
Abstract
Immune thrombocytopenia (ITP) is an autoimmune disorder that induces a decrease in the number of circulating platelets due to spleen destruction and inability of megakaryocytes to restore normal counts. Immunosuppressive therapy with glucocorticoid drugs constitutes the first line of treatment. However, lack of response to these agents is not uncommon, and the management of refractory patients is a matter of controversy. In fact, day-to-day clinical practice shows that, in spite of the current guidelines, splenectomy, which is currently considered a suitable second-choice therapy, is being replaced by treatment with thrombopoietin receptor agonists. These boost platelet production by megakaryocytes. The use of one of these, namely eltrombopag, has been permitted for ITP patients refractory to first-line drugs or splenectomy, for the last 10 years. This review summarizes the experience reported using eltrombopag in ITP, paying attention to efficacy and safety. Results from clinical trials will be discussed, and studies performed in the course of daily clinical practice will also be reviewed, as these are useful to assess the potential of the drug in real-world settings. The management of adverse events and the use of eltrombopag in particular situations will also be covered. The experience reported so far permits us to suggest that eltrombopag efficiently induces recovery of platelet counts. Furthermore, recent papers have demonstrated that a sustained response after discontinuation, initially thought to be problematic, may be possible in a nonnegligible number of cases. The safety profile is satisfactory, although patients presenting with thromboembolism risk factors should be treated with caution until the eltrombopag-associated prothrombotic risk is fully established. In summary, although larger studies are still needed to clarify some issues, eltrombopag may be a useful alternative tool for ITP patients refractory to conventional medical management or splenectomy.
Immune thrombocytopenia
Immune thrombocytopenia (ITP), formerly known as idiopathic thrombocytopenic purpura until the Vicenza Consensus Conference, 1 is an autoimmune disorder characterized by an abnormally low number of circulating platelets, <100 × 103/µl, which promotes purpura, petechiae and bleeding episodes, whose seriousness depends on the location. 2 The most severe manifestation is intracranial hemorrhage, whose frequency is estimated to be ~1.4% in adults and 0.4% in children, and occurs specially when the platelet count drops below 10 × 103/µl. 3 The incidence of primary ITP in adults is 3.3/100,000/year. ITP incidence is multimodal and exhibits three peaks in children, young adults, women aged 30–40 years, and the elderly. The prevalence in adults is 9.5/100,000.2,4 The mechanisms that promote ITP are rather complex and poorly understood, although it is well known that antiplatelet autoantibodies play a central role. These appear as a consequence of an altered T-cell response, in which the splenic T follicular helper cells are involved as inducers of the proliferation and differentiation of autoreactive B-cells. 5 These produce antiplatelet autoantibodies, predominantly of the immunoglobulin (Ig)G isotype, which are able to react with a series of platelet receptors, mainly glycoprotein (GP) IIb/IIIa and GPIb/IX, but also GPV, GPIa/IIa, or GPIV. These autoepitopes induce cell destruction, although the course of the disease may vary in each individual case according to the specific autoantibodies, and targeted surface glycoproteins, which determine the nature of the prevailing pathogenic mechanism (i.e. accelerated clearance, inhibited megakaryopoiesis or platelet apoptosis).6–8 The covered platelets experience splenic sequestration and subsequent phagocytosis by mononuclear macrophages, which react with the cell-complexed autoantibodies via Fc gamma RIIA, and Fc gamma RIIIA receptors. 9 Macrophages still play an additional harmful role in ITP since they behave as the main antigen-presenting cell. 10 On the other hand, CD8+ T-cells also contribute to thrombocytopenia by increasing platelet apoptosis. 11 Recently, the Ashwell–Morell receptor (AMR), which is an asialoglycoprotein counter receptor predominantly expressed in hepatocytes, has also been shown to play an important role in anti-GPIbα-antibody-mediated platelet clearance. 12 As a consequence, the circulating half-life of platelets is markedly reduced. Furthermore, bone marrow megakaryocytes are unable to produce platelets normally, which exacerbates thrombocytopenia: on the one hand, there is an autoimmune response against megakaryocytes; 5 on the other hand, the circulating thrombopoietin (TPO), which is the main growth factor of megakaryocytes, does not increase to a level high enough to stimulate the production of these at the required rate. 13
Formerly, ITP used to be defined as acute, most often in children, or chronic, when the condition lasted for more than 6 months, predominantly in adults. Nevertheless, after the above-mentioned consensus conference, 1 ITP was categorized as newly diagnosed, persistent or chronic, according to a duration of <3 months, 3–12 months or >12 months, respectively.
