
Abstract
Introduction:
The aim of this study was to investigate trends in the prevalence of potentially inappropriate opioid prescribing (PIOP) and identify potential risk factors among Korean noncancer patients.
Methods:
We conducted a cross-sectional study of annual national patient sample data from the Korean Health Insurance Review and Assessment Service (HIRA-NPS) for the period 2012–2018. Noncancer patients who were prescribed non-injectable opioid analgesics (NIOAs) at least once were included. The proportion of patients with at least one PIOP in terms of concurrent use of benzodiazepines or gabapentinoids, substance use disorder, treatment duration, and dosage was evaluated. Multivariable logistic regression was performed to identify the risk factors associated with PIOP.
Results:
Of the 9,772,503 noncancer patients, 1,583,444 (16.2%) were prescribed NIOAs at least once. Among them, 15.7% were exposed to PIOP, and the prevalence was much higher (31.6%) in the elderly group (age: ⩾65 years). The prevalence of PIOP increased 1.1-fold over 7 years (14.8–16.8%) among the total NIOA users and was more pronounced in non-tramadol NIOA users (a 1.5-fold increase, from 13.2% to 19.4%). Multivariable logistic regression indicated that older age, beneficiaries of medical aid or national meritorious service, exposure to polypharmacy, psychological disorder, chronic pain indication, and concomitant sedative use were independently associated with higher odds of PIOP.
Discussion and Conclusion:
We found that the prevalence of PIOP was 15.7% among Korean noncancer patients, and it increased over the 7-year study period. This increasing trend is alarming because it was more drastic with non-tramadol NIOAs compared with that with tramadol. Several patient-level risk factors associated with PIOP would be useful in targeted management strategies for the safe use of opioids.
Plain Language Summary
In Korea, the prevalence of non-injectable opioid analgesic (NIOA) use in noncancer patients steadily increased from 15.3% in 2012 to 17.1% in 2018.
Also, the prevalence of potentially inappropriate opioid prescribing (PIOP) increased from 14.8% in 2012 to 16.8% in 2018.
The following factors were associated with a markedly increased risk of PIOP: age, beneficiaries of medical aid or national meritorious service, polypharmacy, psychological disorder, chronic pain, and concomitant medications.
Introduction
The opioid-related problem is one of the worldwide public health crises. 1 Over the last 10 years, particularly in the United States, various committed efforts for fighting the opioid crisis have culminated in a substantial decrease in the overall national opioid dispensing from 2012 to 2020. 2 However, opioid-related overdose and mortality continued to remain prevalent and unabated. From 1999 to 2019, nearly 247,000 people died in the United States from overdoses involving prescription opioids. 3 In addition, the death rate involving synthetic opioids has increased more sharply than that involving natural and semi-synthetic opioids. 4
Opioid use in Korea is known to be lower than that in other countries; 5 however, the trend in Korea is also increasing.6,7 A recently published study found a significant rise in the opioid prescribing rate (347.5/1000 persons in 2009 to 531.3/1000 persons in 2019) by investigating the 11-year trend of outpatient opioid prescription nationally, in total and then sorted by potency and formulation. 7 Previous studies on opioid analgesics in Korea have mostly focused on chronic opioid use, adverse events, and the evaluation of the outcomes associated with specific opioid ingredients or specific diseases.8 –13
Several studies have reported that the risk of opioid-related harm is highly associated with instances of inappropriate use such as long-term use in patients, use of high doses, a specific drug combination of opioids, or use in patients with mental health disorders, especially substance use disorder.14 –17 Furthermore, the risk of opioid-induced respiratory depression or overdose was higher in opioid users with bipolar disorder/schizophrenia [adjusted odds ratio (aOR): 1.95; 95% confidence interval (CI): 1.43–2.67], high-dose opioid use (100 morphine equivalent dose/day, aOR: 4.96; 95% CI: 3.24–7.61), or benzodiazepine use (aOR: 1.49; 95% CI: 1.22–1.83). 15 Mental health and substance use disorder, opioid use experience, and the use of specific drug combinations have been reported as risk factors for opioid misuse.18,19
Considering these known risk factors for negative outcomes of inappropriate opioid analgesic use, the prescription guidelines of the Centers for Disease Control and Prevention and other institutions recommend that clinicians should evaluate factors such as a history of a substance use disorder, higher dose, and concurrent benzodiazepine use. In addition, to prevent greater than needed quantities of prescription, the initial prescription duration of opioids is recommended to be less than 7 days.20,21 The criteria for opioid use per the drug utilization system of Medicaid or in opioid stewardship strategies include screening for dose, concurrent medications, and prescription duration. 22 In Korea, health insurance limits the duration for which opioid analgesics can be prescribed. However, the official recommendations for opioid prescribing are limited because clinical guidelines for opioid use in noncancer patients have not been published.
