
Abstract
Background:
The perioperative arena is a unique and challenging environment that requires coordination of the complex processes and involvement of the entire care team. Pharmacists’ scope of practice has been evolving to be patient-centered and to expand to variety of settings including perioperative settings.
Objectives:
To critically appraise, synthesize, and present the available evidence of the characteristics and impact of pharmacist-led interventions on clinically important outcomes in the perioperative settings.
Design:
A systematic review and meta-analysis.
Methods:
We searched PubMed, Embase, and CINAHL from index inception to September 2023. Included studies compared the effectiveness of pharmacist-led interventions on clinically important outcomes (e.g. length of stay, readmission) compared to usual care in perioperative settings. Two independent reviewers extracted the data using the DEPICT-2 (Descriptive Elements of Pharmacist Intervention Characterization Tool) and undertook quality assessment using the Crowe Critical Appraisal (CCAT). A random-effect model was used to estimate the overall effect [odds ratio (OR) for dichotomous and standard mean difference (SMD) for continuous data] with 95% confidence intervals (CIs).
Results:
Twenty-five studies were eligible, 20 (80%) had uncontrolled study design. Most interventions were multicomponent and continuous over the perioperative period. The intervention components included clinical pharmacy services (e.g. medication management/optimization, medication reconciliation, discharge counseling) and education of healthcare professionals. While some studies provided a minor description in regards to the intervention development and processes, only one study reported a theoretical underpinning to intervention development. Pooled analyses showed a significant impact of pharmacist care compared to usual care on length of stay (11 studies; SMD −0.09; 95% CI −0.49 to −0.15) and all-cause readmissions (8 studies; OR 0.60; 95% CI 0.39–0.91). The majority of included studies (n = 21; 84%) were of moderate quality.
Conclusion:
Pharmacist-led interventions are effective at improving clinically important outcomes in the perioperative setting; however, most studies were of moderate quality. Studies lacked the utilization of theory to develop interventions; therefore, it is not clear whether theory-derived interventions are more effective than those without a theoretical element. Future research should prioritize the development and evaluation of multifaceted theory-informed pharmacist interventions that target the whole surgical care pathway.
Plain language summary
Why was the study done? The time around the surgery imposes significant risks to patient’s health. While technical aspects of a procedure are important, it should be combined with the provision of optimal healthcare quality to increase the likelihood of desired clinical outcomes. Pharmacists are effective healthcare team members who have the potential to improve patient’s outcomes in the perioperative settings. It is hence imperative to explore the roles and impact of clinical pharmacists in these settings. Thus far, there is no synthesis of literature regarding the pharmacist roles and effectiveness in the perioperative setting. What did the researchers do? We aimed to summarize and appraise the quality of evidence on the characteristics and impact of pharmacist activities on clinical outcomes in the perioperative settings. Three library databases were examined to identify studies eligible for inclusion. Two authors extracted data and assessed the quality of included studies. Statistical analysis was used to look at the success of the pharmacist interventions on different endpoints. What did the researchers find? A total of 25 studies were included. Most pharmacist activities consisted of multiple components (such as medication management and educating other healthcare providers) and spanned the whole perioperative journey. The analysis of included studies showed that pharmacist activities reduced the elapsed time in hospital and the number of times a patient winds up going back to a hospital after discharge. Most studies did not discuss the methods adopted to develop pharmacist activities. What do the findings mean? A number of pharmacist activity types were shown to be successful in reducing the duration of hospitalization and readmission episodes. New directions for future research should investigate the development of pharmacist-led interventions in terms of structure and processes to ensure the reproducibility of these interventions.
Keywords
Introduction
The perioperative period is defined as the time lapse surrounding the surgical act which can be subdivided into three stages: preoperative, intraoperative, and postoperative.1,2 The perioperative environment is known to be one of the most complex and challenging areas within a hospital with significant safety risks. 3 Studies showed that half of all adverse events in hospitals occur in perioperative settings.4,5 Therefore, the World Health Organization launched the campaign ‘Safe Surgery Saves Lives’ in 2008 which aims to improve the safety of surgical procedures and implement patient safety best practices to reduce the incidence of adverse events both in the operating room and in the ward. 6 For decades, the objective of safe surgery was centered on technical procedures. However, there is emerging evidence that improving access to surgical healthcare alone does not result in improved health outcomes unless it is coupled with quality perioperative care. 7 Thus, in recent years, much attention has been devoted to the empowerment of nontechnical skills and interpersonal communication which contribute to the improvement of patient-centered quality metrics and subsequently to reducing harm in perioperative settings.1,6
Multidisciplinary teams have been proposed as an effective approach to enhance the quality and safety of care in perioperative settings and to reinforce the importance of patient-centeredness. 3 While the roles and outcomes of most healthcare providers in these settings are well established in the literature, the roles and impact of pharmacist integration into perioperative settings is seldom examined.8–10 Over the past few decades, the scope of practice for pharmacists has been evolving, which enabled them to embrace new roles in a variety of settings. Pharmacists’ expanded professional role includes variety of activities such as medication reviews, medication therapy management, patient counseling, independent prescribing, telepharmacy services, vaccine dissemination, community education, and emergency preparedness and response.11–13 The American Society of Health-System Pharmacists highlighted the greater demand for increased pharmacy involvement in the perioperative medication-use process by incorporating additional activities. 14 Clinical pharmacists could have unique roles in the perioperative settings owing to their advanced therapeutic knowledge and experience which make them well poised to add value to emergency response efforts as paralleled in other settings.14,15 This could potentially lead to a significant improvement to patient care in terms of both efficacy and safety. 15