Management of ITP
First line of treatment
The first line of treatment of ITP consists of corticosteroids. Classically, prednisone has been the drug of choice, 2 usually administered daily at 1 mg/kg for 2–4 weeks.14,15 However, recent clinical trials suggest that dexamethasone at a high dose may result in increased remission rates in the long term. Importantly, data from a recent meta-analysis that covered nine clinical trials comparing dexamethasone at a high dose (1–3 cycles of 4 days each, at 40 mg/day) versus standard prednisone (1 mg/kg/day for 2–4 weeks followed by a progressive dose lowering) demonstrated that, although there was no difference in the response rate at 6 months, patients on dexamethasone achieved a faster platelet response, and also experienced fewer hemorrhagic complications within the first 10 days of treatment as well as a lower rate of treatment-related adverse events (AEs). 16 These results have led several groups to establish dexamethasone as the first choice for ITP treatment, and a new trial aimed to compare three-cycle dexamethasone versus standard prednisone is currently ongoing. On the other hand, the use of rituximab together with dexamethasone has also been assayed in several trials. Although promising results were observed in terms of platelet count restoration, these were obtained at the expense of an unacceptable toxicity,17,18 and further studies recruiting enough patients and including a suitable follow-up period are warranted to explore the usefulness of this combination. Finally, when hemorrhage is life-threatening as well as when a particularly rapid increase in platelet counts is required, intravenous immunoglobulins, usually at 1–2 g/kg for 3 days, may be incorporated into the treatment. 19
Second line of treatment: TPO receptor agonists to replace splenectomy
Splenectomy, performed at least 6 months after ITP diagnosis, has been classically considered as the second choice when the conventional management of patients with glucocorticoids has previously failed to maintain suitable platelet counts in the long term. 19 However, in the daily medical routine, practitioners are reluctant to apply this practice due to the associated undesirable side effects (i.e. infections, thrombotic events, pulmonary hypertension and others).2,20 In fact, a considerable drop in the use of splenectomy as the second line of ITP treatment has been recently documented. 21 In parallel, an active search for new agents has been noted. Among these, it is becoming increasingly clear that agonists of the so-called TPO receptor (TPO-R) are particularly promising. TPO-R, also called c-mpl, is a member of the hematopoietic growth factor receptor superfamily which is located at the megakaryocyte surface. TPO interacts with TPO-R, thus providing a powerful stimulus for megakaryocyte proliferation and differentiation. For this reason, the use of TPO-mimetic agents was considered as promising to restore platelet counts in ITP patients. However, although recombinant TPO succeeded in increasing the number of circulating platelets,22,23 its administration was associated with the appearance of autoantibodies able to cross-react with endogenous TPO. As a consequence, TPO activity was neutralized, which subsequently led again to a thrombocytopenic condition.24,25 Ever since then, efforts have been made to generate TPO-R agonists (TPO-RAs) whose sequence is different enough from that of TPO to avoid the production of anti-TPO autoantibodies. There are two of them, namely romiplostim (AMG-531, Nplate; Amgen, Thousand Oaks, CA, USA) and eltrombopag (Revolade, Promacta; GlaxoSmithKline, Brentford, UK), that have been recently made available.26,27 In 2008, the United States Food and Drug Administration authorized their use for adult chronic ITP patients who had relapsed after splenectomy and who were refractory to other treatments (i.e. corticosteroids, immunoglobulins), as well as for adult patients in whom splenectomy was contraindicated. 28 In 2015, the use of eltrombopag was extended to any chronic ITP patient older than 1 year, as long as they did not respond to conventional medical management or splenectomy. 29 It is worth noting that, in real clinical practice, TPO-RAs seem to be replacing splenectomy in spite of the recommendations in the current published guidelines, although whether these drugs are really a better alternative still remains under discussion. 21 The present review is aimed to update the efficacy and safety of eltrombopag in ITP, and detailed information on the results concerning its use in the clinical trials reported so far, and in daily clinical practice, will be provided below. Collectively, the use of both agonists has been associated with a response rate ranging between 74% and 94%.30–32 Interestingly, when the analysis is restricted to clinical trials, more than 80% of patients exhibit at least one platelet count >50 × 103/µl, even although, among these, there are patients who had been highly refractory to other treatments. 33
Mechanism of action of eltrombopag
Eltrombopag is a synthetic biphenyl hydrazone, nonpeptide, low molecular weight TPO-RA, which is presented as eltrombopag olamine [3′ -{(2Z)-2-[1(3,4-dimethylphenyl)-3-methyl-5-oxo-1,5-dihydro-4H-pyrazol-4-ylidene]hydrazino}-2′ -hydroxy-3-biphenylcarboxylic acid-2-aminoethanol (1:2); molecular weight: 564.65]. Unlike native TPO, which binds to the extracellular domain of TPO-R, eltrombopag interacts with the transmembrane domain of the latter. As a consequence, the Janus kinase/signal transducer and activator of transcription (JAK/STAT) signaling pathway stimulates megakaryocytopoiesis, while autoantibody generation is not detected. 27 Furthermore, eltrombopag does not influence agonist-induced platelet aggregation or activation, and its oral bioavailability is excellent; circulating peaks are documented at 2–6 h after oral administration. Metabolism takes place in the liver via cytochrome P450 isoenzymes CYP1A, CYP2C8, and uridine diphosphate glucuronosyltransferase, and the half-life is in the range of 21–32 h.29,34,35
Several clinical trials have analyzed the efficacy and safety of eltrombopag in ITP. Interestingly, one of them has recently provided information regarding 5 years of follow up. These trials, as well as other clinical observations arising from daily practice, will be discussed below. The efficacy and safety of the management of ITP with eltrombopag in some particular situations will also be reviewed.
Efficacy of eltrombopag in ITP clinical trials
Several trials have studied the usefulness of eltrombopag in ITP. These are summarized below, and their main findings are outlined in Table 1.
Efficacy of eltrombopag in clinical trials with ITP patients.
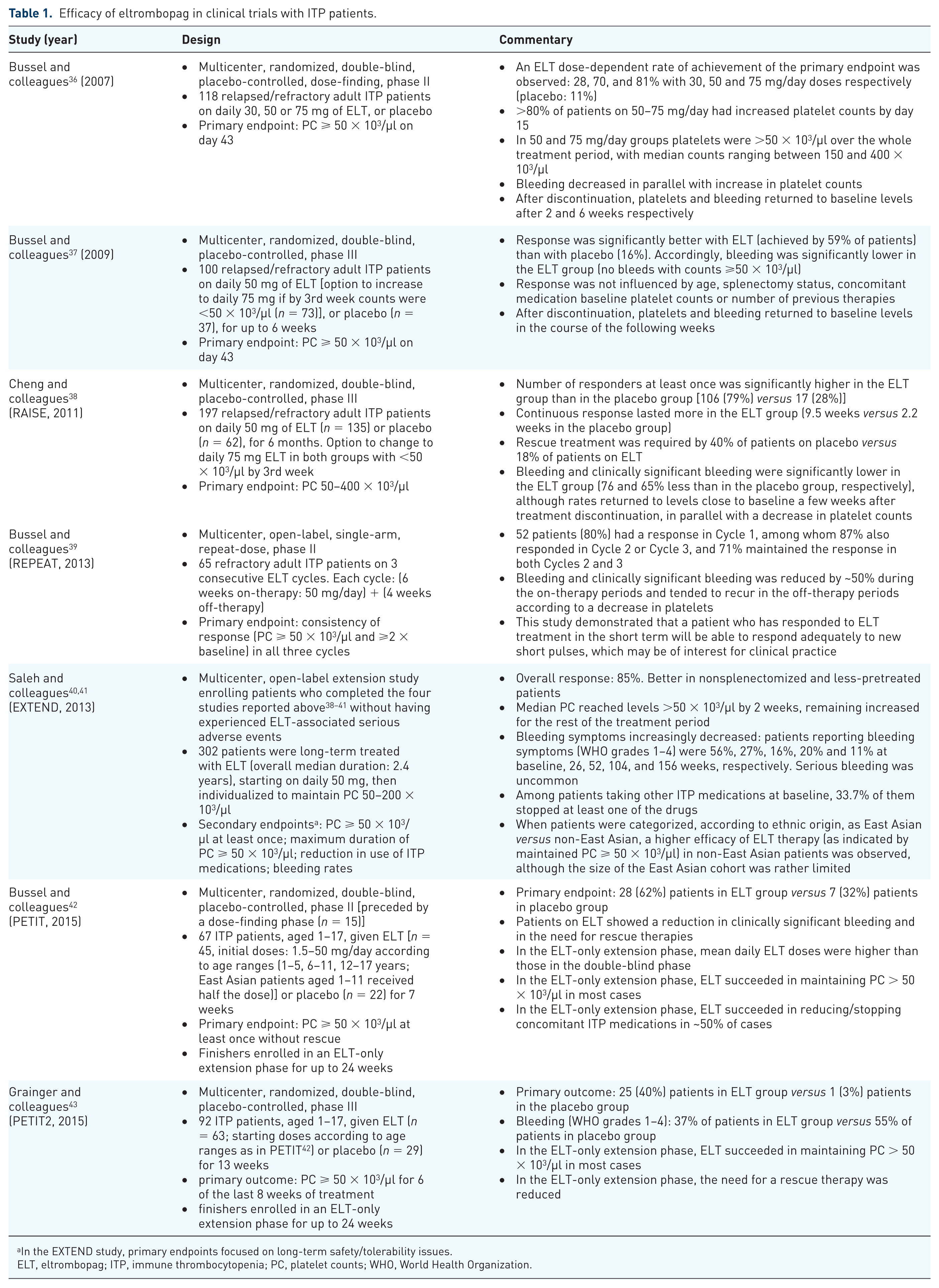
In the EXTEND study, primary endpoints focused on long-term safety/tolerability issues.
