
Abstract
Background:
Anticholinergic burden (ACB) is a recognised risk factor for falls in older people; however, whether ACB in middle age predicts falls in later life is unknown.
Methods:
We examined this association in the middle-aged women of the Aberdeen Prospective Osteoporosis Screening Study (APOSS). ACB was calculated at the second health visit (1997–1999, study baseline) using the Anticholinergic Cognitive Burden Scale. Outcomes were incidence of 1 fall and recurrent falls (⩾2 falls) during the 12 months prior to follow up 2007–2011. Multinomial logistic regression analyses adjusted for potential confounders including demographics, comorbidities and falls history.
Results:
A total of 2125 women {mean age (standard deviation [SD]): 54.7 (2.2) years at baseline and 66.0 (2.2) years at follow up} were included. Prevalence of baseline ACB score of 0, 1 and ⩾2 was 87.1%, 7.3% and 5.6%, respectively. Compared with no ACB, ACB ⩾2 was associated with recurrent falls in the previous 12 months [adjusted odds ratio (OR): 2.34, 95% confidence interval (CI): 1.31, 4.19] at an average of 11 years after initial exposure. No such association was found for an ACB score of 1.
Conclusions:
These findings highlight the potential negative effects of anticholinergic medications in middle age. While cautious use of anticholinergic medications is advisable, further longitudinal research should be conducted to confirm these findings before any specific clinical recommendations can be made.
Lay summary
In this paper we describe the link between medicines that block the chemical acetylcholine and falls in later life in women. We used data from a large study in Scotland and we found that there may be a link between such medicines and recurrent falls in later life.
Introduction
Falls are the leading cause of both nonfatal and fatal injuries in older people (those aged 65 years and over). 1 Around one-third of older adults living in the community and more than half of nursing home residents fall each year, with 30% of these falls resulting in serious injury (an injury severity score > 15).2–4 Whilst only 1% of falls lead to hip fracture, 90% of all hip fractures are a result of falling. 5 In addition to physical injury, falls are associated with loss of self-confidence, loss of independence, depression and increased rates of institutionalisation.3,6 Furthermore, falls result in significant economic burden, with an estimated falls-related expenditure in excess of £2.3 billion for the United Kingdom (UK) National Health Service (NHS) in 2013, and approximately $50.0 billion for the United States (US) health service in 2015.7,8 There are numerous risk factors for falls in older adults, with intrinsic risk factors including abnormalities with gait, balance, vision and cognition. 9 The use of certain medications is also known to increase the risk of falls, with more recent studies looking specifically at the use of anticholinergic medications as a risk factor for falls in older people.9–12 It is important to consider that falls do not affect exclusively older people. A cross-sectional study of middle-aged adults aged 46–65 years showed that 21% of participants fell in a 2-year period, experiencing the same percentage of injuries as their older counterparts aged 65 years and over. 13
Anticholinergic burden (ACB) is a term used to describe the cumulative effect of concomitant use of multiple medications with anticholinergic properties. Around half of the general population use anticholinergic medications, prescribed for medical conditions such as Parkinson’s disease and urinary incontinence.14–16 As well as falls, ACB has been associated with myriad negative sequelae in older people, including increased mortality, functional and cognitive decline and stroke.17–20 Importantly, many commonly prescribed medications that are not considered ‘traditional’ anticholinergics have been shown to have anticholinergic effects (e.g. furosemide, ranitidine and warfarin), necessitating a clear understanding of both the short- and long-term implications of prescribing these medications. 21
Despite increasing research into the adverse effects of ACB in older people, an important literature gap exists regarding the consequent effects of prescribing anticholinergic medications in middle age. Our previous work showed positive association between an ACB score ⩾2 and prevalent falls in the last year [adjusted odds ratio (OR): 1.81, 95% confidence interval (CI): 1.25, 2.62, p = 0.002] in a cross-sectional analysis of 3883 middle-aged women aged 50–62 years of the Aberdeen Prospective Osteoporosis Screening Study (APOSS) cohort. 22 To further our understanding of the long-term consequences of anticholinergic medications in middle age, we used the same middle-aged female population of the APOSS study to examine longitudinally whether ACB in middle age predicts falls or recurrent falls in later life.
