
Abstract
Many studies have investigated the benefits of androgen therapy and neurosteroids in aging men, while concerns remain about the potential associations of exogenous steroids and incidents of cerebrovascular events and ischemic stroke (IS). Testosterone is neuroprotective, neurotrophic and a potent stimulator of neuroplasticity. These benefits are mediated primarily through conversion of a small amount of testosterone to estradiol by the catalytic activity of estrogen synthetase (aromatase cytochrome P450 enzyme). New studies suggest that abnormal serum levels of the nonaromatized potent metabolite of testosterone, either high or low dihydrotestosterone (DHT), is a risk factor for stroke. Associations between pharmacologic androgen use and the incidence of IS are questionable, because a significant portion of testosterone is converted to DHT. There is also insufficient evidence to reject a causal relationship between the pro-testosterone adrenal androgens and incidence of IS. Moreover, vascular intima-media thickness, which is a predictor of stroke and myocardial symptoms, has correlations with sex hormones. Current diagnostic and treatment criteria for androgen therapy for cerebrovascular complications are unclear. Confounding variables, including genetic and metabolic alterations of the key enzymes of steroidogenesis, ought to be considered. Information extracted from pharmacogenetic testing may aid in expounding the protective–destructive properties of neurosteroids, as well as the prognosis of androgen therapy, in particular their cerebrovascular outcomes. This investigative review article addresses relevant findings of the clinical and experimental investigations of androgen therapy, emphasizes the significance of genetic testing of androgen responsiveness towards individualized therapy in post-IS injuries as well as identifying pertinent questions.
Introduction
Androgen therapy, especially testosterone therapy dates back to the 1960s. The rampant use and abuse of anabolic steroids occurs mostly among male athletes, who seek more muscle strength and endurance, as well as better physical performance. Various complications have been reported, including previously underreported accelerated increases in coronary artery plaque volume, 1 polycythemia and acute cerebral infarction, 2 sometimes as severe as cardiomyopathy, thrombosis and fatal ischemic stroke (IS) in a young patient. 3
Another use of androgens is largely for hormone replacement therapy, which is recommended for treatment of androgen deficiency. As men age, longitudinal studies demonstrate that androgen levels decline4,5 and neuro-endocrine aging is likely in progress, which could be reversed with testosterone therapy. 6 This therapy is indicated and of proven clinical benefit in men with primary hypogonadism (HG) having low serum testosterone levels (<300 ng/dl) or symptoms consistent with testosterone deficiency.7,8
A variety of symptoms (physical, pathophysio-logical and neurobehavioral) appear as the levels of testosterone, its metabolites, and or neurosteroids decline, or change. Testosterone therapy can improve symptoms that are attributed to testosterone deficiency, such as decreased muscle mass, bone mineral density loss and osteoporosis, decreased hemoglobin levels or anemia, 9 decreased physical activity and mood. 10 Advantageous effects for androgens, both exogenous and endogenous, have been reported to include bone mineral density, muscle mass, hemopoiesis, lipid metabolism, reducing atherosclerosis, and overall improving health and wellness and quality of life (QoL).6,9,11–13 Although previous studies suggest that testosterone supplementation may improve cognitive functions among older men, new clinical trials show that it causes erythrocytosis (hemoglobin level ⩾17.5 g/dl), with moderate or no improvements in memory or cognitive functions.13,14
There are also numerous reports about adverse effects of testosterone suppression or androgen-deprivation therapy (ADT) including gonadotropin-releasing hormone agonists, indicating cardiovascular events, strokes and occurrence of diabetes mellitus, for example,15–20 demonstrating the positive effects of androgens further.
Along with advantages of androgens, there exist disadvantages and complications. For example, a recent double-blind placebo-controlled study demonstrated that treatment with testosterone for 1 year results in a significant increase (47 mm3, p = 0.003) in coronary artery noncalcified plaque volume among older men with low testosterone (<275 ng/dl) or symptomatic HG without hypertension, myocardial infarction or stroke. Increased plaque volume means possible plaque rupture and thrombosis. However, no major cardiovascular events occurred from the baseline to the 12-month study period. 21 Others believe that testosterone therapy may improve cardiovascular outcome, and caution that accuracy of the diagnosis and appropriateness of treatment and proper follow up are important, as there is a large increase in testosterone prescriptions. 22
Many different formulations and dosage forms of androgenic steroids have been produced and improved over the years; from injectable forms, to dermal patches, gels, and pro-testosterone dietary supplements introduced in recent decades. The testosterone-stimulating compounds (pro-testosterone supplements) are indicated for boosting endogenous androgens levels.
Advances in diagnostic laboratory techniques afford accurate measurements of androgen levels, most importantly for diagnosing testosterone deficiency, and therefore, decisions for appropriate interventions are facilitated. However, functional deficiencies are probable where androgen levels are normal and steroids responsiveness is upset; and unfortunately, no validated diagnostic protocols are available for genetic testing in this regard and determining steroids responsiveness (see Genetic Testing section).
Stroke is a major cause of morbidity and mortality in aging men. Several significant articles have recently been published about the benefits and risks of administering androgenic steroids for therapy or prevention of largely nonstroke complications; while the long-term efficacy and safety of exogenous androgens are unclear for neurological conditions. Although testosterone use may be clinically beneficial for some people, its benefits and risks for the central nervous system (CNS) in the elderly, who are increasingly susceptible to brain stroke, are insufficiently investigated. Therefore, early risk stratifications can mitigate the incidents of cerebrovascular events, stroke disability and mortality, in particular as a result of alterations or imbalances in the nonendocrine levels of the brain steroids, as well as the endocrine steroids. This article focuses on these controversies and potential risks and benefits of androgens use for brain injuries and IS. In addition, select translational science studies are reviewed and discussed in the context. It provides insights into the inferences made from androgen measurements and androgen use in the clinical and experimental models of IS, and genetic testing of androgens as potential biomarkers. The following questions are primarily addressed:
□ Is androgenic therapy, inducing androgen levels above normal physiologic range, safe and effective?
□ Are exogenous steroids neuroprotective/neurotrophic or neurotoxic?
□ Can androgenic steroids affect intima-media thickness, and therefore affect future atherosclerosis and IS?
□ Do androgenic steroids (testosterone or its metabolites and precursors) cause or worsen IS?
□ Can androgens use improve QoL after cerebrovascular events?
□ Can administration of androgens and pro-androgen supplements benefit some individuals more than others (their cerebrovascular outcomes in particular)?
□ Should genetic testing strategies be implemented to predict the benefits and risks of androgen therapy?