ELT, eltrombopag; ITP, immune thrombocytopenia; PC, platelet counts; WHO, World Health Organization.
The first trial was a multicenter, randomized, double-blind, placebo-controlled, dose-finding phase II study. In this, 118 patients aged ⩾18 years, who had a history of persistent (⩾6 months) or chronic ITP, exhibited platelet counts <30 × 103/µl, and who had had relapses within 3 months of previous therapy or had been refractory to at least one conventional ITP treatment, including splenectomy, were recruited. 36 Patients were 1:1:1:1 randomized to receive daily 30, 50, 75 mg of eltrombopag or placebo for 6 weeks. The primary efficacy endpoint was to reach a platelet count ⩾50 × 103/µl on day 43 after the start. Eltrombopag increased dose-dependently the rate of achievement of this goal: this was 28% (median platelet count: 26 × 103/µl), 70% (128 × 103/µl) and 81% (183 × 103/µl) in the groups of patients who had received 30, 50, and 75 mg per day, respectively, versus 11% (16 × 103/µl) among the patients in the placebo group. Among patients who were receiving the two highest doses of eltrombopag, more than 80% had increased their platelet count by day 15: this increment allowed platelets to approach their normal range, and was seen in 88% and 81% of patients receiving a daily dose of 50 or 75 mg respectively, with the median platelet counts ranging between 150 × 103/µl and 400 × 103/µl. Furthermore, in these two groups platelets remained >50 × 103/µl over the entire duration of the treatment. The incidence of bleeding symptoms varied accordingly, since it decreased in all eltrombopag groups as the platelet count increased. Nevertheless, it must be noted that the median platelet counts returned to levels near baseline in the 2 weeks following treatment discontinuation. Bleeding varied accordingly again, and it returned to the levels observed before the start of the therapy by the 6th week of post-treatment follow up. On the other hand, it must be noted that the response to eltrombopag in the cohort was not influenced by prior splenectomy. However, the use of concomitant ITP medication helped to improve response in all groups except in that comprising the patients who were receiving 75 mg of eltrombopag daily. Finally, baseline platelet counts >15 × 103/µl were associated with a higher percentage of responders to eltrombopag in all groups except in the one receiving the lowest dose.
The results of the dose-finding study encouraged the initiation of a new trial to assess the efficacy of eltrombopag in ITP using the daily dose of 50 mg. This was a phase III, randomized, double-blind, placebo-controlled study which followed similar inclusion criteria to the previous one. 37 A total of 100 patients was recruited, and 2:1 randomized to receive 50 mg/day of eltrombopag (n = 73) or placebo (n = 37) for up to 6 weeks. Nevertheless, the patients whose platelet counts were <50 × 103/µl after 3 weeks, were allowed to increase the dose of eltrombopag to 75 mg/day. The primary endpoint was similar to that used in the first study (i.e. to reach a platelet count ⩾50 × 103/µl on day 43 after the start). The response was sigificantly better in the eltrombopag group, since a response was achieved in 59% of patients versus 16% of patients in the placebo group [odds ratio (OR) 9.61, 95% confidence interval (CI) 3.31–27.86; p < 0.0001]. The response to treatment was not influenced by the splenectomy status, and seemed to be as good in elderly patients as in younger ones. Interestingly, unlike what happened in the dose-finding study, neither the use of concomitant ITP drugs nor the baseline platelet counts had a significant effect on the response to eltrombopag, and the number of previous ITP therapies did not change this either. On the other hand, a response was achieved by 10 (29%) of the 34 patients who had increased the dose to 75 mg after 3 weeks of treatment. Finally, bleeding symptoms were significantly fewer among patients in the eltrombopag group during the duration of treatment (OR 0.49, 95% CI 0.26–0.89; p = 0.021), with no significant bleedings reported when platelet counts had increased to ⩾50 × 103/µl. Once treatment was discontinued, the platelet counts returned to baseline levels in the following weeks and the percentage of patients presenting bleeding symptoms increased accordingly.
