
Abstract
Background and objective:
Drug-related problems (DRPs) are often seen when a patient is transitioning from one healthcare sector to another, for example, when a patient moves from the hospital to a General Practice (GP) setting. This transition creates an opportunity for information on medication changes and follow-up plans to be lost. A cross-sectoral hospital pharmacist intervention was developed and pilot-tested in a large GP clinic. The intervention included medication history, medication reconciliation, medication review, follow-up telephone calls, identification of possible DRPs and communication with the GP. It is unknown whether the intervention is transferable to other GP clinics. The aim of the study was to explore similarities and differences between GP clinics in descriptive data and intervention acceptability.
Methods:
A convergent mixed methods study design was used. The intervention was tested in four GP clinics with differing characteristics. Quantitative data on the GP clinics, patients and pharmacist activities were collected. Qualitative data on the acceptability were collected through focus group interviews with general practitioners, nurses and pharmacists. The Theoretical Framework of Acceptability was used.
Results:
Overall, the intervention was found acceptable and relevant by all. There were differences between the GP clinics in terms of size, daily physician work form and their use of pharmacists for ad hoc tasks. There were similarities in patient characteristics across GP clinics. Therefore, the intervention was found equally relevant for all of the clinics. Shared employment with unique access to health records in both sectors was important in the identification and resolution of DRPs. Economy was a barrier for further implementation.
Conclusions:
The intervention was found acceptable and relevant by all; therefore, it was considered transferable to other GP clinics. Hospital pharmacists were perceived to be relevant healthcare professionals to be utilized in GP, in hospitals and in the cross-sectoral transition of patients.
Plain language summary
Why was the study done?
Drug-related problems are often seen in patients transitioning across healthcare sectors.
A pharmacist activity was developed and pilot-tested in a large General Practice (GP) clinic. It was unknown whether the activity was transferable to other GP clinics. The pharmacist activity included talking to the patients about their usual medication and adjustment of prescriptions accordingly. The pharmacist activity also included a review of their medications, a follow-up telephone call to the patients and communication with the GP in case of drug-related problems. The aim of the study was to test the activity in different GP clinics and to explore similarities and differences in descriptive data and acceptability.
What did the researchers do?
The activity was tested in four GP clinics within the same geographical area for three months. Descriptive data about the GP clinics, the patients and the pharmacist’s activities performed were collected. Data about acceptability of the activity was collected through focus group interviews with general practitioners, nurses and hospital pharmacists. This qualitative data was combined with descriptive data to explore similarities and differences between GP clinics.
What did the researchers find?
Overall, the activity was found to be acceptable and relevant by all. There were differences between the GP clinics in terms of size, daily physician work form and their use of the pharmacist for ad hoc tasks. There were similarities in patients across GP clinics e.g. in terms of the number of medications or drug-related problems. The activity was found equally relevant for every clinic. Shared employment with access to health records in both sectors was important in the identification and resolution of drug-related problems. The pharmacist had the possibility to bring issues back and forth between the hospital and the GP clinic. Economy was a barrier for further implementation.
What do the findings mean?
The activity was found acceptable and relevant by all; therefore, it was considered transferable to other GP clinics. Hospital pharmacists were perceived to be relevant healthcare professionals to be utilised in GP, in hospitals and in the cross-sectoral transition of patients.
Keywords
Introduction
Drug-related problems (DRPs) are often seen when patients are transitioning across healthcare sectors.1,2 A study found that 81% of discharged patients had at least one prescription error, clerical error or error due to inadequate communication of medicines stopped during admission. 1 Another study found errors in 20 of 22 discharged patients related to treatment efficacy, safety, adverse effects, dispensing or missing electronic prescriptions. 2 DRPs while transitioning from General Practice (GP) to hospital were shown to be caused by inadequate focus on updated medication information. 3 During patients’ discharge, DRPs were commonly caused by, for example, inadequate information regarding medication changes during admission. 3 DRPs may lead to medication errors which expose patients to unnecessary risk and possibly increased hospital stays, healthcare costs and mortality.4–7
In Denmark, information on patients’ current medication is shared through the Shared Medication Record (SMR) in which both the hospital and GP can access and update the information.8,9 Information quality depends on whether the SMR is properly updated. Other information about the patient is not shared via the SMR, and the hospitals and GPs have separate electronic patient records for this information. There is no easy access to information about the reasons for treatment decisions between the sectors.
Hospital pharmacists play a crucial role in collaborating with physicians and nurses within the hospital setting. They possess extensive knowledge regarding medication-related matters. Pharmacists working in both the Hospital Pharmacy and GP settings have access to patient records in both places. As a result, they can facilitate seamless cross-sectoral transitions for patients.
Previously, the cross-sectoral hospital pharmacist intervention was developed and pilot-tested in a large GP clinic. 3 This intervention included medication history, medication reconciliation, medication review, follow-up telephone calls, identification of possible DRPs and communication with the GP. The pharmacist identified and solved several DRPs, medication errors were avoided and patient safety was improved. The intervention was considered relevant by staff in both healthcare sectors and patients, 3 but it is unknown whether the intervention is transferable to other GP clinics.
The purpose of this convergent mixed methods study was to explore similarities and differences between GP clinics by integrating both quantitative and qualitative data. We conducted qualitative focus group interviews to explore acceptability of the intervention. We used descriptive data of the clinics, patients and pharmacist activities to compare the results from the qualitative and quantitative data collection and analysis.
