
Abstract
Background:
Abuse of prescription opioids, particularly by intravenous (IV) administration, can cause respiratory depression and death. ALO-02, an abuse-deterrent opioid formulation, is designed to release sequestered naltrexone upon manipulation by crushing, thereby antagonizing the pharmacologic effects of oxycodone. This exploratory post-hoc analysis examined the effects of IV administration of simulated crushed ALO-02 on end-tidal carbon dioxide (EtCO2), a surrogate marker of respiratory depression.
Methods:
Data were obtained from a randomized, double-blind, placebo-controlled, three-way crossover study in nondependent recreational opioid users that evaluated the abuse potential of IV administered oxycodone 20 mg + naltrexone 2.4 mg (simulating crushed ALO-02) versus oxycodone 20 mg or placebo. EtCO2 was measured as a secondary endpoint using noninvasive capnography at baseline and postdose intervals, up to 24 h.
Results:
Baseline EtCO2 (mean ± standard error of the mean (SEM)) values (n = 33) were similar across treatments: 33.5 ± 0.9, 33.5 ± 0.8, and 34.0 ± 0.7 mmHg for oxycodone 20 mg + naltrexone 2.4 mg, oxycodone 20 mg, and placebo, respectively. After dosing, mean ± SEM of the maximum effect (Emax) on EtCO2 was 37.5 ± 0.6, 40.5 ± 0.8, and 36.9 ± 0.6 mmHg for oxycodone 20 mg + naltrexone 2.4 mg, oxycodone 20 mg, and placebo, respectively. Emax values were significantly lower for oxycodone 20 mg + naltrexone 2.4 mg versus oxycodone 20 mg (p = 0.0005), and not different from placebo (p > 0.05).
Conclusions:
This abuse-potential study suggests that naltrexone released from ALO-02 tampering by crushing attenuates oxycodone-induced increase of EtCO2 in nondependent recreational opioid users.
Introduction
The abuse of prescription opioids in the USA has become a major public health problem with significant impact on health and mortality.1–3 According to the Centers for Disease Control and Prevention, the death rate in the USA from overdose of commonly prescribed opioids (natural semisynthetic opioids and methadone) increased approximately 3-fold between 2000 and 2015, with an estimate of more than 15,000 deaths in 2015. 4 In addition to the growing number of overdose deaths related to prescription opioids, deaths resulting from heroin overdoses are also alarmingly high and on the rise. 4 Opioid-induced respiratory depression is the primary cause of death following overdose. Opioids negatively affect the ability of the central nervous system to respond to states of hypoxia or hypercapnia, and respiratory depression may occur within minutes of intravenous (IV) opioid administration. 5
Increasing and varied efforts have been aimed at reducing prescription opioid abuse and overdose while preserving patient access to effective opioid medication. 3 These efforts include the introduction of abuse-deterrent opioids such as ALO-02, a pharmaceutical formulation in the form of capsules containing pellets with a layer of extended-release oxycodone hydrochloride surrounding sequestered naltrexone hydrochloride, that has received regulatory approval in the USA (August 2016; Troxyca® ER, Pfizer, New York, NY, USA). 6 Troxyca ER was approved by the US Food and Drug Administration (FDA), but not commercialized thereafter. Naltrexone, a competitive µ-opioid antagonist, is released when the capsule and its contents are manipulated by crushing. This release of naltrexone mitigates the pharmacodynamic effects of oxycodone, including the positive subjective effects associated with abuse such as ‘drug liking’ and ‘high’. When ALO-02 is taken as directed, with the capsule swallowed intact, naltrexone remains sequestered, and the intended therapeutic effects of oxycodone are preserved.7,8
The antagonistic effects of naltrexone have been demonstrated in abuse-potential studies where ALO-02 is crushed and/or dissolved and administered to recreational opioid users via various routes of abuse, including intranasal and IV. In each of these studies, the effects of manipulated ALO-02 on measures of ‘drug liking’ and ‘high’ were significantly lower than those associated with oxycodone alone,9,10 suggesting a reduction of abuse potential of ALO-02 due to the antagonistic action of naltrexone. Among the common routes of abuse, IV administration is particularly dangerous as it poses significant risk of disease transmission through needle-sharing, along with risks of unintentional overdose and potentially fatal respiratory effects. 11
As with the subjective measures of ‘drug liking’ and ‘high’, the release of naltrexone when ALO-02 is abused through IV injection has the potential to mitigate the respiratory-related harmful effects of oxycodone. The objective of this post-hoc exploratory analysis of data from the abuse-potential study of simulated IV ALO-02 10 was to examine the effects of naltrexone on oxycodone-mediated changes in end-tidal CO2 (EtCO2), a surrogate marker of respiratory depression. 12
Methods
Study design
The exploratory respiratory safety endpoints were part of an abuse-potential study, designed as a single-center, randomized, double-blind, placebo-controlled, three-way crossover study in nondependent recreational opioid users (ClinicalTrials.gov identifier: NCT01825447). 10 A detailed description of these exploratory respiratory safety endpoints has not previously been published. The protocol was approved by the New England Institutional Review Board (Newton, MA, USA), and the study was conducted in compliance with the Declaration of Helsinki, the International Conference on Harmonisation Good Clinical Practice Guideline, and all local regulatory requirements. All participants provided written informed consent before any study procedures were initiated.