Efficacy of eltrombopag was next tested in the RAISE trial. This was another phase III, randomized, double-blind, placebo-controlled trial in patients fulfilling inclusion criteria similar to those previously described, and was performed to test the effect of daily 50 mg of eltrombopag administered for a longer period of time (i.e. 6 months). 38 A total of 135 and 62 patients were allocated to the eltrombopag and placebo groups, respectively. Dose modification from 50 to 75 mg/day in the eltrombopag group, and from placebo to 75 mg/day of eltrombopag in the placebo group, was permitted as long as platelet counts remained <50 × 103/µl after 3 weeks of treatment. A reduction to 25 mg/day was also planned for platelet counts >200 × 103/µl, and tapering or even discontinuation could be implemented when platelet counts were >100 × 103/µl on two consecutive visits after 6 weeks of therapy. The odds of response (i.e. of reaching a platelet count of 50–400 × 103/µl), was the primary endpoint, and it was significantly greater in the eltrombopag group as compared with the placebo group throughout the 6-month treatment period (OR 8.2, 99% CI 3.59–18.73; p < 0.0001). Accordingly, the duration of continuous response was longer among eltrombopag-treated patients, with a mean of 9.5 weeks versus 2.2 weeks in the placebo group. Furthermore, 37 (59%) patients receiving eltrombopag reduced concomitant therapy compared with 10 (32%) receiving placebo (p = 0.016), and 24 (18%) eltrombopag-treated patients required rescue treatment versus 25 (40%) placebo-treated patients (p = 0.001). The odds of bleeding and clinically significant bleeding were significantly lower in patients treated with eltrombopag compared with placebo (OR 0.24, 95% CI 0.16–0.38; p < 0.0001, and OR 0.35, 95% CI 0.19–0.64; p = 0.0008, respectively). Nevertheless, the rates of bleeding returned near to baseline after eltrombopag discontinuation, paralleling the decrease in platelet counts.
As the potential of eltrombopag as an alternative to splenectomy or other medications for a second line therapy in ITP was increasingly confirmed, a new trial tested its usefulness when used over repeated short-term cycles. The aim was to find out if a chronic ITP patient who had responded to short-term eltrombopag, but did not require continuous therapy, would respond efficiently to subsequent eltrombopag courses. To accomplish this goal, the REPEAT trial, an open-label, single-arm, repeat-dose phase II study, recruited 65 patients aged >18 years with an ITP of >6 months duration, platelet counts between 20 and 50 × 103/µl, and having received at least one previous therapy, including splenectomy. 39 Patients were administered 50 mg of eltrombopag daily over three cycles, each cycle consisting of up to 6 weeks on-therapy followed by up to 4 weeks off-therapy. A response was considered to be positive when the patient achieved a platelet count ⩾50 × 103/µl and ⩾2 × baseline, and this was evaluated in each cycle. The primary endpoint was the proportion of patients with a response in Cycle 1 who subsequently responded in Cycles 2 or 3. Firstly, 52 of 65 patients (80%) responded in Cycle 1. Remarkably, among these, 87% responded in Cycle 2 or 3 and 71% responded in both Cycles 2 and 3. During the on-therapy periods, the incidence of any bleeding and clinically significant bleeding decreased by approximately 50%, and tended to recur in the off-therapy periods, paralleling the recurrence of thrombocytopenia. Globally, this study contributes to the notion that, once a patient has responded to short-term therapy with eltrombopag, he or she will respond adequately to subsequent short-term cycles when these are given according to their requirements.
Finally, an extension trial explored the efficiency of prolonged treatment of ITP with eltrombopag, and, furthermore, made it possible to control patients for a follow-up period of up to 5 years. The EXTEND trial recruited patients who had completed the four studies described above, irrespective of their platelet counts at entry, and provided that they had not previously experienced any eltrombopag-related serious AEs (SAEs). 40 A total of 302 patients were involved. Treatment was initiated at 50 mg once daily in all patients, but this could be subsequently individualized to accomplish the goal of maintaining platelets in the range between ⩾50 × 103/µl and <200 × 103/µl. The mean average daily dose was 50.2 mg, and the overall median duration of exposure was 2.4 years. The overall response was 85%. The median platelet counts had increased to >50 × 103/µl by 2 weeks, and remained increased throughout the study. The response was better in nonsplenectomized and less-pretreated patients, as compared with splenectomized and heavily pretreated ones. At 1 year after the start, bleeding symptoms decreased from 57% to 16%. Serious bleeding was uncommon. Furthermore, 33.7% of patients who were taking some other form of ITP medication at baseline stopped at least one of these medications. Finally, a subanalysis to compare efficacy between East Asian and non-East Asian patients indicated that the latter achieved continuous platelet counts ⩾50 × 103/µl in a higher proportion than the former, although the limited patient numbers in the East Asian group (n = 41) suggests that we should take this observation cautiously, and wait for the results of the investigations that are currently ongoing. 41
The efficacy of eltrombopag has also been tested in children aged 1–17 years with ITP lasting for 6 months or longer, platelet counts <30 × 103/µl, and who had received at least one previous treatment. For this purpose, two randomized, double-blind, phase II and phase III studies, respectively, have recently been reported. The first one, so-called PETIT, firstly consisted of a dose-finding phase that established the following initial doses: 1.5 mg/day (0.8 mg/day for East Asian patients) for patients aged 1–5 years; 50 mg/day (25 mg/day for East Asian patients) if weight ⩾27 kg or 25 mg/day (12.5 mg/day for East Asian patients) if weight <27 kg for patients aged 6–11 years; 37.5 mg/day for patients aged 12–17 years. A total of 67 additional patients were subsequently recruited to be administered eltrombopag (n = 45) or placebo (n = 22) once a day for 7 weeks. 42 Notably, the primary endpoint (i.e. to reach a platelet count ⩾50 × 103/µl at least once without rescue), was achieved by 28 (62%) eltrombopag-treated patients compared versus 7 (32%) who received placebo (OR 4.31, 95% CI 1.39–13.34, p = 0.011). A reduction in clinically significant bleeding as well as in the need for rescue therapy was also observed in the eltrombopag group. On the other hand, patients who had completed the randomized phase were allowed to enter an extension phase to continue treatment for up to 24 weeks, during which platelet counts were kept >50 × 103/µl in the majority of cases. Furthermore, in this period concomitant medication was discontinued or reduced in roughly half the patients.
PETIT-2 confirmed the findings obtained in PETIT. This was a randomized, double-blind, phase III study which recruited 92 patients according to inclusion criteria similar to those used in PETIT, to be treated with eltrombopag (n = 63) or placebo (n = 29) for 13 weeks. 43 Starting doses were roughly similar to the ones used in PETIT. The primary outcome was to exhibit platelet counts ⩾50 × 103/µl for 6 of the last 8 weeks of treatment, and was achieved by 25 (40%) patients who received eltrombopag versus only 1 (3%) who was administered placebo (OR 18.0, 95% CI 2.3–140.9, p = 0.0004). The proportion of patients who suffered bleeding events graded 1–4 according to the World Health Organization (WHO) bleeding scale was lower on eltrombopag (37%) than on placebo (55%). Similar to what happened in PETIT, the need for a rescue therapy was reduced, and platelet counts were mostly maintained >50 × 103/µl during the subsequent extension phase which was prolonged for up to 24 weeks.
