
Abstract
Background:
Androgenic anabolic steroids (AASs) have a number of licensed clinical indications but are also subject to abuse within the body building community. They have a number of potentially important adverse pharmacological effects, and users require health monitoring, including selected laboratory investigations. The extent to which AAS users are able to seek medical supervision and the ability of healthcare providers to respond to the needs of users is uncertain. The present study sought to ascertain how AAS abusers interact with healthcare providers, and self-reported knowledge among doctors regarding the healthcare effects and need for monitoring of AAS users.
Methods:
Questionnaires were administered, and there were 216 respondents among AAS users and 134 doctors.
Results:
A high proportion of AAS users cited various barriers to accessing healthcare, including 136 of 189 (72%) that reported a fear of reproach, and 107 of 194 (55%) that had avoided seeking medical advice; 137 of 193 respondents (71%) did not disclose AAS use to healthcare professionals. Doctors across a broad range of seniority stated a lack of knowledge of AASs; 130 (97%) had received no formal training, and 109 (82%) did not know which blood tests could be used for safety monitoring.
Conclusions:
The present study has highlighted some perceptions among the body-building community that create obstacles to them accessing appropriate safety monitoring while using AASs. Doctors may not have adequate knowledge of AASs, which may prevent them giving accurate and complete information. Further work is needed to address the barriers of communication between users and health professionals in order to facilitate better healthcare monitoring and drug safety.
Introduction
Anabolic androgenic steroids (AASs) are a group of compounds that include the naturally occurring sex hormone testosterone, as well as synthetic derivatives. The pharmacological mechanisms of action include anabolic effects that promote muscle growth, and androgenic effects causing masculinization. Human studies of AAS compounds date back to the experiments of Charles Brown-Séquard in the late 1800s. There came significant advances in the 1930s when German and Dutch chemists synthesized pharmaceutical grade testosterone.1,2 During the 1940s, AAS were explored for other therapeutic areas, and remain in clinical use today with a diverse range of indications including growth impairment, infertility, anaemia, renal insufficiency, and as an adjunct to reduce muscle wasting in conditions, including HIV infection. 3
The potential for use of AASs as performance-enhancing drugs among athletes has long been recognized. In 1945, Paul de Kruif described the anabolic capabilities of testosterone, testosterone propionate and methyltestosterone in a book entitled ‘The Male Hormone,’ which proved to be a catalyst for the rise in use among body builders in the West Coast of the United States in the late 1940s and early 1950s.4,5 Use was confined to elite athletes until the 1980s, after which greater awareness and availability led to increasing uptake by a broader range of users. 6 A popular book by Dan Duchaine ‘Underground Steroid Handbook’ published in 1981, gave details of how to self-administer AASs, typical adverse effects, and the optimal dosing strategy; other similar publications followed.7,8 In response to public concern regarding the potential for adverse effects and increasingly widespread use of AASs, in 2012 they were added to the list of Class C substances in the Misuse of Drugs Act 1971.