To the best of our knowledge, currently, no study has evaluated potentially inappropriate opioid prescribing (PIOP) by applying multifaceted criteria and associated risk factors in Korea. Therefore, based on the previous literature, we sought to investigate a 7-year trend (2012–2018) in the prevalence of opioid use and PIOP and identify risk factors associated with PIOP among noncancer patients.
Methods
Database and population
In this cross-sectional study, noncancer patients who were prescribed non-injectable opioid analgesics (NIOAs) approved for pain control in Korea (ATC code: N02A, R05DA04) were identified from the annual national patient sample data of the Health Insurance Review and Assessment Services (HIRA-NPS) for the period 2012–2018. HIRA receives and evaluates claims from all medical institutions in Korea; thus, its databases include information on healthcare utilization, medication prescription, and basic demographic characteristics of 98% of the Korean population, including both inpatients and outpatients. HIRA-NPS possesses information on 3% of Korean patients, which is extracted using a stratified randomized sampling method. Cancer patients were identified using the following International Classification of Diseases 10th (ICD-10) codes and excluded: C00–C97, D00–D09, D32–D33, and D37–D48. The study was approved by the institutional review board of Yeungnam University (IRB: YU 2019-01-001).
Variables
To evaluate the trend of opioid analgesic prescription patterns, the annual prevalence of opioid analgesic use and PIOP in noncancer patients was evaluated as follows.
Based on a review of previous studies, we defined the well-known risk factors of opioid-related harm as PIOP, as follows: (1) chronic use, yearly NIOA use duration of ⩾90 days; (2) concurrent benzodiazepine or gabapentinoid use for more than 7 days; (3) a diagnosis of substance use disorder; and (4) daily dose, use of a daily morphine equivalent dose of >100.15 –17,23,24 For identification of chronic use, we allowed a certain gap period between NIOA prescriptions. Discontinuation of opioid use was defined as the existence of a long treatment gap between the last date of the prior prescription and the start date of the following prescription; this treatment gap should have been longer than the greater value among 1.5 times the days’ supply of the prior prescription and 30 days. Subsequently, we calculated the duration of NIOA use using the opioid prescription before discontinuation. Furthermore, the prescription frequency and duration, number of ingredients, daily morphine equivalent dose, chronic pain indication, and number of prescribers of NIOAs per patient were identified to evaluate opioid use patterns. In reference to previous studies and the ICD-10 disease code, chronic pain indications were captured using the ICD-10 codes in the opioid prescription as follows: back and neck pain (M40, M41, M42, M43, M45, M46, M47, M48, M49, M54, M50, M51, M53, M54), arthritis and joint pain (M code excluding other chronic pain indication), neuropathic pain (G501, G500, G521, G54, G570, G571, M792, B022, G530), and other pain (R52, F454, M797, M796, G43, G44, R51, R52). When patients had two or more categories of chronic pain indications, the most frequent diagnosis was selected as the chronic pain indication. 25
Analysis
When identifying polypharmacy and the type of concurrent medication, only the medications that overlapped with NIOAs for more than 7 days were considered so as to exclude temporary combinations. In Korea, tramadol use is not as limited as that of other opioid analgesics. Therefore, a subgroup analysis was performed for patients who used tramadol alone and those who used non-tramadol NIOAs. Furthermore, trends in the prevalence of opioid use according to age group (<45 years, 45–64 years, and ⩾65 years), sex, and insurance type were evaluated.
Regarding descriptive statistics, the chi-square and t tests were used for nominal and numerical data, respectively. To explore the risk factors for PIOP, multivariable logistic regression analysis was performed with the following independent variables: age, sex, insurance type, comorbid diseases excluding substance use disorder based on ICD-10 codes, main indications for opioid analgesic use based on ICD-10 codes, concurrent medications excluding gabapentinoids or benzodiazepines, and the number of NIOA prescribers. The Cochran–Armitage trend test was used to evaluate trends in opioid analgesic prescription patterns. This test evaluates the trend for binominal proportions against the ordinal explanatory variable with k categories. 26 Data management and statistical analyses were performed using SAS version 9.4 (SAS Institute, Inc. Cary, NC, USA).