The results of a recently published meta-analysis covering the trials aimed to assess the efficacy of eltrombopag in adults and children are suitable to summarize this section, since it was concluded that eltrombopag efficiently increases platelet counts and reduces clinically significant bleeding in adults and children with persistent or chronic ITP. 44
Safety of eltrombopag in ITP clinical trials
The same trials that studied the efficacy of eltrombopag in ITP addressed the question whether the treatment could be associated with significant safety concerns. The most relevant information is presented below and is outlined in Table 2, except the bleeding-related AEs, which were documented in the previous section, since these are incidences rather related to the efficacy of the therapy.
Safety profile of eltrombopag in clinical trials with ITP patients.
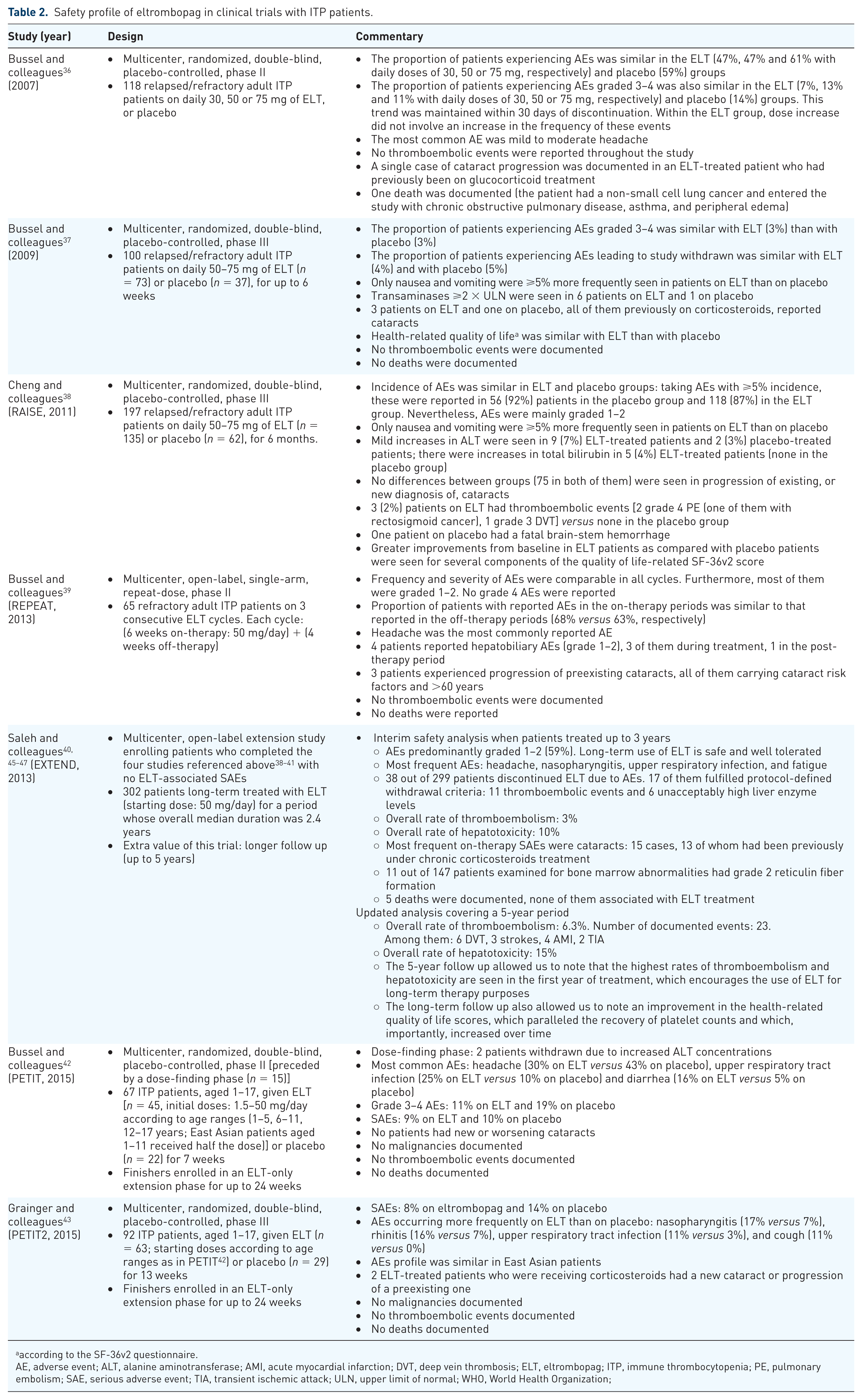
according to the SF-36v2 questionnaire.
AE, adverse event; ALT, alanine aminotransferase; AMI, acute myocardial infarction; DVT, deep vein thrombosis; ELT, eltrombopag; ITP, immune thrombocytopenia; PE, pulmonary embolism; SAE, serious adverse event; TIA, transient ischemic attack; ULN, upper limit of normal; WHO, World Health Organization;
In the first trial, with 118 adult patients randomized to receive for 6 weeks daily 30, 50, 75 mg of eltrombopag or placebo, 36 the incidence and severity of AEs were similar in the placebo and eltrombopag groups, with the most common AE being mild to moderate headache. Remarkably, the number of patients experiencing grade 3 or 4 AEs, during the study or within 30 days after discontinuation, was not higher with eltrombopag as compared with placebo. No thrombotic events were documented. The only case of cataract progression was reported in a patient who had previously been treated with glucocorticoids. Mean scores for health-related quality of life according to the SF-36v2 questionnaire were similar at baseline and at the end of the study. The only death occurred in a 50 mg/day eltrombopag-treated man aged 66 years, who suffered a pneumonectomy for non-small cell lung cancer and had entered the study with chronic obstructive pulmonary disease, asthma, and peripheral edema.