Methods
Design
A convergent mixed methods design was used in which quantitative and qualitative data were collected and analysed independently, then integrated and interpreted together 10 (Figure 1).

The convergent mixed methods design. 10
The study is reported in accordance with the guidelines for Good Reporting of A Mixed Methods Study (GRAMMS). 11
Setting
The study was performed in four GP clinics within the same cluster (Northern Djurs Municipality) and their local hospital, Randers Regional Hospital (RRH), located in Denmark. Characteristics of the Danish healthcare system and RRH are described in Table 1.
Characteristics of the setting.

eMAR, electronic Medication Administration Record; SMR, Shared Medication Record.
Participants
Quantitative study groups – descriptive data
Four GP clinics with differing characteristics participated in the study. Two of the clinics were solo practices (respectively 1570 and 2270 patients), one was of medium size (3800 patients) and one was a large clinic (8740 patients).
Patients in cross-sectoral transition were also participants. Patients were consecutively recruited Monday to Friday at RRH by pharmacists, or at the GP clinics by the GPs, a nurse or a pharmacist. Written informed consent was obtained. Patients ⩾18 years old were eligible for inclusion but were excluded if admitted to the maternity ward, hospitalized due to a psychiatric diagnosis, considered too ill (suicidal, cognitive impairment, life-threatening illness), or were unable to speak Danish.
Additionally, three pharmacists from the Hospital Pharmacy (Central Denmark Region) who performed the intervention were part of the quantitative study. They ranged between 15 and 27 years of experience and frequently dealt with medication reviews on a daily basis (see Table 2 for a description of a medication review).
Description of the cross-sectoral hospital pharmacist intervention. 3

This table gives information on the interventions performed by the three hospital pharmacists who were partly employed in the GP clinics during the study. The intervention was primarily patient-oriented and therefore, the GP-staff was affected, when a record note was made or the pharmacist talked to the GP about a DRP.
Pharmacist collecting informed consent.
Could be performed from the hospital if the pharmacist had remote access to the GP record.
DRP, drug-related problem; GP, general practice; SMR, Shared Medication Record.
Qualitative study groups – acceptability
Hospital pharmacists and healthcare professionals (HCPs) from the GP clinics participated in the qualitative study.
Intervention
The cross-sectoral intervention was developed and piloted prior to this study and included medication history, medication reconciliation, medication review and follow-up telephone call to patients after discharge 3 (Table 2), and ad hoc tasks.
During the study, the pharmacists had a shared employment between the Hospital Pharmacy and the GP clinic. The pharmacists were physically present in the clinic 3–6 days in January 2022 where they were introduced to the GP-staff and the intervention. In the study period (February–April 2022), they were in the GP clinics 1–2 days a week depending on the clinic size (10–20 days totally).
Outcomes
Quantitative outcomes – descriptive data
Descriptive data on the GP clinic characteristics, the patients and the pharmacist activities were included.
Qualitative outcomes – acceptability
The Theoretical Framework of Acceptability (TFA) 16 was used to assess acceptability of the intervention. TFA describes affective attitude, burden, perceived effectiveness, ethicality, intervention coherence, opportunity costs and self-efficacy. 16 Additionally, perspectives on future intervention implementation were explored.
Integrated mixed methods outcomes
Quantitative and qualitative data were integrated and interpreted to highlight similarities and differences between clinics.
Data collection and analysis
Quantitative data – descriptive data
Descriptive data were presented as numbers, means, medians, interquartile range or proportions when relevant.
DRPs were defined as events or circumstances involving drug therapy that actually, or potentially, interfered with desired health outcomes. 17
Continuous outcomes were compared using the Kruskal–Wallis rank test or Bartlett’s equal-variances test, depending on whether or not data were considered normally distributed (more than two groups). Binary outcomes were compared in a Chi-squared test.
Pharmacists’ ad hoc activities were registered by the hospital pharmacists during the intervention.
Qualitative data – acceptability
Semi-structured focus group interviews were conducted in May–June 2022. For each GP clinic, two interviews were held; firstly, with the hospital pharmacist involved and secondly, with HCPs in each clinic.
The interviews were facilitated by the last author (CO) and supplemented by the first author (CAS) in the clinics and at the Hospital Pharmacy. Interview guides were prepared with inspiration from the TFA reflecting the seven component constructs 16 (Supplemental Appendices 1 and 2). They were pilot-tested on one pharmacist (data included in the data analysis).
The interviews were audio-recorded, transcribed verbatim by CAS and anonymized. The transcripts were read by CO and CAS. A preliminary analysis was performed by CAS and discussed with the authors in an interdisciplinary workshop. NVivo (1.5.2) was used for deductive coding into the seven TFA component constructs 16 and a category for ‘Thoughts of future implementation’. Quotations were chosen by CAS, CO and the second author (LJ).
Integrated mixed methods data
Similarities and differences between the GP clinics were explored and integrated in a joint display. 18
Results
Quantitative results – descriptive data
GP clinic characteristics and study recruitment data is presented in Table 3. The clinics varied in size, types of HCPs, record system and daily work form. In clinic 1, six different types of HCPs were employed, and the senior physicians used supervision of junior physicians as their primary daily work form. Most of the smaller clinics were more traditional in their daily work form with consultations, and only employed physicians, nurses and a secretary.
