)), and the incidence of grade ⩾3 AST elevation caused by SG was 1.05% (95% CI: 0.00–3.28; Figure 9(b)). Among all grades, T-Dxd caused the highest incidence of AST elevation, whereas, among grade ⩾3 AST elevations, T-DM1 caused the highest incidence of AST elevation.

Forest plot of the incidence of AST elevation in ADCs in breast cancer patients. (a) Incidence of all grades of AST elevation in ADCs in the treatment of breast cancer and (b) incidence of grade 3–5 of AST elevation during ADCs in the treatment of breast cancer.

Forest plot of the incidence of AST elevation in T-DM1 in breast cancer patients. (a) Incidence of all grades of AST elevation in T-DM1 in the treatment of breast cancer and (b) incidence of grade 3–5 of AST elevation during T-DM1 in the treatment of breast cancer.

Forest plot of the incidence of AST elevation in T-Dxd in breast cancer patients. (a) Incidence of all grades of AST elevation in T-Dxd in the treatment of breast cancer and (b) incidence of grade 3–5 of AST elevation during T-Dxd in the treatment of breast cancer.
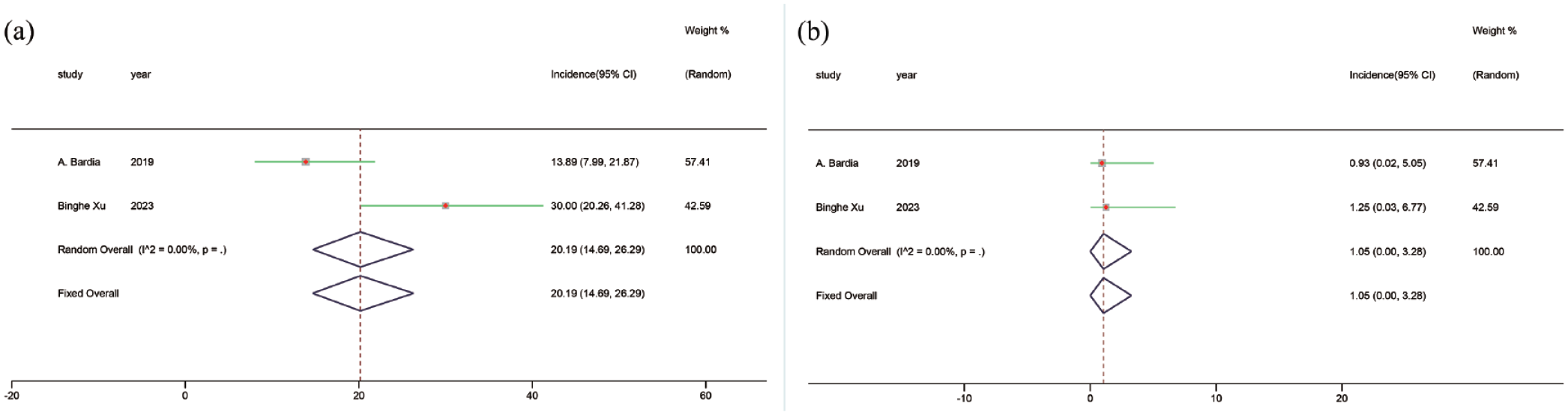
Forest plot of the incidence of AST elevation in SG in breast cancer patients. (a) Incidence of all grades of AST elevation in SG in the treatment of breast cancer and (b) incidence of grade 3–5 of AST elevation during SG in the treatment of breast cancer.
Incidence of ALP elevation caused by ADCs in breast cancer
The overall incidence of all grades of ALP elevation caused by ADCs was 10.87% (95% CI: 6.16–16.62; Figure 10(a)), and the overall incidence of grade ⩾3 ALP elevation caused by ADCs was 1.68% (95% CI: 0.48–3.41; Figure 10(b)).

Forest plot of the incidence of ALP elevation in ADCs in breast cancer patients. (a) Incidence of all grades of ALP elevation in ADCs in the treatment of breast cancer and (b) incidence of grade 3–5 of ALP elevation during ADCs in the treatment of breast cancer.
Incidence of blood bilirubin elevation caused by ADCs in breast cancer
The overall incidence of all grades of blood bilirubin elevation caused by ADCs was 3.76% (95% CI: 0.83–8.09; Figure 11(a)), and the overall incidence of grade ⩾3 blood bilirubin elevation caused by ADCs was 0.63% (95% CI: 0.00–5.16; Figure 11(b)).