Results
Study population
The characteristics of the study population are summarized in Table 1. From January 1, 2012, to December 31, 2018, 1,583,444 (16.2%) individuals, from among a total of 9,772,503 patients, were prescribed NIOAs at least once. Among them, 248,524 (15.7%) were identified as having been exposed to PIOP. Overall, the number of patients with NIOA prescriptions were the highest (40.7%) among patients aged 45–65 years. However, those aged ⩾65 years were more likely to use opioids inappropriately compared with the other age groups. Furthermore, the potentially inappropriate opioid users were mostly female (62.7%); they were also more likely to have mood disorders, anxiety, or other mental illnesses. Regarding concomitant medications, nonopioid analgesics were the most common, followed by benzodiazepines and muscle relaxants. Among the NIOAs studied, tramadol was the most frequently used medication during the study period, accounting for 88.5% of the total use. The results of patients who used non-tramadol NIOAs and tramadol alone are shown in the Supplemental Table 1.
Baseline characteristics of noncancer patients prescribed non-injectable opioid analgesics during 2012–2018.

NMS, national meritorious service.
Patterns of opioid use
Table 2 presents the opioid use patterns. The prevalence of PIOP over the 7-year study period was 15.7%. Most of the PIOP were due to the concomitant use of benzodiazepines or gabapentinoids with opioids (72.6%) and chronic opioid use (47.3%). However, opioid use in patients with substance abuse (2.4%) and high daily doses of opioids (0.2%) accounted for relatively small portions of PIOP.
Patterns of non-injectable opioid analgesic use in noncancer patients.
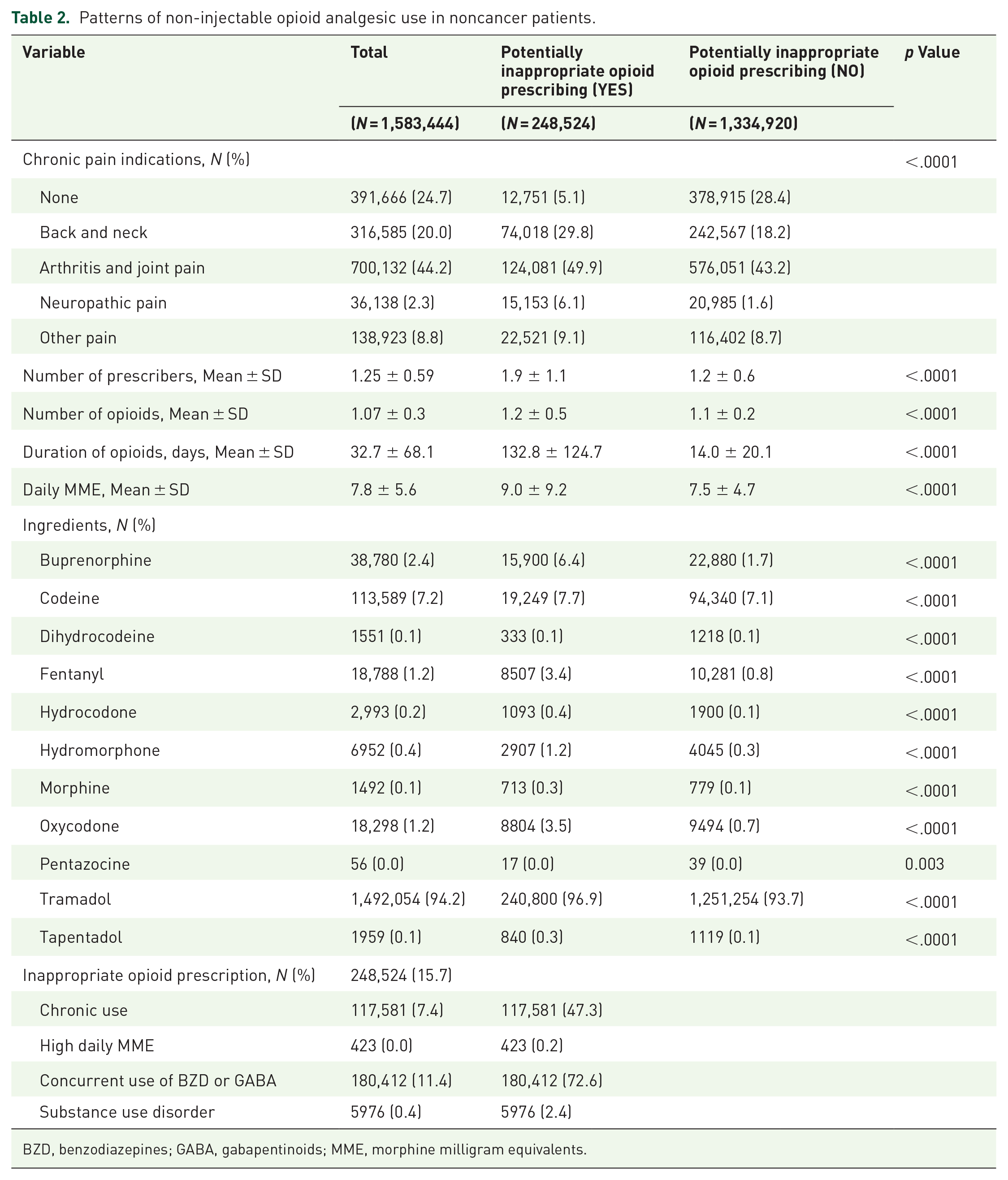
BZD, benzodiazepines; GABA, gabapentinoids; MME, morphine milligram equivalents.
The most common indication for opioid use in all patients was arthritis and joint pain (44.2%), followed by back and neck pain (20.0%). Compared with appropriate opioid users, potentially inappropriate opioid users were more likely to have chronic pain indications. The latter were also more likely to have several prescribers and use the drugs for a longer duration compared with appropriate opioid users (1.9 