Methods
Participants and study design
Participants were drawn from the Aberdeen Prospective Osteoporosis Screening Study (APOSS), for which full study design has been detailed previously. 23 In summary, 7200 women aged 45–54 years were selected randomly from a primary care register and invited to participate in an osteoporosis screening study. Of these, 5119 women attended the initial enrolment health visit between 1990 and 1994. A second health visit occurred between 1997 and 1999 (n = 3883, now aged 50–62 years) and a third between 2007 and 2011 (n = 2126, aged 60–73 years).
Physical activity data, comorbidity data and falls data were collected at the second and third health visits. Additionally, medication data were collected at the second health visit. For this present study, baseline data were collected from the second health visit (1997–1999) and follow up data from the third health visit, 2007–2011, henceforth referred to as ‘baseline health visit’ and ‘follow up health visit’, respectively. All women provided written consent to participate. The study was approved by the East of Scotland Research Ethics Service and was conducted in accordance with the principles of the Declaration of Helsinki 1964.
Data collection
Outcome of falls
The incidence of 1 fall and recurrent falls (⩾2 falls) in the 12 months before follow up were examined. Falls data were collected at the follow up health visit (2007–2011) by means of a questionnaire asking ‘Have you fallen in the last 12 months?’. If participants gave an affirmative response, a subsequent question asked the number of falls.
Medications and calculation of ACB
At the baseline health visit, 1997–1999, a self-reported list of current medications was collected. Medications with anticholinergic properties were assigned a score according to the Anticholinergic Cognitive Burden Scale (score 1 = possible anticholinergic effects; scores 2 and 3 = definite anticholinergic effects). 21 Total ACB was calculated by summing scores.
Potentially confounding covariates
At the health visits, trained nurses measured height and weight. Height was measured to the nearest 0.1 cm using a stadiometer (Holtain Ltd, Crymych, UK) with shoes removed. Weight was measured to the nearest 0.1 kg using scales (Seca, Hamburg, Germany) with participants wearing light clothing and with shoes removed. Body mass index (BMI, kg/m2) was calculated by dividing weight (kg) by the square of the height (m2). Physical activity level (PAL) was obtained by dividing total energy expenditure by basal metabolic rate. Total energy expenditure was calculated using a questionnaire asking participants about the duration and intensity of activity in a 24-h period for both working and non-working days. Detailed methodology has been previously described. 24 National deprivation category, calculated based on residential postal codes from 1997 to 1999, was used as a measure of socioeconomic status (category 1 = most affluent; category 7 = most deprived). 25 A questionnaire at baseline asked about a history of asthma, osteoarthritis, rheumatoid arthritis, diabetes mellitus, myocardial infarction, osteoporosis and stroke, amongst other comorbidities not included in this analysis. Participants were also asked whether or not they had fallen in the 12 months prior to baseline.
Statistical analyses
Statistical analyses were carried out in Stata 15.1 SE (StataCorp, College Station, TX, USA). Figure 1 shows a flow diagram of the selected participant population and summary of missing data. Missing data were imputed using multiple imputation. First, a participant with missing data for BMI and history of asthma was excluded due to perfect prediction of the variables to be imputed. Multiple imputation was performed using chained equations with 10 iterations. The following missing data were imputed: PAL (n = 252); follow up falls group (no falls, 1 fall or ⩾2 falls, n = 238); baseline falls (yes or no, n = 22); national deprivation category (n = 7); ACB (n = 2). PAL was imputed using truncated linear regression with a lower limit of zero. Baseline falls was imputed using logistic regression. Follow up falls group, national deprivation category and ACB were imputed with predictive mean matching using five neighbors. Variables included as predictors in the imputation models were: age; history of osteoarthritis; history of rheumatoid arthritis; history of asthma; and BMI.