Outcome indicators are increasingly used in quality measurement programs in various countries to monitor and compare hospital performance, with the aim of identifying areas for improvement. Three outcome measures that are frequently used to evaluate quality of care in hospitals are in-hospital mortality, readmission rate, and length of stay (LOS).16–18 LOS is considered a pivotal clinical outcome metric used as a proxy of efficient hospital and healthcare systems management. Prolonged LOS not only decreases reimbursement margins but is also associated with negative patient and staff experience, as well as increased inpatient complications (e.g. falls, adverse drug events, hospital-acquired infections).19–22 Similarly, decreasing the rate of hospital readmissions has been targeted as a high priority for hospitals across the globe, hastened by implementation of public reporting and financial penalties for excess readmissions.23,24 Furthermore, to obtain a comprehensive picture of quality, it is attractive to jointly report outcome measures to ensure consistent improvement in all outcomes of interest. For instance, mortality may be very low in some patient groups but readmission rate is high. 25
It is hence imperative to explore the roles and impact of pharmacists on these clinical outcomes in perioperative settings. This systematic review and meta-analysis aimed to critically appraise, synthesize, and present the available evidence of the characteristics and impact of pharmacist-led interventions on clinically important outcomes in the perioperative settings.
Methods
This systematic review and meta-analysis was conducted utilizing the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guideline (Supplemental Materials 2, see ESM) 26 and is registered prospectively in the International Prospective Register of Systematic reviews (PROSPERO): (CRD42023460812).
Literature search
We searched the following databases from index inception until September 2023: PubMed, Embase, CINAHL, and Google Scholar. The literature search was carried out using natural language keywords and, where applicable, MeSH terms and EMTREE (controlled vocabulary thesaurus) for data search in PubMed and Embase, respectively. Each database was searched using variants of keywords such as pharmacist, pharmacy, pharmaceutical care, perioperative period, perioperative care, surgery, and procedure (Supplemental Materials 1, see ESM). The reference lists of included studies were manually reviewed to search for any additional studies.
Types of studies and eligibility criteria
Studies were included if they were (1) randomized controlled trials (RCTs), quasi-experimental, pre-post-, prospective, and retrospective cohort; (2) evaluated a clinical pharmacist-led intervention; (3) conducted in the perioperative period; (4) had a control or comparison group (with healthcare professionals other than a pharmacist); (5) measured any of the following clinically important endpoints [LOS, readmission, mortality, emergency department (ED) visits, unplanned outpatient visits, any healthcare encounter]; (6) published in a peer-reviewed journal in English or Arabic languages and available in full text. Case reports, expert opinions, systematic reviews, letters to editors, commentaries, correspondences, news articles, and qualitative studies were excluded from this review, as were conference abstracts if not available in full text. We also excluded studies focusing on pediatric patients.
Study selection
The articles found in the database search were transferred to Rayyan, a web application for systematic reviews, to identify and delete any duplicated articles. 27 Two authors (LN, SK) independently screened the titles and abstracts of all retrieved studies. Then, full-text screening of each potentially eligible study was independently done by two reviewers (LN and SK or BA and MA), and discrepancies were resolved through consensus. If the difference remained unresolved, a third reviewer adjudicated to reach a predefined consensus.
Data extraction
A bespoke data extraction tool was developed based on the Descriptive Elements of Pharmacist Intervention Characterization Tool (DEPICT-2). 28 DEPICT-2 is a validated instrument for accurately describing and characterizing the details of pharmacist interventions. The tool consists of 93 items, subsumed into 11 domains: contact with recipient, setting, target population, clinical data sources, variables assessed, pharmacist intervention, timing of intervention, material that support intervention, repetition, communication with recipient, and changes in therapy and laboratory tests. 28 The final data extraction sheet included the following components:
General information: author(s), year, country, study design, objectives, population, sample size, study duration, and surgical unit(s).
Description of intervention: recipients, focus of intervention, setting, method of communication, clinical data source, pharmacist action, timing and frequency of action, and materials that support action.
Key findings.
The final data extraction sheet was piloted on four studies prior to its use. An independent, duplicate data extraction of each study was undertaken (LN, SK, MA, or BA).
Quality assessment
Quality assessment of the selected articles was undertaken by independent reviewers working in pairs (LN, SK, MA, or BA) using the validated Crowe Critical Appraisal tool (CCAT) version 1.4. 29 The CCAT contains 22 items grouped into 8 categories and is applicable to all study designs, with the highest possible score being 40. The tool helps in recording scores for each category so that the final score is not influenced by an overall opinion about the study. The quality of studies was categorized as follows: high quality (36 and above), moderate quality (30–35), and low quality (29 and below). This was based on a consensus reached by the reviewers to group studies by quartiles, a similar approach adopted by Donnelly et al. 30 and El-Awaisi et al. 31 The author of the CCAT tool was also contacted to ensure that this method of interpretation was valid.
