
Abstract
Background:
Patients with diabetic kidney disease (DKD) are at an increased risk of frailty. The exposure to muscle relaxants frequently leads to adverse effects despite their modest therapeutic efficacy, but whether muscle relaxants predispose users to frailty remains unclear.
Methods:
Patients with DKD from a population-based cohort, the Longitudinal Cohort of Diabetes Patients, were identified between 2004 and 2011 (N = 840,000). Muscle relaxant users were propensity score-matched to never-users in a 1:1 ratio based on demographic features, comorbidities, outcome-relevant medications, and prior major interventions. Incident frailty, the study endpoint, was measured according to a modified FRAIL scale. We used Kaplan–Meier analyses and Cox proportional hazard regression to analyze the association between cumulative muscle relaxant use (⩾ 28 days) and the risk of incident frailty.
Results:
Totally, 11,637 users and matched never-users were enrolled, without significant differences regarding baseline clinical features. Cox proportional hazard regression showed that patients with DKD and received muscle relaxants had a significantly higher risk of incident frailty than never-users [hazard ratio (HR) 1.26, 95% confidence interval (CI) 1.04–1.53]. This increase in frailty risk paralleled that in cumulative muscle relaxant dosages (quartile 1 versus 2 versus 3 versus 4, HR 0.91 versus 1.22 versus 1.38 versus 1.45, p = 0.0013 for trend) and in exposure durations (quartile 1 versus 2 versus 3 versus 4, HR 1.12 versus 1.33 versus 1.23 versus 1.34, p = 0.0145 for trend) of muscle relaxants.
Conclusion:
We found that cumulative muscle relaxant exposure might increase frailty risk. It is prudent to limit muscle relaxant prescription in patients with DKD.
Plain language summary
Keywords
Introduction
Frailty, a degenerative syndrome characterized by the accumulation of subclinical deficits across multiple domains accompanying chronological or biological aging, emerges as an important public health concern worldwide. 1 Exhibiting the frailty phenotype predisposes older adults to an increased risk of functional impairment, disability, hospitalization/institutionalization, and mortality in the long run. 2 Similar influences can be found in populations with disease-associated accelerated aging, such as those with diabetes mellitus (DM), chronic kidney disease (CKD), and diabetic kidney disease (DKD). Indeed, clinicians in endocrinology and nephrology fields increasingly recognize that the incidence of frailty rises evidently in patients with DM and CKD, among whom the presence of frailty introduces adverse functional and overall outcomes.3,4 From this perspective, a prompt detection of frailty and the reduction/amelioration of risk factors associated with frailty assumes priority during both geriatric care and potentially specialty-based care.
A substantial heterogeneity in the incidence of frailty has been observed in at-risk populations, including those with DM and CKD, and this variation likely results from an inadequate understanding of under-recognized risk factors. 5 A prior review identified multiple non-conventional risk factors for CKD-associated frailty, including dialysis-related vascular access types, education status, and serum testosterone levels; 6 diabetic complications and the status of glycemic control also influenced the risk and severity of DM-associated frailty. 7 We previously discovered that gustatory dysfunction and subclinical vascular morbidities could be potential modifiers of the risk of frailty among older adults with and without CKD.8,9 Polypharmacy is also a putative contributor to frailty; however, very few studies currently evaluate the risk of frailty introduced by specific medication type(s).
Muscle relaxants are a heterogenous class of medications frequently harnessed to treat musculoskeletal conditions, including but not limited to truncal or limb physical pain, headache of various etiologies, and myofascial pain syndrome. 10 They serve as a useful adjunct to acetaminophen or non-steroidal anti-inflammatory drugs (NSAIDs) for the management of discomfort with a musculoskeletal origin. Prior studies disclosed that muscle relaxants were more likely to be prescribed for relieving back pain compared with NSAIDs or cyclo-oxygenase-2 inhibitors, 11 supporting their popularity among physicians who treated related discomfort; however, their adverse effects are less commonly appreciated by prescribers. A meta-analysis of 30 trials involving muscle relaxants identified that their exposure was associated with a doubled risk of central nervous system disturbance compared with non-users, 12 and the risk might increase with a longer duration of exposure. Furthermore, it has been shown that cognitive impairment and physical frailty share common pathogenic machineries, 13 and subjective cognitive decline is pinpointed as an independent predictor of frailty. 14 These scenarios are expected to be more frequent in patients with DKD, which increases the susceptibility to frailty. Consequently, we hypothesized that muscle relaxant exposure, when prolonged, in patients with DKD might place them at risk of developing incident frailty. We then utilized a population-based cohort of diabetic patients with CKD to test and verify this hypothesis.