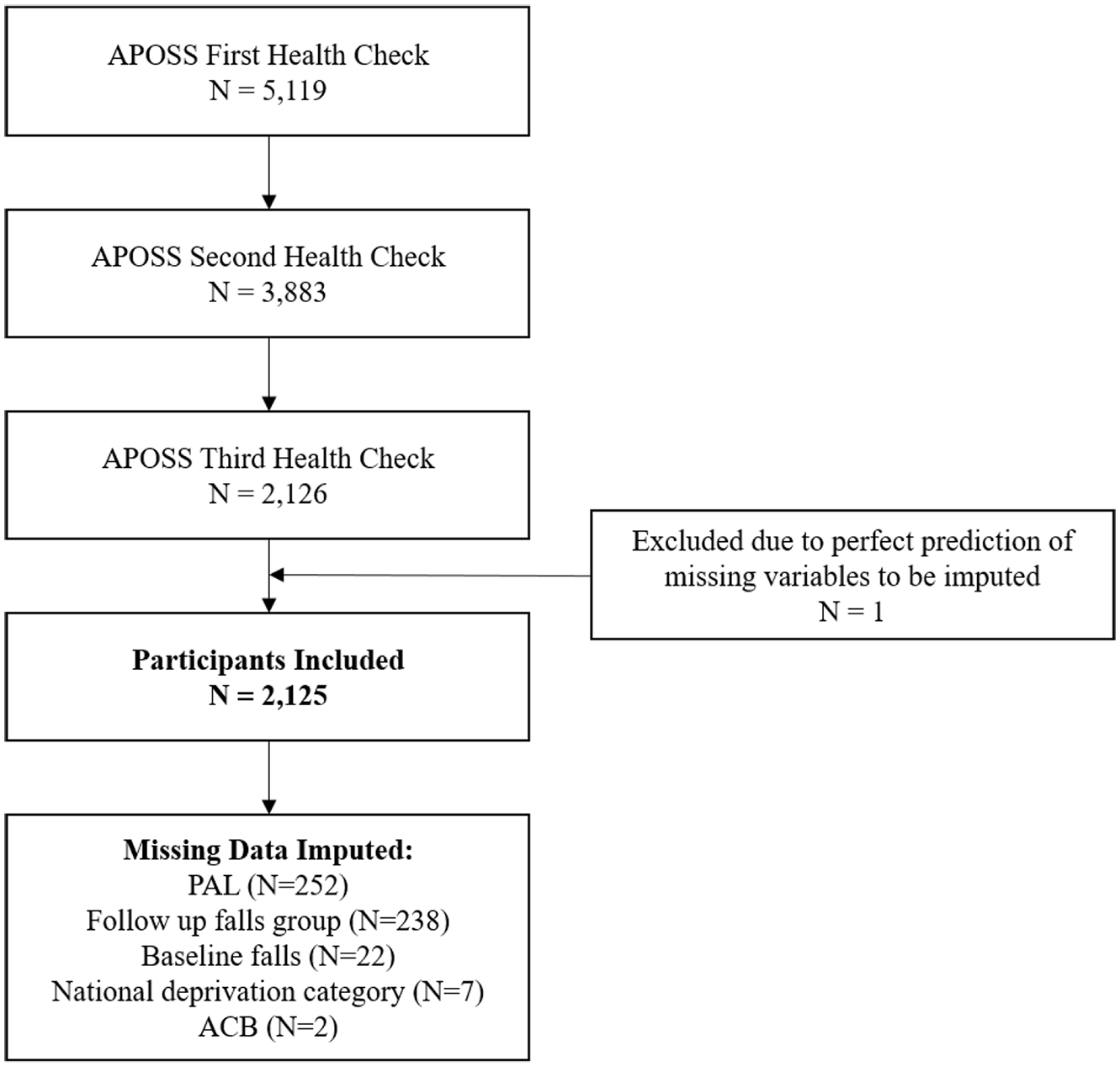
Flow diagram showing the selection of participant population and summary of missing data.