GP clinic characteristics and study recruitment.

Minor in brackets – Supervision: Practice assistants (medical student), physicians under education and nurses have consultations, senior physicians supervise when needed. (Consultation): Senior physicians may have consultations in smaller numbers. Consultation: Senior physician have patient consultations. (Supervision): Nurses and/or physicians under education have consultations; senior physicians supervise when needed.
GP clinic 3 is located in a rural area and consults patients from the rural district around.
Incl. practice assistants (medical students).
Accountant of the clinic.
Physician’ work form.
Only the Hospital pharmacists participated in the duties with the transitions of care between the hospital and GP clinic.
GP, General Practice; RRH, Randers Regional Hospital.
A total of 511 patients were referred to the medical, surgical or orthopaedic surgery outpatient clinics at RRH; 13 patients were recruited. A total of 321 patients were hospitalized; 110 of them were included. Eleven patients were withdrawn due to death or unrecorded reasons.
Patient characteristics are described in Table 4.
Patient characteristics.
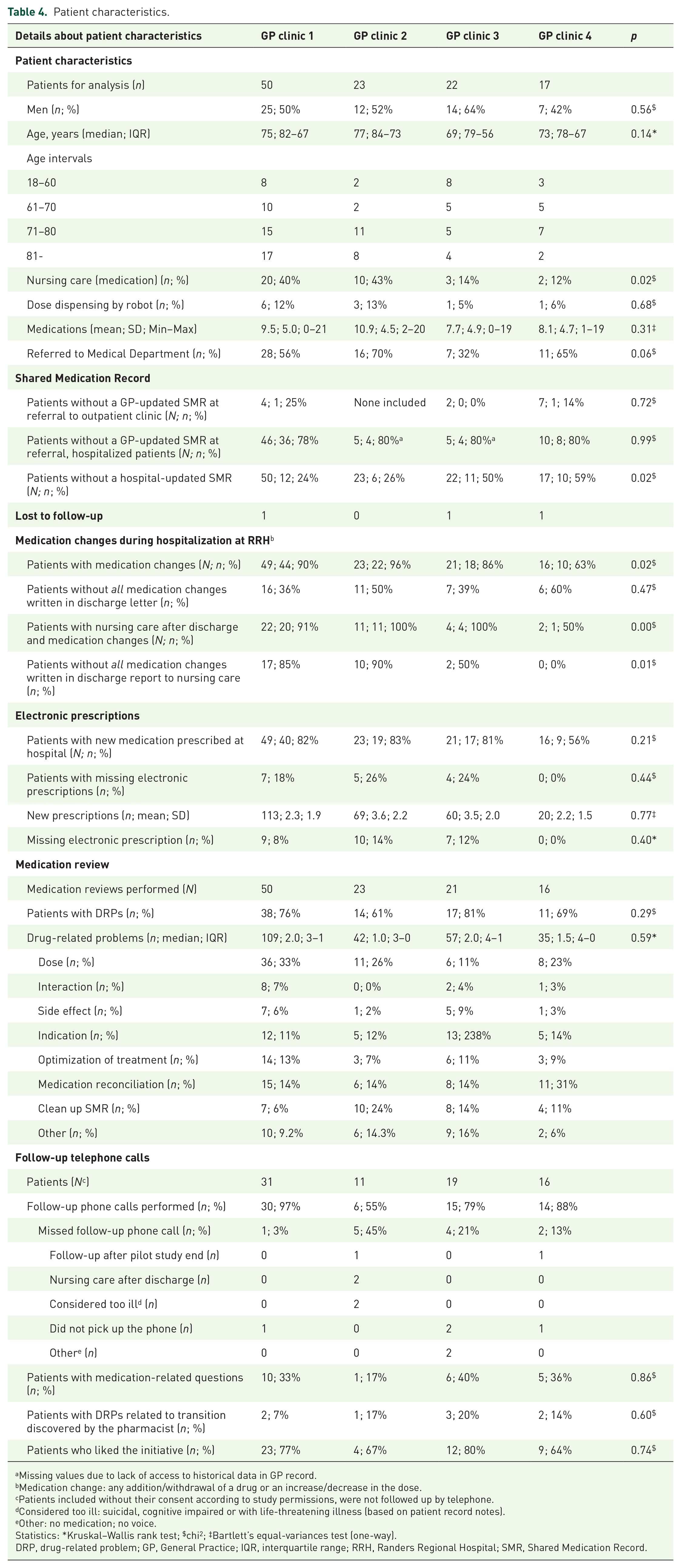
Missing values due to lack of access to historical data in GP record.
Medication change: any addition/withdrawal of a drug or an increase/decrease in the dose.
Patients included without their consent according to study permissions, were not followed up by telephone.
Considered too ill: suicidal, cognitive impaired or with life-threatening illness (based on patient record notes).
Other: no medication; no voice.
Statistics: *Kruskal–Wallis rank test; $chi2; ‡Bartlett’s equal-variances test (one-way).
DRP, drug-related problem; GP, General Practice; IQR, interquartile range; RRH, Randers Regional Hospital; SMR, Shared Medication Record.
A total of 66% of patients were older than 70 years; around half of them were men.
The patients received from 0 to 21 medications prior to hospital contact (mean: 9.2 medications). In total, 86% of patients had hospital medication changes; 43% of these patients did not have their medication changes properly described in the discharge letters to the GP. In 81% of patients, the discharge reports to municipal nursing care lacked information about medication changes.