Methods
Identification of study participants and the enrollment procedure
The current study was performed based on enrollees assembled from the Longitudinal Cohort of Diabetes Patients (LCDP), a population-based cohort receiving prolonged follow-up using the claim dataset. We identified those recruited between 2004 and 2011, and imposed a stringent criterion for recognizing DM by requiring ⩾3 times of out-patient diagnosis or ⩾1 time of in-patient diagnosis. 15 Those with DKD were further extracted from diabetic participants by excluding those without a CKD diagnosis prior to enrollment. Exclusion criteria included pediatric patients (age ⩽20 years), those with missing demographic data, and those with the outcome of interest (frailty) prior to the index date, defined according to the date when participants satisfied both the diagnosis of DM and CKD. Clinical variables, including demographic data, lifestyle factors, comorbidities, and treatment variables, were recorded from all enrollees prior to the index date. Comorbidities were identified if the diagnosis was made prior to the index date. Treatment variables were defined according to procedure codes within 1 year prior to the index date. For relevant medications, we defined users as those having at least one prescription record between the index date and the end of follow-up or the development of outcomes. To allow an adequate period for baseline data ascertainment and for observation of outcome development, we further excluded those with an index date prior to 1 January 2004 or those starting their follow-up after 31 December 2010.
Participants with DKD subsequently underwent selection according to whether they received cumulative muscle relaxants exposure. Users were propensity score-matched to those who did not receive any muscle relaxants throughout the study period, in a 1:1 ratio, based on demographic features (age, sex, lifestyle factors, comorbidities, medications, prior major interventions, and the number of FRAIL variables). Users and never-users were prospectively followed up until the development of frailty (the outcome of interest), death, or 31 December 2011, whichever occurred first. In our cohort established based on the LCDP database retrospectively, participants were continuously followed up during the study period.
Ascertainment of muscle relaxant exposure
The types of muscle relaxants identified in this study were based on the existing literature, including anti-spasmodic benzodiazepines and non-benzodiazepines, as well as anti-spasticity agents (Supplemental Table online). 16 Several types of anti-spasmodic benzodiazepines and non-benzodiazepines were unavailable in Taiwan (cinolazepam, flutoprazepam, halazepam, ketazolam, loprazolam, pinazepam, quazepam, tetrazepam, and metaxalone) and therefore were unselected. We defined cumulative muscle relaxant use as those who consumed at least one type of medicine for ⩾28 days within the preceding year of the index date, a strategy utilized by other pharmacoepidemiology studies.17,18
Frailty as the primary outcome of interest
We assessed frailty based on modifications of the FRAIL scale to screen for frailty among study participants, using the operational criteria described previously.4,19,20 In brief, there are five components in the original FRAIL scale (Fatigue, Resistance, Ambulation, Illness, and Loss of body weight). 21 The component of Fatigue is ascertained based on patients’ self-report experience of chronic fatigability, while Resistance is deemed positive if patients are unable to climb at least 10 steps without resting. The component of Ambulation is deemed positive if patients are unable to walk several hundred yards alone. The component of Illness is recognized if patients have at least five out of 11 comorbidities, while the component of Loss of weight becomes positive if patients have at least 5% of weight loss within 1 year. We operationalized each of these components using close morbidities and phenotypes available from our dataset based on diagnostic code combinations available from the LCDP database, due to the fact that the LCDP database did not contain interview information, physical examination or laboratory data. The exact codes harnessed to operationalize each component of the FRAIL scale have been delineated in our prior work. 19 These codes are selected after a rigorous process of extensive literature review followed by rounds of expert meeting and consensus reaching. 19 This approach has been adopted repetitively in the existing literature.4,19,20