Outcome measures
Impact of clinical pharmacist interventions on clinically important outcomes in the perioperative setting was the primary measure of interest identified in included studies. Clinically important outcomes include any of the following endpoints: LOS, readmission, mortality, ED visits, unplanned outpatient visits, and any healthcare encounter.
The secondary outcome was to describe the adopted clinical pharmacist interventions in accordance with the DEPICT-2 tool to assess the following domains: target population, setting where the intervention took place, contact with recipients, pharmacist activities, source of guide for the intervention, and materials that support intervention.
Data analysis
Our analysis included studies that reported at least one of the following clinically important outcomes: healthcare utilization (LOS, readmission, mortality, ED visit, and any healthcare encounter) and mortality compared with usual care. Where adequate data for the meta-analysis were reported, the odds ratios (ORs) for dichotomous outcomes or standard mean differences (SMDs) for continuous outcomes, both with 95% confidence intervals (CIs) and two-sided p values for each outcome, were derived. Statistical heterogeneity between studies was quantified using the Chi-squared test and the I2 statistic. A random-effects model was used to calculate the pooled effect estimate for outcomes as heterogeneity (I2 > 50%) was expected due to the variation in the interventions and patient populations. We evaluated publication bias by inspection of funnel plot and Egger’s regression test. In all analyses, significance was established at values of p < 0.05. Data analyses were performed using IBM Statistical Package for Social Sciences (IBM SPSS Statistics, Version 29.0; IBM Corp, Armonk, NY, USA).
Results
Search results and study selection
A total of 6816 potential articles were identified from searches in the electronic databases, and 8 additional records were identified in reference lists of included studies (Figure 1). Of these, 115 were reviewed in full text, and 25 were included.

PRISMA chart describing study retrieval and selection.
Description of included studies
Countries and surgical departments
The majority of studies were conducted in the United States (n = 9; 36%)32–40 and China (n = 9; 36%),41–49 followed by the United Kingdom (n = 3; 12%),50–52 and one (4%) each in Australia, 53 Netherland, 54 Pakistan, 55 and Sudan 56 (Table 1). Most of the studies (n = 8; 32%) were carried out in orthopedic surgery,35,37,38,41,44,47,49,52 followed by five (20%) studies each that included multiple units43,53–56 and general surgery39,42,46,50,51 (Table 1). Three studies (12%) were conducted in bariatric surgical units,33,34,40 and two (8%) each in cardiothoracic36,48 and transplant units.32,45 The majority of studies were published in 2019 onward, except for one each in 2015, 54 2016, 48 and 2018. 38
Characteristics of included studies.

ASA, American Society of Anesthesiologists; BLA, beta-lactam allergy; CI, confidence interval; CPGT, clinical pharmacist-led guidance team; ED, emergency department; EQ-5D EuroQOL-5 dimension questionnair; ESMOS, Enhanced Surgical Medicines Optimization Service; GI, gastrointestinal; HPB, hepato-pancreato-biliary; IQR, interquartile range; KPNW, Kaiser Permanente Northwest; LOS, length of stay; MED, morphine equivalent dose; PJI, periprosthetic joint infection; PONV, postoperative nausea and vomiting; PREP, PeRiopErative and Prescribing; QoL, quality of life; RCT, randomized controlled trial; RR, relative risk; RYGB, Roux-en-Y gastric bypass; SAP, surgical antimicrobial prophylaxis; SD, standard deviation; SG, sleeve gastrectomy; SMD, stndard mean difference; SUREPILL, Surgery and Pharmacy in Liaison; THR, total hip replacement; TJA, total joint arthroplasty; TKR, total knee replacement; UKR, unicompartmental knee replacement.
Study design
The majority of studies (n = 20; 80%) used an uncontrolled study design, 12 (48%) retrospective,32–34,37,39,41,42,45,46,49,51,52 5 (20%) prospective,35,36,43,50,55 3 (12%) retro-prospective studies,40,44,48 with a variety of observational methodological designs (Table 1). The remaining five (20%) were controlled, all of which were randomized.38,47,53,54,56 Follow-up duration among the included studies ranged from 9 days 52 to 36 months. 41
Study population
The studies’ sample sizes ranged between 65 47 and 1227 patients 35 (Table 1). Other than specifying one or more surgical units, the majority of studies (n = 13; 52%) focused on a particular class of medication including antibiotics (n = 5; 20%),36,48,49,55,56 analgesics (n = 3, two of which on opioids),37,38,44 and one each on anticoagulants, 41 antidiabetic drugs, 39 antiemetics, 43 proton pump inhibitor, 46 and total parenteral nutrition (TPN) 42 (Table 2). Among the reminder studies, two focused on patients with mild systemic disease50,51 and two on patients at higher risk for medication misadventures.38,53 One study included female patients only as they are at higher risk for postoperative nausea and vomiting 43 (Table 1).
Description of pharmacist intervention according to DEPICT version 2.