Participants were divided into three groups based on ACB: ACB = 0, ACB = 1 and ACB ⩾2. Multinomial logistic regression was performed to examine the association between the categorical outcome of follow up falls (no falls, 1 fall or ⩾2 falls in the 12 months prior to the follow up health visit) with ACB as the predictor. ACB = 0 was used as the reference category and no falls as the base outcome.
The APOSS study collected a wide range of participant demographics and comorbidities. From these, we selected those covariates with potential or proven associations with falls or physical function.26,27 Despite their associations with falls or physical function, several comorbidities were not included in the regression models due to their low prevalence in our study cohort and thus multicollinearity with our outcome: diabetes mellitus (n = 11), myocardial infarction (n = 8), osteoporosis (n = 14) and stroke (n = 4).
Regression model 1 was unadjusted. Model 2 adjusted for participant demographics at baseline: age, national deprivation category, PAL and BMI. Model 3 additionally adjusted for comorbidities: rheumatoid arthritis, osteoarthritis and asthma. Regression model 4 additionally adjusted for falls in the 12 months prior to the baseline health visit (baseline falls). A sensitivity analysis was performed by repeating our multinomial logistic regression analysis on complete cases. The results of hypothesis testing are reported using two-sided p values.
Results
Baseline characteristics and crude outcome rates
A total of 2125 women were included in the analysis. The pooled mean age [standard deviation (SD)] was 54.7 (2.2) years at study baseline (range 52–62 years) and 66.0 (2.2) years at follow up (range 60–73 years). Mean time between baseline and follow up was 11.4 years (SD 1.3 years).
Baseline characteristics and crude outcome rates of participants by ACB groups are shown in Table 1. Prevalence of baseline ACB score of 0, 1 and ⩾2 was 87.1%, 7.3% and 5.6%, respectively. Those with an ACB ⩾ 2 had lower PAL than those in the ACB = 0 or ACB = 1 groups. Additionally, increasing ACB group was associated with increased prevalence of osteoarthritis, asthma, myocardial infarction and stroke, but not osteoporosis. Highest prevalence of rheumatoid arthritis and diabetes mellitus was seen in the ACB = 1 group. Participants with ACB had higher BMI than those with ACB = 0. Increasing ACB group was associated with higher crude rates of recurrent falls at follow up [128/1851 (6.9%), 17/156 (10.9%) and 18/118 (15.3%) for ACB score of 0, 1 and ⩾2, respectively].
Baseline characteristics and crude outcome rates of included participants from the APOSS, UK, 1997–2011, stratified by anticholinergic burden groups.

ACB, anticholinergic burden; APOSS, Aberdeen Prospective Osteoporosis Screening Study; BMI, body mass index; PAL, physical activity level; SD, standard deviation; UK, United Kingdom.
Denotes comorbidities not included in multinomial logistic regression models due to a prevalence of less than 1% in the Aberdeen Prospective Osteoporosis Screening Study cohort.
Study outcome variable.