According to the original construct, those with ⩾3 out of the five components were deemed frail, while those with <3 components were considered non-frail. The results of FRAIL scale have been shown to correlate closely with those of other established frailty-screening instruments such as Cardiovascular Health Study scale and frailty index,22,23 and a greater severity of FRAIL-identified frailty predicts a significantly increased risk of incident disability and mortality. The applicability of FRAIL scale has also been tested and validated in a population with similar ethnicity and in patients with DM and/or CKD.24,25
Statistical analysis
For continuous variables, we described them in means with standard deviations and compared results between two groups by the Student’s t-test. Categorical variables were described in numbers with percentages, and compared between groups by the Chi-square test. After identifying muscle relaxant users and propensity score-matched never-users, we first compared the clinical features, including demographic profiles, comorbidities, severity of DM, relevant medications, and prior treatment variables between these two groups. We also compared the baseline FRAIL component count and prevalence between groups. Subsequently, we used Kaplan–Meier analyses and Cox proportional hazard regression models to examine the relationship between cumulative muscle relaxant use and the risk of incident frailty, incorporating variables outlined above. We also analyzed the dose- and duration-dependent effect of muscle relaxant use on the risk of frailty in these participants. The association between different subtypes of muscle relaxants and the risk of incident frailty was examined as well. Several sensitivity analyses were arranged. First, we performed another Cox regression analysis to account for the influences of other muscle relaxant indications [muscular disorders including muscle cramping; International Classification of Diseases 9th version – Clinical Modification (ICD-9-CM) code 728.xx] and any opioid use. 26 In addition, we further examined the risk of frail severity transition according to the baseline frailty status; that is, we analyzed the risk of turning frail among participants who were robust (no FRAIL component) or pre-frail (1 – 2 FRAIL components), and the risk of turning pre-frail among participants who were robust, using multiple logistic regression. Another analysis was arranged to evaluate the relationship between muscle relaxant use and overall survival. For all statistical analyses, STATA version 14 (Stata Corp., College Station, TX, USA) was used. A p value lower than 0.05 was deemed statistically significant.
Ethics statement
The protocol of this study was approved by the institutional review board of National Taiwan University Hospital (NO. 201802063W) as a subanalysis. The implementation of this study adhered to the Declaration of Helsinki. Informed consent was deemed unnecessary by the review board, since all data from the current dataset were anonymized prior to being collected and analyzed.
Results
During the study period, totally 840,000 patients with at least one time of DM diagnosis were identified; after applying the exclusion criteria outlined in Figure 1, we included 157,466 patients with DKD for further analysis. Among these patients, we further selected those who were chronic muscle relaxant users (n = 41,448) and those who had never received prescriptions of muscle relaxants (n = 33,586) (Figure 1), followed by a propensity score-matching process between users and never-users, yielding 11,637 cases and matched controls. There were no significant differences between muscle relaxant users and never-users with regard to their demographic features, lifestyle factors, comorbidity profiles and Charlson comorbidity indices, diabetic severity (using the adapted Diabetes Complications Severity Index 27 ), medications (anti-diabetic ones and others), or prior major procedures (Table 1).
Characteristics of patients with diabetic kidney disease receiving muscle relaxants and matched never-users.

Based on the adapted Diabetes Complications Severity Index.
ACEi, angiotensin-converting enzyme inhibitor; ARB, angiotensin receptor blocker; CCI, Charlson Comorbidity Index; CKD, chronic kidney disease; COX, cyclo-oxygenase; IQR, interquartile range; NSAID, non-steroidal anti-inflammatory drug.