ACCP, American Association of Chest Physicians; ADR, adverse drug reaction; ARISE, Arthroplasty Rehabilitation in Scotland Endeavor; ASA, American Society of Anesthesiologist; BPMH, best possible medication history; CMS, Centers for Medicare & Medicaid Services; DEPICT, Descriptive Elements of Pharmacist Intervention Characterization Tool; GP, general practitioner; EMR, electronic medical record; ERAS, enhanced recovery after surgery; ESMOS, Enhanced Surgical Medicines Optimization Service; ESPEN, European Society for Clinical Nutrition and Metabolism; EUSEM, European Society for Emergency Medicine; MDT, multidisciplinary team; MRF, medication reconciliation form; N/A, not applicable; NHFPC, National Health and Family Planning Commission; NHS, National Health Service; PONV, postoperative nausea and vomiting; PPI, proton pomp inhibitor; PREP, PeRiopErative and Prescribing; SAP, surgical antimicrobial prophylaxis; TPN, total parenteral nutrition; VPN, Virtual Private Network; VTE, venous thromboembolism.
Description of pharmacist-led interventions
Table 2 and Figures 2 and 3 describe the pharmacist-led interventions in each study as described by DEPICT-2. 28

Stacked bar chart representing quality of included studies.

General characteristics of the interventions performed by the pharmacists.
Recipients of the intervention
Fourteen studies (56%) reported that patients were the target of the implemented pharmacist-delivered services,33–35,38–40,44,45,47,50–54 while seven studies (28%) reported that patients alongside medical staff were the recipient of the intervention.32,36,41,43,46,48,49 Four studies (16%) reported that the pharmacist intervention was intended for medical staff, mainly surgeons with or without other healthcare providers such as nurses or anesthesiologists.37,42,55,56
Setting where recipient received intervention
All studies, except for one, 39 reported the settings where the intervention took place. The intervention was delivered at hospital bedside in nine studies (36%),33,35,40,41,43–45,47,54 while another nine (36%) reported other settings alongside the hospital bedside such as hospital clinic, 32 recipient’s home,51,53 hospital in general (refers to interventions that included educational session),37,46,48 or a combination of them.49,50 Two studies (8%) only included educational initiatives and were conducted in the hospital,55,56 while one study included both delivering education in the hospital and interviewing patients in their homes. 36 Two interventions took place only at the recipient’s home38,52 and one in a hospital-based clinic. 34
Communication with recipients
Most interventions (n = 9; 36%) were conducted through one-on-one contacts with the patients either in the clinic or during the medication reconciliation process,33,34,40,47,50–54 while five interventions (20%) were contact with group which was mostly either clinical rounds or educational sessions.37,46,48,55,56 Eight interventions (32%) included a combination between one-on-one and contact with group.32,35,36,41,43–45,49 Smith et al. 38 reported that they provided one-on-one contact but only if needed, while Tong et al. 42 reported that there was no direct contact as the intervention was to develop TPN software. Only one study did not report the mode of contact with the recipients. 39
The method of communication was largely (n = 13; 52%) through face-to-face contacts with patients or other healthcare providers,33–35,37,40,41,43,45–47,54–56 while nine studies (36%) encompassed telephone,32,36,51,53 written contacts,44,48,49 or both50,52 beside the face-to-face communication. It is worth pointing out that the studies that used a combination method of contact was mainly through virtual contact with the patient before admission to reconcile the medications (as it might be too late to make necessary changes upon admission), followed by in-person contact after admission. Smith et al. 38 included written communication via mailed brochure and telephone if needed. Four studies did not involve direct contact with the patient as the intervention targeted healthcare providers37,42,55,56 and one study did not report whether there was a direct patient contact or not. 39
Of the 25 included studies, 14 (56%) demonstrated a continuous provision of the pharmacist services over the perioperative period,32,33,35,39,41,43,45–49,51,54,56 while nine (36%) studies reported that the frequency of contact was limited to a specific number of times (ranging from one to four times).34,36,38,40,44,50,52,53,55 Among the former, some studies (n = 6; 24%) reported that the services were only delivered on or during patient admission,38,43,45,46,48,56 while others reported that the intervention was initiated before admission (n = 1; 4%), 51 extended after discharge (n = 6; 24%),33,41,47,49,54 or both (n = 1; 4%).32,35 Among the latter, the timing of the pharmacist intervention was variable including delivery of services only preadmission,34,36 preadmission and on discharge,50,53 preadmission and postdischarge,38,52 preadmission, during admission (once each preoperatively and postoperatively) and on discharge, 44 and postoperative. 40 For studies that involved contacting the patient before admission, it was done 48 h to 2 weeks beforehand, whereas for studies that involved contacting the patient after discharge, it took place 7–15 days of discharge.
Pharmacist action(s)
Most studies conducted a multifaceted pharmacist-led intervention (Figure 3 and Table 2). This involved clinical pharmacy services during admission such as attending ward rounds, reviewing patient records, medication reconciliation, answering drug inquiries, and patient counseling. Additionally, some interventions incorporated medication reconciliation before admission by contacting the patient (in a physical or virtual clinic) or the patient’s general practitioner or community pharmacist as part of the patient preparation for the surgery. This could reduce discrepancies upon admission and allow the pharmacist to advise on holding/starting/adjusting medications in the appropriate timeframe as it could be too late if it was stopped on admission (e.g. anticoagulation medications should be stopped 3–7 days before surgery). Some interventions also incorporated follow-up appointment with the patient postdischarge in a virtual of physical clinic, this was particularly important in patients who underwent surgeries that might require long-term use of medications (e.g. transplant or cardiothoracic).