DRPs were identified during medication review in up to 81% of the patients – often related to dose, optimization of treatment, indication, medication reconciliation and a clean-up of the SMR. The severity of the DRPs were not assessed.
At follow-up, up to 40% of the patients had medication-related questions. Most patients liked the initiative with a follow-up telephone call. DRPs related to transition were discovered by the pharmacist in up to 20% of the patients. For example, a patient was discharged on amlodipine, and there was a discrepancy in the dosing between the SMR and discharge letter. A similar incident occurred with another patient who was discharged on acetylsalicylic acid. In the SMR, it was documented that the patient was taking acetylsalicylic acid 75 mg twice a day. However, in the discharge letter, it was documented that acetylsalicylic acid was reduced to once daily, thus revealing a discrepancy between the SMR and discharge letter.
Hospital pharmacist’s ad hoc activities in the GP clinics are described in Table 5.
Pharmacist ad hoc activities performed in the GP clinics.

The GP clinics were given the opportunity to ask the hospital pharmacist to perform ad hoc activities when needed. This table shows the types and numbers of these activities.
Triple-whammy (concurrent use of a diuretic, a renin–angiotensin system inhibitor and a NSAID).
Best practice in SMR.
Introduction of pharmacist students.
360° evaluation of a physician under education.
GP, General Practice; NSAID, non-steroidal anti-inflammatory drug; SMR, Shared Medication Record.
In clinic 3, the GP-staff had many questions to the hospital pharmacist about medicines, for example, drug choice, dosing interval and drug formulations. Also, in clinic 4, three cases of drug information were registered, for example, a question about long-term side effects.
Qualitative results – acceptability
In clinic 1 and 2, a GP, a nurse and the hospital pharmacists participated in the interviews [one interview with each of the two hospital pharmacists; one interview with each of the clinics (two participants each)]. In clinic 3, two GPs and the hospital pharmacist participated [one interview with the hospital pharmacist; one interview with the clinic (two participants)]; and in clinic 4, the GP, two nurses, a secretary and the hospital pharmacist participated [one interview with the hospital pharmacist; one interview with the clinic (four participants)].
Acceptability is presented for each of the seven TFA component constructs 16 below.
Affective attitudes (how an individual feels about the intervention)
Affective attitudes were expressed in positive terms by both GP-staff and hospital pharmacists. The intervention gave a feeling of better collaboration between healthcare sectors and was considered relevant by the GP-staff.
Because you come from the hospital and reach out to general practice – it gives a feeling of better collaboration. (GPclin1) She just went into it and was a part of it [the clinic], so it was really sad when she stopped. (GP1clin3) It gave a feeling that it [the intervention] made sense. (GPclin4)
The pharmacists felt welcome. It was exciting to work in the GP clinics and to see a different everyday life.
The GP-staff were really great at welcoming new people. You felt welcome and comfortable, being there. And everyone had a reason to be there. (Pharmacist1) I think the collaboration has been good. They have been very open to – they have not been dismissive of me as a person, or have not been dismissive of me as a professional group or of the project itself. (Pharmacist2)
The pharmacists also felt a humility about not wanting to disturb the physicians unnecessarily.
It was difficult to catch physicians and nurses because they were sitting in their treatment rooms with patients, so you don’t just go and knock [interrupt]. (Pharmacist1) I don’t know if it’s part of being a pharmacist, or if it’s individual, but you don’t want to disturb unnecessarily. (Pharmacist3)
Burden (perceived amount of effort that is required to participate in the intervention)
The staff in all GP clinics expressed that it had not been a burden to participate in the intervention. It made them reflect on the way they normally work, but their everyday life in the clinic did not change.
It has only been positive that we have gained a different perspective on it [the medicine]. (GPclin1) We have so much to consider and medicine is just a small part of it. It was great to have someone who just focused on it [the medicine]. (Nurseclin2) I don’t think it interfered in any way. You didn’t think – Oh no, the pharmacist is coming and getting in the way. Not at all. It wasn’t troubleshooting. No, it wasn’t that experience at all – troubleshooting and pointing fingers. You can’t use that for anything, simply. (GPclin2)
Carrying out the intervention was not a professional burden to the hospital pharmacists. On the contrary, it was very rewarding to have direct contact with the patients.
I wasn’t challenged professionally, but I don’t think you should put in the youngest colleague. You have to have a certain ballast to be able to have a discussion with the GP. (Pharmacist2)
The pharmacists in clinic 1 and 3 found it difficult to find the right moment to talk to the GPs about patients and to offer ad hoc tasks.
They each have their own calendar, where patients are booked in. So it was rare that there was time to catch them between patients. (Pharmacist3) It had a lot to do with whether you were visibly present. (Pharmacist 3)
In contrast to this, the pharmacist in the solo practices found that the doctors were easy to get hold of.
There has been easy access to the staff. There was easy access to the GP, and if you came and asked about something, they knew exactly what, and who, you were talking about. (Pharmacist2)
The pharmacist in the solo practices got their own office from day 1. In clinic 3, the pharmacist was allocated a place to sit from time to time (in an examination room or in a hallway). In clinic 1, a seat at a cafe table in the conference room was allocated. This challenged the working environment.