Participants
As recommended by the FDA for abuse-potential studies, participants were healthy men and women identified as nondependent recreational drug users. 13 Recreational use was defined as nonmedical use of opioids on at least 10 occasions within the last year and at least once in the previous 8 weeks (prior to the screening visit); nonmedical use must have included IV use on at least 1 occasion and/or intranasal use on at least 3 occasions within the last year. Among participants who completed the study, all reported using opioid drugs recreationally in the last 12 months. The most commonly abused subject-reported opioids were Lortab® (hydrocodone bitartrate and acetaminophen) (n = 24), oxycodone (n = 18), Percocet® (oxycodone and acetaminophen) (n = 12), and/or hydrocodone (n = 6). 10 Other key inclusion and exclusion criteria are provided elsewhere. 10
Procedure
The study consisted of the following phases: screening, naloxone challenge, drug discrimination, treatment, and end-of-study visit. The details are provided elsewhere, 10 and described briefly here. Following standard medical screening to determine eligibility, a naloxone challenge was conducted where individuals were evaluated for signs of opioid withdrawal following IV administration of naloxone to exclude participants who were physically dependent on opioids. Participants then entered the drug-discrimination phase to confirm participant safety and ability to distinguish oxycodone from placebo, based on prespecified measures of ‘drug liking’ and ‘take drug again’. After a washout period of at least 3 days, eligible participants then entered the main portion of the study, the treatment phase, which evaluated simulated ALO-02 on measures of abuse potential, reported elsewhere, 10 and respiratory depression. Over the course of three visits, participants received randomized double-blind IV administration (over 4 min ± 15 s) of the following treatments: (a) oxycodone hydrochloride 20 mg + naltrexone hydrochloride 2.4 mg (to simulate IV injection of a crushed and dissolved ALO-02 20 mg/2.4 mg capsule); (b) oxycodone hydrochloride 20 mg; (c) placebo (0.9% sodium chloride). Administration of each of the three treatments, that is, each visit during the treatment phase, was separated by at least 5 days. The simulated dose of ALO-02 (oxycodone hydrochloride 20 mg/naltrexone hydrochloride 2.4 mg, herein referred to as oxycodone 20 mg/naltrexone 2.4 mg) was chosen based on previous abuse-potential studies with oxycodone, 14 and the equivalent oral dose of ALO-02 (oxycodone hydrochloride 40 mg/naltrexone hydrochloride 4.8 mg) as a dose that is both safely tolerated and expected to produce significant drug effects. Upon completion of the treatment phase, participants returned for an end-of-study visit for final safety assessments.
Endpoints
EtCO2 (mmHg) was measured using noninvasive capnography (CO2SMO ETCO2/SpO2 Monitor, Model 7100, Novametrix Medical Systems Inc., Wallingford, CT, USA) at baseline, at 5, 15, 30, and 45 min, and at 1, 1.5, 2, 3, 4, 6, 8, 12, and 24 h postdose. Respiratory rate and pulse oximetry were also measured at the same time points. Other pharmacodynamic measures related to abuse potential, along with pharmacokinetic and safety endpoints, were taken. These measures included adverse events, physical examinations, laboratory tests, and 12-lead electrocardiograms. The results of these measures are reported elsewhere. 10
Statistical analysis
The mean maximum (peak) effect (Emax) was calculated as the maximum change from baseline. An estimation of the treatment effect occurring within 2 h after dosing, a prespecified parameter in the statistical analysis plan for the study, was assessed by calculating the area under the effect curve (AUE0–2h). EtCO2, Emax, and AUE0–2h were analyzed using a mixed-effects model, with sequence, period, and treatment as fixed effects and subject within sequence as a random effect.