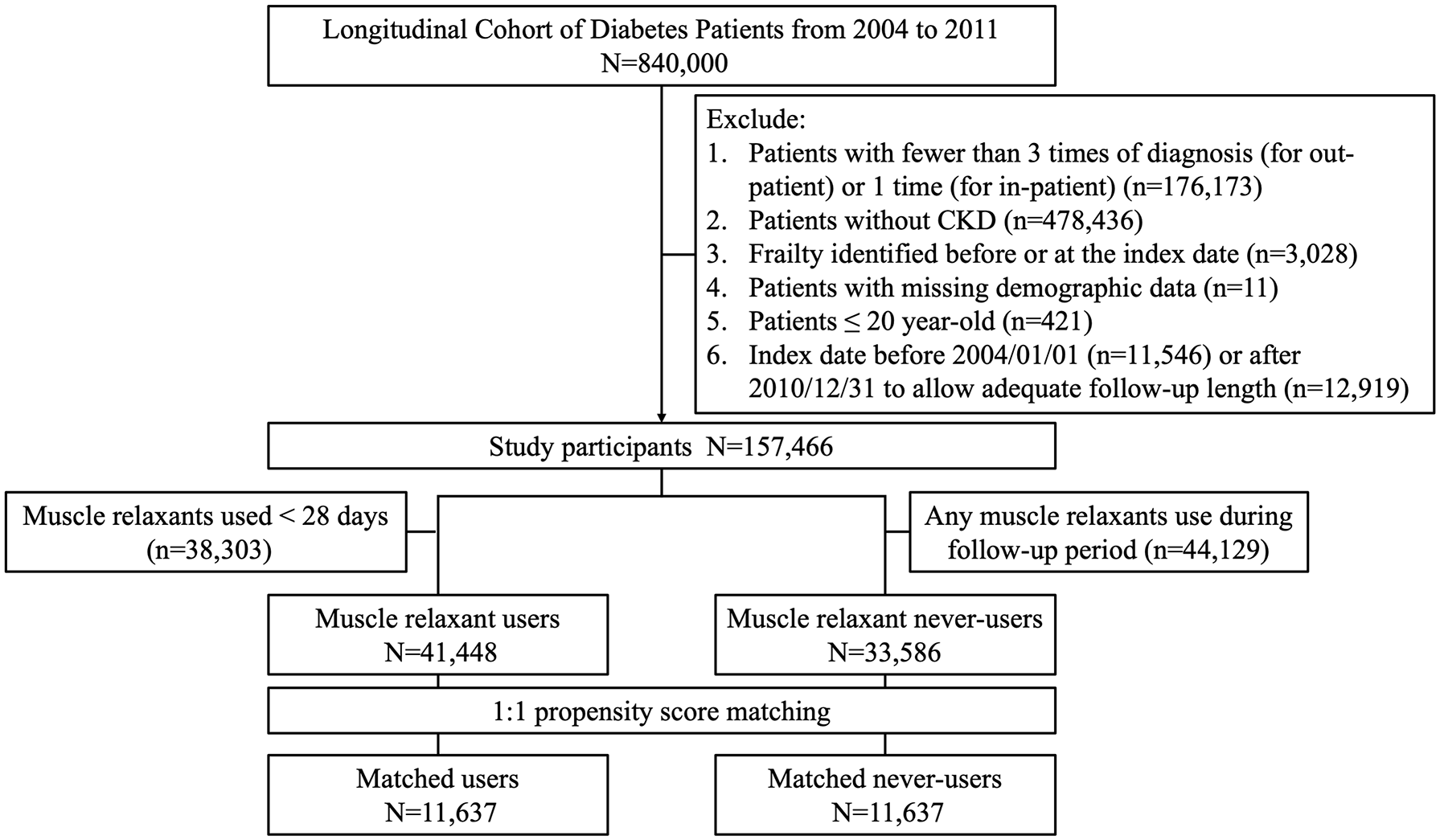
The algorithm of participant selection in this study.
We also compared the prevalence and number of positive FRAIL components between muscle relaxant users and never-users (Table 2). There was no significant difference between users and never-users regarding the proportion of participants without and with 1, 2 FRAIL components, as well as the proportion of having each positive component, except the Illness component (Table 2).
FRAIL components depending upon muscle relaxant use or not.

FRAIL, Fatigue, Resistance, Ambulation, Illness, and Loss of body weight.