Searching strategy
The clinical and complementary translational studies about androgen therapy and stroke, especially recent ones, are reviewed. The interactions of exogenous steroids, neurosteroids, as well as the endocrine system are discussed. The latest publications related to testosterone, and examples of its pharmacologic analogs [testosterone propionate (TP), testosterone undecanoate (TU)], leading metabolites [dihydrotestosterone (DHT)] and androgen-boosting precursors [dehydroepiandrosterone (DHEA), dehydroepiandrosterone sulfate (DHEAS)] are reviewed. Selected publications in Medline were reviewed using the listed keywords. Our assessments focused on whether these publications are proportionate with the scope and questions raised. Datasets that appeared insufficient were excluded. Some contradictory research/review findings that have exclusively underlined the positive attributes of androgens therapies, overt conflicts of interests, apparent partiality in researches, especially in company sponsored researches, were mostly excluded. Inclusion criteria were based primarily on data quality, adequacy of sample size and statistical significance.
Vascular
Proponents of androgen therapy generally advocate that men with low testosterone or HG can benefit from this therapy,23,24 and both men and women benefit from pro-androgenic supplements.25,26 A clinical study published in 2015, with retrospective data about 2 years of follow up of testosterone supplementation therapy (TST), evaluated benefits and cerebrovascular events or other suspected complications, and the results are independent of age. 24 In a large clinical trial conducted recently on a general healthcare population, men with low testosterone who were on TST marginally benefited from the risk of cardiovascular events, but also exhibited a higher trend for stroke risk. 27
Vigen and colleagues 28 previously reported that men with known cardiovascular risks who were treated with testosterone have an added risk of stroke. TST is also associated with risk of venous blood clotting in a population of relatively healthy men; it increases venous thromboembolism which peaks within the first 3 months after testosterone therapy for those with and without known risk of thrombophilia or those with and without pathological hypogonadism. 29 Relevancy of this finding to cerebral venous thrombosis is unexplored. In contrast, two other recent studies suggest that there is an inverse relation between testosterone replacement therapy (TRT) and risk of stroke, provided that testosterone is given to relatively healthy men30,31 (Table 1). Overall, these findings suggest a cautionary approach for TST, particularly in men with underlying risk factors for stroke.
Testosterone treatment and risks of thromboembolism and stroke.
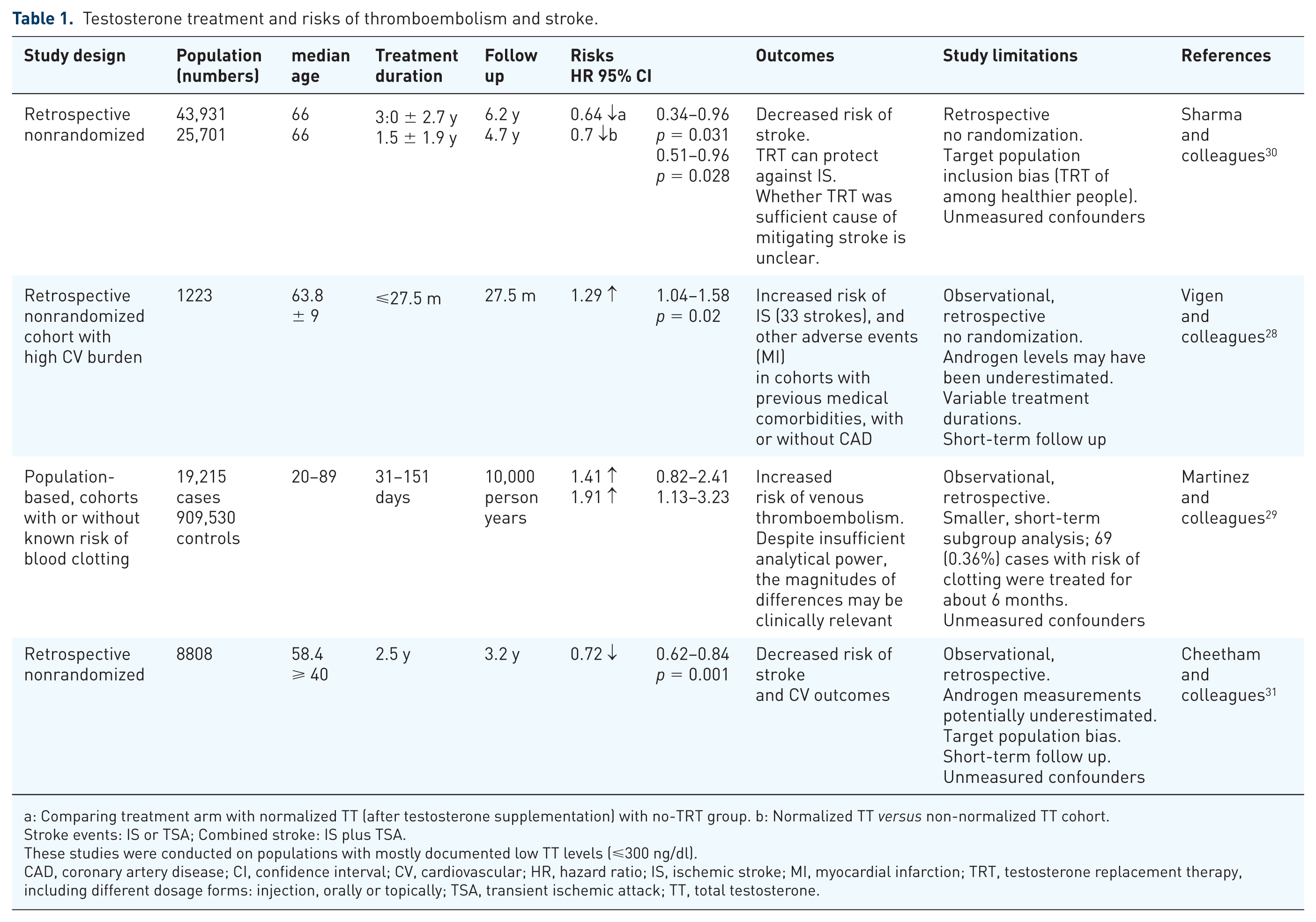
a: Comparing treatment arm with normalized TT (after testosterone supplementation) with no-TRT group. b: Normalized TT versus non-normalized TT cohort.
Stroke events: IS or TSA; Combined stroke: IS plus TSA.
These studies were conducted on populations with mostly documented low TT levels (⩽300 ng/dl).
CAD, coronary artery disease; CI, confidence interval; CV, cardiovascular; HR, hazard ratio; IS, ischemic stroke; MI, myocardial infarction; TRT, testosterone replacement therapy, including different dosage forms: injection, orally or topically; TSA, transient ischemic attack; TT, total testosterone.
