
Abstract
Background:
Along with the increasing use of immune checkpoint inhibitors comes a surge in immune-related toxicity. Here, we review the currently available data regarding neurological immune adverse events, and more specifically aseptic meningitis and encephalitis, and present treatment and diagnostic recommendations. Furthermore, we present five cases of immunotherapy-induced aseptic meningitis and encephalitis treated at our institution.
Recent findings:
Neurological immune-related adverse events, including aseptic meningitis and encephalitis, secondary to checkpoint inhibitors are a rare but complex and clinically relevant entity, comprising a wide range of diseases, most often presenting with symptoms with a wide range of differential diagnoses. Our case-series highlights the challenges of such entities and the importance of properly identifying and managing aseptic meningitis and encephalitis.
Summary:
Checkpoint inhibitor-induced meningoencephalitis warrants prompt investigations and treatment. Properly diagnosing aseptic meningitis, encephalitis, or mixed presentations may guide the treatment decision, as highlighted by our case-series. After rapid exclusion of alternative diagnoses, urgent corticosteroids are the therapeutic backbone but this could change in favour of highly specific cytokine-directed treatment options.
Plain language summary
Over the course of the past decade, checkpoint inhibitors have revolutionized cancer care. With their favourable toxicity profile and potential for durable and deep responses, they have become ubiquitous across the field of oncology. Furthermore, combination checkpoint inhibitors are also gaining ground, with increased efficacy and, unfortunately, immune-related toxicity. While there are guidelines based on extensive clinical experience for frequent adverse events, uncommon entities are less readily identified and treated. Neurological immune-related adverse events secondary to checkpoint inhibitors are a rare but complex entity, comprising a wide range of diseases, most often presenting with aspecific symptoms. In this paper, we discuss a single institution case-series of patients with autoimmune aseptic meningitis and encephalitis, and we perform a narrative literature review on this subject. We conclude with our treatment recommendations based on available evidence.
Keywords
Introduction
Over the course of the past decade, immune checkpoint inhibitors (ICIs) have revolutionized medical oncology, with hitherto unseen long-term, durable responses and improved overall survival. Modern ICIs are divided into two main categories: anti-cytotoxic T lymphocyte antigen-4 (CTLA4) antibodies (such as ipilimumab and tremelimumab) and antibodies targeting the programmed death 1 (PD-1) axis, including anti-PD-1 (pembrolizumab, nivolumab, cemiplimab) and its ligand (anti-PD-L1; durvalumab, atezolizumab, avelumab). Others are under development and may soon affect the treatment landscape. 1
Since their initial use in melanoma, ICIs have rapidly gained ground, expanding to metastatic non-small cell lung cancer (NSCLC), urothelial cancer, and many other cancer types.2,3 While initially investigated as monotherapy, ICI combinations have proven their efficacy and have already become front-line options in melanoma and kidney cancer.4,5 The possibility to combine chemotherapy with ICIs has further expanded the indications of these drugs, ensuring that virtually all fit patients with metastatic NSCLC and head and neck squamous cell carcinoma could be exposed to front-line ICIs,6–9 with the exception of most patients with actionable mutations.10–12 Advanced or metastatic urothelial carcinoma management has also been modified, with ICIs being used as second-line therapy, and recently also in the maintenance setting after first-line chemotherapy. 13 ICIs are also explored in the neoadjuvant setting in some tumour types 14 (ClinicalTrials.gov identifiers: NCT03425643 and NCT03158129).
ICIs are globally considered safer than chemotherapy, because of lower rates of grade 3 or 4 adverse events. Nevertheless, they are not without risk, with potential serious immune-related adverse events (irAEs), with an estimated 2% of treatment-related mortality. 15 Neurological immune-related adverse events (NAEs) secondary to checkpoint inhibitors are a rare but complex entity, comprising a wide range of diseases, most often presenting with nonspecific symptoms. In this paper, we analyse currently available data about aseptic meningitis and encephalitis and summarize all known cases of these adverse events, including those in our centre. We conclude with management recommendations for checkpoint inhibitor-induced aseptic meningitis and encephalitis.
Methods
We searched PubMed with the following keywords for all available cases reported in English (“immune checkpoint inhibitor”, “ipilimumab”, “nivolumab” “pembrolizumab”, “atezolizumab”, “durvalumab”, “neurologic toxicities”, “neurologic immune-related adverse events”, “meningitis”, “encephalitis”, “ meningoencephalitis”). We also collected all cases of aseptic meningitis or/and encephalitis among patients treated with ICIs from our immunotoxicity board. We identified five cases between 2015 and 2019, described below (Table 1).
Autoimmune meningoencephalitis case reports from Geneva and the literature.