In the second trial, with 73 and 37 adult patients receiving 50 mg/day of eltrombopag or placebo, respectively, for up to 6 weeks, 37 the frequency of grade 3–4 AEs during treatment was also irrespective of treatment (3% in both groups). Furthermore, the number of AEs leading to study discontinuation was also similar (4% and 5% for eltrombopag and placebo groups, respectively). Nausea and vomiting were the only AEs reported by ⩾5% more patients receiving eltrombopag than placebo. Overall, six patients treated with eltrombopag and one treated with placebo exhibited transaminase concentrations twice the upper limit of normal (ULN). As above, reporting of cataracts involved patients who had been previously treated with corticosteroids. Health-related quality of life according to SF-36v2 was similar in both groups. Thromboembolic events were not reported. No deaths occurred during the study.
AEs in the RAISE trial, which involved 135 and 62 adult patients treated for 6 months with daily 50 mg of eltrombopag or placebo, respectively (with the option of increasing the dose up to 75 mg in both groups from the 3rd week on), 38 were mainly graded 1–2 in severity. Incidences of on-treatment AEs reported for the eltrombopag or placebo-treated groups were comparable. As previously seen, nausea and vomiting were the only AEs to be reported by ⩾5% more patients receiving eltrombopag than placebo. Nevertheless, three (2%) patients receiving eltrombopag had thromboembolic events compared with none in patients on placebo. A total of nine (7%) eltrombopag-treated patients versus two (3%) in the placebo group had mild increases in alanine aminotransferase (ALT) concentration, and five (4%) eltrombopag-treated patients versus none in the placebo group had increases in total bilirubin. Finally, significantly greater improvements from baseline were shown for patients receiving eltrombopag than for those receiving placebo for several of the components of the SF-36v2 score (among them, physical and emotional roles) and the FACT-Th6 score.
The analysis of AEs in the REPEAT trial, which tested the efficacy of eltrombopag administered in the short term in 65 adult patients in three consecutive cycles each consisting of up to 6 weeks on-therapy (50 mg/day) followed by up to 4 weeks off-therapy, 39 revealed that neither the frequency nor the severity of AEs increased over successive cycles. Furthermore, the proportion of patients who experienced AEs was similar in the on-therapy and in the off-therapy periods of the cycles (68% and 63% respectively). No thrombotic events were reported. The majority of AEs were graded 1–2 (i.e. mild to moderate). The most common AE reported was headache. A total of four patients reported hepatobiliary AEs, three of them during treatment and the other one in the post-therapy period. All of them were graded 1–2 in severity, and resolved. Progression of preexisting cataracts occurred in three patients who presented with cataract risk factors and were older than 60 years. No grade 4 AEs or deaths were documented.
The evidence presented so far seem to support the notion that eltrombopag is a safe and well tolerated drug and, therefore, suitable for ITP patients. However, they were obtained in trials lacking follow-up periods large enough to explore safety in the long term. In this sense, the EXTEND trial represents an important step to assess eltrombopag safety, not only because of the number of participants (i.e. patients who completed the four trials previously described), but, particularly, because of the duration of the follow-up period, up to 5 years. The first safety evaluation comprised 299 patients treated for up to 3 years, initially with a daily dose of 50 mg, which could be subsequently adjustable according to the platelet counts achieved. 40 Long-term treatment with eltrombopag was generally safe and well tolerated, and no new or increased incidence of safety issues was identified. AEs were graded 1–2 in 59% of patients. The most frequent ones were headache, nasopharyngitis, upper respiratory infection, and fatigue. Nevertheless, 38 patients (13%) experienced AEs leading to trial withdrawal. Protocol-defined withdrawal criteria were met in 17 cases, 11 of whom reported thromboembolic events, while the other 6 exceeded liver enzyme thresholds. Overall cohort rates of venous thromboembolism and hepatotoxicity were 3% and 10%, respectively. Cataracts were the most frequently reported on-therapy SAE, and were documented in 15 cases, 13 of whom had been under chronic treatment with corticosteroids previously. Among the 147 patients examined for bone marrow abnormalities, 11 of them had grade 2 reticulin fiber formation, but only one showed an increase in grade at ⩾2 years of follow up. Overall, two patients were diagnosed with lymphoma. A total of five deaths occurred, although none of them were related to the use of eltrombopag. An update of these observations, covering a follow-up period of up to 5 years, has recently been made available: 45 hepatic enzyme elevation and thromboembolic events have been documented in 15% and 6.3% of patients, respectively. Interestingly, the data indicate that the highest incidences of these two AEs occurred during the first year of treatment, which substantiates the notion that long-term eltrombopag therapy exhibits a positive benefit–risk relationship for treatment of ITP in adults. Furthermore, long-term follow up not only confirmed the improvement in the health-related quality of life scores associated with the recovery of platelet counts upon eltrombopag therapy, 46 but showed that such improvement increased over time. 47
The safety of eltrombopag was also assessed in the trials recruiting children. In the first one, PETIT, which enrolled 67 ITP patients aged <18 years who received eltrombopag at doses according to age ranges once a day for 7 weeks (and for up to 24 additional weeks in an extension phase), 42 two patients discontinued eltrombopag due to increased ALT concentrations during the dose-finding phase. Neither grade 3–4 AEs nor SAEs were more frequent among patients on eltrombopag than on placebo [grade 3–4 AEs: 5 (11%) on eltrombopag versus 4 (19%) on placebo; SAEs: 4 (9%) versus 2 (10%)]. The most common AEs were headache [13 (30%) on eltrombopag versus 9 (43%) on placebo], upper respiratory tract infection [11 (25%) versus 2 (10%)], and diarrhea [7 (16%) versus 1 (5%)]. No thrombotic events or malignancies were documented.
PETIT’s safety observations were roughly confirmed by PETIT-2, in which 92 ITP patients aged <18 years were treated with eltrombopag or placebo during, first, a 13-week period and, second, an extension phase of up to 24 weeks. 43 AEs that occurred more frequently on eltrombopag than on placebo were nasopharyngitis, rhinitis, upper respiratory tract infection, and cough. However, SAEs were not more frequent on eltrombopag (8%) than on placebo (14%), and no deaths, malignancies, or thromboses were documented. In sum, the experience with eltrombopag in children with ITP allows us to claim that this drug is also suitable to treat them. Few patients discontinue treatment because of AEs, and no new safety concerns have been identified.