We subsequently evaluated the association between muscle relaxant use and the risk of developing incident frailty, after a mean 2.53 years of follow-up with a frailty incidence rate of 1.84%. Among 23,274 muscle relaxant users and matched never-users with DKD, the former exhibited a trend of higher incident frailty compared with the latter. Cox proportional hazard regression showed that muscle relaxant users with DKD had a significantly higher risk of developing frailty than never-users [hazard ratio (HR) 1.26, 95% confidence interval (CI) 1.04–1.53], independent of all clinical variables and FRAIL component prevalence/numbers (Table 3). If we divided the users’ cumulative dose into quartiles, higher doses of muscle relaxant use were accompanied by a progressively rising risk of incident frailty (quartile 1 versus 2 versus 3 versus 4, HR 0.91 versus 1.22 versus 1.38 versus 1.45 compared with never-users, p = 0.0013 for trend) (Table 3). A similar phenomenon was observed if we divided the duration of exposure into quartiles (1 versus 2 versus 3 versus 4, HR 1.12 versus 1.33 versus 1.23 versus 1.34 compared with never-users, p = 0.0145 for trend) (Table 3). If we analyzed the risk according to subtypes of muscle relaxants, anti-spasmodic benzodiazepines and anti-spasticity agent users exhibited a significantly higher risk of frailty compared with never-users, while anti-spasmodic non-benzodiazepines did not (Table 3). Sensitivity analyses additionally adjusting for muscular disorders (the indication of muscle relaxant use) and opioid use still identified a significant association between muscle relaxant use and the risk of frailty in these patients (HR 1.28, 95% CI 1.05–1.55) (Table 3). Muscle relaxant users who were robust prior to the index date had a significantly higher risk of turning pre-frail compared with non-users [odds ratio (OR) 1.18, 95% CI 1.02–1.35] (Table 4). However, the risk of turning frail among users who were robust (OR 1.69, 95% CI 0.51–5.62) and pre-frail (OR 1.15, 95% CI 0.94–1.4) compared with non-users was insignificant, owing to low event numbers (Table 4). Finally, analyses addressing the association between muscle relaxant use and mortality showed that users were at a higher risk of mortality than never-users (p < 0.01) (Figure 2), and Cox proportional hazard regression revealed the same findings (HR 1.15, 95% CI 1.10–1.20). We also compared the median time to frailty development between muscle relaxant users and non-users. The median time to frailty development in users and non-users was 0.85 (0.23, 1.81) and 0.74 (0.32, 1.86) years, respectively, without significant difference (p = 0.624).
Risk of developing frailty according to muscle relaxant use depending upon the doses, durations of use, and subtypes.

p < 0.05.
p < 0.01.
p < 0.001.
Per 1000 patient-years.
Incorporating age/gender, lifestyle factors, all comorbidities, aDCSI, all medications, treatment variables, positive FRAIL component prevalences and numbers.
Model A additionally adjusted for muscle cramping and the use of any opioid.
aDCSI, adapted Diabetes Complications Severity Index; CI, confidence interval; HR, hazard ratio.
Risk of frail severity transition according to muscle relaxant use.

Per 100 persons.
Incorporating age/gender, lifestyle factors, all comorbidities, adapted Diabetes Complications Severity Index, all medications, treatment variables, and frail severity transition variable.
a, p < 0.05; b, p < 0.01; CI, confidence interval; OR, odds ratio.

Kaplan–Meier survival curves of muscle relaxant users and never-users (controls).
We also analyzed data among study participants in both groups who developed frailty during follow-up (n = 428), with regard to the proportion of having at least one FRAIL item during the period between the time of frailty development and the end of follow-up. We found that only 29.4% of frail patients subsequently did not have any FRAIL item during the post-event period, suggesting that the rate of frailty reversal was relatively low in this study.
Discussion
In this study, we conducted a population-based longitudinal study to examine the effect of muscle relaxant exposure on the risk of frailty among 23,274 patients with DKD. Cumulative muscle relaxant use was significantly associated with an increased risk of incident frailty, and the relationship became more prominent with longer duration of use and higher cumulative dosages. Based on our findings, it may be prudent to limit the prescriptions of muscle relaxants in patients with DKD and at risk of frailty, preferably to a short-term basis only and using as lower dosages as possible.
According to a recent large-scale survey, the rate of prescribing skeletal muscle relaxant, regardless of purposes, nearly doubled between 2005 and 2016 in United States; 28 what is more worrisome is that the number of new prescriptions for muscle relaxant during the study period remained static, while the number of continued prescriptions tripled, suggesting that prolonged exposure to muscle relaxants becomes common. This is further compounded by the high probability of opioid co-prescription (~67%), 28 which likely enhances the risk of adverse events associated with muscle relaxant use. Muscle relaxants have already been listed as a class of potentially inappropriate medication in the Beers list. Based on the literature results and our findings, the gradual increase in the global prevalence and incidence of frailty may be partially explained by the cumulative exposure to muscle relaxants among susceptible populations including those of advanced age and with DKD, although other factors can play a role as well.