The adverse effect profile of AASs is generally derived from clinical studies within their licensed therapeutic indications, and few systematic data are available regarding their adverse effects within a body-building context. Recognized cardiovascular effects include adverse lipid profile, hypertension, left ventricular hypertrophy, thrombosis, myocardial fibrosis, myocarditis, and dysrhythmias. 9 Liver effects include intrahepatic cholestasis and liver necrosis, and AASs use can suppress the immune system.10,11 Masculinization may be observed in women, as a direct result of excess androgen effects, and conversely, feminizing effects in males can occur due to the conversion of excess androgens to oestrogens, and suppression of gonadotropin-releasing hormone, luteinizing hormone, and follicle-stimulating hormone. 12 AAS use is a recognized cause of impaired male fertility due to a reversible fall in sperm numbers and motility, and there are concerns that disruption of normal testosterone cell signalling might exert carcinogenic effects. 13 Adverse behavioural symptoms have been reported, including irritability and hostile behaviour, which are thought to arise from the direct effects on the amygdalo-fugal pathway connecting the central nucleus of the amygdala to the brainstem, which is involved in cognitive–emotive and homeostatic processes; indirect effects on serotonergic, dopaminergic, and glutamate signalling pathways in the anterolateral hypothalamus have also been implicated. 14 Depression can occur during the post-treatment phase, when the concentrations of endogenous hormones fall below normal as a result of suppressed luteinizing hormone.15–18 There has been recent published guidance regarding blood test monitoring in AAS users (Table 1). 19
Various laboratory investigations to monitor health effects among AAS users. 18

AAS, androgenic anabolic steroid; ECG, electrocardiogram; FBC, full blood count; HDL, high-density lipoprotein; LDL, low-density lipoprotein; LFT, liver function test;
It is difficult to accurately estimate the extent of current AAS use. The 2016 to 2017 annual Crime Survey for England and Wales found an increase in reported anabolic steroid use among 16–24 year-olds from 0.1% to 0.4%; although the level of reporting was low, it would equate to around 19,000 additional young adult users in 1 year in England and Wales. 20 With continued use of these agents within the body-building community, and concern that their use is increasing, it is especially important that healthcare professionals are aware of the patterns of use of AASs and the impact on users’ health. Doctors should be sufficiently empowered to inform users about potential adverse effects and be aware of how best to minimize these risks and identify health effects. There is uncertainty regarding where AAS users seek information and support, and whether they would access health resources in a conventional way. There are some parallels with drug misuse, tobacco use, and alcoholism where patients may be reluctant to seek advice from healthcare professionals. 21 There is a perception that the medical community might have a lower overall awareness of the health effects of AASs. For example, why the use of AASs in addition to resistance training boosts muscle growth more than the physiological hormonal changes that occur after resistance training alone. 22 The effects of administering supraphysiological testosterone doses have long been recognized by the body-building community but there was a long time lag before this finding became accepted within the wider medical community. 23 Recent reports have shown that the Internet provides anecdotal information that may misinform users and propagate dangerous practices. 24
The aim of the present study was to identify the level of knowledge among doctors and to assess how confidently they could manage health effects associated with AASs. We also sought to examine the views of users within the body-building community regarding their willingness to seek advice from healthcare professionals. We sought to identify possible barriers to accessing healthcare arising from perceptions among users and healthcare professionals, with a view to promoting better communication and public health education in this patient group.
Methods
We performed two separate surveys using online data collection tools. Survey 1, entitled ‘Body builder’s Experiences of Interactions with Doctors Regarding Performance Enhancing Drugs’ was targeted at body builder groups identified using the social media platforms, Facebook and Instagram. Groups were identified from a search of clubs using the search term ‘body-building’ or ‘body builder’ in the group title; additional individuals were identified as those linked to the original search groups that expressed an interest in body-building. Participants were invited to complete a questionnaire, via a link to the online survey, that included 10 open-ended and closed questions. Survey 2, entitled ‘Doctor’s Confidence with Managing Patients Using Performance Enhancing Drugs in Body-building’ was administered to doctors working at Royal Derby Hospital, as well as doctors reached via social media on Facebook and Instagram. The surveys are summarized in Tables 2 and 3. This included general practitioners, hospital consultants, and trainee doctors, using a link to an electronic survey, again this involved 10 questions. Both studies were performed between August and September 2016. Guidelines from our local research and development department determined that the project was an audit project and formal ethical approval was therefore not required. No personally identifiable data were collected or stored by the investigators. Descriptive data are used to present the survey results.
Survey 1 ‘Body builder’s Experiences of Interactions with Doctors Regarding Performance-Enhancing Drugs’; free text comments were permitted for each question.

PED, performance-enhancing drug.
Survey 2 ‘Doctor’s Confidence with Managing Patients using Performance-enhancing Drugs in Body-building’; free text comments were permitted for each question.

GP, General Practitioner; PED, performance-enhancing drug; SHO, Senior House Officer.