Frequency and management of AEs occurring during treatment with eltrombopag
The information obtained in the studies addressed above, together with the ample post-marketing experience, enables us to assess the frequency of the AEs associated with the use of eltrombopag. Data allow us to be optimistic about the safety of eltrombopag when used in the long term; as stated above, hepatic alterations and thrombosis usually occur during the first year of treatment, and long-term follow up has allowed us to observe the improvement in health-related quality of life scores associated with the recovery of platelet counts increases over time.45–47 Table 3 lists AEs according to the MedDRA system organ class and frequency associated with the use of eltrombopag in ITP. It must be said that a nonnegligible number of events described as ‘uncommon’, are almost certainly unrelated to the study drug, as is often the case in this kind of study. This section provides information on the management of potentially serious AEs that may be related to eltrombopag in ITP patients, as well as on use of eltrombopag in particular ITP populations.
Frequency of adverse events observed in patients on treatment with eltrombopag.
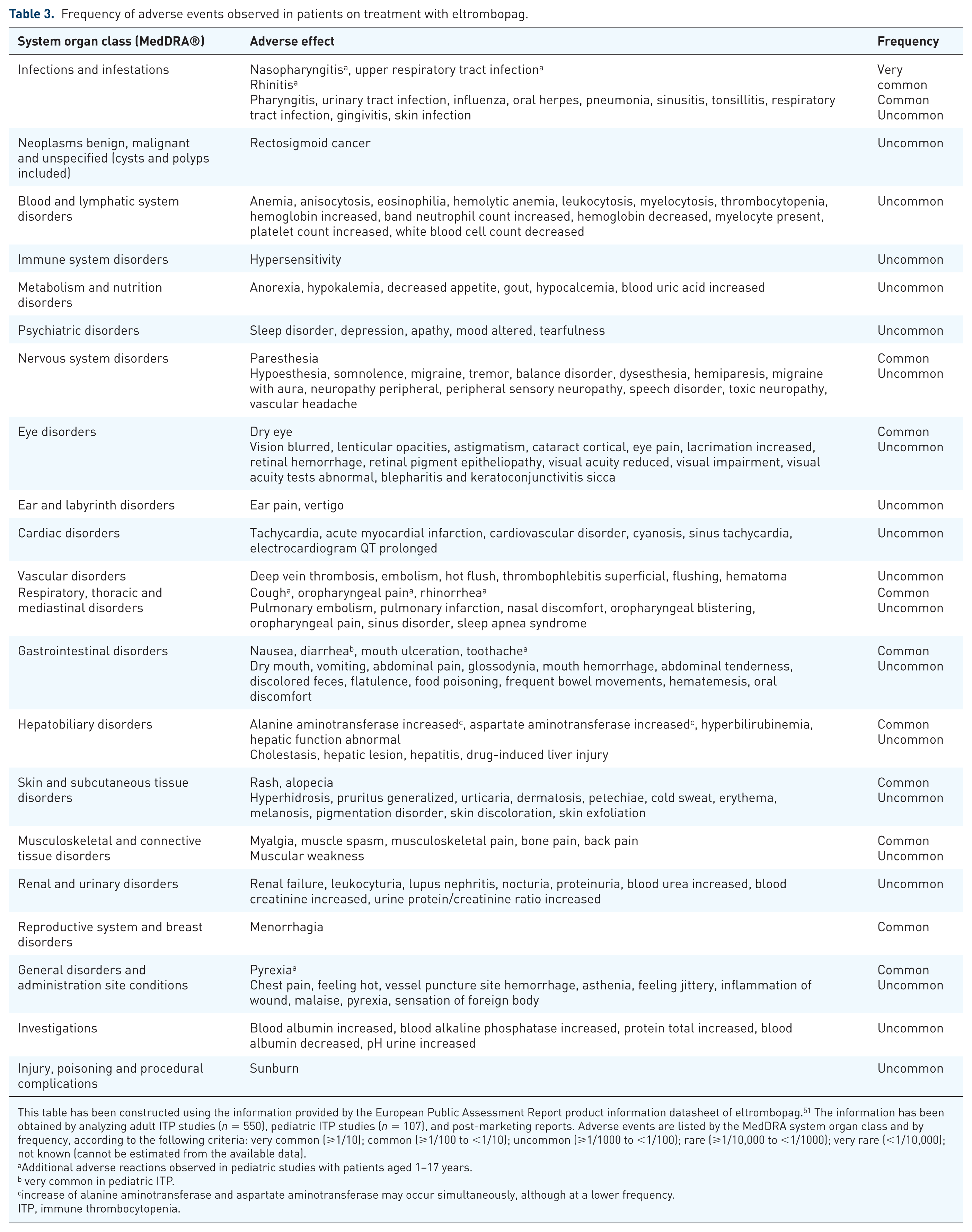
This table has been constructed using the information provided by the European Public Assessment Report product information datasheet of eltrombopag. 51 The information has been obtained by analyzing adult ITP studies (n = 550), pediatric ITP studies (n = 107), and post-marketing reports. Adverse events are listed by the MedDRA system organ class and by frequency, according to the following criteria: very common (⩾1/10); common (⩾1/100 to <1/10); uncommon (⩾1/1000 to <1/100); rare (⩾1/10,000 to <1/1000); very rare (<1/10,000); not known (cannot be estimated from the available data).
Additional adverse reactions observed in pediatric studies with patients aged 1–17 years.
very common in pediatric ITP.
increase of alanine aminotransferase and aspartate aminotransferase may occur simultaneously, although at a lower frequency.
ITP, immune thrombocytopenia.