Other interventions comprised pharmacist-led structured educational programs (either alone or in addition to the clinical pharmacy services) delivered to various healthcare providers (mainly surgeon and nurses).36,37,41,46,48,49,55,56 Pharmacists also developed protocols (e.g. surgical antimicrobial prophylaxis) or TPN software to assist surgeons during their practice, in some of the studies the pharmacist was also responsible for implementing and ensuring that the protocols were accurately followed.36,37,42,56 Conducting internal audits and report findings was another intervention that emerged among the included studies, in which findings from the audit were utilized to provide individualized or group feedback. 48 Referral to other healthcare providers has also been identified among the included studies. 50 The level of detail regarding the development, structure, and processes of these interventions was limited.
Source of guide for intervention
Twenty out of the 25 included studies (80%) furnished some information on the basis for developing the implemented intervention (Table 2). The primary source of guide for the pharmacist-led interventions was clinical guidelines32,42,43,48,55 and institutional protocols.36,39,40,52,54 Along with the guidelines, some studies employed other sources such as drug instructions,41,46 expert consensus,33,44 or published official documents. 48 Three studies based the intervention on primary literature search.35,37,47 Bansal et al. 51 reported the use of the previously developed ‘Always Events’ toolkit. Smith et al. 38 reported that the brochures were developed by the research team using qualitative methods with input from patients and orthopedic surgeons, while the telephone calls were based on the motivational enhancement principles.
Materials that supported the intervention
Only nine studies (36%) reported that they utilized materials to support the intervention (Table 2). This mainly included forms/notes (whether impeded in the electronic medical record or not) to facilitate communication between healthcare providers,33,36,40,50,53 and brochures/handouts to patients38,44 or surgeons and nurses.48,49 One study used WeChat work groups to improve communication with patients. 44
Outcomes of the pharmacist-led interventions
Length of stay
Of the 21 studies that reported data on the inpatient LOS, only 11 reported adequate data for meta-analysis.32,39,41,43,44,46–49,52,55 These studies demonstrated a SMD (n = 4905 patients) favoring the pharmacist intervention group of −0.09 days (95% CI −0.49 to −0.15) with considerable heterogeneity (I2 = 86%, overall effect p = 0.0002) (Figure 4). There was no evidence of publication bias based on the symmetrical distribution of studies along the funnel plot’s null line and Egger’s regression test (p = 0.995) (Figure 5).

Forest plots of intervention effects on length of stay (LOS).

Funnel plot to assess the publication bias for studies assising phamacist impact on length of stay (LOS).
Among studies that were not included in the meta-analysis, only half of the studies showed significant decrease in the LOS.36,37,50,51,56 Studies that did not show statistical significance mainly shared one or more of the following factors: (1) the intervention comprised only one pharmacist service (mainly medication reconciliation); (2) the intervention was not continuous throughout the perioperative period; (3) there was a lack of preadmission contact with the patient to optimize drug therapy prior to admission.
All-cause readmission
Eight of nine studies that measured all-cause readmissions were pooled. Seven studies reported this outcome at 30 days,32,33,35,40,45,47,50 while one each reported at 3 and 6 months.49,54 Although only two studies showed statistically significant reductions in readmissions,33,35 the ORs and CIs for studies with higher weight were only marginally nonsignificant32,54; therefore, the overall effect was significant. The pooled analysis across all interventions (n = 3271 patients) showed some significant difference between the intervention and usual care (OR 0.60; 95% CI 0.39–0.91; Figure 6). Evidence showed moderate heterogeneity (I2 = 46%) in this outcome. The funnel plot revealed no marked asymmetry supported by Egger’s test value of 0.905; hence, no evidence of publication bias (Figure 7).