Ab, antibody; AE, adverse event; ASCT, autologous stem cell transplantation; atezo, atezolizumab; C, cycle; cc, cell count; cemi, cemiplimab; chemo, chemotherapy; CNS, central nervous system; CR, complete response; CT, computed tomography; d, day; DD, differential diagnosis; dexa, dexamethasone; EBV, Epstein Barr virus; EEG, electroencephalogram; EGFR, Epidermal Growth Factor Receptor; F, female; FLAIR, Fluid-attenuated inversion recovery; FU, follow up; GCS, Glasgow coma scale; gr, grade; GVHD, graft versus host disease; h, hour; HCB, haematocephalic barrier; HRT, hormone replacement therapy; ICI, immune checkpoint inhibitor; Ipi, ipilimumab; irAE, immune-related adverse event; i.v., intravenous; IVIG, i.v. immunoglobulin; JC, John Cunningham virus; lambro, lambrolizumab; LP, lumbar puncture; ly, lymphocytes; M, male; methylpred, methylprednisolone; MRI, magnetic resonance imaging; MSI, microsatellite instability; NAE, neurological adverse event; nivo, nivolumab; NSCLC, non-small cell lung cancer; PCI, prophylactic brain irradiation; PD, progressive disease; PR, partial response; pembro, pembrolizumab; RCC, renal cell carcinoma; SCLC, small-cell lung cancer; SD, stable disease; St, stage; UK, unknown; w, week; WBRT, whole-brain radiotherapy; yo, year old.
For the narrative literature review, we used the sources found on PubMed with the above search, as well as data from international guidelines.
Cases
First case: a 46-year-old woman with metastatic (liver and peritoneum) uveal melanoma started ipilimumab at 3 mg/kg. After two cycles, she developed headaches with episodes of fainting. Blood tests found inaugural central hypothyroidism, which quickly led to panhypopituitarism. This immune-related grade 2 hypophysitis was treated with methylprednisolone and hormone replacement therapy.
After effective hormonal replacement and a switch to hydrocortisone, the ICI treatment was resumed. After the fourth cycle, the patient developed headaches with bilateral hearing loss, nausea and grade 3 asthenia. She was subfebrile and described morning dizziness. At admission, she had static cerebellar syndrome.
A brain magnetic resonance image (MRI) showed regressive sequelae of hypophysitis, without secondary lesions or bleeding.
A lumbar puncture (LP) demonstrated pleiocytosis with 91% of lymphocytes, elevated protein level, and normal cytology and flow cytometry. After the LP, antibiotics (ceftriaxone) and antivirals (acyclovir) were started with pulse intravenous methylprednisolone.
The Gram stain and viral polymerase chain reaction (PCR) tests were negative and corresponding treatments were stopped. Onco-neuronal antibodies were not detected. The diagnosis of grade 3 aseptic meningoencephalitis was retained.
After 48 h of corticosteroids, the patient was afebrile, and hearing loss and dizziness began to improve. A second LP reported a decreasing pleiocytosis and normal protein levels.
Given the positive clinical course occurring 7 days after intravenous (i.v.) steroids, they were replaced with oral prednisone and slowly tapered. After 5 weeks, despite ongoing prednisone, she presented recurring headaches, bilateral hearing loss and ataxia, with fever.
No brain MRI or LP was repeated, but 4 days before the symptoms reappeared, a LP showed a rise in central spinal fluid (CSF) lymphocytes and protein levels. Corticosteroids were increased and antibiotic and antiviral treatments resumed, with no improvement after 4 days. Bacterial cultures and viral PCRs were negative, allowing to a further increase in steroid dose finally leading to a slow positive evolution. Infliximab was considered but not given, and steroids were maintained for 4 weeks then tapered over 4 weeks.
Ipilimumab was permanently discontinued, and the patient had a partial response for 2 years. Upon progression, she was treated with pembrolizumab (2 mg/kg every 3 weeks) without any neurological adverse events. ICIs were stopped at disease progression. The patient died 8 months after the initiation of this last line of treatment.
Second case: a 70-year-old man was diagnosed with metastatic (lung) renal clear cell carcinoma. He had a left radical nephrectomy and splenectomy, and begun treatment with a combination of nivolumab 1 mg/kg and ipilimumab 3 mg/kg within a clinical trial. At 5 days after his first cycle, he developed increasing neck pain, followed by fever, and finally confusion, gait disturbance and aphasia.
At day 10, he was admitted with fever, confused speech, neck stiffness and gait disturbance. An LP showed pleiocytosis with elevated lymphocytes and high protein levels. The brain scan was normal and the interpretation of the brain MRI was limited because of the patient’s agitation, but suggested ventriculitis.
Empiric treatment with acyclovir, amoxicillin and ceftriaxone was stopped when the Gram stain, culture and viral PCR results came back negative. Dexamethasone allowed for a rapidly favourable clinical course: he became afebrile, and his gait and speech improved. At 8 days after admission, a regimen of oral prednisone was initiated and the patient went home.