Forest plot of the incidence of Blood bilirubin elevation in ADCs in breast cancer patients. (a) Incidence of all grades of blood bilirubin elevation in ADCs in the treatment of breast cancer and (b) incidence of grade 3–5 of blood bilirubin elevation during ADCs in the treatment of breast cancer.
Incidence of GGT elevation caused by ADCs in breast cancer
The overall incidence of all grades of GGT elevation caused by ADCs was 5.86% (95% CI: 2.26–10.87; Figure 12(a)), and the overall incidence of grade ⩾3 GGT elevation caused by ADCs was 2.44% (95% CI: 0.72–4.99; Figure 12(b)).

Forest plot of the incidence of GGT elevation in ADCs in breast cancer patients. (a) Incidence of all grades of GGT elevation in ADCs in the treatment of breast cancer and (b) incidence of grade 3–5 of GGT elevation during ADCs in the treatment of breast cancer.
Assessment of the included studies
The results of the quality assessment revealed that the included randomized controlled trials were of essentially low risk (Supplemental Figure 13). The results of the nonrandomized clinical trials assessed using the MINORS criteria were all of high quality (Supplemental Table 2). Significant publication bias was observed in all data (Supplemental Figure 14), and funnel plots were used to depict publication bias (Supplemental Figure 15).
Discussion
ADCs are widely used in clinical practice due to their ability to target and kill tumor cells; however, the toxic side effects of ADCs should not be underestimated. Hepatotoxicity is a side effect of ADCs, which mainly manifests due to abnormalities in serum ALT, AST, and other laboratory indicators and is of great concern in clinical treatment. 41 The ADC gemtuzumab (GO) was withdrawn from the US market in 2010 due to significant hepatotoxicity 42 ; therefore, we investigated the hepatotoxicity induced by ADCs in patients with breast cancer.
In this study, we performed a meta-analysis to systematically evaluate the hepatotoxicity produced by different ADCs in patients with breast cancer. To the best of our knowledge, this is the first meta-analysis to compare the incidence of elevation of different indices of liver function caused by different ADCs in patients with breast cancer. With the increasing use of ADCs in the clinic, the results of this meta-analysis may ADC developers and clinicians in detecting and treating hepatotoxicity experienced during ADC administration ADCs in patients with breast cancer.
The possible mechanisms by which ADCs cause hepatotoxicity are as follows: (1) normal cells express low levels of target antigens that may lead to specific toxicity; (2) early cleaved antibody–drug linkers in somatic circulation cause premature loss of small molecules before internalization in the ADC target cells, leading to off-target toxicity caused by nonspecific drug release; (3) ADC drugs have a bystander effect, whereby the free payload of the ADC may enter the target antigen-negative cells via passive diffusion, transporter protein-mediated uptake, or other nonspecific endocytosis mechanisms to cause cytotoxicity; (4) nonspecific endocytosis induces ADC uptake into healthy hepatocytes leading to the generation of cytotoxicity; and (5) receptor-mediated uptake is induced, whereby the receptor mediates target-independent internalization of the drug by normal cells by recognizing the Fc region of the IgG skeleton in ADCs.43,44 Our results showed that the overall incidence of all grades of ADC-induced ALT elevation and grade ⩾3 ADC-induced ALT elevation was 21.53% (95% CI: 16.09–27.50) and 2.68% (95% CI: 1.54–4.06), respectively. The overall incidence of all grades of ADC-induced AST elevation and grade ⩾3 AST elevation was 24.95% (95% CI: 19.17–31.21) and 3.27 (95% CI: 2.06–4.69).The overall incidence of all grades of ADC-induced ALP elevation was 10.87% (95% CI: 6.16–16.62), and that of grade ⩾3 ALP elevation was 1.68 (95% CI: 0.48–3.41). The overall incidence of all grades of ADC-induced blood bilirubin elevation was 3.76% (95% CI: 0.83–8.09), and the overall incidence of grade ⩾3 blood bilirubin elevation induced by ADCs was 0.63% (95% CI: 0.00–5.16). The overall incidence of all grades of ADC-induced GGT elevation was 5.86% (95% CI: 2.26–10.87), and the overall incidence of grade ⩾3 GGT elevation caused by ADCs was 2.44% (95% CI: 0.72–4.99). Pan Ma’s study concluded that elevated serum concentrations of AST (4.3%) and ALT (2.9%) were the most common grade 3 or 4 AEs reported in patients using T-DM1. 