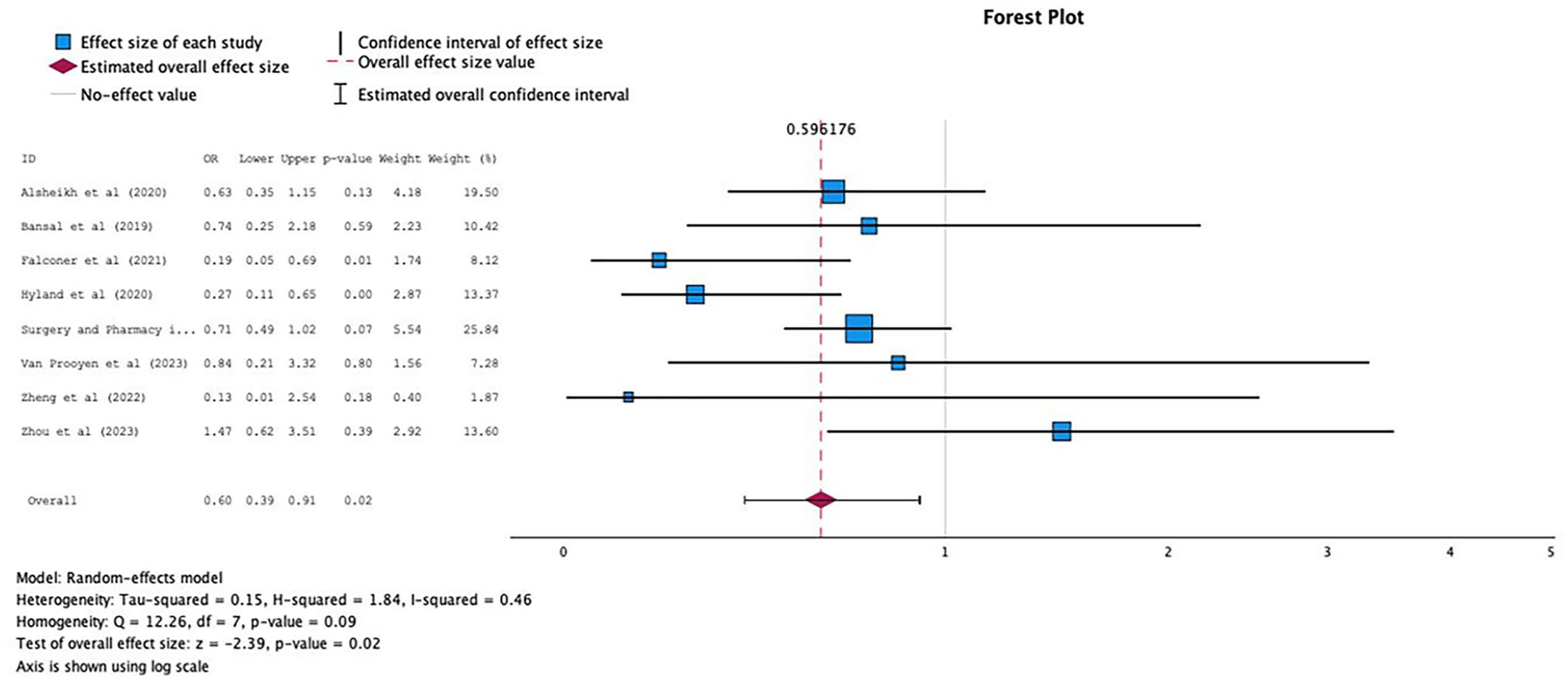
Forest plots of intervention effects on all-cause readmission.

Funnel plot to assess the publication bias for studies assising phamacist impact on all-cause readmission.
Only one study was not included in the meta-analysis. The readmissions in Yang et al. 45 were 0% in both groups at 7 and 30 days. Overall, studies that showed significance implemented a multicomponent continuous intervention that involved structured discharge counseling or postdischarge follow-ups.
Other clinically important outcomes
Only five studies investigated other clinically important outcomes, with one study exploring two endpoints of interests (Table 1).33,38,40,47,52 Three outcomes emerged from included studies which are physical or virtual (via phone calls or email) unplanned outpatient visits,33,38,47 ED visits,38,40 and any healthcare encounter. 52 None of the included studies examined the impact of pharmacist interventions on mortality.
Smith et al. 38 distributed educational brochures to patients without direct contact with the pharmacist, findings showed a slight increase in unplanned outpatient visits (face to face, telephone, or e-mail). Similarly, Falconer et al. 33 focused on patients undergoing bariatric surgery and showed a significant increase in outpatient medication-related phone calls from 31% to 39% (p = 0.04). 33 In contrast, Zheng et al. 47 included patients undergoing orthopedic surgeries and showed an insignificant decrease in unplanned outpatient visits within 30 days of discharge (p > 0.05). 47
While Van Prooyen et al. 40 showed a slight increase in ED visits within 30 days from 2.4% to 5.9% (p = 0.28), 40 Smith et al. 38 revealed an insignificant decline in the number of ED visits. A UK-based retrospective study that focused on orthopedic patients showed a significant decrease in 9-day any healthcare encounter (p = 0.03). 52
Quality of evidence
The scores ranged between 25 and 36, with a median score of 32.16. The review indicated that the majority of studies (n = 21; 84%) were of moderate quality, while three (12%) showed low quality, and one (4%) was identified as a high-quality article. The key limitations centered on sampling, data collection, and ethical matters (Figure 2).
Discussion
This systematic review and meta-analysis is the first to examine the effectiveness of pharmacist-led interventions in the perioperative settings on clinically important outcomes. It also provides a comprehensive summary of the characteristics of the pharmacist-provided interventions. It is evident from our systematic review that research focusing on the impact of pharmacist interventions during the perioperative period has been rapidly accelerating since the year 2019.
Healthcare resource utilization
This review has shown better outcomes in favor of pharmacist-provided interventions. We found a substantial reduction in the LOS (SMD −0.09 days; 95% CI −0.49 to −0.15) and all-cause readmissions (OR 0.60; 95% CI 0.39–0.91). Previous research showed mixed findings in relation to the impact of pharmacist-delivered services on the LOS. For example, two meta-analyses that implemented pharmacist-led medication reconciliation and medication-related interventions demonstrated no effect on the hospital LOS.57,58 Conversely, implementation of a ward-based pharmacist who performed multiple services shortened the LOS by (SMD −1.74 days; 95% CI −2.76 to −0.72). 59
Less variation has been noted among studies that explored the influence of pharmacist interventions on the readmission rate. In line with our findings, different pharmacist-led interventions have shown significant reduction in readmission rate in various settings and patient populations.57,59−62 However, most studies concluded that the quality of evidence is low and that there is lack of high-quality RCTs.