Steroid tapering was complicated by several recurrences of neck pain, nausea and fever of unknown origin. Prednisone was maintained at 15 mg daily for two more months and weaned over 7 months for this grade 4 immune-related meningoencephalitis. Due to the grade of the complication and according to the trial rules, no ICIs were reintroduced.
It is interesting to note that after only one cycle, the cancer was controlled for 7 months, at which point a second-line treatment with pazopanib was introduced, with an ongoing good partial response at last follow-up.
Third case: a 44-year-old woman with relapsed metastatic (muscle, skin and liver) colorectal adenocarcinoma with microsatellite instability initiated ipilimumab 1 mg/kg and nivolumab 3 mg/kg. After three cycles, she developed fever, followed by headaches, photophobia and anorexia. On admission the clinical exam was normal, except for fever. LP demonstrated a pleiocytosis with lymphocytosis, and elevated protein levels.
Acyclovir and amoxicillin were given until CSF analyses came back negative for infection, while methylprednisolone, initiated concurrently with anti-infectious treatments, was continued. Oral prednisone was started on day 3, after the fever and symptoms improved. It was slowly weaned over 6 weeks. At this point, in an asymptomatic patient who had rapidly responded to therapy, while there was a risk of relapse of the grade 3 aseptic meningitis, the potential treatment benefit outweighed the risk. Nivolumab was reintroduced, with a good response. The patient is still on treatment and has not experienced a recurrence or any new NAE.
Fourth case: an 82-year-old man with an history of stage IIA early favourable Hodgkin’s lymphoma, initially treated with two lines of chemotherapy, presented a second recurrence 4 years after the initial diagnosis. Given his good clinical condition and lack of important comorbidities, he was started on pembrolizumab at a 200 mg flat dose. At 10 days after the first dose, his wife noted progressively increasing confusion, impaired speech, and gait disturbance. On admission, he had fever, a Glasgow coma score (GCS) of 14/15, with confusion and unstable gait. The brain scan was normal for his age. LP revealed lymphocytic pleiocytosis with elevated protein level. Antibiotics (ceftriaxone and amoxicillin) and antivirals (acyclovir) were administered until CSF analyses came back negative. The concurrent methylprednisolone was continued.
A few days after the LP, a brain MRI showed multiple leptomeningeal contrast enhancements, compatible with aseptic meningitis. At 1 day after the initiation of steroids, the patient became afebrile and gradually regained normal gait and cognition in the following days. Steroids were weaned over the course of 3 months.
Because of this grade 3 immune-related meningoencephalitis, ICIs were not reintroduced. Moreover, 2 months after the single cycle of treatment, the patient had a complete radiological and metabolic response. Since then, the patient has remained asymptomatic and has been under surveillance.
Fifth case: a 70-year-old female smoker with stage II chronic obstructive pulmonary disease was diagnosed with a neuroendocrine small cell lung cancer (SCLC) with metastatic cervical nodes. Because of a poor performance status and an intercurrent infection, her first chemotherapy cycle consisted of carboplatin AUC5 alone, allowing for an improvement in her performance status. The next three cycles consisted of carboplatin AUC5 and etoposide, combined with atezolizumab 1200 mg.
At 2 days after the fourth cycle, she was admitted to the emergency room for disorientation and visual hallucinations, with an otherwise normal neurological exam. The brain MRI was compatible with limbic encephalitis, with a bilateral abnormal signalling in the hippocampus. The LP found pleiocytosis and high protein levels, and was negative for infection, so antimicrobial treatments were stopped. An electroencephalogram (EEG) showed encephalopathy with an epileptic focus on the left side, leading to the introduction of lacosamide, with rapid EEG improvement.
From day three after therapy, she received high-dose corticosteroids, but remained disoriented. Anti-Hu antibodies were found in the CSF, leading to a differential diagnosis of paraneoplastic encephalitis versus autoimmune encephalitis on atezolizumab. Natalizumab (anti-integrin) was considered, but rituximab was initiated a week later, leading to improvement in her memory and a second cycle of rituximab 2 weeks later. In parallel, steroids were slowly tapered until 10 mg/d.
At 2 months later, she presented with confusion. The brain MRI showed likely recurrence of limbic encephalitis, and the thoraco-abdominal computed tomography (CT)-scan showed disease stability. Corticosteroids were raised to 1 mg/kg/d, and rituximab was given every 6 months, while i.v. immunoglobulins were administered every 4 weeks. The memory problems did not resolve and upon progression 4 months later, she received palliative care and died 4 months later.