The thing about not having a permanent workplace. And it’s not because, when you only come twice a week, you have to have a specific workplace. But I was sitting at such a round cafe table. It faces the opposite of all computer desks, so I actually sat really badly. (Pharmacist1)
Ethicality (the extent to which the intervention has good fit with an individual’s value system)
In all clinics, the intervention agreed well with their ethical values. The hospital pharmacists had not interfered in a negative way. Access to record systems in both healthcare sectors was perceived as particularly advantageous, but a contract or an employment in the clinic is necessary.
I have not experienced it as untimely interference, but more like positive sparring. (GP1clin3) You have a duty of confidentiality in both places. So I simply can’t see how that would be a blocking factor. (GPclin1) When you do something like this. Then there must be official agreements. (GPclin4)
The intervention was in line with the hospital pharmacist’s ethical values. The hospital pharmacist in clinic 1 expressed a concern whether it could be confusing for the patients that another HCP looks at their medicine. Others could perhaps do it, but it requires allocating time to maintain a cross-sectoral focus.
What I did, they would be able to do in the clinic. The doctor would be able to do it. Or the nurse could do it. But will it be done? They focus on delivering the treatment that the patient demands that day at that time, and within the framework they now have. (Pharmacist1)
Intervention coherence (the extent to which the participant understands the intervention and how it works)
Overall, there was good coherence between GP-staff and hospital pharmacist perspectives, and the purpose of the intervention. The hospital pharmacist intervention was a link between healthcare sectors, and having access to both record systems was perceived as a really good idea. The extent to whether the GP-staff understood the elements of the intervention and how these worked is unknown.
It will be better for the patient because it catches some things that would otherwise fall through the safety net. (GPclin2). That someone in a different and more systematic way reviews patients’ medication and makes some suggestions for adjustments or discontinuations. It is always useful. Definitely. (GPclin1) We have access to e-journals [hospital records], but it is wildly outside the scope of what GP can offer. (GPclin4) They are busy in the hospital. . . we are busy here. We don’t have time. We constantly think that it is their responsibility, and this is mine. So it is good that there is someone who builds this bridge [between sectors]. (GPclin4)
Opportunity costs (the extent to which benefits, profits and values must be given up to engage in the intervention)
The staff in all of the GP clinics thought it was important to focus on the sector transition. Additionally, the staff believed they would benefit from having a hospital pharmacist to perform other delegated tasks in the clinic, for example, medication reviews, education and drug information.
Someone who has knowledge, and sort of knows what is up to date and what has just been found out. I think it would be fruitful. (GPclin4)
In GP clinic 1, the staff saw the hospital pharmacist’s input as a benefit for the patients’ annual check-up. The record note would be taken into account there and not months before, unless something life-threatening was discovered.
I would say if you have a medication review note, or something that you know is there, and then you say: now I need it; now we have to look at medicine. Okay, then we will find it and read it. Then it is a saving. Although it is an extra thing to have. (GPClin1)
Economy was a barrier to implementation in three of four clinics.
Economy is a barrier, and so is practicality. Where do you get hold of someone like that – we can’t hire a full-time pharmacist. (GPclin1) A fee would be motivating; if you could take a fee within the payment system we have now. I actually think that you could use that argument. (GPClin1) Basically if it is us who has to pay for it, you can say that it also has to pay off in another way, and I don’t know how. (GP2clin3)
In the solo practices, the GP preferred not to have an employer–employee relationship, as this would affect the professional relationship.
So, she’s independent, you could say, impartial. She becomes more neutral in her being here when she does not have an employment relationship. So she’s coming and if we’re just looking politically at this thing with local hospitals, and we need to have more coherence, right? Then I could easily see a – not a pharmaconomist – it must be a pharmacist, I’m sorry to say. (GPclin2) I think that the effective, and the good and the fruitful – it is that there is someone who is neutral in relation to both the hospital, and us, and sees things from a higher perspective, and can see where the hell things are going wrong and has access to both records. (GPclin4)
The hospital pharmacists saw the cross-sectoral task as particularly important; however, every patient cannot be followed up by a hospital pharmacist. Shared employment and access to both records systems was a benefit.
We are not very good at discharging patients. It is of course a superficial solution to put in another professional group to deal with what the first professional group may not have done well enough, but there is no one else who has that focus. (Pharmacist2) The thing about a patient always being followed home by a pharmacist. I think it is a resource intensive task, but perhaps you could find another communication model. (Pharmacist1)
Perceived effectiveness (the extent to which the intervention is perceived as likely to achieve its purpose)
The GP-staff found it valuable to have a person with an overview of the patient’s medical treatment in both healthcare sectors as the cross-sectoral transition is often problematic. The staff experienced benefits from having a collaboration with a hospital pharmacist with shared employment between Hospital Pharmacy and GP. Both the great insight into what goes on at the hospital, and the advantages of having access to both record systems. For clinic 2, it was crucial that the hospital pharmacist came from their own local hospital, so the pharmacist would know about local circumstances.
The intervention has changed the GP’s way of working with updating SMR, but apart from that it has not changed their daily workflow.
The medication reviews were useful; however, the GPs did not act on suggestions right away, but may be the next time the patient is in the clinic.
According to the secretary in clinic 4, patients often required prescriptions after a discharge, so it made good sense to have someone who catches it before it becomes a problem.