Other studies focused on testosterone therapy in patients without stroke, mainly about cardio/venous thrombotic complications.23,32–34 As for other complications, although a meta-analysis concludes that short-term testosterone treatment for some routes of administration is associated with increased risk of prostate cancer (PCa), there is no compelling data to reach statistical significance of indicating testosterone treatment and increased risk of PCa. 35 Some studies demonstrate that testosterone can safely be given, even to men on prostate cancer surveillance. 36 However, others caution that TRT may promote PCa, and encourage the tracking of endogenous androgen levels and testosterone suppression therapy to lower the risks for activation/progression and recurrence of PCa cells that appear almost all androgen receptor (AR)-driven.37,38
Risk factors
Some articles highlight that DHT, not testosterone, is a major risk factor for IS. These articles might be misinterpreted, and divert attention from other major root causes of risk, such as testosterone, cholesterol and cortisol. Conversely, research on stroke models in animals can lead to serendipitous results that may look different or difficult to interpret or relate to clinical observations that suffer from their own drawbacks or a set of confounding variables. Such inconsistencies can deepen if preclinical studies are designed based upon trial and error, or likewise, if clinical investigations are conducted without a predetermined set of criteria, for example to rule out or rule in a predefined null hypothesis.
Intima-media thickness (IMT) a predictor of stroke and myocardial infarction,39–41 may have some correlations with sex hormones. In a study of 935 aging males, mean carotid IMT, metabolic syndrome, and testosterone were significantly and independently correlated with each other. 42 In a Tromsø cohort study, in North Norway 1101 men were enrolled in 1994 and were followed until 2001. They found again, an inverse relationship between total carotid plaque area and testosterone levels (p < 0.05) after adjustment for age, hypertension, smoking and use of statins, but there were no prospective associations between sex hormone levels and change in IMT from 1994 to 2001. This lack of associations may be because of increased use of antilipid and antihypertensive drugs during the study period. 43 In a three-city population-based cohort study including 354 men aged 65 and over, IMT analysis by carotid ultrasonography showed an inverse association of IMT with baseline testosterone (total and bioavailable), but not with sex hormone-binding globulin, and estradiol (E2) levels in a low-grade inflammation state. 44
A recently published article reports relationships of carotid IMT with sex hormones, in two groups with and without coronary artery disease (CAD), 426 and 496 persons, respectively. Testosterone quantity was inversely correlated with carotid IMT and prevalence of carotid plaque only in the non-CAD group. In contrast, E2 quantity was directly correlated with carotid IMT only in the non-CAD group. Increased DHT and E2 were associated with reduced carotid plaque only in the CAD group. In non-CAD men, higher testosterone had a favorable impact on carotid IMT and lowering the rate of carotid plaques, while higher E2 had worse impact on carotid IMT. In men with CAD, higher DHT or E2 were correlated with less carotid plaque. 45 The analyzed data demonstrated differential associations of endogenous androgens and common cardiovascular risk factors, including carotid IMT and atheroma, as clinical surrogate endpoints. 45 The study suggests that high DHT, like E2, may be neuroprotective. However, it does not indicate a causal relation between high testosterone in connection with TST, as predictive biomarkers for stroke mitigation in men. In addition, any added benefits and risks of testosterone may depend upon treatment configuration (dose, duration/frequency, route of administration) and underlying risk factors.
Cerebrovascular events
Few studies have addressed the threshold levels of all androgens in blood/plasma and the effect site. In the analysis adjusted for stroke risk factors, longitudinal studies on 1032 men, with a median of 10 years of follow up, show that both high and low plasma levels of DHT (above or below 50–75 ng/dl) are associated with a significant risk of stroke (114 of 1032; 11%, p = 0.006). 46 It shows that abnormally high and low levels of DHT, but not total and free testosterone, are associated with increased incidences of IS. 46 This analysis excluded the men who were on androgen suppression therapy or finasteride, a 5-alpha-reductase inhibitor to lower DHT. Consistent with this observation, it has been recommended that testosterone use in elderly men should be restricted to known low-T levels and thereby clinically justified, because aging men sustain higher incidents of stroke than women.47,48
A separate larger cohort study followed up for 8 years differs from the Shores 46 findings, and demonstrates that elevated levels of circulating androgens decrease incidents of stroke nearly in half [testosterone, hazard ratio (HR) = 0.56, or DHT, HR = 0.57, p = 0.002]. 49 However, multiple adjustments were made in regard to conventional stroke risk factors that could have contributed to the observed outcome, suggesting that higher testosterone (455–1340 ng/dl) and DHT (53–209 ng/dl) are independent significant predictors for the reduced nonfatal and fatal stroke, but not myocardial infarction in older men. This observational study discriminated reasonably well by including nearly all healthy participants in one community, and the assessment did not track the outcomes in men prescribed androgens in randomized clinical trials.
A parallel investigation by Shores reported 436 cerebrovascular disease events in these men, and 777 all-cause mortality cases occurred during the first 9 years of the follow up. 50 Unless proven otherwise, these observations imply that a portion of testosterone can cause stroke through its conversion to DHT or lack thereof. Likewise, alterations in the androgenic pathways and the concentrations of androgens in the effect sites, as well as total and free plasma levels of testosterone and its metabolites, can influence cerebral tissue.
Furthermore, levels (and relative ratios) of the free circulating testosterone and its metabolites and precursors can serve as biomarkers, which together may provide predictive clues for their impact on cerebrovascular events. These studies45,46 raise further questions for continued investigations of cerebrovascular outcomes in men on androgens. Plausible scenarios are illustrated (Figure 1).