ACB and falls
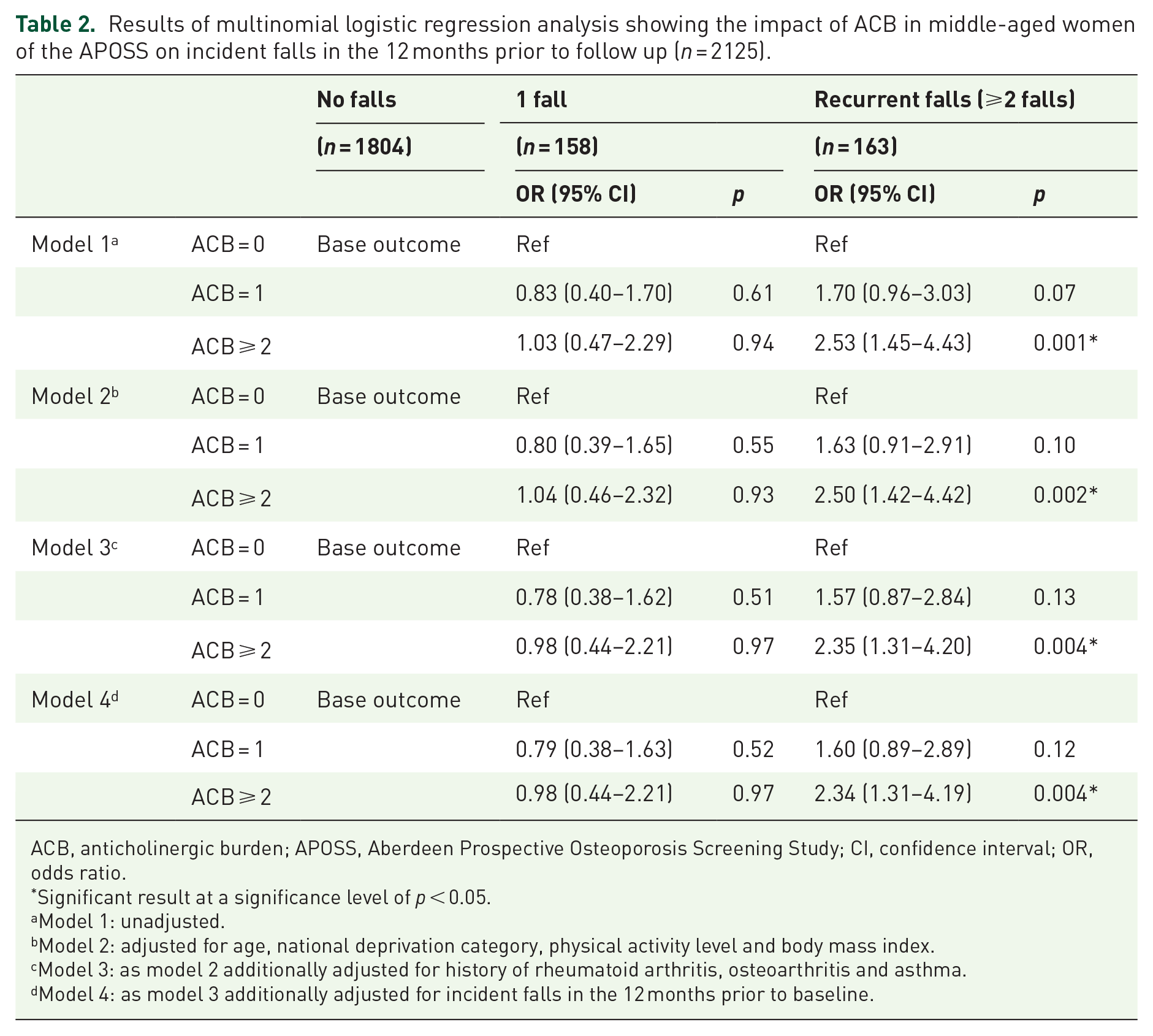
Table 2 shows the ORs for the association between ACB group and incidence of falls (1 fall and recurrent falls) in the 12 months prior to follow up. We found no association between ACB group and incidence of 1 fall in any model used. Additionally, we found no association between an ACB score of 1 and recurrent falls. However, an ACB score of ⩾ 2 was associated with increased odds of recurrent falls in the previous 12 months at an average of 11 years after initial exposure in the unadjusted and adjusted models [fully adjusted OR (95% CI) 2.34 (1.31, 4.19) p = 0.004].
Results of multinomial logistic regression analysis showing the impact of ACB in middle-aged women of the APOSS on incident falls in the 12 months prior to follow up (n = 2125).
ACB, anticholinergic burden; APOSS, Aberdeen Prospective Osteoporosis Screening Study; CI, confidence interval; OR, odds ratio.
Significant result at a significance level of p < 0.05.
Model 1: unadjusted.
Model 2: adjusted for age, national deprivation category, physical activity level and body mass index.
Model 3: as model 2 additionally adjusted for history of rheumatoid arthritis, osteoarthritis and asthma.
Model 4: as model 3 additionally adjusted for incident falls in the 12 months prior to baseline.