Results
Body builders’ experiences of interactions with doctors regarding performance enhancing drugs
There were 216 respondents, and a 90% completion rate for the submitted responses. Participants had used AASs for between 1 month and 24 years, and 91 (42%) said that they had healthcare checks including regular blood tests to monitor health while using AASs. Of the participants that did access healthcare, the frequency of monitoring varied significantly, with some attending once per month, every quarter, or every 6 months, whereas others attended before and or after a receiving a cycle of AAS treatment. A total of 140 respondents (65%) said that they would not trust their General Practitioner to report blood tests accurately in the context of AAS use. Only 24 of the 108 (22%) who answered the further question relied on a National Health Service (NHS) doctor to interpret their lab data, whereas 54 (50%) consulted a private specialist, 7 (6%) relied upon interpretation by a nonmedical friend, and 23 (22%) relied on other general resources to interpret the lab data.
There were 106 (49%) respondents that cited various barriers to them accessing healthcare and monitoring while using AAS: fear of judgement by healthcare professionals 27 (26%), perceived lack knowledge of AAS by the medical community 8 (7.5%), healthcare professional unwilling to arrange testing 14 (13%), cost would be prohibitive 14 (13%), did not know where testing could be arranged 8 (8%), and did not want AAS use on their health records 7 (7%) (summarized in Table 4). There were 136 respondents out of 189 (72%) that reported a perceived judgemental attitude from their healthcare provider regarding AAS use, and 107 out of 194 (55%) said that they have held back from seeking medical advice because of fear of judgement regarding AAS use. There were 9 (4%) that did not feel blood tests were needed and were not concerned about barriers to accessing healthcare.
Reasons cited by body builders for not accessing healthcare monitoring while using AASs, summarized in convenience categories of response.
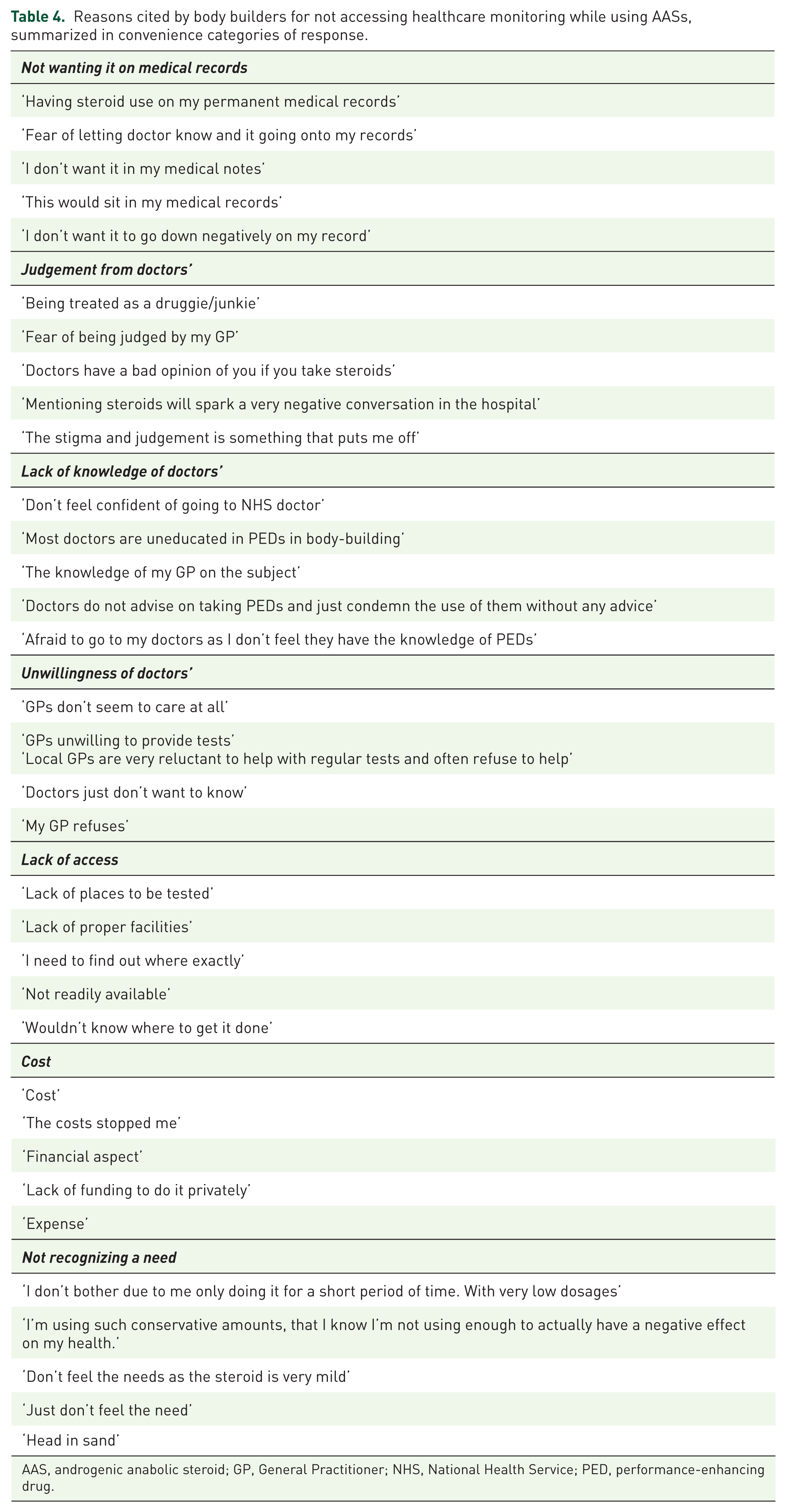
AAS, androgenic anabolic steroid; GP, General Practitioner; NHS, National Health Service; PED, performance-enhancing drug.