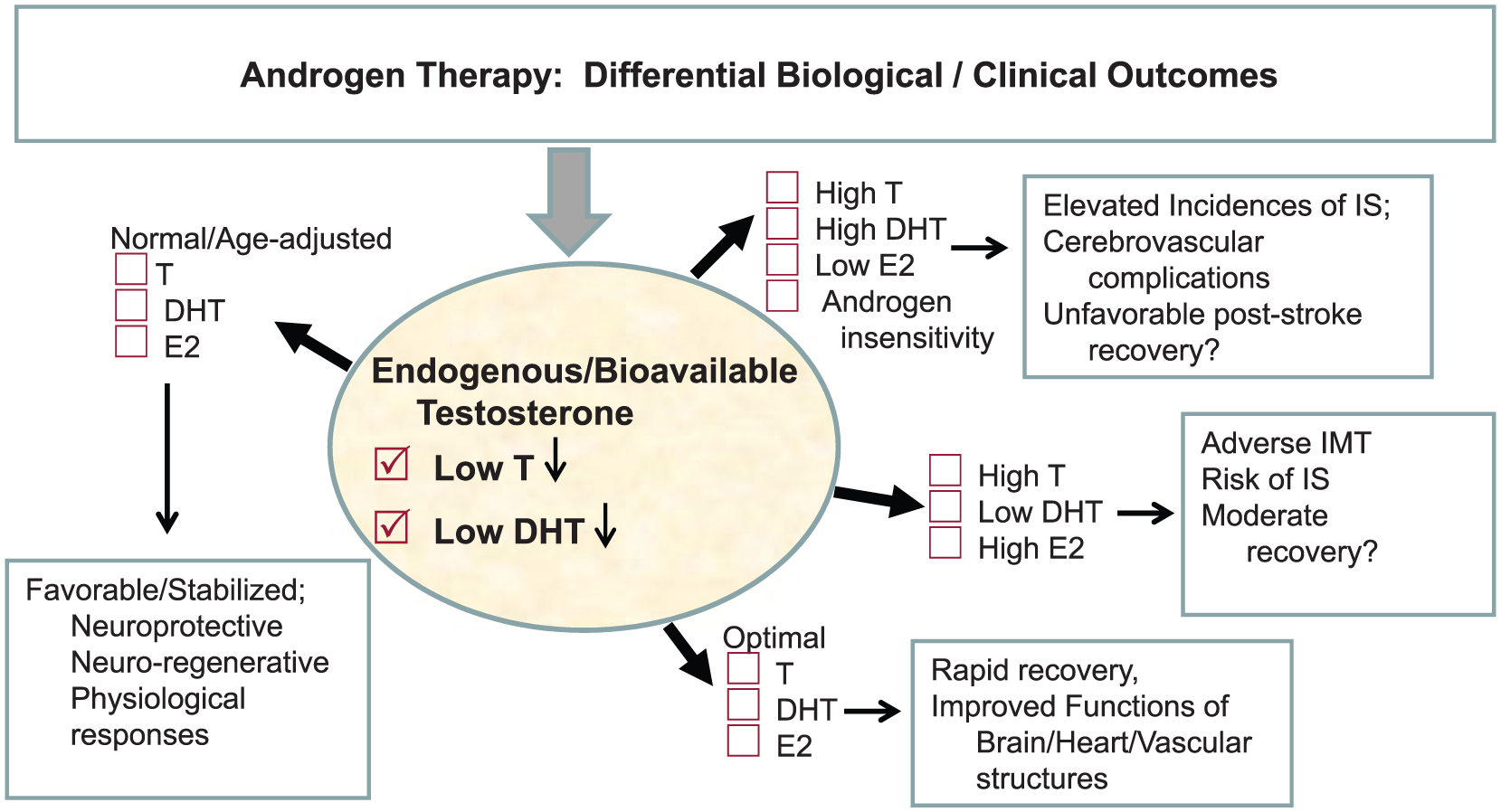
Androgens impact on cerebrovascular outcomes. What might occur when testosterone or a pro-androgen is given pre- or post-brain injury? Androgens can be either neuroprotective or suboptimal/destructive; such outcomes maybe related to their variable ratios of total testosterone (low < 300, normal 300–742, high > 742) with its metabolites (e.g. high testosterone + high DHT + low E2) or (high testosterone + low DHT + high E2) at the effect site. Neuroactive steroids, biochemical conditions and functionality of the endogenous steroids can influence cerebrovascular pathology. Potential added benefits of testosterone may in part be mediated by its metabolites DHT and E2, and depend upon the functionally of the steroidogenesis enzymes. In the event of IS/cerebrovascular injury, changes in steroids can exert distinct biological and clinical outcomes.
Mechanisms, translational studies
Neuroprotective and trophic effects of testosterone have been primarily attributed to nonandrogenic metabolic processes without sufficient clinical evidence. For instance, data extrapolated from stroke-induced experimental animals to human stroke have demonstrated neuroprotection after progesterone treatments. Translational applications of this knowledge were discouraging when two multi-center phase III clinical trials failed to demonstrate benefits for patients with traumatic brain injury (TBI). 51 In light of these disappointing outcomes, further clinical developments for IS appear on hold, subject to an in-depth investigations with a back-to-basics consideration of questions on issues such as possible interaction of progesterone with tissue plasminogen activator (tPA), sex-specific effects, and development of progesterone receptor-specific targets. 51 Meanwhile, new promising studies on mice suggest a sex difference in stroke effects affecting brain respiratory chain reactions and actions of progesterone on mitochondrial functions, which might participate in its neuroprotective properties. 52
In other areas of research, small cross-sectional clinical studies propose that pre-screenings for certain serum biomarkers (e.g. tests for thrombophilia and thrombosis) can provide clues to prevent testosterone-induced vascular thrombotic events.32,33
After injury, scar tissue is triggered via apoptotic activations and hence a loss of astroglial and neural cells, collectively referred to as astrogliosis. 53 This phenomenon is affected by androgens, as explained below.
Aromatization of testosterone generates E2. This reaction usually occurs in nonendocrine cerebral cells, and can be activated in responses to the brain injury. In cerebrovascular accidents (e.g. as a result of cranial trauma and brain hypoxia), a selective expression/activity of aromatase and production of estrogen, promotes the release of neurotrophic factors. In male rats, the locally available testosterone and its metabolites in the brain, especially E2, decrease reactive astroglia, reduce infarction (pathological gliosis), enhance survival of the neurons, and improve/stimulate neuroplasticity or neuronal cell connectivity. 53 Therefore, the brain aromatase in turn is neuroprotective. This enzyme is found in mammalian radial glia and neural progenitor cells. 54 In stroke models in rats, a timely expression of the estrogen synthetase [aromatase cytochrome P450 (CYP450)] initiates and increases the production (and enables distribution) of estrogen in astroglial cells. This molecular reaction mitigates gliosis and induces neuronal repairs, shortly after the brain injury. 55 Similar conditions were observed in estradiol-treated mice after an ischemic cerebral injury which involved numerous other intermediary elements, for example hypoxia-inducible factor 1-alpha (HIF-1α) and vascular endothelial growth factor in infarct zones. 56 Ischemic-induced cellular responses in relations to endogenous androgenic signaling mechanisms may lead to opposing beneficial and detrimental effects.53,56,57 Deprivation of testosterone and E2 and a simultaneous activation of cortisol syntheses are possible mechanisms for a compromised neurogenesis and slow functional recovery in aging (male)-dominant stroke events.
Does DHT impact on the outcomes of brain stroke?
Testosterone-treated animals, but not DHT-treated, exhibit decreased infarct volumes (20 versus 33%, p < 0.05). This beneficial effect was attributed to increased E2 levels in testosterone-treated animals. In addition, administration of testosterone to male rodents increase testicular aromatase (P450arom) levels (3.6 versus 0.2 ng/ml, p < 0.0001). 58 E2 derived from such reactions can positively modulate neurotrophic factors involved in neuroprotection and repair.
The question as to why males sustain a greater neuronal damage after cerebral injury has eluded researchers for decades. Dose response studies on a cardiac arrest/cardiopulmonary resuscitation (CA/CPR) model in male mice revealed that testosterone can increase neuronal tissue damage following global cerebral ischemia. 59 The observed outcome was dose dependent: moderate amounts of testosterone showed no dangerous effects, whereas high or low doses exacerbated neuronal damage and sensorimotor deficits. Given that flutamide inhibited these negative effects, the ARs were presumably engaged in the process; although this does not seem that testosterone triggers such outcomes. However, it’s clear that sex-linked differences in cerebrovascular events can be rooted in the unusually low/high levels of testosterone.