Discussion
Immune-related adverse event pathogenesis
ICIs cause an overstimulation of the immune system, increasing the risk of immune-mediated toxicity. While the precise physiopathology remains unknown, there are multiple hypotheses about the underlying mechanism for developing irAEs. One of them, the “hidden autoimmunity theory”, relies on the previous existence of subclinical autoantibodies, even at a low level or “hidden” by immune-tolerance. ICIs may disrupt this equilibrium, triggering an autoimmune reaction.52,53 While there is an estimated 27–42% risk of exacerbating a pre-existing autoimmune disease with ICIs, there are currently no predictive markers for the incidence or severity of the reaction. 23 Moreover, given the inherently greater risk of irAEs in these groups, patients with autoimmune disease or history of transplantation (solid organ or stem cells) are excluded from most prospective ICI trials, limiting available data to retrospective series and case reports. For instance, in a series of 22 patients with kidney transplant, half experienced rejection when challenged with ICIs. 54 Likewise, among patients previously treated with allogenic hematopoietic stem cells transplantation, ICIs increase the risks of graft versus host disease and mortality. 55 These are very selected populations but highlight that ICIs should not be viewed as innocuous. Benefits and potential complications must be discussed and evaluated with each patient.
In daily practice, there may also be a higher incidence of irAEs in high-tumour-mutational-burden diseases, such as NSCLC and melanoma, due to the greater number of neoantigens in these cancer types, leading to cross-reactivity with self-antigens, also known as the “molecular mimicry theory”.53,56,57 The site of cancer can also lead to an increased cross-reactivity with other organs in which antigens are more similar to those in the tumour sites. 58
The physiopathology of irAEs can vary depending on the affected organ. For NAEs, the main explanation relies on onconeural peptides that are released during cancer cell death. They trigger the formation of onconeural autoantibodies, potentially leading to organ damage. 59 Classical paraneoplastic syndromes (PNSs), such as Ma2-associated syndromes, have drastically increased with the use of ICIs. 60 Similarly, it is unknown whether the presence of onconeural autoantibodies, without any accompanying PNS, as can be detected in around 16% of patients with SCLC, increases the risk of developing NAEs with ICI therapies. 59 Investigations are ongoing to evaluate whether underlying germline factors or bacterial flora may affect the host immunity and the response and toxicity to ICIs. 55 In preclinical studies, interleukin (IL)-1, one of the main cytokines in the acute phase of inflammation, has been shown to be central in the pathogenesis of autoimmune encephalitis, by enhancing the differentiation of IL-17-producing T lymphocytes. 61 In checkpoint inhibitor-induced aseptic meningitis, contrarily to encephalitis, onconeural antibodies have not been shown to play a role. Interestingly, brain radiotherapy does not increase the risk of NAEs. 62
While there is no shortage of hypotheses, we are currently unable to predict who will develop irAEs, which organ will be targeted and when. Except for autoimmune disorders and transplantation, there are no identified risk factors for the development of irAEs. While it is by no means ready for clinical use in this context, artificial intelligence could provide answers. A radiomic model was described to have a strong ability to predict immunotherapy-induced pneumonitis: radiomic and pathomic biomarkers could predict irAEs in the future.63,64
The exact relationship between irAEs and response to therapy is uncertain. Some irAEs seem to correlate with a radiological response to ICIs, such as the association between developing vitiligo and responding to ICIs in melanoma, or skin toxicity and response as well as survival in NSCLC.65–67 Regarding NAEs, there are very limited data, based on small and uncontrolled observations, suggesting an increase in objective response rate (ORR) in patients who developed NAEs (ORR 50–70%) compared with those who did not (20–30%). 23
The relationship between the use of corticosteroids and outcomes in patients receiving ICIs is not fully understood but the available data seem to demonstrate that immunosuppressive therapies for irAEs do not attenuate their efficacy, but rather that steroid use at treatment initiation is a negative prognostic factor reflecting a poor prognosis subgroup.55,68
The incidence of irAEs and neurological irAEs
In a recent meta-analysis comprising 125 clinical trials of single-agent PD-1 or PD-L1 inhibitors, involving 20,128 patients, irAEs were reported in 66% of patients, with 14% grade 3 or higher. 24 With anti-CTLA4 antibodies, irAEs develop in 60% to 85% of patients, with 10% to 29% of grade 3 or higher.2,69 The combination of anti-CTLA4 (ipilimumab) and anti-PD-1 (nivolumab) antibodies increases the risk of irAEs, with adverse events reported in 95% of patients, with 55% of grade 3 or higher. 69
Every organ can be affected, but cutaneous (pruritus in 10.61% and vitiligo in 3.26% of patients), gastrointestinal (diarrhoea in 9.47% of patients) and endocrine (hypothyroidism in 6.07% of patients) irAEs are most frequent. 24
NAEs are uncommon, developing in roughly 2–6% of patients receiving single-agent ICIs. However, with combined PD-1 and CTLA4 inhibition, this rises to 12%.70,71 For PD-1 inhibition alone, an early onset of symptoms a few days after treatment is common, but NAEs can also develop after several weeks of treatment. 72