Overall satisfaction with NHS consultations regarding AASs was rated by 184 respondents as ‘poor’ in 131 (71%), ‘average’ in 47 (25%), ‘good’ in 5 (3%), and ‘excellent’ in 2 (1%). Overall, 137 of 193 (71%) respondents said that they had withheld their AAS use from healthcare professionals, and 96 (49.5%) out of 194 respondents that said they had received information regarding AAS by healthcare professionals that they considered inaccurate, summarized in Table 5.
Information offered to body builders by healthcare professionals perceived to be incorrect or misleading.

ECG, electrocardiogram; GP, General Practitioner; PED, performance-enhancing drug.
Doctors’ confidence with managing patients using performance enhancing drugs in body building
There were 134 responses from doctors, including 60 (45%) General Practitioners, and 74 hospital doctors across a range of seniority: 7 (5%) Foundation Year trainees, 41 (31%) Senior House Officers, 17 (13%) Specialist Trainees, and 9 (7%) consultants. Respondents were working in a range of specialties at the time of the study: anaesthetics, psychiatry, palliative care, Sports and Exercise medicine, oncology, respiratory, gastroenterology, haematology, paediatrics, breast surgery, trauma and orthopaedics, vascular, and urology. Overall, two doctors (1.5%) reported prior use of AASs themselves. All questions were completed fully, spending on average 1 minute on the survey.
When asked whether they remember having formal teaching about AASs used in body-building in medical school, 130 (97%) answered no. Responses regarding how confident doctors felt in their knowledge about AASs are shown in Figure 1. When asked if they would confidently know which blood tests are indicated to monitor health while using AASs, 109 (82%) said no, and 107 (80%) said that they would not feel confident in safely interpreting blood tests results in someone using AASs. Among doctors, 83 (62%) said that blood test monitoring for AAS users should not be provided by the NHS.
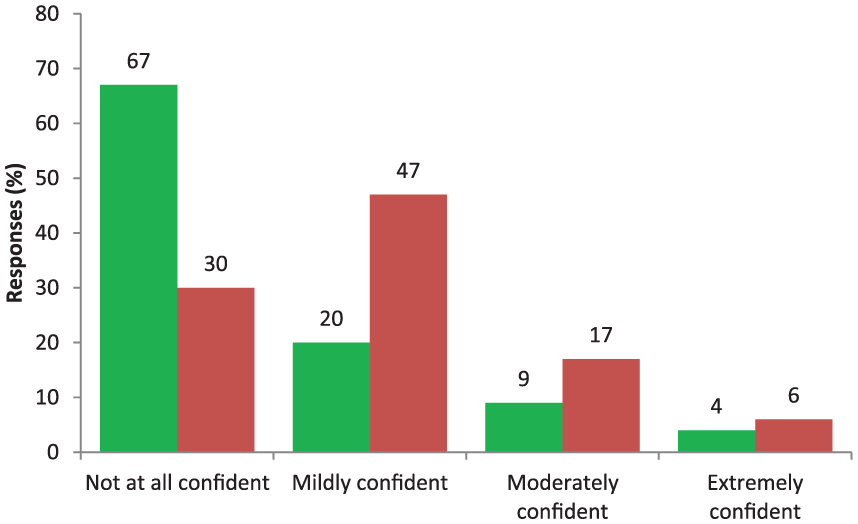
Doctor self-reported confidence regarding AASs, (a) drugs available, doses, administration routes (green boxes), and (b) potential health risks of AAS (red boxes), as percentage values (n = 134).