Consistent with this, supraphysiological doses of testosterone and DHT abolish neurogenesis in germinal areas of dentate gyrus in damaged striata in adult male mice, which were subjected to transient middle cerebral artery occlusion to induce ischemic damage. 57 Therefore, TST with high plasma levels of the bioavailable testosterone may trigger similar unfavorable outcomes, which can inhibit neural cell repair and recovery. Signs of post-ischemic neurogenesis were undetectable when AR was blocked by flutamide or when animals were castrated, suggesting that endogenous androgens do not overtly affect post-ischemic acute brain injury. A continuous blockade of AR suppresses the maturation of newborn neurons in dentate gyrus. 57 Further improvements to the damaged tissue or motor functions were not explored.
High doses of either testosterone or DHT exacerbates the cerebral infarcts, which were inhibited by the testosterone competitor flutamide, although restoration of the physiological levels of testosterone (before and after an acute ischemic reperfusion injury) in surgically-castrated mice result in smaller infarct sizes and better motor functions. 60 These observations seem to point out that testosterone-mediated reactions can benefit neuronal damage and cerebral infarctions provided that its levels are kept within a ‘normal range.’ These outcomes can be summarized as follows:
Testosterone can cause neuroprotective and neurodamaging effects on cerebral tissue, depending upon the amount and dose/timing of the treatments, before or after an IS attack.
Anti-testosterone pharmacotherapy or a concurrent treatment with antiandrogen medicines, like flutamide, can hinder recovery of the damaged neurons, if utilized in acute IS.
The aromatization of testosterone precursors to E2 are well documented in studies conducted over a decade ago in the aromatase knock-out experimental stroke models and other degenerative brain disease models in mice.61,62 In these investigations, aromatase is either pharmacologically inhibited or structurally/functionally impaired, and the neuronal cell repair can presumably be undermined after stroke. Further research is needed to differentiate the core risk factors in IS in relation to the dynamics of endocrine, nonendocrine, and neurosteroids network, and underlying genetic components.
Testosterone and DHT
The underlying causes of IS are diverse and multifaceted and maybe related to acute vascular thrombosis, blood clots or atherosclerosis, blood pressure, trauma, or other causes, some of which might be influenced by testosterone and its metabolites, DHT and E2. DHT is nonaromatizable metabolite and the most potent form of testosterone, which is present in the brain and other organs, such as liver, muscles and skin. Elevated activity of 5α-reductase or its reactive end product DHT can negatively influence the human body fat distributions, a generally recognized risk factor for cardiovascular disease. 63 Overall, DHT is like a ‘double-edged sword’: its high and low levels are detrimental. However, positive regenerative/neuroprotective attributes of testosterone might outweigh its negative effects. This may depend upon many other interactive medications, such as 5α-reductase inhibitors, as well as the endocrine system and nonendocrine androgens homeostasis in the brain.
Pharmacology and biodistribution
Many different dosage forms of androgens have been approved, and some of which are in active trials for enhanced or expanded indications (www.clinicltrials.gov). Distinct synthetic formulations such as testosterone esters (e.g. TP and TU) and anabolic steroids are derivatives of circulating endogenous testosterone synthesized largely by Leydig cells in the testis. Both pharmacologic and endogenous testosterone is metabolized to the more potent metabolites, DHT and E2. 64 Androgens used by intravenous injections or other routes of delivery, in addition to increasing levels of circulating testosterone, can target the brain by crossing the blood–brain barrier, or enter directly by diffusion through brain tissue and transport through nerve projections. 65 Testosterone can distribute and accumulate in most brain regions where it can be modified enzymatically in vivo, partly converted into DHT and partly to E2, and can elevate levels of other neurobiologically active compounds.65,66 TU is a long-acting formulation and administered in aging men with mild-to-severe testosterone deficiency. 67 To the best of our knowledge, there is no organized documentation or registry about men with stroke risk factors, or with cerebrovascular events, utilizing different forms of androgens.
Testosterone can exert positive neuroprotective and negative neurotoxic effects, largely through the activities of its metabolites, E2 and DHT. The information extracted from above clinical and translational studies is illustrated in Figure 2.
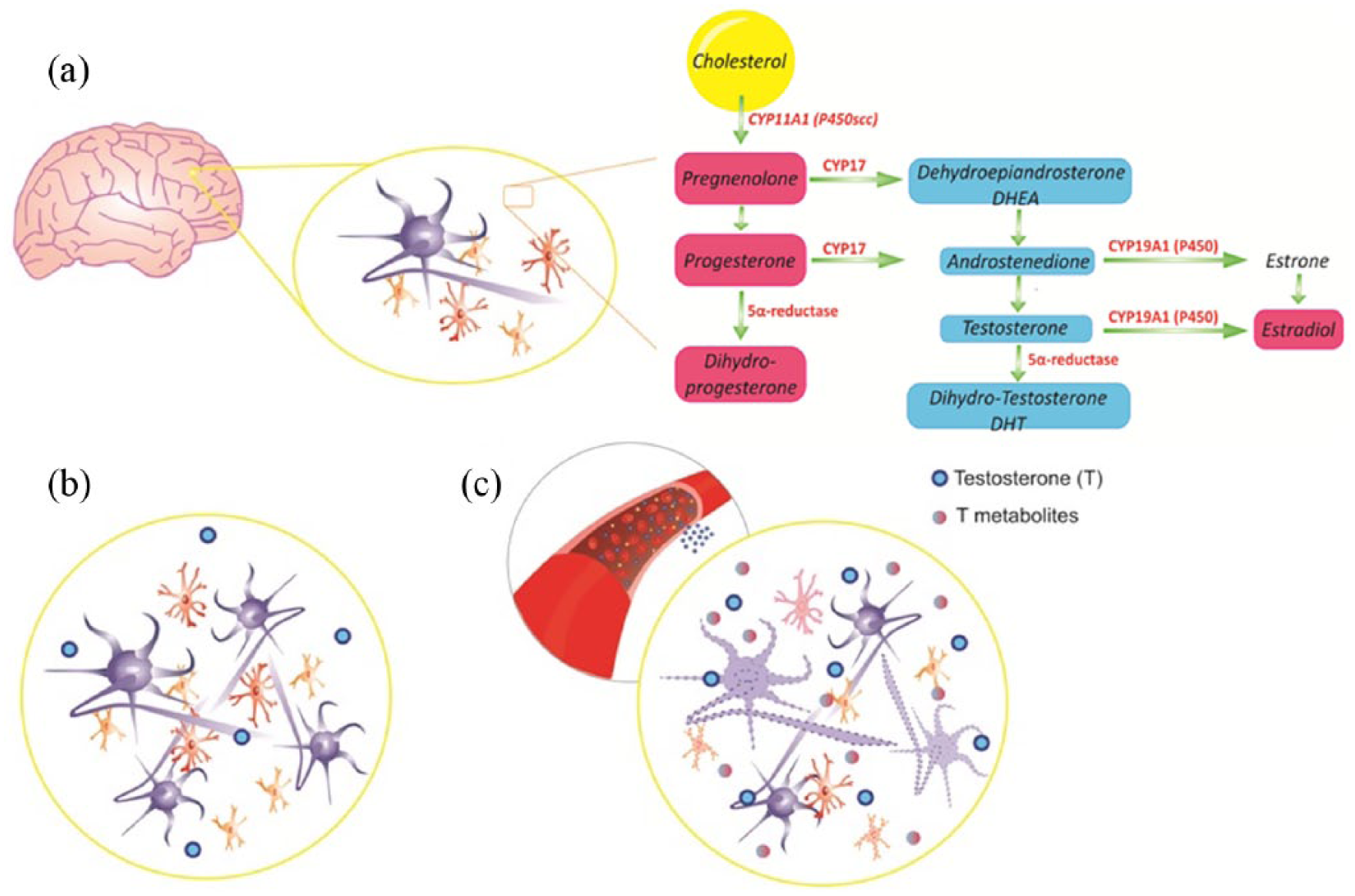
A schematic overview of testosterone and other steroids in the brain: (a) Indicates the metabolic pathways beginning with cholesterol and producing testosterone and other steroids by the enzymes involved. The very complicated pathways have been abstracted. (b) Endogenous testosterone, apart from modulating the HPA axis, has neuroprotective effects in the CNS, including neurogenesis, survival of the neurons and neuroglia, functional reconstruction of neural networks. It can also overcome IS injury-induced brain damage. (c) Exogenous testosterone, in particular in a supraphysiological dose, floods the brain through the blood vessels. Testosterone or its metabolites can then interfere with biosynthesis of neuroactive steroids, or changes in endogenous neurosteroids, and induce apoptosis of the cells in the nervous system.