Supplemental Table S1 reports the same analysis performed on complete cases only. There were no significant differences between the multiply imputed and complete case analyses. An ACB score of ⩾ 2 was associated with increased odds of recurrent falls in the unadjusted and adjusted models [model 4 OR (95% CI) 2.54 (1.35, 4.78) p = 0.004].
Discussion
We have shown that an ACB score of ⩾ 2 in middle-aged women may be associated with more than 2-fold increased odds of recurrent falls in later life. To the best of our knowledge, this study is the first to report the potential association between ACB in middle age and recurrent falls in later life. Participants with an ACB score of ⩾ 2 had lower levels of physical activity and higher incidence of comorbidities than those in the ACB = 0 group; however, the association between ACB and recurrent falls remained after adjustment for these and other confounders.
Prevention of falls, particularly in older people, is of high global importance with direct impact on patient outcomes and health expenditure. History of falling is a significant risk factor for future falls and falling at a younger age has been shown to be the greatest risk factor for developing a fear of falling in older people, with resultant exclusion from physical and social activities.27–29 Existing literature has shown an association between use of medications with anticholinergic properties and increased risk of falls in older people.10–12,30 Due to the heterogeneity between studies it is difficult to quantify the increased risk proposed. However, the largest of these studies (n = 6343) reported that regular use of medication with anticholinergic properties (defined as use at two or three examinations over a 4-year period) increased the odds of falls in non-institutionalised older men and women by 60% [adjusted OR (95% CI) 1.6 (1.2, 2.1)]. 11 Several studies have additionally found an association between anticholinergic medication use and recurrent or injurious falls in older people.31–33 Despite the longitudinal design, Richardson et al. examined medication exposure at baseline and falls in the 12 months prior to the follow up visit, which occurred at around 2 years after baseline. 33 As in our study, they were unable to explore medication dose or potential variation in anticholinergic exposure during the follow up period. Interestingly, Marcum et al. were able to examine the influence of duration of anticholinergic exposure on the likelihood of recurrent falls. 32 They found that increasing duration of anticholinergic exposure was associated with an increased likelihood of recurrent falls. However, they too did not collect data on anticholinergic medication dose. 32 Many commonly prescribed medications that are not considered ‘traditional’ anticholinergics have been shown to have anticholinergic effects. 21 However, there does appear to be a dose-response relationship in terms of ‘anticholinergic potency’ and adverse outcomes (i.e. stronger anticholinergics exhibit a stronger relationship with outcomes). 34 Until further evidence emerges that similar relationships exist for the outcome of falls, the current public health message perhaps should focus on the potential link between anticholinergics and falls risk with the view to reduce ACB when possible.
A few mechanisms may explain the relationship between ACB and recurrent falls. Cholinergic blockade is associated with pupillary dilation and an inability to accommodate, thus resulting in visual impairment, particularly with regards to near vision. 35 Anticholinergic medications have been additionally associated with dizziness, cognitive impairment and slowed reflexes. 36 We observed that participants with an ACB ⩾2 had lower PAL than those with an ACB score of 0 or 1. Individuals taking anticholinergic medications generally have more comorbidities, which may contribute to a less active lifestyle due to physical impairment from disease. Thus, reduced physical activity may act as a mediator between ACB and recurrent falls. Decreased physical activity increases falls risk through muscle strength, balance and gait deficits. 37 Trials of tai chi or combinations of strength, gait, balance, and endurance training have been shown to reduce falls rates by as much as 46%. 37
We observed that, whereas ACB ⩾ 2 was associated with future recurrent falls in all models employed, there was no such association with an ACB of 1 after adjustment for comorbidities. Similarly, the association between ACB ⩾ 2 and the risk of suffering from any number of future falls disappeared after adjustment for comorbidities. It may be that the high incidence of falls in older people (15.1% in a 1-year period for our sample aged 60–73 at follow up) is a result of predisposing functional comorbidities such as arthritis, stroke and myocardial infarction, but that above this baseline risk of falls in the functionally impaired, an ACB ⩾2 independently increases the risk of falling repeatedly over a 12-month period.