45 Second, a higher risk of elevated ALT and AST was also noted with ADC use in Yukio Suzuki’s study. 46 These results suggest that the incidence of serious hepatotoxicity caused by ADCs is low. The incidence of ALT and AST elevations was higher than that of other parameters, probably owing to the high sensitivity and responsiveness of ALT and AST to hepatocellular damage. The incidence of all grades of ALT elevation caused by SG was 25.30% (95% CI: 19.29–31.82), which was the highest incidence of all grades of ALT elevation. This may be related to the monoclonal antibodies hRS7IgG1κ and SN-38. SG is a novel ADC in which the CL2A linker connects the monoclonal antibody hRS7IgG1κ to the payload SN-38 by chemical coupling. The monoclonal antibody hRS7IgG1κ has potent antibody-dependent cell-mediated cytotoxicity. The bystander effect of SG is powerful because of the cleavability and moderate stability of the linker CL2A. Furthermore, SN-38, the active metabolite of irinotecan, showed stronger cytotoxicity than irinotecan in vitro and has become a more cytotoxic small-molecule drug in ADC studies.47,48 Moreover, among grade ⩾3 AST and ALT elevations, T-DM1 caused the highest incidence, with the incidence of 3.95% (95% CI: 2.39–5.85) and 3.42% (95% CI: 1.95–5.24), respectively. In Zhiwen Fu’s study, it was mentioned that among the most common grade ⩾3 adverse events in T-DM1 treatment, the incidence of AST elevation was 4.3%, while the incidence of ALT elevation was 2.9%. 49 In addition, in Kuan Liu’s study, it was mentioned that the incidence of ALT elevation was 2.6% and the incidence of AST elevation was 3.4% in breast cancer patients treated with T-DM1. 12 Serious hepatotoxicity of T-DM1 was observed in all these studies. Furthermore, T-DM1 increased ALP, blood bilirubin, and GGT. T-DM1-induced hepatotoxicity is mentioned in the black box warning issued by the Food and Drug Administration, and the underlying mechanism for hepatotoxicity may be related to its nonspecific activity. DM1 is a cytotoxic drug mertansine A derivative of, which acts through the enzyme cytochrome P4503A4/5 (CYP3A4/5) pathway for hepatic metabolism. Cytoskeleton-associated protein 5 may be a new target for T-DM1-induced hepatotoxicity, as their interaction on the hepatocyte surface induces cell membrane damage, inward calcium currents, and microtubule network dysfunction. 50 The European Association for the Study of the Liver (EASL) guidelines and the American College of Gastroenterology (ACG) guidelines state that liver function should be monitored prior to initiating T-DM1 therapy and before each subsequent dose. The dosage of the drug should be adjusted or the treatment should be discontinued in a timely manner based on changes in laboratory findings, such as liver enzymes and bilirubin levels, as well as liver imaging and, if necessary, histopathological examination.51,52. T-Dxd caused the highest incidence of all grades of AST elevation, with a prevalence of 31.89% (95% CI: 18.56–46.85). AST is mainly distributed in hepatic mitochondria, and its elevation indicates more severe hepatocyte injury. Compared with the molecular design of T-DM1, T-Dxd has made a breakthrough and innovation in the junction-payload system. Using protease-cleavable junctions, more efficient payloads, and higher drug-antibody ratios, T-Dxd can trigger a strong bystander effect and improve anticancer efficacy. However, its strong bystander effect may result in higher toxic side effects, 53 which may account for the highest incidence of AST elevation at all levels.