The positive attributes of testosterone (or its potent metabolites DHT and E2) can diminish and physiologically become less and less effective, in hypogonadal men and elderly men for a variety of other reasons. Such biochemical unresponsiveness may greatly be subject to metabolic or lifestyle differences and other confounding variables, and importantly, to intra- and inter-individual genetic variability in the steroids processing enzymes (see further).
Aromatization of testosterone
Aromatase or estrogens synthetase (CYP450 19A1) can convert testosterone to 17β-estradiol (E2) within the CNS cells. This key enzyme, if genetically mutated, can become functionally suboptimal or inactive in the brain tissue; thus, any of its significant positive attributes, such as neuroprotective/neurotrophic effects, may be compromised. Importantly, variations in the aromatase gene or its expression can influence both the endocrine and nonendocrine androgens, and hence, invariably affect the brain injury outcomes. Aromatized steroids can mediate expressions of the neurotrophic factors, for example nerve growth factor and brain-derived neurotrophic factor (BDNF),68,69 and promote neurogenesis in distinct regions of the brain, including the hippocampus.69,70
Through the brain aromatase activity and related cellular and molecular mechanisms, testosterone, in physiological concentrations, can mitigate the infarcts and cell damages, improve motor functions and cognitive deficits after stroke. Conversely, testosterone metabolites or precursors, for example DHEA and DHT, can induce apoptosis-inducing signals, and de novo formation of gliosis or scar tissues, which would take time to develop but are thought to slow down the spread of hypoxic cell damage in infarct zone. 71
Detailed findings expand the above hypothesis and suggest that inter-individual differences in androgen metabolism can affect the individual’s ability to recover from stroke. E2 and its metabolite methoxyestradiol (2-ME) are known to inhibit microglia proliferation, proinflammatory responses and phagocytosis, key steps in stroke recovery. 72 The effects of 2-ME are mediated partly in an estrogen receptor (ER)-independent mechanism, while the effects of estradiol, 2-hydroxyestradiol (2-OE; estradiol metabolite produced by CYP450), and 2-ME [produced by catechol-O-methyltransferase (COMT) and its metabolites] are regulated by multiple enzymes. For instance, inhibition of COMT selectively blocks the conversion of 2-OE to 2-ME and the antimitogenic effects of 2-OE, but not 2-ME. 72 Thus, pharmacological inhibitors of CYP450 and COMT, as well as aromatase imitated reaction of the testosterone metabolites are sensible targets for individualized diagnostics and therapeutic interventions in IS brain injury.
DHEA
DHEAS
Pharmacologic (testosterone-boosting) steroids DHEA and its sulfated metabolite DHEAS have been developed as cognitive-enhancers and energy-producing nutritional supplements in the market. These steroids are available in many countries, and are currently over-the-counter medicines in the United States (US). Administration of DHEA elicits cognitive improvements in nonstroke patients25,26 and multi-infarct dementia. 73 Both compounds (DHEA/S) are commonly produced by the adrenal glands, gonads, and brain. 74 They are the most abundant neurosteroids synthesized in the glial cells of the CNS. DHEA is converted to testosterone by reactions of the 3- and 17-beta-hydroxysteroid dehydrogenases (3β-HSD, 17β-HSD) (Figure 2). DHEA/S are indicated for rehabilitation of TBI patients, and for healthy adults as ‘cognitive-enhancers or de-stressors’. Overall, DHEA is attributed mostly for its anabolic properties, whereas DHEAS purportedly for its broad neurobiological (neuroexcitatory, neurotrophic, neuroprotective) attributes.25,26,74
In a cohort of 231 acute IS patients, DHEAS [odds ratio (OR) 1.21, 95% confidence interval (CI) 1.01–1.49], but not DHEA (OR 1.01, 95% CI 0.99–1.04) was prognostic for adverse functional outcomes of stroke. 75 Consistently, lower levels of DHEAS are associated with a greater risk of IS in women (relative risk = 1.41; 95% CI 1.03–1.92). 76 No further studies have examined DHEAS levels and the risk of IS in men. Continued research suggests that DHEAS relieves clinical signs of occupational stress disorders, such as excess stress in military personnel, whether male or female, based on limited cross-sectional clinical and preclinical research. 26 The sample sizes of these studies are small, and they are based upon limited clinical endpoints and follow ups.
Administrations of DHEA (20 mg/kg) during 3–48 h after transient global cerebral ischemia in male rats, exhibit neuroprotection, a reduction of ischemia-induced neuronal death in the hippocampal CA1 and improvement of ischemia-induced learning deficits. However, DHEA treatments shortly (1 h) before or after cerebral ischemia is neurotoxic: it exacerbates the neuronal damage. 71 Although DHEA is thought to boost the release and activity of testosterone, the mechanism of its neurotoxicity is quite unclear. One plausible explanation is that DHEA augments DHT release/activity. It can also indirectly increase intracellular Ca(2+) concentrations through stimulation of the N-methyl-D-aspartate receptors in cerebral impairments. 71 This study indicates that the timing of DHEA treatment is critical when there are acute ischemic brain cells. This can result in apoptosis/neuronal cell damages and cognitive (learning/memory) injury.
There are two cardinal questions remaining that require longitudinal studies: Do DHEA/S supplementations bring promise or peril to IS (acute/chronic) patients? How efficacious are these agents, if examined in a non-inferiority clinical study, relative to a prescription-based androgen?