Discussion
The study has provided novel data in an area that has received comparatively little research attention. The findings indicate a wide range of practices within the body-building community, suggesting a lack of clarity regarding the optimal strategy for of health monitoring and blood checks during AAS use. Body builders expressed a number of barriers to accessing health care and blood tests for monitoring. This was mirrored by self-reported knowledge gaps regarding the pharmacological and adverse effects of AASs among doctors that participated in this study. A key finding that the study highlights is a lack of trust by body builders in healthcare professionals, and a surprisingly high proportion of users rated their overall interaction with healthcare professionals as poor. Users often concealed the use of AASs from their physician, largely due to a fear of critical judgement or lack of understanding. Around half said they had held back from seeking medical help for fear of judgement or that AAS use was associated with stigma. These factors appear to be important barriers to receiving medical support or accessing laboratory investigations.
A study conducted at Harvard Medical School, USA in 2004 among weight-lifters found that 56% of AAS users had never disclosed this to a physician, and they perceived that healthcare professionals were unlikely to have any greater knowledge of the pharmacological effects than their friends, the Internet, or the person who supplied their drugs. 25 The present study found that many AAS users felt that they had been provided with inadequate or inaccurate information; similarly, around two thirds of the doctors reported feeling a lack of knowledge regarding AASs, across a broad range of seniority. High proportions of doctors in the present survey felt unsure about the use of blood tests to monitor AASs (82%) or how to interpret the results (80%). A lack of knowledge concerning AASs has previously been identified in General Practitioners in the UK in the 1990s, which found that 12% incorrectly believed that they were permitted to prescribe AASs for nonmedical reasons. 26 Other reports from the Balkans and France have shown that community doctors have perceived gaps in their knowledge regarding the pharmacological and adverse effects of AASs in athletes.27,28 Data from Australia have pointed out a lack of doctors specializing in sport science and a need for better education of healthcare professionals in order to reduce stigma related to AAS use. 29
A limitation is that the study participants were drawn mainly from a single hospital and region, and the findings might not be generalizable to other parts of the UK or other countries. The design involved a convenience sample, and the lack of systematic recruitment means that we cannot exclude participant selection bias. Further work is needed to systematically evaluate the findings in a wider population and to examine whether significant differences exist between survey participants in other regions. The surveys were intentionally brief to encourage participation, and the study design did not allow us to verify that the respondents were medically qualified. In addition, we did not collect data concerning the specific agents, dose, or frequency of AAS use because we were concerned that this level of detail might deter some participants; a limitation of the study is that we are not able to draw any comparison between experienced versus infrequent AAS users.
In conclusion, the present study has highlighted important perceptions within the body-building community that create obstacles to them accessing healthcare or laboratory monitoring during AAS treatment, mainly related to fear of criticism or judgement. Doctors themselves do not feel adequately confident in their knowledge of AASs, which may result in them providing inaccurate or incomplete information, further undermining patient trust. Additional work is needed to examine whether the findings are generalizable to clinicians working in other regions. It would seem likely that a multinational approach would be helpful to examine in closer detail the hazards posed by AASs, perhaps by registries that would allow closer follow up of health effects in users. Improving knowledge of the pharmacological actions and adverse effects of AAS within the medical community is important in establishing a clearer consensus approach to addressing healthcare needs in this patient group, including a more uniform approach to laboratory analyses. This study identifies important barriers that need to be addressed, aiming for a better understanding between AAS users and healthcare professionals to minimize the adverse effects of treatment.