It also is important to note that some of the previously discussed studies showed improvement in one endpoint but not the other. Interventions have the potential to create trade-offs between outcomes. Reducing LOS might increase concerns for readmission risk or shifting costs of care to the outpatient setting.21,63 Nevertheless, new evidence suggests that there is no correlation between readmission rates and LOS rates.64,17 In fact, it was proposed that shorter LOS might be associated with lower readmission rate if the patients was not discharged prematurely, and if there was emphasis on ambulatory operations throughout this time and on easier access to outpatient appointments, especially within 7 days of discharge. 65 Therefore, evidence emerging from our review is pivotal as it confirms that pharmacist interventions in perioperative settings have positive impact on both LOS and readmission which highlights the importance for comprehensive multidimensional interventions that are continuous throughout the perioperative period.
Pooling data was infeasible for other relevant outcomes (unplanned outpatient visits, ED visits, and any healthcare encounter); however, findings from these studies were conflicting. Thus, at present, the strength of evidence is insufficient to reach firm conclusions on the role of pharmacist on these outcomes. It is worth noting that this kind of evaluations often requires larger sample sizes due to high variability. 66
Components of the pharmacist interventions
Most studies implemented multicomponent interventions including an array of clinical services (e.g. medication reconciliation, attending rounds, patient counseling) alongside other interventions such as education of health professionals, developing clinical pathways, and referral to other healthcare providers. Pharmaceutical care combined with education was the most common intervention strategy amongst included studies. This is consistent with a previous review focused on people living with HIV/AIDS. The study concluded that pharmacist care improves a wide range of clinical outcomes and that the most common intervention type in this setting is education combined with pharmaceutical care. 67 It hence is imperative to reinforce the importance of educational interventions as previous research highlighted that education has been integrated into each intervention strategy and is seen as a key to improving multiple clinical outcomes.68,69
Nevertheless, single component interventions (most commonly medicines reconciliation) were also relatively common in our review. Although we did not conduct a subgroup analysis, individual studies with multifactorial interventions showed a trend toward significance as compared to single component interventions. This finding is consistent with previous research suggesting that interventions consisting of intermingled components are associated with improvement in various medication safety and patient outcomes as compared to a single isolated intervention. For instance, a meta-analysis focusing on patients transitioning out of the intensive care unit showed that multicomponent interventions led to a fourfold reduction in deprescribing on hospital discharge as compared to twofold in the single component arm. 58 Similarly, another meta-analysis illustrated that various combinations of interventions were associated with lower risk of injurious falls compared with usual care in older adults. 70
While studies that focused on pharmaceutical care provided relatively sufficient details on the characteristics of the intervention, studies presenting other types of interventions provided a considerably varied level of details and was generally lacking which could hinder the reproducibility of these interventions. This long-standing issue has been extensively discussed in the literature.69,71–75 Therefore, our findings suggest that, to some extent, there is progress in characterizing pharmaceutical care interventions in recent years especially that most of the included studies are recent. Yet, describing other kinds of interventions is still lacking.
Timing and frequency of the pharmacist interventions
A small majority of the included studies employed a continuous intervention throughout the perioperative period. By looking at each individual study, it was evident that those studies mostly resulted in significant findings as opposed to studies that were limited in terms of timing or frequency.
Additionally, studies that showed a significant reduction in the LOS shared the fact that most of them incorporated a preadmission contact with the patient (mostly 1–2 weeks preadmission) to reconcile medications and optimize drug therapy prior to admission. Nonetheless, studies that only implemented a medication reconciliation program upon admission mostly did not yield any meaningful improvements. This contrasts with a previous meta-analysis that proved pharmacist-led medication reconciliation services as an effective standalone intervention. 57 This suggests a plausible temporal relation that is specific to the perioperative settings, between the reconciliation and its effectiveness. Patients who are scheduled for surgery are usually admitted 1 day before the surgery. 76 This means that the patients are not reviewed by a pharmacist until the day of admission for surgery. By this time, it is often too late to make any significant changes to perioperative drug management and on occasions patients may not be seen on the morning of scheduled surgery.
Similarly, studies that showed significance regarding the readmission rate generally implemented a continuous intervention that involved structured discharge counseling or postdischarge follow-ups. This substantiates previously published evidence that multicomponent interventions that involve high-quality discharge planning and structured planned postdischarge support decreases readmission rate.23,65,77,78 Notably, current literature also suggests that obtaining an accurate preadmission medication history have great potential to reduce harm, as they can propagate throughout a patient’s hospitalization and after discharge.23,79
Development of the pharmacist interventions
Our findings suggest a paucity of data from all included studies on the basis of the intervention development which could hamper the application of these interventions by other researchers and policymakers. Whilst it was noted that most reviews relied on local or international guidelines as the scientific basis for the development, no further details were provided. Furthermore, only one study reported a theory underpinning intervention development which was the motivational enhancement theory without any further detail on how it was applied. 38 There is an accumulation of evidence that theory-informed interventions are more likely to yield positive and sustainable outcomes compared to pragmatic approaches.72,80–82 Similarly, Glasgow and Linnan 83 suggest that the use of theory ‘results in more powerful interventions’. The absence of reporting on the theoretical underpinnings of the included interventions limited our commentary on its effectiveness. Moreover, reporting the impact of theory-driven interventions in this area remains unknown. It has also been explicated by Michie et al. 84 that even if the theory does not confer a positive effect on outcomes in favor of the intervention, it helps to clarify what does and does not work in an intervention.