Genetic testing
There is a high probability that genetic predisposition or prevalence of a particular set of genomic signatures of the androgenic metabolizing enzymes or AR impact on androgen efficacy and safety. Genetic testing for enzymes involved in processing or syntheses of steroids (such as aromatase, CYP450 family of genes) in relation to androgen use and brain injuries in humans have not effectively been explored. It may provide clues to predict therapeutic responsiveness and tolerance to androgens, adverse outcomes, as well as susceptibility to antiandrogen medications, such as inhibitors of the 5α-reductase, aromatase or CYP450. Such biomarkers can be useful in forecasting the androgens efficacy and toxicity. Therefore, aberrant or suboptimal activities of these genes may influence the risks and outcomes of androgen use.
One of the advantages of pharmacogenetic measurement is that it can aid to determine the risks, and hence, adopt appropriate interventions, while forecasting the treatment outcomes. Individuals that have either low metabolizers or high metabolizers of androgens may be at a higher risk of stroke. There is a high probability that:
Utilization of pharmacogenomics data (e.g. biomarkers of 5α-reductase and aromatase CYP450 genes) can aid in predicting androgens responsiveness, and prognosis of brain stroke/injury outcomes.
Individualized optimization of brain steroids through appropriate interactive medications may facilitate the neural repair and recovery after stroke.
For instance, CYP19A1 polymorphisms and clinical outcomes were evaluated in relation to the daily endogenous testosterone quantity and E2/testosterone ratio in cerebrospinal fluid (CSF) and serum samples from 110 adults with severe TBI, and the datasets were compared with those from healthy individuals. 77 Patients with brain injuries initially had high endogenous testosterone, but the serum and CSF testosterone levels declined over time, with a concomitant decrease in E2 levels. Higher CSF E2/testosterone ratios were associated with better clinical outcomes, as well as lower mortalities (p = 0.019) and better QoL scores (p = 0.030). Conversely, individuals with multiple mutations in this enzyme exhibited worse outcomes. With an extensive search we found no studies evaluating the pharmacogenetic profiles of stroke patients in relation to steroid therapy. However, the above evidence implies that CYP19A1 gene variations can markedly affect the pharmacodynamics of the steroidal interventions, as well as homeostasis of the endogenous endocrine dynamics during acute and chronic phases of brain injury and stroke. Thus, an independent set of risk factors or covariates such as loss of function or inhibition of certain genes involved in the hypothalamus pituitary adrenal (HPA) axis, cholesterol metabolism and optimal ratios of neuroactive steroids in the brain, or in cholesterol side-chain cleavage enzymes that synthesize neurosteroids, can all affect the pathology of neuronal injury and IS (Figure 2).
As another example, translational studies in mice suggest that polymorphisms of cholesterol 24-hydroxylase (CYP46A1) gene, which converts excess cholesterol to 24-hydroxy-cholestrol and exports it from the CNS to blood circulation, is associated with brain atrophy. 78 Inhibition of CYP46A1 results in accumulation of cholesterol in the neurons, which leads to cognitive deficits and atrophy of hippocampus, because of apoptotic neuronal death. 79
Androgens and corticosteroids appear closely involved in acute stroke pathology. A recent prospective clinical study suggests that elevated levels of DHEAS correlate with increased release of cortisol, and then with severity and poor functional outcomes and mortality of stroke in men. 80 Alteration in HPA axis activity can arise in part from genetic polymorphisms in enzymes involved in steroidogenesis, in addition to external stimuli and corticosteroidal responses. For instance, activity of the 11β-Hydroxysteroid dehydrogenase type 1 (11β-HSD1) converts inert cortisone to active cortisol. Increased cortisol synthesis is associated with incident depression (HR 1.28, 95% CI 1.03–1.59). 81 Such variability can impact on both nonendocrine and endocrine androgens, which might undermine the effectiveness of medicinal androgens. Consistent with other degenerative conditions such as multiple sclerosis (MS), pharmacologic corticosteroids can worsen neuronal damage, inhibit proliferation of astroglial precursor cells, and inhibit remyelination and neuronal repair.82,83 Hence, variability in the responsiveness or resistance to steroids may be traced to differences in the genes and activities of the enzymes that catalyze pharmacologic and endogenous steroids in the brain.
Ultimately, genetic testing of the enzymes that catalyze cholesterol, or are involved in the HPA axis and nonendocrine regulations, for example cholesterol 24-hydroxylase (CYP46A1 gene), 11β-HSD1, aromatase CYP450, and 5α-reductase, may provide key information about ‘missing links’ in the prognosis of androgens efficacy and safety in cerebrovascular events.
Discussion
Upon review of the literature, there are many gaps in the clinical, epidemiological and translational studies concerning the safety and efficacy of the testosterone and its metabolites in IS. It is generally known that in aging men after their forties, compared with adolescents and adults, the process of tissue repair and recovery slows down.
Androgens therapy improves symptoms of testosterone deficiency with no major safety concerns for cerebrovascular events, are based on short-term observational studies. The unwanted risks next to intended (e.g. myotrophic) effects may depend upon partially dissociable functions of the synthetic androgens, and dosage forms (pro-androgenic, anabolic steroids, and modified formulations). Anabolic steroids or so-called dietary supplements (androstenedione, androstenediol, DHEA) are utilized for boosting testosterone or estrogens. The US Food and Drug Administration regulates anabolic steroids or ‘testosterone adjuncts’, except oral supplementation by DHEA/S, which remain unregulated since these compounds are not considered anabolic steroids. DHEA can increase androstenedione, free testosterone and estrone levels and decrease body fat mass. 84 Reported cases of anabolic steroids use and increased risks for plaque volume, thrombosis and stroke, call for further investigations on these public health issues, as well as androgen supplementation therapy.
Most translational studies are conducted in young and healthy rodents. Such disease models may not exactly mimic acute stroke, slow recovery and cell repair which occur in older men. An example of the aging process is the decline of androgens. Low androgen levels exists in hypogonadal men even in early aging. One recent article shows an improvement in QoL in hypogonadal men, independent of age. 24 Most studies that were reviewed between 2007–2009 focused on the beneficial effects of TST, together with recent reviews, largely conclude that testosterone use should be restricted to testosterone-deficient men.47,48 However, treating late-onset HG or older men with low testosterone requires an advanced algorithm and optimized strategy to improve promises and minimize CNS perils. Small cohort studies can introduce limited or skewed information. Since steroids utilizations seem prevalent, high-powered prospective studies are needed to calculate the HRs and relationships about androgens deficiencies, TST, brain and stroke.
An established association between high testosterone levels and PCa is a myth, although traditional science data recommend androgen suppression therapy and tracking diminished serum testosterone threshold levels of ⩽20 ng/dl. 38 However, favoring testosterone supplementation by promising health benefits for men with PCa 85 and opposing the traditional views that supraphysiological concentrations of androgens can influence progression and recurrence of PCa cells, 86 may further spike a widespread use of androgens in the general population, and elevate other safety concerns. Thus, underlying biochemical and genetic risk factors should be considered prior to implementing a strategy for androgen use.