prescribers versus 1.2 prescribers and 132.8 days versus 14.0 days, respectively). The most prescribed NIOA was tramadol (94.2%), followed by codeine (7.2%) and buprenorphine (2.4%). Among potentially inappropriate opioid users, 6.4%, 3.4%, and 3.5% filled buprenorphine, fentanyl, and oxycodone prescriptions, respectively, whereas the corresponding percentages among appropriate opioid users were only 1.7%, 0.8%, and 0.7%. The results of patients who used non-tramadol NIOAs and tramadol alone are shown in Supplemental Table 2.
Trend
Figure 1 shows the prevalence of NIOA use and potentially inappropriate prescription according to patient characteristics for the 7-year study period. The prevalence of NIOA use in noncancer patients steadily increased from 15.3% in 2012 to 17.1% in 2018, a 1.1-fold increase (p value < 0.001). The prevalence of PIOP also increased from 14.8% to 16.8% (p value < 0.001). Of note, the elderly group (age: ⩾65 years) showed no change in the rate of opioid use but showed a significant (p value < 0.001) increase in the prevalence of PIOP. Patients who were beneficiaries of medical aid or national meritorious service (NMS) showed an increasing trend in the prevalence of NIOA use. Notably, the prevalence of PIOP was very high and steadily increased (36.7–42.0%) in this group.

Trends for prescription and potentially inappropriate prescribing of non-injectable opioid analgesics in noncancer patients. The p values for the Cochran–Armitage trend test were less than 0.0001 except for the following: (a) overall opioid use, all NIOA users: ⩾65 years (p value = 0.22) and (b) potentially inappropriate opioid prescription, only tramadol: ⩾65 years (p value = 0.07).
The increasing trend was more pronounced for non-tramadol NIOAs. The overall prevalence of non-tramadol NIOA use and their potentially inappropriate prescription increased 1.4- and 1.5-fold, respectively. In contrast, the prevalence of tramadol use and its potentially inappropriate prescription only increased by 1.1-fold over the 7-year study period. Unlike the results obtained for all NIOAs considered in the study, the elderly age group (age: ⩾65 years) showed an increasing trend in non-tramadol NIOA use but showed a decreasing trend in tramadol use.