Strengths and limitations
To the best of our knowledge, this is the first systematic review and meta-analysis to evaluate the available literature on the characteristics and impact of pharmacist interventions on clinically important outcomes in perioperative settings. The DEPICT-2 tool was used for systematic extraction and analysis of the intervention’s core components among included studies, which eliminated the rater effect and, hence, provided more consistency to our results. 28 The protocol was prospectively registered on PROSPERO.
There are some limitations. First, the study was limited to English and Arabic language publications; this may have excluded relevant references published in other languages. Second, included studies were restricted in terms of the sample size and follow-up duration which is required to detect the investigated outcomes comprehensively. Third, there was considerable heterogeneity in the data from the meta-analysis; however, this limitation is expected in multifactorial complex interventions. Fourth, although we searched Google Scholar to assist in locating nonindexed articles, using Google Scholar alone may not be sufficient. 85 Hence, there may be gray literature that was not identified in our search.
Future directions
Findings from our study suggest that multifaceted pharmacist-delivered interventions are promising in improving clinically important outcomes, primarily LOS and readmission, in perioperative settings. Therefore, developing and implementing interventions tailored specifically to these settings should be a policy and practice priority, being particularly pertinent to the complexity of surgical patients and the significant differences in the perioperative environment and infrastructure. Future research should therefore address the contextual factors (e.g. medication discrepancies, medication management perioperatively, unsafe discharge) contributing to negative outcomes across the whole surgical care pathway. 14
It is noteworthy that none of the included studies investigated the impact of pharmacist interventions on mortality even though mortality is considered an integral outcome measure to assess the quality and efficacy of hospitals and healthcare systems.16–18 We therefore encourage future researchers to consider investigating the effect of pharmacist-led interventions on mortality to have a holistic view of the pharmacist impact on clinical outcomes. We also encourage researchers to conduct a comprehensive cost assessment (e.g. cost-effectiveness analysis) of pharmacist-led interventions in the perioperative setting to inform evidence-based policy decisions. This will subsequently assist policymakers in developing targeted strategies and allocating resources.
The current study also highlighted the lack of theory-driven interventions. Thus, there is a need for several sufficiently powered randomized studies of a theoretically derived intervention aiming to improve clinical outcomes in the perioperative settings. The Medical Research Council Framework of Complex Interventions in the United Kingdom advises the use of theory and exploratory studies to identify barriers to change while developing complex interventions. 86 It is imperative that future interventions utilize behavioral theories to strengthen the impact and ensure the sustainability of interventions. 87 This is of extreme importance as the follow-up duration for studies included in our review was short, which could raise concerns regarding the long-term effect of these interventions. Additionally, the various interacting components in behavior change research makes it challenging to identify the active, effective components within interventions and for others to replicate them.
On that account, it is of paramount importance that detailed descriptions of the interventions, in terms of structures, processes, and outcomes, are included in publications to allow them to be reproduced and for readers to consider the studies within the context of their own practice. We therefore endorse the use of the DEPICT-2 tool to structurally describe the intervention of interest in pharmacy practice research. 28
Furthermore, it should be noted that none of the studies investigated prescribing (either independently or collaboratively) as part of the clinical pharmacy practice. Pharmacist prescribing showed promising results as it offers a wide range of benefits such as quicker and more efficient access to medicines for patients, a reduction in physician workload, and enhanced professional satisfaction.88,89 These favorable outcomes might be amplified in perioperative settings due to additional barriers that exist in surgeons’ practice such as logistics, time, and knowledge about medications, which might affect their ability to prescribe safely.90,91 Therefore, pharmacist prescribing in perioperative settings could be a potential area of work in the future.
Conclusion
The results of this meta-analysis indicate that pharmacist-led interventions in perioperative settings decreased the LOS and readmissions. However, the effect on other healthcare utilization endpoints is inconclusive based on the current body of evidence. There is some evidence that multifaceted complex interventions that occurred throughout the perioperative period, starting from preadmission medication reconciliation to comprehensive discharge plan, are more likely to yield positive impact but this is generally of low quality and insufficient volume. Findings from this review help policymakers design appropriate theory-informed pharmacist interventions in perioperative setting by keeping in view their available resources.
Supplemental Material
sj-docx-1-taw-10.1177_20420986241260169 – Supplemental material for Interventions and impact of pharmacist-delivered services in perioperative setting on clinically important outcomes: a systematic review and meta-analysis
Supplemental material, sj-docx-1-taw-10.1177_20420986241260169 for Interventions and impact of pharmacist-delivered services in perioperative setting on clinically important outcomes: a systematic review and meta-analysis by Lina Naseralallah, Somaya Koraysh, Bodoor Aboujabal and May Alasmar in Therapeutic Advances in Drug Safety
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.