As NAEs can present with a wide range of symptoms, some of which are easily attributed to the cancer itself (fatigue, weakness, headache, dizziness), they can be difficult to diagnose and are likely underestimated. As with other irAEs, NAEs most often present as grade 1–2 toxicity, comprising mainly headaches (55%), dysgeusia (13%) and dizziness (10%). The incidence of serious (⩾grade 3) NAEs is below 1%, and this encompasses a highly heterogeneous spectrum of neurological symptoms.57,71,73,74 Even if any-grade NAEs are more frequent with PD-1/PD-L1 antibodies (6.1%) than with anti-CTLA4 (3.8%), anti-CTLA4 seem to confer a higher risk for serious (grade 3–4) NAEs (0.7%) than anti-PD-1/PD-L1 antibodies (0.4%). 71 Aseptic meningitis or encephalitis develops in 0.1–0.2% of patients on ICIs. 23
While irAEs mostly develop between 3 and 6 months after treatment initiation, NAEs arise slightly more rapidly, with a median time to NAE of three cycles (6–9 weeks) of treatment. 2 In a Japanese ICI safety trial, aseptic meningitis developed shortly after ICI initiation (21–32 days), 75 and some cases were even described within the first weeks of treatment. 23
Interestingly, non-neurological irAEs could precede NAEs, and a careful history is also mandatory when suspecting an NAE. 76
Aseptic meningitis and encephalitis
The clinical manifestations of NAEs are broad, can be atypical, and encompass overlapping syndromes. Peripheral involvement appears to be more common than central, with peripheral neuropathy representing up to two-thirds of all NAEs, possibly linked to previously administered neurotoxic chemotherapy. 52 Other neurological conditions reported are myopathy/myositis, myasthenic syndrome, encephalopathy/encephalitis, aseptic meningitis, myelitis, Guillain–Barre-like syndrome, as well as immune-related PNSs.
It is important to correctly evaluate the patient for any neurological symptoms and deficits before initiating ICI therapy. Subsequently, any new neurological disorder during or after ICIs should be suspected to be a NAE, and a comprehensive differential diagnosis should investigated and ruled out. In these rare and potentially serious situations, investigations and therapies must rely on an experienced multidisciplinary team.
In aseptic meningitis, the clinical presentation can mimic an infectious meningitis with headache, neck stiffness, vomiting, photophobia and fever. However, it is likely that only one or two of these symptoms are present. Encephalitis can also be aspecific, but it differs from aseptic meningitis in that it includes altered cognition or abnormal cerebral function. 77
One key aspect is that there can be overlapping presentation. It is important to distinguish, whenever possible, meningitis from encephalitis, as their pathogenesis and management are not strictly identical. However, they usually share the same initial workup and are sometimes grouped together under the term of meningoencephalitis. 16
Currently, as we note in our case-series and literature review, almost all cases of encephalitis have concurrent findings of meningitis. The term meningoencephalitis can be viewed as encephalitis, as opposed to pure aseptic meningitis, in which there is no sign of encephalitis (such as confusion).
The workup must rule out an infectious or metabolic cause. First, taking a medical history, evaluating current medication, and a clinical exam are critical. Then a blood test should explore any metabolic abnormalities or signs of infection.
A brain MRI is used to rule out vascular events and (progressing) metastases. Meningeal enhancement appears in half the cases of aseptic meningitis, though its absence does not preclude the diagnosis. Parenchymal enhancement can also be found in encephalitis. Non-ICI-related autoimmune encephalitis may have a normal MRI in up to 60% of cases, so imagery should not rule out this diagnosis. 17
An LP can detect an elevated opening pressure and must include cell count, chemistry, cytology, viral PCR (including Herpes simplex, Varicella zoster, enterovirus, Cytomegalovirus, Parechovirus), bacterial direct exam (Gram staining) and cultures, and flow cytometry in the case of a haematological malignancy. With aseptic meningitis, CSF typically reveals lymphocytic pleiocytosis, elevated protein levels, and normal glucose levels. The viral and bacterial screening is negative.
Positive onconeural antibodies help to diagnose neurologic PNSs; however, their presence is not always associated with PNSs,18,19 and when antibodies are detected in light of neurological symptoms in patients on ICIs, we do not know whether we are facing a classical neurological PNS or an immune-related NAE mimicking one. The “hidden autoimmunity theory”, cited above, would suggest the symptoms are NAEs, as they are not compatible with the usual presentation of PNSs, with symptoms developing before the underlying cancer detection and subacute onset. 59
Detailed examples of initial workup results can be seen in our report of all cases reported in the literature, including the five cases identified in our institution from 2015 to 2019 (Table 1).
The initial workup will have some specificity depending on the clinical presentation. For suspected aseptic meningitis, the brain MRI and the blood examination can rule out hypophysitis and explore adrenal function (MRI with a pituitary protocol, and blood cortisol and adrenocorticotropic hormone (ACTH)). For suspected encephalitis, an EEG is necessary to detect subclinical seizures. 20
Even if all of the above-cited investigations are normal, aseptic meningitis and autoimmune encephalitis cannot formally be ruled out, thus remaining a challenging diagnosis.