The shared employment and access to both record systems has made decidedly good sense, because it would have taken us a very long time to solve the problems ourselves. It was actually quite effective. (GPclin1) The thing about having someone who covers both sectors, is actually quite nice. (GPclin4) Before, updating SMR was something that we didn’t really know what was used for elsewhere. Now it has actually become something we use, because we hand over information to someone who can use it at the hospital. I think that is a big advantage. (GPclin1) It gave me quite a lot, especially those ‘Attention’ patients, since they are not patients I otherwise pay attention to. I think that this small project has probably changed my way of thinking more than those big surveys. (GPclin2) It [the medication reviews] was useful. And also something that could result in making some changes. (GP1clin3) Yes, you take it [a medication review note] to heart. But it’s not certain that you act on it now. It’s not like we act urgently on a comment. It may well be six months before you see the patient again. But the note from the pharmacist will still be there. (GPclin2) My experience was that when I asked about something, she explored it thoroughly and spent a long time on it. She took things seriously and was thorough. (GP2clin3)
The hospital pharmacists perceived that the intervention was effective in optimizing patients’ medication in the sector transition – particularly as no one else has that focus. It has made very good sense to be employed in both sectors and to have access to both health records. It gave an understanding of both worlds and an opportunity to take topics back and forth between hospital and GP.
It [being employed in both places] makes really good sense, and it has meant that I have been able to take some things back to the hospital and say: This, it doesn’t work in general practice. Can we do something about it? (Pharmacist2) It has of course been good that you have had insight into both record systems. Because discharge letters sometimes come a day too late in relation to what is actually needed. (Pharmacist3)
It was difficult for the hospital pharmacists to find the optimal time for the follow-up telephone calls to the patients when the pharmacist was in the clinic only once or twice a week; however, most patients were happy about the call.
I haven’t called anyone who thought I should not. There were some who perhaps didn’t think they were in the target group. It helped to call them, because that’s where you get the truth. Sometimes they don’t take the medicine that the doctor believes. (Pharmacist2) The patient could have been discharged on Thursday, and when I came the next Tuesday a lot could have happened during the weekend. (Pharmacist1) When you are at the hospital, you should really have been in the GP clinic. And when you are in the GP clinic you should really be in the hospital. It is a challenge that I do not know how to fix. Besides having several pharmacists working in the same way. (Pharmacist2)
The hospital pharmacists reported that they lacked feedback on the notes in the medical record.
It would have been nice to know what they thought about the relevance of my comments. (Pharmacist1) I made some notes in the system, but I don’t think that the physicians necessarily took a position on the notes that I made. But I also have to respect that the doctor knows how far he can go with the patient. (Pharmacist 2)
Self-efficacy (the participant’s confidence that they can perform the behaviour(s) required to participate in the intervention)
In GP clinic 1 and 4, the GP-staff felt confident with the intervention and the hospital pharmacist’s role; however, the hospital pharmacists’ tasks were not fully incorporated in their daily routines in clinic 1.
If we had actively hired the pharmacist, then we would also have had it much more under our skin. Not as such a project that comes like ‘icing on the cake’. (GPClin1) I was pleasantly surprised. That’s because you don’t know what they [the pharmacists] represent. Knowledge, that is – great knowledge, I think. (NurseClin4)
In GP clinic 2, it took some time for the GP-staff to build confidence, and in clinic 3, the GP-staff did not feel confident with the intervention or how best they could use a hospital pharmacist.
Quietly we got confident, but I could probably have been introduced a little better. (NurseClin2) So, exactly that, what can they be used for? Not that I don’t know what they [pharmacists] stand for. . .No, but from there and then to what you can use them [pharmacists] for in your own daily practice. (GP2Clin3)
The hospital pharmacists felt confident performing the intervention but were challenged by the fact that the GP-staff did not know how a hospital pharmacist could best be utilized in the clinic. They thought that the study period had been too short.
They found it difficult to define what kind of tasks they wanted to use the pharmacist for ad hoc. It was also only perhaps in the last 14 days, when you really started to get to know each other, that you could have the dialogue there. So perhaps the study period was too short. (Pharmacist3)
Thoughts of future implementation
The staff in all of the GP clinics saw advantages of having a collaboration with a hospital pharmacist in the future. Besides cross-sectoral tasks, medication reviews and teaching, the GPs highlighted delegated tasks that could be carried out in the clinic, for example, follow-up of patients in treatment of hypertension or a medication review as part of the annual check-up.
It is important that it is someone with a connection to both sectors. Otherwise it will only be tasks in the clinic, and then we will not utilise the advantages of having focus on the sector transition and access to both systems. (GPclin1) I have considered if we could create a ‘hybrid clinic’. Were a pharmacist could follow-up on our patients with hypertension and also have an extra eye on the patients that are discharged from the hospital. A ‘sector transition clinic’. Politically, maybe that is a better name. (GPclin2)
Economy was a barrier to most of the GP clinics; however, the possibility to share a hospital pharmacist between the clinics was a considered option. The small clinics did not want an employer–employee relationship; they preferred a neutral relation. However, it was still important that they were familiar with the pharmacist, so they would feel it as a collaboration and not as a correction.