Results
Of the 33 participants randomized to study treatment, 29 completed the study. The disposition, demographics, and participant characteristics are reported elsewhere. 10 Briefly, the population (safety population, n = 33) was predominantly White (88%) and male (88%), with a mean age of 26.2 years (range, 18–42). 10
Oxycodone increased EtCO2 within the first 15 min of administration (Figure 1(a)). The effect diminished over approximately 2 h but remained elevated relative to placebo up to 4–8 h post-dosing. The combined administration of oxycodone 20 mg and naltrexone 2.4 mg (administered simultaneously), simulating ALO-02, resulted in a slight increase in mean EtCO2 levels, but the effect over time was generally similar to that seen with placebo (Figure 1(a)).

Mean (SEM) levels of EtCO2 (mmHg) at baseline and time points postdose (a), and mean (SEM) Emax EtCO2 (mmHg) compared with predose (b).
Mean Emax values at baseline and following drug treatment are shown in Figure 1(b). Oxycodone alone significantly elevated EtCO2 levels compared with placebo (p = 0.0001), and the effect was significantly reduced when naltrexone was co-administered with oxycodone (simulating ALO-02) (p = 0.0005). The maximum change in Emax values from baseline to test, calculated using least squares means, was consistent with these observations; a significantly greater change was observed following oxycodone alone versus placebo (p = 0.0001), and this effect was significantly attenuated when oxycodone was combined with naltrexone (p = 0.0035) (Table 1). Similar findings were observed when considering the effect over the first 2 h of dosing, AUE0–2h (Table 1).
Maximum change in Emax and AUE0–2h EtCO2 from baseline: least squares means (90% confidence interval).
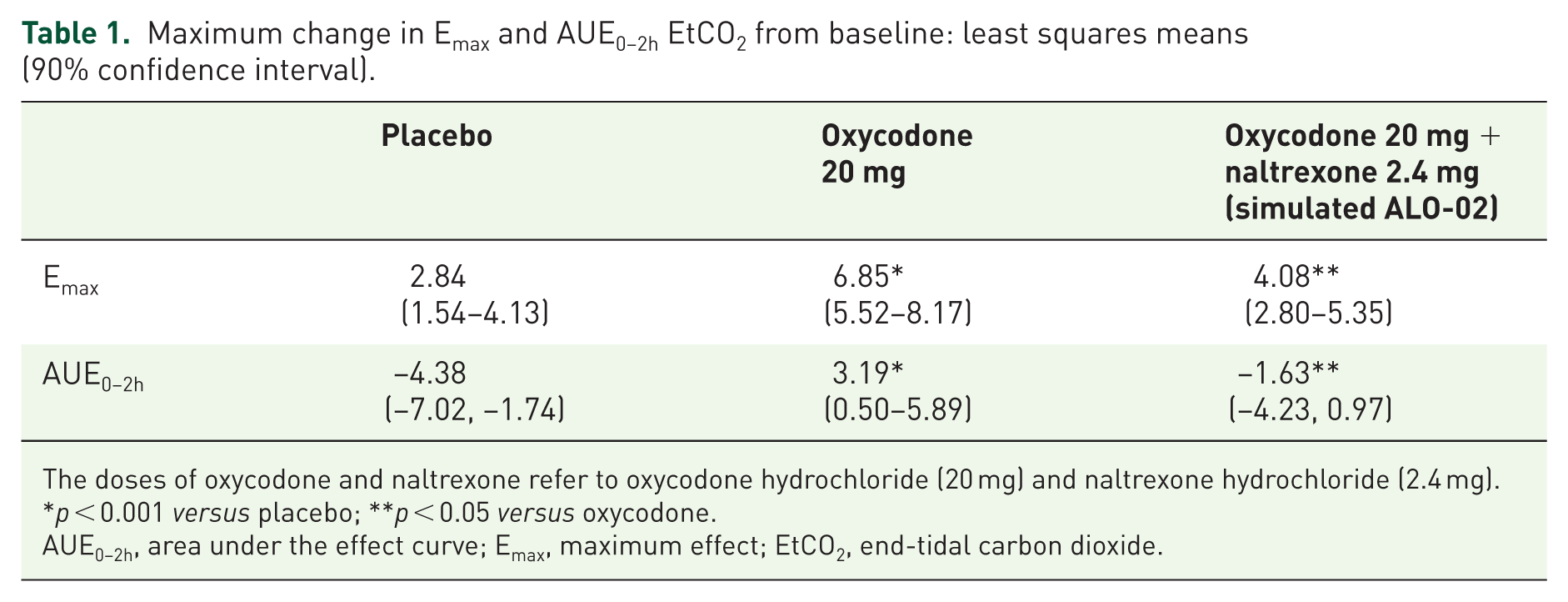
The doses of oxycodone and naltrexone refer to oxycodone hydrochloride (20 mg) and naltrexone hydrochloride (2.4 mg).