The management of aseptic meningitis and encephalitis
Management guidelines for NAE, including aseptic meningitis and encephalitis, exist.20,21 These guidelines are based on expert consensus, institutional experience, and review of literature and are continuously being updated.
All irAE therapy recommendations are based on case reports, expert consensus and very rare and small prospective trials. By analogy with other irAEs, it is assumed that early recognition and aggressive treatment of aseptic meningitis and encephalitis could provide a rapid response and decrease possible residual symptoms or complications.
Some physicians believe that any NAE should be considered as grade 3 or 4, given its potential to induce severe neurological impairment. 59 However, most guidelines suggest different management protocols according to the grade of the toxicity.20,21
In grade 1 NAEs, ICIs could be continued with close monitoring. In grade ⩾2 NAE, ICIs should be withheld. Corticosteroids should be introduced rapidly, the dose and route of administration depending of the NAE severity: for grade 2, oral prednisolone (0.5–1 mg/kg/d), for grade 3–4, i.v. methylprednisolone (1–2 mg/kg/d).15,20,22,57 It is important to note that hours to days might be necessary before definitive results of viral PCR and bacterial exams are available, so concurrent antivirals and antibiotics should be administered until infection has been ruled out.
There is usually a clinical response within the first 24 h, with no or very few sequelae. Nonetheless, the mortality rate is 5–11% 52 for encephalitis.25,26
For encephalitis only, in case of severe or progressing symptoms in spite of up to 2 mg/kg steroids, pulse corticosteroids (i.v. methylprednisolone 1 g/d for 3–5 days), sometimes associated with i.v. immunoglobulins (0.4–2 g/kg/d) might be necessary. If there is no improvement in the first 48–72 h under corticosteroids, this “steroid-refractory” situation may require other immunosuppressive drugs, such as rituximab or infliximab, and plasmapheresis may be considered.20,27,28
After a favourable clinical course, steroids are generally maintained at a high dose for 2 weeks, then slowly tapered over at least 4–6 weeks, because of the long half-life of ICIs. If the symptoms relapse, high-dose corticosteroids are reintroduced. If corticosteroid weaning is impossible, steroid-sparing therapies such as rituximab, infliximab, or cyclophosphamide, may be added. 27
American and European medical societies have management guidelines for NAEs.20–22 Based on those, and the published outcomes, including the present case-series, we suggest recommendations for the treatment of aseptic meningitis and autoimmune encephalitis (Figures 1 and 2) (Table 1).
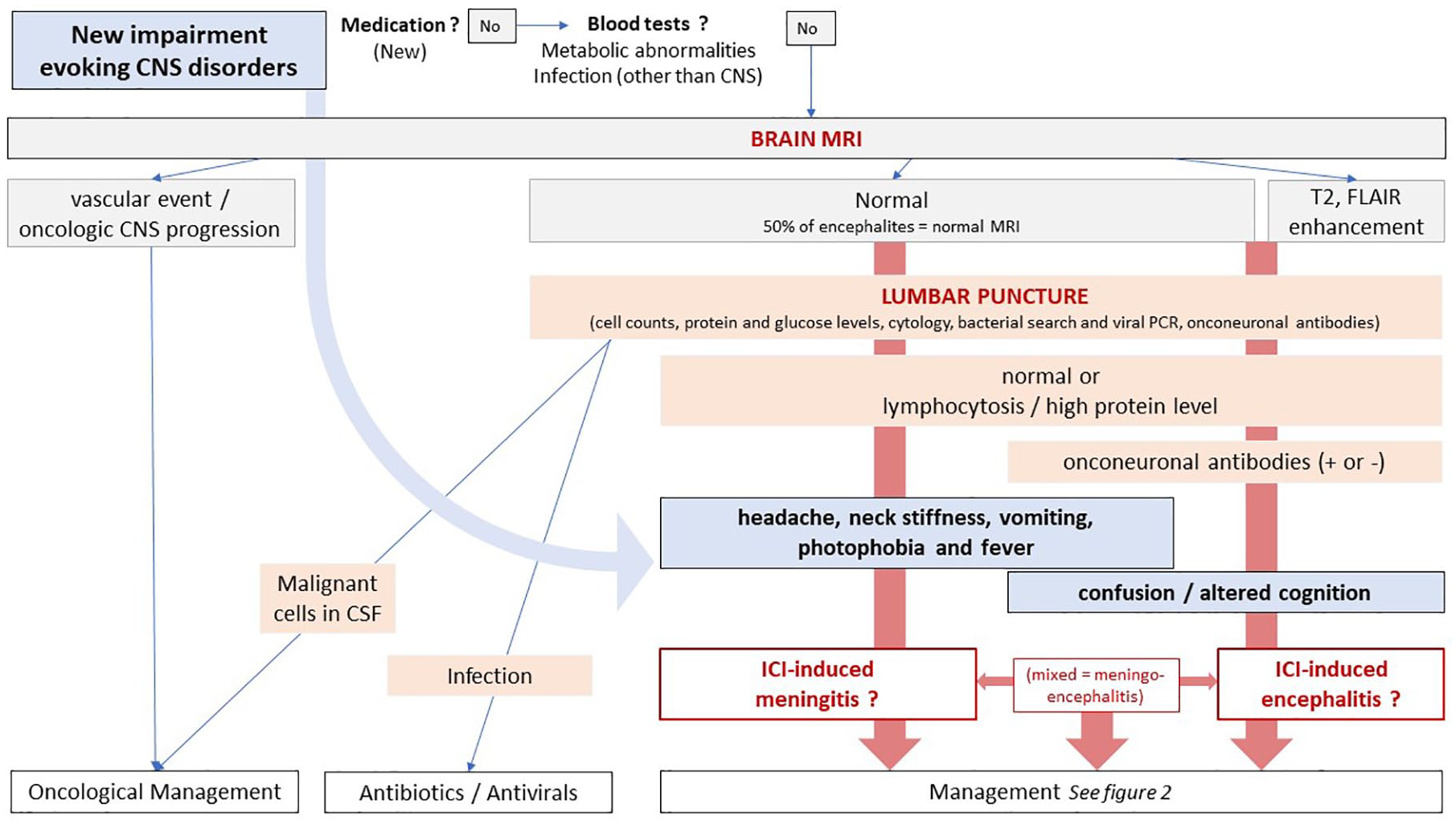
Workup of suspected checkpoint inhibitor-induced meningitis and encephalitis.
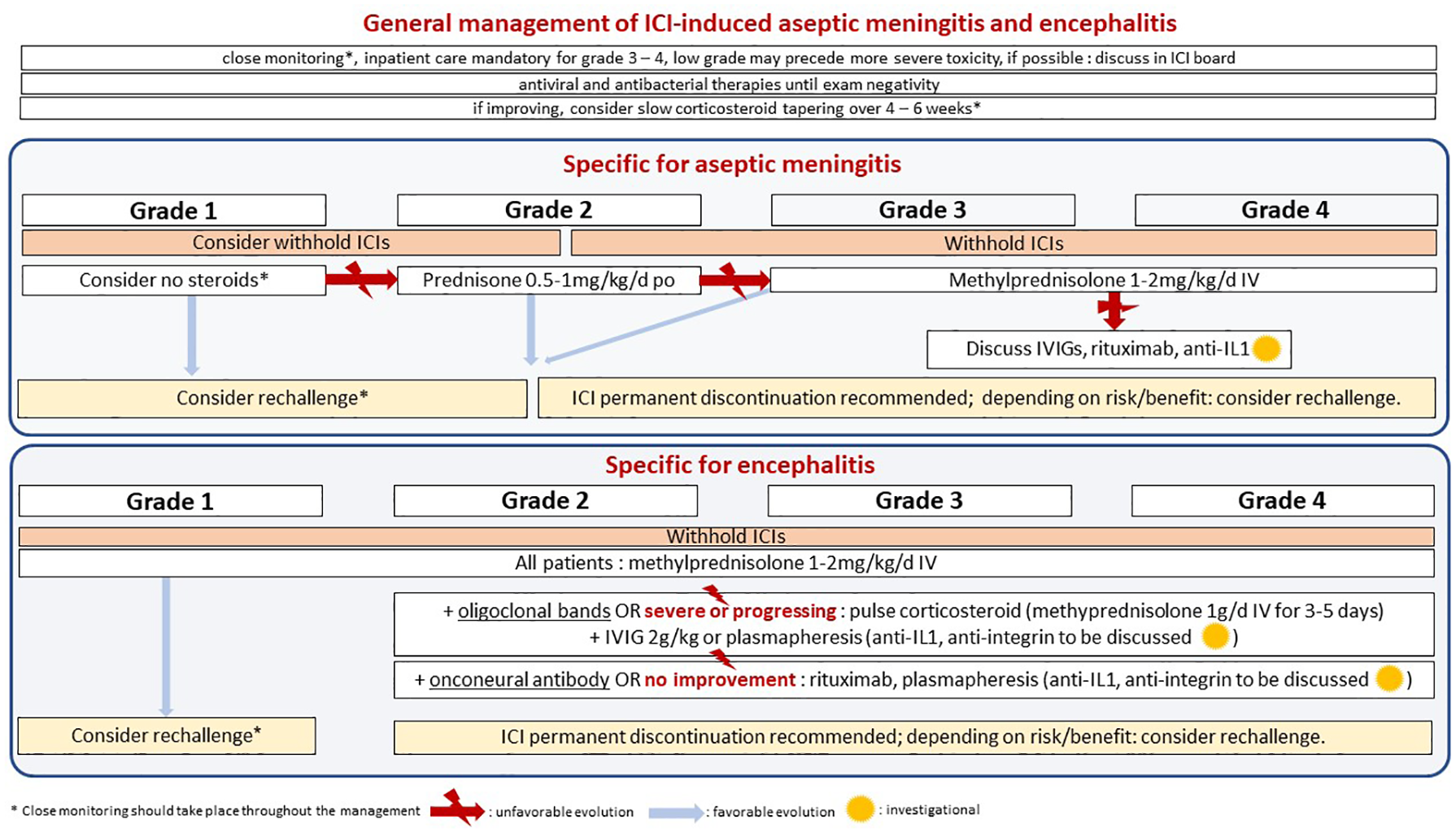
Management of checkpoint inhibitor-induced meningitis and encephalitis.