It is important that it is a person that you can relate to, so that it is not a system. Because as soon as it is a system, you can get the feeling that you are being corrected. So it’s much nicer when it’s a collaboration. (GPclin4)
The hospital pharmacists saw advantages of working in a GP clinic alongside working at the Hospital Pharmacy. In addition to cross-sectoral tasks, medication reviews and teaching, other delegated tasks were mentioned, such as the possibility of a pharmacist being available to the municipal nursing care after discharge. However, the challenges of identifying which patients are in need of being followed up by a hospital pharmacist was highlighted.
The hospital pharmacists also contemplated the advantages of the hospital discharge process, which included enhanced communication regarding the medication changes and follow-up plans. Currently, discharge letters – written by various practitioners – are received by the GP and municipal nursing care, leading to inconsistent messages.
Integrated mixed methods results
Aggregated quantitative and qualitative data are presented in Table 6. Similarities and differences are described as well as interpretations of integrated results.
Joint display of mixed methods integration and interpretation.

GP, General Practice; HCP, healthcare professional.
Discussion
In this study, we tested a cross-sectoral hospital pharmacist intervention in four GP clinics to explore similarities and differences between the clinics using quantitative and qualitative data. Overall, the intervention was well-accepted by the GP-staff and the hospital pharmacists.
The GP clinics
There were differences in clinic sizes and the way their daily work was organized.
The smaller clinics prepared an office for the pharmacist. The pharmacist experienced easy access to the GP and felt integrated in the team. The larger clinics were used to interdisciplinary collaboration allowing the pharmacist more freedom to work independently, although pharmacists had less access to the GPs due to GPs busy schedule.
There were differences in the way the GP clinics chose to use the pharmacist resource for ad hoc tasks. In the largest clinic, they oversaw the opportunity whereas others requested drug information, medication reviews or teaching. The differences may be due to busyness, visibility or an expression of different needs. It may also be because most of the GP clinics did not know what tasks a pharmacist could perform.
When looking at patient characteristics, we found patients with similar baseline characteristics (e.g. age and number of medications), SMR update, medication changes, DRPs identified in the medication reviews and at follow-up. Thus, patient characteristics were similar across clinics and therefore, the cross-sectoral pharmacist intervention was found equally relevant to all of the GP clinics.
The intervention
The intervention made sense to GP-staff as they experience many DRPs in cross-sectoral patient transitions. This is in line with previous research where DRPs were seen in 81–91% of discharged patients.1,2 In our study, the cross-sectoral intervention identified and solved several DRPs; in this way medication errors were avoided.
DRPs could be avoided if the hospital had more focus on the discharge process; however, this will not solve every problem. Some DRPs happen when transitioning patients between the hospital and the GP. No one else, besides the pharmacists in this study, has particular focus on medicine in the cross-sectoral field. Additionally, if the patient doesn’t understand what medication changes have been made, there can still be DRPs after discharge. Some patients have low health literacy,19,20 leading to increased health inequality. 21 To reduce inequality in healthcare, we need to differentiate the treatment and healthcare offered to the individual to mitigate unequal access to and use of healthcare services (equity). 22 A cross-sectoral hospital pharmacist intervention with special focus on frail patients may be an option. In addition to improved treatment, communication and fewer readmissions, 23 coherence of the treatment is expected to improve. The population in the Northern Djurs Municipality may be different from other municipalities as 87% of the population has low socio-economic status 19 ; therefore, the intervention may be more applicable to clinics serving this population. Not every country has an electronic SMR as in Denmark, and communication about the patients’ medication may be even more challenged in these countries.
Staff in all of the GP clinics saw possible benefits of delegating tasks to a pharmacist. This is in line with previous reviews describing possible pharmacist tasks in GP, for example, medication reconciliation, medication review, patient counselling/follow-up, drug information and education.24–26 Shared employment and access to health records in both healthcare sectors was considered valuable by all. This was also the case when the intervention was pilot-tested. 3 The GP clinics already have access to the hospital record (e-journal); however, it requires detective work to find the information they are looking for, and for some it is ‘wildly outside the scope of what GP can offer’.
The shared employment also gave the pharmacist the opportunity to bring issues back to the hospital.
The pharmacists lacked feedback from the GPs on their medication review notes. As patients often are hospitalized for a very short time, the pharmacists are accustomed to working quickly and getting response from the hospital physicians shortly after their medication reviews. GP clinics primarily treat patients for current issues on the specific day. The GPs stated that they had taken the notes into consideration; however, the notes would be used at a later date when the patient had a consultation, for example, at an annual check-up. Thus, what the pharmacists considered as lack of commitment or an inefficiency of the intervention was actually due to differing cultures/expectations among the different HCPs. A study period of 3 months may have been too short to start a feedback loop and see the effect of the study; however, this was not the aim of the study. It is unethical to have a cross-sectoral pharmacist intervention and a medication review note that is not taken into consideration before the patient revisits the clinic. A lot can happen in 6 months. If a cross-sectoral intervention is implemented in the future, the GPs must reconsider the work flow to gain the most of the intervention.
The pharmacist reported that the timing of the telephone call to the patients after discharge was difficult, as they were only in the GP clinics 1–2 days a week. Perhaps the use of remote access to the GP record system or having a team of several pharmacists working the same way would solve this problem.
Implementation in the future?