Risk factors of PIOP
Table 3 shows the differential risk factor profiles of potentially inappropriate opioid prescriptions with 95% CIs. Elderly patients (aOR: 2.12; 95% CI: 2.08–2.16), beneficiaries of medical aid or NMS (aOR: 1.59; 95% CI: 1.56–1.62), polypharmacy (aOR: 18.50; 95% CI: 18.13–18.87 for ⩾10 concurrent medications), and mental disorders including mood disorders (aOR: 1.34; 95% CI: 1.31–1.36), anxiety (aOR: 2.28; 95% CI: 1.31–1.36), and other mental illness (aOR: 1.52; 95% CI: 1.50–1.54) markedly increased the risk of PIOP. A similar trend was observed for the medications used to treat these mental conditions. Patients with chronic pain indications were more likely to be prescribed opioids inappropriately than those without these indications. Of note, patients with neuropathic pain were at a significantly higher risk of PIOP (aOR: 12.43; 95% CI: 12.01–12.85). The numbers of NIOA ingredients and prescribers were also associated with a higher risk of PIOP. An analysis of non-tramadol NIOAs showed results similar to those obtained for all the NIOAs considered. Although age was significantly associated with PIOP, the difference in the magnitude of ORs was not evident between the age groups 45–65 years (aOR: 1.42; 95% CI: 1.55–1.61) and ⩾65 years (aOR: 1.48; 95% CI: 1.40–1.56).
Risk factors of potentially inappropriate opioid prescribing in noncancer patients.
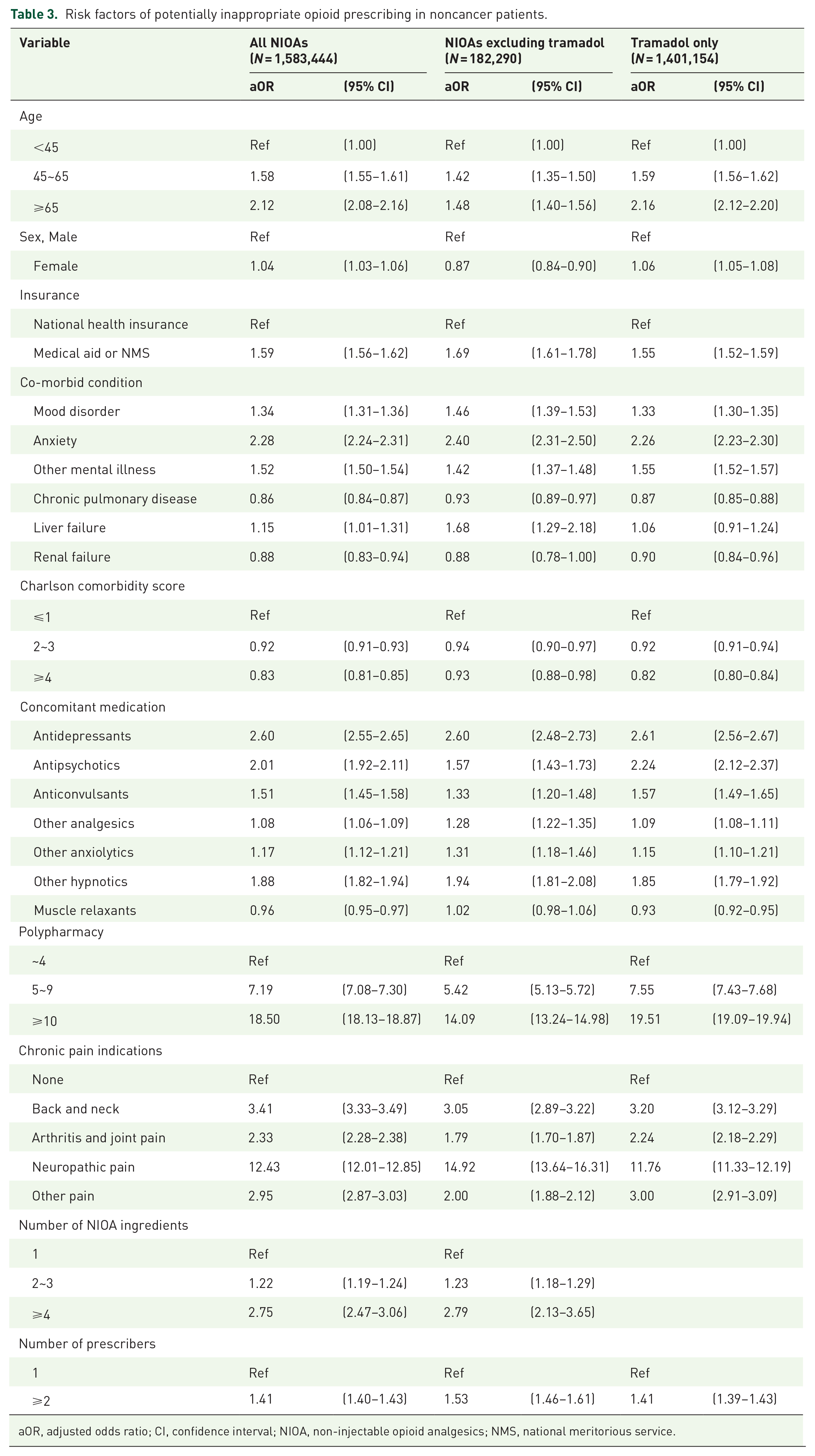
aOR, adjusted odds ratio; CI, confidence interval; NIOA, non-injectable opioid analgesics; NMS, national meritorious service.