p < 0.001 versus placebo; **p < 0.05 versus oxycodone.
AUE0–2h, area under the effect curve; Emax, maximum effect; EtCO2, end-tidal carbon dioxide.
Oxycodone reduced oxygen saturation (relative to placebo) within the first few hours post-treatment, and this reduction was attenuated by naltrexone (Figure 2). No consistent changes in respiratory rate over time or differences between treatment groups were observed (Figure 3).

Mean (SEM) pulse oximetry (%) at baseline and time points postdose.

Mean (SEM) respiratory rate (respirations/min) at baseline and time points postdose.
Discussion
Using simultaneous IV administration of oxycodone 20 mg and naltrexone 2.4 mg to simulate IV administration of crushed ALO-02 (capsule strength, 20 mg/2.4 mg), this exploratory analysis demonstrated that the oxycodone-induced elevation of EtCO2 (relative to placebo) was significantly reduced when naltrexone was simultaneously administered with oxycodone. Similar results were observed for pulse oximetry, but not respiratory rate, although statistical analyses were not performed on these exploratory measures. Considering EtCO2 as a measure for depression of alveolar ventilation, these results suggest that, should capsules of ALO-02 be manipulated by crushing, naltrexone release may attenuate the oxycodone-induced elevations of EtCO2. Although the pattern of elevated alveolar EtCO2 and reduced peripheral capillary oxygen saturation (SpO2) after oxycodone alone may indicate the initial phases of opioid-induced respiratory depression, respiratory rates were not yet significantly clinically affected. Nevertheless, at the 20 mg oxycodone dose tested in this study, the increases in EtCO2 or reductions in SpO2 were not seen following oxycodone + naltrexone as they were after oxycodone alone. The effect of naltrexone on oxycodone-induced respiratory depression, as assessed by respiratory rates, may only be determined by examining higher doses of oxycodone that elicit an increased pharmacological opioid response, resulting in a clinically significant reduction in respiratory rates and thus respiratory depression.
The results of this analysis are generally consistent with a previously reported exploratory analysis of an extended-release morphine sulfate and sequestered naltrexone hydrochloride formulation (EMBEDA®, Pfizer Inc.). 15 The analysis examined the potential for concurrent IV administration of naltrexone and morphine to reduce EtCO2 versus morphine alone and demonstrated similar findings to those reported here for ALO-02. 16 Together, these results suggest that pharmacologically based abuse-deterrent formulations may offer a respiratory safety benefit should the drug be abused via IV administration.
A recent preclinical study identified a biphasic effect of low to moderate doses of oxycodone on oxygen levels in the nucleus accumbens. 17 An initial transient decrease was followed by a subsequent increase, with the increase attributed to cerebral vasodilation induced by neural activation. When considering ALO-02, these pharmacodynamic actions of oxycodone may supplement the effect of naltrexone in preventing or reversing respiratory depression upon crushing of the capsules. However, this would depend on the apparent concentration of oxycodone that crosses the blood–brain barrier, since in the study by Solis and colleagues, high doses of oxycodone only decreased oxygen levels. 17 Such effects of low to moderate doses of oxycodone would need to be confirmed by clinical studies in humans. Additional preclinical evaluation of oxycodone on respiratory depression has shown that it dose-dependently acts as a partial opioid agonist of short duration. 18 These findings would appear to support the results of the current study whereby the effects of oxycodone on respiratory depression are limited and reversible by naltrexone. However, at higher doses, the effects of oxycodone on respiratory depression are likely to be more pronounced.