Another recent clinical study indicates that cortisol levels are high during the first week after stroke, and are associated with disability, morbidity and mortality. 80 The study has several limitations, as pointed out by the authors; for example, fluctuations in DHEA/S and cortisol depend upon intra-individual and inter-individual variability. Also, for a small number of patients (9 of the 231) oral corticosteroids were administered, which presumably lowered their DHEA and stimulated cortisol, with no changes in DHEAS levels. The study fails to reject a causal relationship between activation of the HPA axis and stroke onset, since the samples were not collected before the onset. 80 Likewise, datasets derived from translational models should be cautiously interpreted; for instance, lacking 17α-hydroxylase (CYP17) in rodents can result in synthesis of corticosterone instead of cortisol. 87
Cortisol levels may be an independent biomarker for risk in relation to stroke in humans; although sex hormones (testosterone, DHT, E2) and corticosteroids are known to essentially originate from cholesterol by cleavage enzymes acting on cholesterol side-chains, androgens are not ordinarily converted to cortisol or vice versa. Because cortisol is nonaromatized, its elevation might partly signify anti-inflammation/tissue destructions in the CNS (generation and restriction of astrogliosis and edema) and partly other elements, such as psychometric measures. This phenomenon is important and might occur more in hemorrhagic stroke than IS.
DHT, a nonaromatizable potent form of testosterone, is produced via an irreversible reduction of testosterone by catalytic activity of 5α-reductase. Detrimental effects of DHT can originate from testosterone, particularly in supraphysiological levels, which may shunt excess testosterone levels to DHT, as well as to E2. Therefore, androgenic risk factors for cerebrovascular events may fluctuate, depending upon which steroidal pathway prevails.
Testosterone, DHT and E2 are differentially associated with preclinical carotid atherosclerosis in a cardiovascular phenotype-specific manner. Higher testosterone is associated with more favorable carotid IMT and lower prevalence of carotid plaque in community-dwelling elderly men, while higher DHT and E2 are associated with lower prevalence of carotid plaque in men with pre-existing CAD. 45 Comparison of different clinical studies suggest that, on one hand, higher testosterone levels are associated with reduced vascular IMT and lower prevalence of carotid plaque IMT, 45 thus presumably lesser risk of stroke and myocardial infarction in men with CAD. On the other hand, both high and low plasma levels of DHT are associated with an elevated risk of stroke. 46 These studies have utilized inconsistent outcome measures. Thus, a meta-analysis to reconcile the conflicting observations would be challenging. However, changes in levels of testosterone and its metabolites are obvious biomarkers for prevention or susceptibility of atherosclerosis and therefore can affect risk, outcome and prognosis of related stroke.
On the contrary, considering the proposed beneficial effects of androgenic treatments, the question is: how should androgens be clinically offered, when and in what treatment configurations (dose frequency/intensity, route of administration, cumulative exposure)? The answers for these questions require subgroup analyses on longitudinal, randomized clinical investigations to monitor the safety and efficacy of androgens in brain injury and stroke. Most clinical studies have focused more on the cardiovascular risks than cerebral risks. Many publications endorse the positive biological attributes of testosterone-boosting compounds, although some raise overall cautionary notes. Sparse studies compare testosterone and E2 effects within the same study design. Insufficient sample size, in the matter of number, sex, age, demographic and ethnic varieties are notable.
Recent meta-analyses on cohorts of general populations followed up for 29 years raise an uncertainty as to whether or not low testosterone is the cause or consequence of a poor metabolism and IS. This study indicates that a large number of men (524 of 4615) and women (563 of 4724) developed IS, but only low concentrations of endogenous testosterone were associated with a 33% increased risk of IS in men and 44% in men who were overweight/obese and hypertensive. 88 Other extreme concentrations of testosterone or E2 as risk factors were excluded. In this study, inter-individual variability and insufficiency of outcome measures limit the ability to draw a firm conclusion on the role of other androgenic metabolites in the observed IS events.
Study limitations
Recognizing limitations of the observational studies (Table 1), to make extrapolations or inferences for caution or benefits and risks of TST to the general population are challenging. First, associations between the distinct treatment effects and observed risks, HRs, may have been compromised, as selection biases exist in target populations in most studies. Second, the magnitude or distribution of true effects of the drug–event pair can be masked as a result of disproportionate reporting, 89 (i.e. measures of disproportionality associated with the 95% CIs between the treatment effects and underlying causes are unavailable). Third, the decreasing risk estimates are based on a relatively healthy proportion of the population. Fourth, the rate ratios of the outcomes were adjusted for all confounders, without a documented evidence of absence for underlying risk factors in all follow ups. Thus, the study heterogeneity and study methods can account for significant differences in outcomes. Fifth, treatment effects can also be gradual and occur beyond the data range or study endpoint, akin to the chronic low or high endogenous DHT levels that were correlated with an increased risk of stroke.
Some studies that rely on subject-reported outcomes, including psychological and QoL measurements, may add more complexity to data interpretations. Many studies conclude that TST and androgens supplements improve QoL. Few studies address the adverse events and risk stratification. Other issues can include limited study variables or outcome measures, or impartial interpretation of the data. Thus, the available labeling information for steroid use in men is insufficiently clear, largely lacking adequate evidence-based science. The Endocrine Society clinical practice guideline vaguely recommends against the use of testosterone for women for various biological, cognitive, and physiological indications. 48 A similar guideline is unavailable for men, but needed. A prospective randomized controlled trial in post-‘man’opausal men androgen supplementation versus placebo with predetermined criteria will conclude the sex-specific steroids effect for males known for a high risk of cerebrovascular events. In addition, considerations given for the use of genetic biomarkers can provide supportive information in elucidating the benefit–risk profiles of neuroactive steroids.
Conclusion
New clinical and translational studies suggest that testosterone in excess may in part convert to DHT and expose its deleterious effects, rather than the neuroprotective attributes of conversion of testosterone to estrogen. Atypically high and low DHT levels appear as risk factors for stroke. Insufficient data are available to reject a causal relationship between androgens or pro-androgenic steroids and incidences of acute cerebral infarction. Although testosterone supplementation may increase coronary artery noncalcified plaque volume, a risk factor for thrombosis and ischemic attack, significant changes in atherosclerotic intima thickening may also occur in major arterial locations. Long-term health benefits of androgens supplementation in androgen-deficient individuals in relation to cerebrovascular events are unknown. These concerns call into question the likelihood of distinct genetic biomarkers and predispositions (e.g. high metabolizers versus low metabolizers) that may influence the efficacy and safety of pharmacologic androgens. These hypotheses require further research to determine the relative/absolute HRs to complete risk stratifications of androgen use in the general population.
Footnotes
Acknowledgements
All authors contributed to the writing of this article.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The authors declare no conflicts of interests with respect to the research and publication of this article. The opinions and conclusions of the authors are provided solely for the purposes of medical and scientific advancements.