There are several potential reasons responsible for the observed association between cumulative muscle relaxant exposure and a higher risk of frailty in this study. First of all, it is well established that the receipt of muscle relaxants is associated with dizziness, lightheadedness, and consciousness disturbance, 10 all of which may elevate the risk of frailty through overlapping pathogenesis such as vascular insufficiency, hormonal alterations, chronic inflammation, and nutritional impairment. 29 The frequent co-prescription of muscle relaxants with other pain relievers, including opioids or their derivatives, also introduces side effects such as central nervous system suppression. 30 This is particularly problematic in those with CKD; for example, baclofen confers a higher risk of encephalopathy in patients with CKD. 31 In addition, the direct effect of therapeutic muscle relaxant use, the relief of painful skeletal muscle contraction, may simultaneously raise the probability of decreasing muscular activities involving uninflamed muscles. This unwanted phenomenon can lead to postural imbalances, functional impairment, and disability if prolonged neuromuscular weakness occurs. A recent study further shows that the use of muscle relaxants potentially aggravates esophageal motility and causes ineffective swallowing; 32 this phenomenon can compromise ones’ nutritional status and predispose them to frailty. Third, several muscle relaxants, such as tizanidine, have been found to cause hemodynamic instability through their hypotensive effect, 33 which is augmented if combined with other cytochrome P450-modifying medicines. Besides, chronic muscle relaxant use is associated with an increased risk of sensory dysfunction such as vision blurring. 10 Emerging studies discovered that certain muscle relaxants might pathologically increase acoustic reflex thresholds and render hearing apparatus vulnerable to noise, through weakening the stapedial muscle. 34 The multi-pronged negative effects posed by muscle relaxants may account for the risk of frailty they bring. A brief summary of these plausible mechanisms is illustrated in Figure 3.
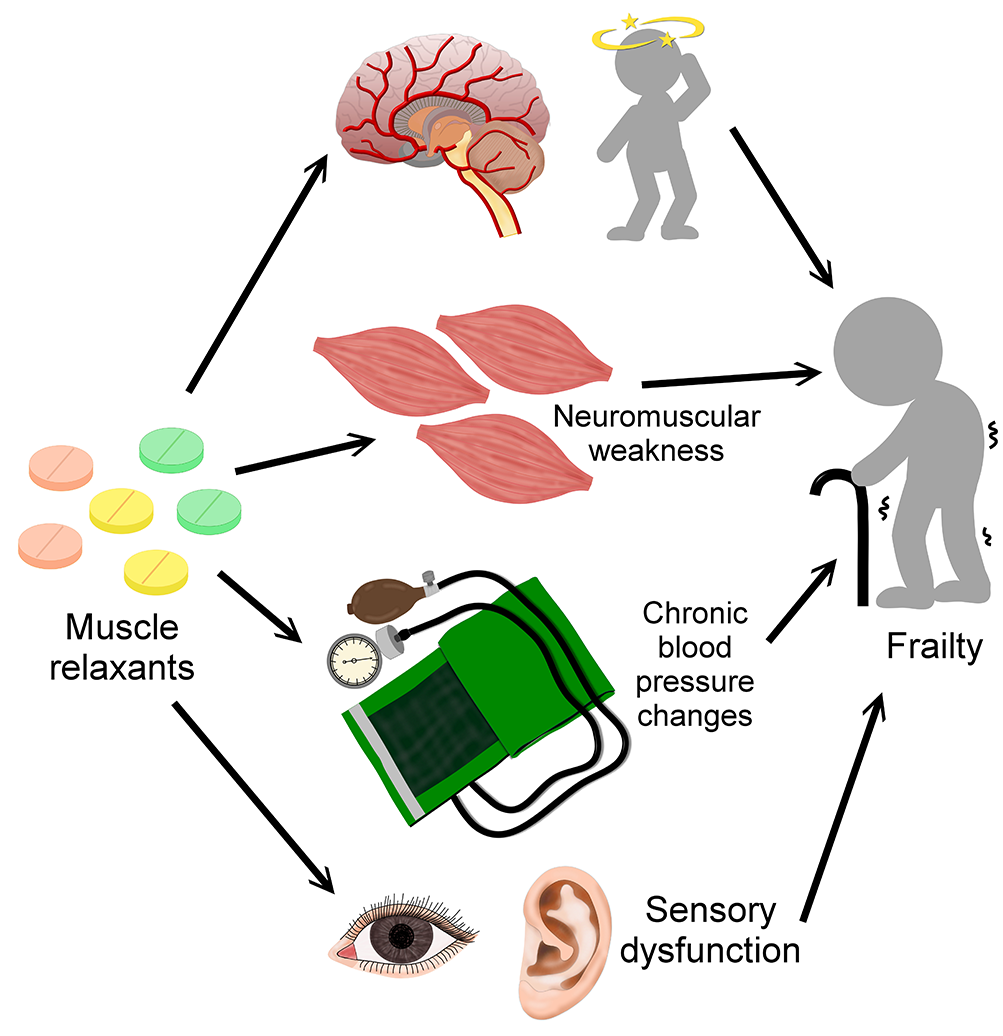
An illustrative diagram depicting the plausible mechanisms between muscle relaxant exposure and incident frailty.