As a result of the growing number of overdose deaths related to both prescription opioids and heroin, the FDA, as part of the Opioid Initiative launched by the US Department of Health and Human Services, is supporting greater public access to over-the-counter naloxone formulations to treat opioid overdose. 19 Their efforts, along with the availability of pharmacologically based abuse-deterrent formulations of prescription opioids, may be effective strategies in reducing the number of opioid-related overdose deaths.
The results and conclusions of this post-hoc analysis should be considered within its limitations. The original abuse-potential study from which these data were obtained was powered to show a reduction in the primary pharmacodynamic parameters of ‘drug liking’ and ‘high’ (based on visual analog scales). Further studies, including those evaluating additional doses and other methods of abuse (e.g. intranasal or oral administration of crushed ALO-02) that are powered using direct measures of respiratory function, are needed to confirm if the risk of respiratory depression is reduced when oxycodone is co-administered with naltrexone in the same fixed ratio in ALO-02. Furthermore, this study utilized a single-dose simulation of crushed and fully dissolved ALO-02, rather than actual tampered product, to avoid the adverse effects caused by IV injection of excipients (i.e. talc) or other particulate matter that may be present in manipulated ALO-02. This safety precaution necessitated an extrapolation of the effects on EtCO2 following IV injection of actual manipulated ALO-02. Finally, changes in EtCO2, SpO2, and respiratory rate over time were not analyzed prospectively and could be included in the analysis plan of any future studies.
Conclusion
The results of this exploratory analysis show a significant attenuation of the increase of EtCO2 after IV injection of oxycodone + naltrexone versus oxycodone alone, at concentrations chosen to simulate crushed and dissolved ALO-02. These results are an initial indication that naltrexone release from crushed, dissolved, and injected ALO-02 may attenuate the potentially harmful respiratory effects of oxycodone.
Footnotes
Acknowledgements
Medical writing support was provided by Diane Hoffman, PhD, Charles S. Cheng, MS, Alexandra Bound, PhD, and David Cope, PhD, of Engage Scientific Solutions and was funded by Pfizer.
Portions of these data were presented at the American College of Emergency Physicians 2015 Research Forum, 26–29 October 2015, Boston, MA, USA.
Funding
This study was sponsored by Pfizer.
Data sharing statement
Upon request, and subject to certain criteria, conditions and exceptions (see ![]() for more information), Pfizer will provide access to individual de-identified participant data from Pfizer-sponsored global interventional clinical studies conducted for medicines, vaccines and medical devices (a) for indications that have been approved in the USA and/or EU or (b) in programs that have been terminated (i.e. development for all indications has been discontinued). Pfizer will also consider requests for the protocol, data dictionary, and statistical analysis plan. Data may be requested from Pfizer trials 24 months after study completion. The de-identified participant data will be made available to researchers whose proposals meet the research criteria and other conditions, and for which an exception does not apply, via a secure portal. To gain access, data requestors must enter into a data access agreement with Pfizer.
for more information), Pfizer will provide access to individual de-identified participant data from Pfizer-sponsored global interventional clinical studies conducted for medicines, vaccines and medical devices (a) for indications that have been approved in the USA and/or EU or (b) in programs that have been terminated (i.e. development for all indications has been discontinued). Pfizer will also consider requests for the protocol, data dictionary, and statistical analysis plan. Data may be requested from Pfizer trials 24 months after study completion. The de-identified participant data will be made available to researchers whose proposals meet the research criteria and other conditions, and for which an exception does not apply, via a secure portal. To gain access, data requestors must enter into a data access agreement with Pfizer.
Conflict of interest statement
KTM and BKM are full-time employees of Pfizer and hold stock and/or stock options. AB and GW were full-time employees of Pfizer during the conduct of this study and held stock and/or stock options. LKW is a full-time employee of PRA Health Sciences (formerly CRI Lifetree), where the study was conducted. In the past 12 months, LKW received honoraria/travel expenses for consultation and advisory board participation for the following companies: AstraZeneca, Cara Therapeutics, Charleston Laboratories, Depomed, Egalet, Insys Therapeutics, Jazz Pharamaceuticals, Kaleo, Marathon Pharmaceuticals, Merck, Pfizer, Proove Biosciences, Teva Pharmaceutical Industries, Trevena, Shionogi, and Zogenix.