Discussion
In this study, we comprehensively assessed the long-term prevalence of opioid use and PIOP in noncancer patients in Korea. Opioid misuse, overdose, and disorder continue to be global public health crises. Compared with the prevalence of opioid use in other countries, especially North American countries, the prevalence in Korea is relatively low.27,28 Because of the low prevalence, thus far, there was no urgent need to investigate medical opioid consumption and the subsequent risk of misuse in Korea. However, we noted the continuously increasing prevalence of NIOA use in noncancer patients. A recently published study by Cho et al. confirmed that overall opioid outpatient prescription rates have risen over the past 11 years. This recent study provided consistent evidence of the alarming opioid use in South Korea but did not consider a more specific investigation for PIOP, which is more closely linked to opioid-related harm. 7 When the current situation and problems related to opioid use are identified, preventive measures can be proactively considered. This study, which focuses specifically on inappropriate opioid use in noncancer patients, has additionally identified the risk factors associated with inappropriate opioid prescribing.
Our results suggest that the overall prevalence of NIOA use between 2012 and 2018 was 16.2%. Despite the relatively low prevalence of NIOA use, we found an upward trend over this 7-year period in noncancer patients. Our results also showed that the major reason for NIOA use in noncancer patients was physical pain, such as back and neck pain, arthritis, and joint pain. These results are consistent with recent trends in the acceptance of opioid use for the management of chronic physical pain.29,30 These trends raise concern about the possibility of chronic opioid use in patients with physical pain. Unlike cancer or postoperative pain, chronic back or arthritis pain often persists for years, which could result in long-term opioid use and increase the risk of opioid dependence and disorder.31,32 Furthermore, there is a lack of evidence regarding the benefits of long-term opioid treatment for chronic physical pain. Previous studies revealed that chronic users of opioids for noncancer pain still show persistently high levels of pain, a poor quality of life, and significant safety concerns.33,34
In a previous study based on data for 2003–2013, Kim et al. 6 reported a marked increase in tramadol consumption (relative change: +67.3%). In contrast, our results based on relatively recent data (2012–2018) showed an increase of only 1.1-fold over 7 years in the number of tramadol users, which implies that the increasing trend has almost reached its peak. However, unlike the number of tramadol users, the number of non-tramadol NIOA users increased steeply, by 1.5-fold, during the same period. Another notable trend was the decline in tramadol use in the elderly group (age ⩾ 65 years), while an increase was observed in the use of non-tramadol NIOAs. In addition, we observed a marked increase in potentially inappropriate prescription of non-tramadol NIOAs in this population. This is a concern, as it has been reported that elderly patients are more vulnerable to nonfatal and fatal respiratory events with opioids. 35
Notably, the findings in our study suggest that chronic pain is highly associated with an increased risk of PIOP. In particular, an elevated risk was found in patients with neuropathy. A systematic review and meta-analysis recognized that a higher risk of opioid misuse was associated with neuropathic pain than with other chronic pain conditions. 36 Despite our results being consistent with those of prior studies, the associated ORs in our study were extraordinarily high. However, caution is advised when interpreting this finding, because our definition of PIOP included concurrent use of gabapentinoids, which are among the first-line agents used for the management of neuropathic pain. Nevertheless, combining gabapentinoids with opioids is a critical problem, which might increase the abuse potential of opioids and potentially cause life-threatening interactions. A previous study reported a significantly higher risk of death from an opioid overdose associated with concomitant use of gabapentinoids and opioids. 24
Polypharmacy is one of the factors most associated with PIOP. Several studies conducted in Korea have demonstrated that polypharmacy is highly associated with inappropriate medication use and drug–drug interactions.37,38 Regarding polypharmacy, the risk analyses showed a tendency toward increased risks with significantly higher ORs associated with PIOP in users of more than 5 or 10 medications. However, we could not rule out the possibility of reverse causation, that is, polypharmacy due to PIOP. Patients using opioid analgesics are more likely to take multiple drugs, because opioid users tend to have multimorbid health conditions. 39 In addition, the ‘prescribing cascade’ of opioids may have contributed to an increase in the number of prescribed medicines. 40 Patients with PIOP may require additional medications because of the side effects of opioids, such as nausea, dizziness, and constipation.