It is known from our study that hepatotoxicity due to ADCs is common. Discontinuation and dose reduction due to hepatotoxicity also occur frequently, which can significantly affect the drug’s efficacy and the patient’s prognosis. Hepatotoxicity is initially manifested clinically by abnormalities in laboratory tests such as ALT and AST, which can lead to sinusoidal obstruction syndrome or veno-occlusive disease.10,54,55 Therefore, when ADC drugs are used in the clinic, liver function should be closely monitored. The degree of liver injury should be promptly assessed when abnormal liver function-related laboratory test results occur, and imaging tests or even liver histology should be performed when necessary. If any of the following conditions occur, ADC drugs should be discontinued promptly, and the dose can be reduced if the primary disease necessitates treatment and there are no other alternative options: (1) ALT or AST >8 × ULN (upper limit of normal value); (2) ALT or AST >5 × ULN, lasting for 2 weeks; (3) ALT or AST >3 × ULN with TBil >2 × ULN or INR (International Normalized Ratio) >1.5; and (4) ALT or AST >3 × ULN with a gradual worsening of fatigue and gastrointestinal symptoms. In addition, for patients with acute liver injury characterized by markedly elevated ALT and other indicators, hepatoprotective drugs such as glycyrrhizic acid preparations and ursodeoxycholic acid tablets are recommended for routine hepatoprotective treatment. The prognosis for drug-induced hepatotoxicity is generally good, with gradual recovery achievable after discontinuation of the drug.56,57
Although the hepatotoxicity of ADCs should not be underestimated, their efficacy is far more significant. The DESTINY-Breast03 trial demonstrated a median PFS of 25.1 months for T-Dxd compared to 7.2 months for T-DM1. T-Dxd showed sustained PFS benefits compared to T-DM1. The median OS was 52.6 months for T-Dxd and 42.7 months for T-DM1, and T-Dxd significantly reduced the risk of death. 36 In the IMMU-132 study, the median PFS for SG was 6 months, while the median OS was 16.6 months. 40 Based on the current study, among the three ADCs, T-Dxd demonstrates better overall efficacy than T-DM1, with SG being the least effective. Therefore, when using three drugs in clinical settings, a comprehensive evaluation is essential. While ensuring efficacy, we must also consider safety issues. According to our study’s conclusions, when taking hepatotoxicity into account, T-Dxd may be the preferred drug for breast cancer patients with pre-existing liver disease. However, decisions should be made comprehensively and adjusted according to the patient’s condition when appropriate.
However, this study has some limitations. First, clinical trials on SG were fewer than those on T-DM1 and T-Dxd, which may have led to biased results. Second, RC-48 has not been frequently used in breast cancer treatment, and no clinical trials on its hepatotoxicity have been conducted. Third, most trials in our study were nonrandomized controlled studies, which might have led to a more pronounced publication bias. In addition to this, most of the current clinical studies on ADCs are based on reporting changes in serologic indices such as ALT and AST, and few studies have reported the effects of ADCs on the liver in terms of imaging tests or liver puncture biopsy. Therefore, our study lacks comprehensiveness. In future studies, the effects of ADCs on the liver can be comprehensively evaluated by combining serologic indexes, imaging examinations, and liver biopsies.
Conclusion
In this study, we concluded that the overall incidence of hepatotoxicity caused by ADCs used to treat breast cancer was high. SG resulted in the highest incidence of ALT elevation in all grades compared with other ADCs. T-Dxd caused the highest incidence of all grades of AST elevation. T-DM1 resulted in the highest incidence of either AST or ALT elevation. Therefore, when considering hepatotoxicity, T-Dxd is the preferred drug among the three ADCs. In addition, our results suggest that clinicians should closely monitor the liver function of breast cancer patients receiving ADCs and promptly assess the degree of liver injury in patients who develop abnormal liver function indices. If necessary, dosage reduction or discontinuation of the drug should be considered. For patients with acute liver injury, hepatoprotective agents should be used to minimize the effects of ADCs on the liver.
Supplemental Material
sj-docx-1-taw-10.1177_20420986241304680 – Supplemental material for Incidence of antibody–drug conjugate-related hepatotoxicity in breast cancer: a systematic review and meta-analysis
Supplemental material, sj-docx-1-taw-10.1177_20420986241304680 for Incidence of antibody–drug conjugate-related hepatotoxicity in breast cancer: a systematic review and meta-analysis by Ping Yang, Hengheng Zhang, Jinming Li, Zitao Li, Zhen Liu, Miaozhou Wang, Fuxing Zhao, Jiuda Zhao, GuoShuang Shen and Yi Zhao in Therapeutic Advances in Drug Safety
Supplemental Material
sj-docx-2-taw-10.1177_20420986241304680 – Supplemental material for Incidence of antibody–drug conjugate-related hepatotoxicity in breast cancer: a systematic review and meta-analysis
Supplemental material, sj-docx-2-taw-10.1177_20420986241304680 for Incidence of antibody–drug conjugate-related hepatotoxicity in breast cancer: a systematic review and meta-analysis by Ping Yang, Hengheng Zhang, Jinming Li, Zitao Li, Zhen Liu, Miaozhou Wang, Fuxing Zhao, Jiuda Zhao, GuoShuang Shen and Yi Zhao in Therapeutic Advances in Drug Safety
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.