For most, economy was a barrier for further implementation. The possibility to share a pharmacist within the cluster was considered an option. The possibility to delegate tasks from the GP to the pharmacist was also considered, for example, medication review prior to an annual check-up or follow-up on hypertension patients in a ‘hybrid clinic’. This would give a chance to receive a fee covering the costs of having a pharmacist. This would, however, not cover cross-sectoral tasks as in the intervention. The Danish healthcare system works in silos, both economically, and professionally. In the spaces between the silos, no one is responsible for things being connected. 27 There is an ambition to have a future healthcare system, which supports a preventive and coherent healthcare system with more equality. 28 With the current lack of physicians and nurses, we perceive hospital pharmacists to be a relevant HCP to be used in GP, in hospitals and in the cross-sectoral transition of patients. The question is, who should pay for the pharmacist?
The largest clinic perceived that an employer–employee relationship would commit them more; however, in both solo practices, they preferred not to have this relationship fearing it would not be neutral.
Future research
As perceived by one of the pharmacists, it would be very resource-intensive if every discharged patient were followed up by a pharmacist. Therefore, future research with focus on which patients may benefit the most from this intervention, is considered.
Possibilities for a pharmacist to be more integrated in the discharge process is considered. In some hospitals in England, a pharmacist prescriber is embedded within the medical team and is in charge of writing about medication in the discharge letter and review prescriptions. 29 In the OPTIMIST study, 23 the extended pharmacist intervention included medication review, three motivational interviews, communication with the primary care physician, pharmacy, and nursing home, and follow-up after 6 months. This study showed to reduce the short- and long-term rates of readmissions.
As economy was a barrier to most of the clinics, further investigation on financial models is needed – who pays and how should the work of a pharmacist in a shared employment between the Hospital Pharmacy and GP clinics be organized?
Strengths and limitations
This study has strengths and limitations that merit further discussion.
Strengths
The intervention was initially tested in one GP clinic 3 and afterwards in four GP clinics with differing characteristic; therefore, acceptability was thoroughly explored.
The study was a mixed methods study including both quantitative and qualitative methods. The two data types were integrated and expanded the understanding of the topic.
Acceptability was assessed using TFA 16 as it represents a deliberate way to assess acceptability in the feasibility phase of a complex intervention. TFA captures key dimensions of acceptability, a strong tool when assessing acceptability.
Limitations
The collaboration between pharmacists and GP clinics is new in Denmark; therefore, not all of the GP-staff knew how a pharmacist can be utilized prior to the study. The study period was 3 months and in the solo practices the pharmacist worked there once a week, giving around 10 days where the pharmacist and the GP-staff met. Additionally, some of the pharmacists had a personal mind-set of not wanting to disturb the GPs unnecessarily. Therefore, a study period of 3 months may have been too short for the GP-staff and the pharmacist to become familiar with each other.
The GP clinics volunteered to participate when the Hospital Pharmacy was recruiting clinics for the study, possibly introducing selection bias.
Recruitment of patients referred to an outpatient clinic did not work so well. The GP-staff had to collect written informed consent from the patient, which drowned in busyness. If the intervention was implemented as part of daily work in the clinic, this process would not have been necessary.
Conclusion
The cross-sectoral hospital pharmacist intervention was found acceptable and relevant by all and; therefore, considered transferable to other GP clinics. The pharmacist in the smaller clinics had easier access to clinicians and felt integrated in the team. The larger clinics were more used to interdisciplinary collaboration, allowing the pharmacist more freedom to work independently.
The intervention was found equally relevant for all GP clinics; however, further investigation on how to choose patients for the intervention is needed. To increase equity in healthcare, differentiated solutions are needed. In a time with a shortage of physicians and nurses, hospital pharmacists are perceived to be a relevant HCP to be used in GP, in hospitals and in the cross-sectoral patient transition.
Shared employment with unique access to health records in both sectors was an important tool in the identification and resolution of DRPs. Financial models need further investigation.
Supplemental Material
sj-docx-1-taw-10.1177_20420986231213714 – Supplemental material for Acceptability of a cross-sectoral hospital pharmacist intervention for patients in transition between hospital and general practice: a mixed methods study
Supplemental material, sj-docx-1-taw-10.1177_20420986231213714 for Acceptability of a cross-sectoral hospital pharmacist intervention for patients in transition between hospital and general practice: a mixed methods study by Charlotte Arp Sørensen, Linda Jeffery, Klaus Roelsgaard, Solveig Gram, Jannik Falhof, Philipp Harbig and Charlotte Olesen in Therapeutic Advances in Drug Safety
Supplemental Material
sj-docx-2-taw-10.1177_20420986231213714 – Supplemental material for Acceptability of a cross-sectoral hospital pharmacist intervention for patients in transition between hospital and general practice: a mixed methods study
Supplemental material, sj-docx-2-taw-10.1177_20420986231213714 for Acceptability of a cross-sectoral hospital pharmacist intervention for patients in transition between hospital and general practice: a mixed methods study by Charlotte Arp Sørensen, Linda Jeffery, Klaus Roelsgaard, Solveig Gram, Jannik Falhof, Philipp Harbig and Charlotte Olesen in Therapeutic Advances in Drug Safety
Footnotes
Acknowledgements
This study could not have been performed without the participation of patients and staff in the GP clinics. Thanks to Randers Regional Hospital and the four GP clinics in Northern Djurs Municipality for active participation in the study. Thanks to the participating pharmacists – without their engagement, the study would not have been possible. Thanks also must be given to the steering committee for their support throughout the study. Thanks to the funders for seeing the potential of the study.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.