Psychological disorders, especially depression, are closely linked to opioid misuse or disorder. Previous studies reported that depressed patients not only initiated opioid therapy more often than non-depressed patients but also were twice as likely to transition to long-term use even at lower intensity levels of pain.41 –43 Furthermore, the risk of opioid use disorder in patients with psychological disorders was twice as high as that in those without psychological disorders. 44 Consistent with prior studies, our study demonstrated that patients with mood disorders or anxiety were more likely to be prescribed opioids inappropriately. In addition, beneficiaries of medical aid and NMS were one of the contributing factors that increased the risk of PIOP. Our study results were consistent with those of other studies showing a higher prevalence of opioid misuse and disorder in uninsured and low-income adults. 28 Because pain management requires comprehensive and multidisciplinary care, alternative pain relief options remain out of reach for patients who need medical aid. This suggests that financial disadvantage could be associated with PIOP.
This study has some limitations. First, because of the nature of the claims database, we could not consider some well-known sociodemographic risk factors of inappropriate opioid prescribing, such as smoking behavior and alcohol consumption, which may increase the likelihood of inappropriate opioid use. Furthermore, we could not identify individuals’ pain intensity, which could be a possible confounder by mediating the selection and duration of analgesics prescribed. Second, because patients’ records could only be checked for up to a year, the prevalence of chronic opioid use may have been underestimated in patients who started opioids in the latter half of the year. Third, because this study had a cross-sectional design, we could not determine causal inferences or temporal relationships. Therefore, we cannot exclude the potential for reverse causality. Fourth, the effects of neuropathic pain and anxiety disorder on PIOP could have been overestimated because of our definition of PIOP. Because gabapentinoids are the first-line agents for the management of neuropathic pain and benzodiazepines are widely used for treating anxiety disorders, patients with neuropathic pain or anxiety disorder are more likely to have used such medications. For instance, an abnormally high risk of neuropathic pain for PIOP may result from this issue (aOR: 12.43; 95% CI: 12.01–12.85).
Conclusion
In Korea, although the insurable doses of opioids and days of supply are limited for noncancer pain, the prevalence of NIOA use is continuously increasing, as is the proportion of PIOP among NIOA users. This trend was consistent and steeper even after the exclusion of tramadol use. We also identified several important risk factors associated with PIOP, such as older age, medical aid or NMS beneficiaries, presence of psychological disorders, polypharmacy, and chronic pain indications. To safely use opioids, healthcare providers should be aware of the potential risk factors of PIOP and avoid them if possible. Considering the high vulnerability of the elderly or medical aid beneficiaries and the high proportion of PIOP in these subgroups, strategies such as targeting these populations to evaluate the need for opioids and future health outcomes of opioid treatment could be safe ways to manage the appropriate use of opioids.
Supplemental Material
sj-docx-1-taw-10.1177_20420986221091001 – Supplemental material for Trends in potentially inappropriate opioid prescribing and associated risk factors among Korean noncancer patients prescribed non-injectable opioid analgesics
Supplemental material, sj-docx-1-taw-10.1177_20420986221091001 for Trends in potentially inappropriate opioid prescribing and associated risk factors among Korean noncancer patients prescribed non-injectable opioid analgesics by Yoojin Noh, Kyu-Nam Heo, Yun Mi Yu, Ju-Yeun Lee and Young-Mi Ah in Therapeutic Advances in Drug Safety
Footnotes
Author contributions
Conflict of interest statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by National R&D Program through the National Research Foundation of Korea (NRF) funded by the Korea government (MSIP; Ministry of Science, ICT & Future Planning; no. NRF-2019R1G1A1011055).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.