Our case-series and literature review emphasize the difficulty, to differentiate between aseptic meningitis and encephalitis. This is a major issue in daily practice. Almost all cases of encephalitis presented with signs of concurrent meningitis in their cerebrospinal fluid analysis. Whether an underlying different pathogenesis and presentation should lead to a different management is not clear, and current recommendations are mostly derived from other causes of encephalitis, including paraneoplastic encephalitis. However, data are currently lacking to deviate from such guidelines.
Recently, Martins and colleagues published specific treatment algorithms for irAEs relying on their pathogenesis and on the predominant immune infiltrate in the targeted organ, which has to be biopsied. 58 The authors evoke the possibility to treat severe irAEs with targeted cytokine-directed monoclonal antibodies or anti-integrins from the onset of symptoms, rather than using high-dose corticosteroid therapy, or to use this approach in case of poor response to steroids. For example, in aseptic meningitis and encephalitis, they suggest anti-IL-1 blockade (e.g. anakinra or canakinumab), which they suspect could be more effective than i.v. immunoglobulins or anti-CD20 antibodies (rituximab, ofatumumab, obinutuzumab, ocrelizumab). In meningitis, a neutrophilic infiltrate causes acute inflammation, partially mediated by IL-1, explaining the rationale for targeting this protein, and we have seen that IL-1 may have a central role in the pathogenesis of encephalitis.
Other strategies, such as targeting integrin 4, could be effective for meningitis and encephalitis without impairing ICI efficacy, specifically targeting lymphocyte adhesion in the blood–brain barrier. 29 A patient with NSCLC and severe anti-Hu positive encephalitis due to ICIs was successfully treated with natalizumab, an anti-integrin 4 monoclonal antibody, without impairing the oncological outcome. 30
This area of investigation could bring steroid-sparing treatments to the front-line therapy in patients who develop irAEs, with a short course of specific antibodies chosen according to the immune-infiltrate characteristics of the injured organ, obtained either by biopsy or even blood biomarkers.
In spite of their exciting biological rationale, these strategies need further clinical validation and are currently not recommended as upfront therapy, though they are discussed by immunotoxicity boards in the refractory setting.
ICI rechallenge after an irAE
After any severe irAE, including an NAE, discontinuation of ICIs is recommended, particularly for grade 3–4 NAEs. There are, however, neither clear evidence nor recommendations concerning ICI rechallenge. Retrospective data have shown that among patients with grade 2 or greater irAEs, half of patients rechallenged develop irAEs, and there is generally no increase in the severity of the event. 31 Nonetheless, the centre did not rechallenge patients with NAEs, explaining this by the fact that the consequences could be fatal. 32
Some could advocate for more caution after encephalitis than meningitis, given its potential neurological disability. However, given the lack of strong evidence or consensus, decisions should be tailored to each patient, based on the potential risks and possible benefits. 33 Among our cases, the two patients with encephalitis who were rechallenged with ICIs after grade 3 toxicity did not present recurring or new adverse events (Table 1). For this reason, we advocate for a tailored case-by-case evaluation, without restrictive rules about rechallenge decisions (Figure 2).
Conclusion
With the major therapeutic advance and ubiquitous use of ICIs comes a new class of adverse events. Of these, neurological irAEs, and more precisely aseptic meningitis, encephalitis and other central NAEs are very uncommon but may be underestimated because of nonspecific symptoms and diagnostic challenges. It is important to be aware of these entities to include them in the very first differential diagnoses and initiate appropriate treatments rapidly. Current management of NAEs is mainly based on expert opinions, with initial ICI discontinuation and high-dose steroids, with differences between aseptic meningitis and encephalitis, underlying the importance of distinguishing these two entities during initial workup, when possible. Emerging therapeutic strategies based on the underlying supposed pathogenesis (cytokines, integrins) could lead to more precise and steroid-sparing therapies and need to be studied. With these new strategies under investigation, a multidisciplinary approach, with the integration of clinical and paraclinical findings, can help in the treatment decision-making process, as highlighted within our case-series.