The risk of frailty associated with muscle relaxant use prompts the consideration of deprescribing these medications in vulnerable populations; however, this practice is uncommon and not easily achievable. Mechanical intervention and cognitive motivational counseling have been found to be useful strategies to reduce muscle relaxant prescriptions. It may also be useful to learn from other deprescribing approaches for similar pain-relieving medications such as opioids, including physician re-education, guideline establishment, inter-disciplinary collaboration, et cetera. 35
Our study has its strengths and weakness. The large size and population-based nature of our cohort as well as the balanced distribution of all clinical confounders render our findings unlikely to be biased. The spectrum of muscle relaxants identified in this study is comprehensive and encompasses all available types according to the literature. Our findings in patients with DKD have been rarely addressed before in the literature and are highly informative. However, several issues warrant consideration before interpreting our results. First, we did not include those with short-term muscle relaxant use (<28 days), and the influence of short-term muscle relaxant exposure on the risk of frailty was unclear. Second, the mean follow-up duration of this cohort might not be long enough to permit an accurate estimation of long-term frailty risk. Moreover, the size of effect might vary depending on the population being tested. Third, the assessment of frailty was based on the operationalization of each FRAIL item using administrative code combinations instead of in-person examinations. Fourth, there might be un-identified factors that influenced our findings but were not collected by the LCDP database. The retrospective nature of this study might preclude us from drawing definite conclusions. Finally, the incidence of frailty might alter if other frailty measurement strategies are adopted. More reports are needed in the future to verify our findings.
Conclusion
In conclusion, using a population-based cohort of patients with DKD, we showed that cumulative exposure to muscle relaxants might increase the risk of incident frailty, independent of conventional frailty risk factors such as demographic profiles, morbidities, medications, and major therapeutic events. Longer durations and higher cumulative dosages significantly elevate the risk, supporting the biologic plausibility of the relationship between muscle relaxant use and frailty. Judging from our findings, it may be prudent for patients with DKD to decrease their chances of receiving muscle relaxants, in order to lessen their probability of developing frailty.
Supplemental Material
sj-doc-1-taw-10.1177_20420986211014639 – Supplemental material for Muscle relaxant use and the associated risk of incident frailty in patients with diabetic kidney disease: a longitudinal cohort study
Supplemental material, sj-doc-1-taw-10.1177_20420986211014639 for Muscle relaxant use and the associated risk of incident frailty in patients with diabetic kidney disease: a longitudinal cohort study by Szu-Ying Lee, Jui Wang, Hung-Bin Tsai, Chia-Ter Chao, Kuo-Liong Chien and Jenq-Wen Huang in Therapeutic Advances in Drug Safety
Footnotes
Acknowledgements
We are grateful to the Second Core Laboratory, Department of Medical Research of National Taiwan University Hospital and the National Taiwan University Center of Genomic and Precision Medicine for their technical input. Sponsors’ role: the sponsors have no role in the study design, data collection, analysis, and result interpretation of this study.
Author contributions
Study design: CTC, JW, JWH; data analysis: SYL, CTC, JW, KLC; article drafting: SYL, HBT, CTC, JW, JWH, KLC; all authors approved the final version of the manuscript.
Availability of data and material
The raw data for conducting this analysis are unavailable due to administrative regulations.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study is financially sponsored by National Taiwan University Hospital BeiHu Branch (11001) and Ministry of Science and Technology, Taiwan (MOST 109-2314-B-002-193-MY3)
Ethics statement
The study protocol has been approved by the institutional review board of National Taiwan University Hospital (NO. 201802063W) as a subanalysis.
Informed consent
Informed consent was deemed unnecessary due to participant anonymization prior to analysis of this population database, as adjudicated by the review board.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.