Our study benefits from several strengths. Our study includes a well-characterised cohort of participants selected randomly from a primary care register. Current literature only examines the association between ACB and falls in those aged 65 and over. Our study highlights the potential association between the prescription of anticholinergic medications in middle-aged women and the significant outcome of recurrent falls in later life. This should act as an incentive to conduct further research in this area to confirm this important relationship.
We note some limitations. As an observational study, medications were not assigned randomly among cohort members, thus residual confounding cannot be completely excluded. Furthermore, we performed secondary data analysis on the APOSS study. As a result, ACB was calculated only at baseline based on self-report of medications, hence we cannot account for changes in ACB throughout follow up, potentially leading to misclassification. Therefore, our findings should be interpreted with caution as it is possible that participants’ anticholinergic exposure varied throughout the follow up period. As a result, there is the potential that our findings are explained by the cross-sectional relationship between high ACB at follow up and resultant falls. Without further data on anticholinergic exposure from the APOSS study, we were unable to evaluate this possibility. Nevertheless, our findings highlight the possible detrimental effects of anticholinergic exposure in middle age and emphasise the need for further research in this area. While participants of our study were exclusively female, we believe that, due to the possible explanatory mechanisms outlined above, our results are generalisable to both male and female patients. Duration and dose of anticholinergic medications were not recorded, thus it is unclear whether length or degree of cholinergic blockade is a risk factor for falls. Additionally, the outcome of falls was self-reported and has the potential to be influenced by recall bias. Participants were only asked to report falls in the 12 months before the follow up health visit, possibly leading to missed falls events. Nevertheless, participants are unlikely to accurately recall events that occurred more than 1 year previously. Falls are likely to be under-reported as opposed to over-reported, which would attenuate our results.
From a clinical perspective, reduction in falls would lead to decreased mortality, fewer fractures, greater mobility, improved psychological wellbeing and ultimately better quality of life in an increasingly older population. Strategies to minimise the prescription of anticholinergic medications in older adults have proven effective in reducing anticholinergic exposure; however, this does not necessarily translate into improved outcomes. One study found that alerting consultant clinicians to patients’ ACB scores significantly reduced anticholinergic drug exposure in hospitalised patients. 38 Future research to explore the effects of anticholinergic exposure in middle age and strategies to reduce the prescription of anticholinergic medications would be useful. Furthermore, research should assess if a reduction in anticholinergic exposure improves patient outcomes.
In conclusion, our study provides evidence that exposure to an ACB score of ⩾ 2 in middle-aged women may be associated with recurrent falls in later life. Given the ubiquity of prescription of anticholinergic medications for myriad conditions and in the absence of data from randomised controlled trials, we advise cautious prescribing of anticholinergic medications in this group. We hope that our study will act as a catalyst for further research into this important and unexplored area of drug safety.
Supplemental Material
Supplementary_Table_1 – Supplemental material for Anticholinergic burden in middle-aged women and recurrent falls in later life: findings from the Aberdeen prospective osteoporosis screening study (APOSS)
Supplemental material, Supplementary_Table_1 for Anticholinergic burden in middle-aged women and recurrent falls in later life: findings from the Aberdeen prospective osteoporosis screening study (APOSS) by Samuel R. Neal, Adrian D. Wood, Andrew D. Ablett, Jenny S. Gregory, Jordan Guillot, Helen M. Macdonald, David M. Reid and Phyo K. Myint in Therapeutic Advances in Drug Safety
Footnotes
Acknowledgements
We gratefully acknowledge the Steering Committee of APOSS for their permission to conduct this research.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Aberdeen Prospective Osteoporosis Screening Study (APOSS) was funded by the Grampian Osteoporosis Trust. SRN received an Aberdeen Summer Research Scholarship supported by funding from the Institute of Applied Health Sciences, University of Aberdeen, UK. The funder had no role in design, analysis, interpretation or reporting of the work presented.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.