Prevention/management of particular situations
Thromboembolic events
Thrombotic risk in ITP patients merits discussion. Although, in theory, venous thrombotic risk is only slightly higher and arterial risk is negligible, there may be a number of circumstances (i.e. age, splenectomy, risk factors), which could increase the odds of suffering a thrombotic event. Importantly, these personal hallmarks may be of particular importance when on treatment with TPO-R, since some authors claim that there is indirect evidence of a risk of both arterial and venous thromboembolism associated with this therapy. 48 Nevertheless, this topic is a matter of controversy, since other authors have not found such a relationship, and have even reported resolution of thrombotic episodes in spite of nondiscontinuation of TPO-R therapy.49,50 Nevertheless, thromboembolic events have been observed in eltrombopag-treated ITP patients with normal and even low platelet counts.38,40,45 Thus, caution is recommended if eltrombopag has to be administered to ITP patients with classical congenital (factor V Leiden, deficiency of protein C, protein S or antithrombin) or acquired (antiphospholipid syndrome, advanced age, prolonged immobilization, malignancies, contraceptives and hormone replacement therapy, surgery/trauma, obesity or smoking) thromboembolism risk factors. Indeed, the risk–benefit balance should be considered before starting eltrombopag therapy in a patient at thromboembolic risk. In this sense, platelet counts must be closely monitored, and if these exceed the target level, dose reduction or discontinuation should, at least, be considered. Accordingly, eltrombopag should be used in ITP patients with hepatic impairment (Child–Pugh score ⩾5) only when the expected benefit clearly outweighs the risk of portal venous thrombosis. 51 Finally, it is worth mentioning that avatrombopag is another TPO-RA, which has been licensed for use in thrombocytopenia associated with liver disease. Although further studies are needed, preliminary observations suggest that avatrombopag may confer a particularly low thrombotic risk due to the nature of its metabolites, which would induce portal vein clotting to a lesser extent than eltrombopag or romiplostim. 52
Risk of hepatotoxicity
Eltrombopag inhibits an organic anion transporter, so-called OATP1B1, and a glucuronosyltransferase, UGT1A1, and thus may alter the catabolism of bilirubin. For this reason, eltrombopag could cause abnormal liver function and hepatotoxicity, which might be potentially life-threatening. Although mostly mild, serum ALT, aspartate aminotransferase (AST) and bilirubin increases have been repeatedly observed with eltrombopag use in adults and children.36–40,42,43,45 It is recommended that circulating ALT, AST and bilirubin levels be measured prior to initiation of eltrombopag, and, during therapy, every 2 weeks during the dose-adjustment phase, and monthly once a dose has been established. If bilirubin is elevated, fractionation should be performed. When serum liver tests are abnormal, testing should be repeated within 3–5 days. Monitoring should continue until resolution, and treatment discontinuation should be decided upon increase of ALT levels (⩾3 × ULN when liver function is normal, or ⩾3 × baseline or >5 × ULN, whichever is the lower, when transaminases are elevated at pretreatment), provided that this increase is progressive, or persistent for ⩾4 weeks, or accompanied by increased direct bilirubin, or by clinical symptoms of liver injury or evidence for hepatic decompensation. Indeed, therapy must be cautiously administered in patients with hepatic disease, and the starting dose has to be lower than the normal one. 51
Bone marrow fibrosis
Development or progression of reticulin fibers within the bone marrow has been observed upon eltrombopag treatment, which may be the result of the activity of cytokines (e.g. transforming growth factor-β). 40 Initially, a study showed low-grade bone marrow reticulin fibrosis in most ITP patients treated with TPO-RAs (eltrombopag among them), although the number of patients evaluated was rather low. 53 Later on, biopsy specimens from 117 participants of the EXTEND study revealed a moderate to marked reticulin fibrosis in the bone marrow of two patients, one of which reverted to normal after withdrawal from the study. 54 Finally, a prospective study assessed the effects of eltrombopag in the long term (i.e. 2 years), on bone marrow in 93 chronic ITP patients, and found that in 89% of these, eltrombopag was not associated with clinically relevant increases in bone marrow reticulin or collagen formation. 55 However, these studies are not conclusive enough to establish the relevance, if any, of bone marrow fibrosis in patients on eltrombopag. Nevertheless, it is recommended that, prior to initiation of therapy, an examination of the peripheral blood smear should be performed to establish the baseline level of cellular morphologic abnormalities. Once a dose of eltrombopag has been fixed, a full blood count and, specifically, white blood cell count, should be performed monthly. If one of these periodic examinations reveals immature or dysplastic cells, an examination of the peripheral blood smear should be considered in order to identify new, or worsening, morphological abnormalities or cytopenias. If such alterations are confirmed, eltrombopag should be discontinued, and a bone marrow biopsy, including staining for fibrosis, would be advisable. In conclusion, a loss of response to eltrombopag (i.e. the inability to recover platelet counts, at least partially), should suggest a test of bone marrow reticulin, since its progression may hamper platelet expansion. 51 Nevertheless, the fact that nonadherence to dietary restrictions is a more common cause of loss of response should also be considered.
Ocular changes
Studies in young rodents revealed that eltrombopag might lead to cataract development, at doses ⩾4 times the usual human clinical exposure. 56 Development of new cataracts or progression of preexisting ones have been observed in several of the trials aimed to test eltrombopag in adult and pediatric ITP. However, these cases were always associated with classical risk factors, mostly prior chronic treatment with corticosteroids.36,37,39,40,43 Nevertheless, routine ophthalmologic monitoring of patients on eltrombopag is recommended. 51
Management of particular populations
Patients with renal impairment
Although they have to be closely monitored (serum creatinine and/or urine analysis), no dose adjustment is required. 51
Patients with hepatic impairment
As anticipated above, ITP patients with hepatic impairment (Child–Pugh score ⩾ 5) should be treated with eltrombopag only when the expected benefit outweighs the risk of portal venous thrombosis. In such cases, the starting dose should be 25 mg, administered once daily. Only after 3 weeks may the dose be increased. 51
Eltrombopag in the elderly
No relevant differences in terms of safety have been observed between patients aged ⩾65 years and younger ones. Nevertheless, since the information available on the use of eltrombopag in ITP patients aged 65–85 years is limited, and there is no information regarding patients aged >85 years, greater sensitivity of some individuals, especially among the oldest ones, cannot be ruled out. 51
Pediatric population
Eltrombopag should not be used in children aged <1 year since there are not enough data available on safety and efficacy. 51
Patients of East Asian ancestry
Patients of Chinese, Japanese, Taiwanese, Korean or Thai origin, including those with hepatic impairment, should initiate treatment at a dose of 25 mg once daily. Subsequently, platelet count monitoring should permit dose adjustment following standard criteria. 51
Efficacy and safety of eltrombopag in daily clinical practice
With no exception, the trials that have been presented above have offered an encouraging panorama on the usefulness of eltrombopag to treat ITP, since this has behaved as an efficient, and reasonably safe, agent to restore platelet counts to suitable levels. However, it is accepted that trials do not necessarily reflect accurately what happens in clinical practice. For this reason, there are several groups that have recently assessed the efficacy and safety of eltrombopag in ‘real-world’ settings, and whose results contribute to build a more reliable picture on the validity of this therapy.
First, a multicenter, retrospective study performed in Spain involved 164 unselected chronic ITP patients with a median age of 63 years, who had been heavily pretreated with no success. 31 Overall, 30% of them presented bleeding symptoms the month before the start of eltrombopag therapy, after which they were followed up for 15 months. Eltrombopag was highly effective and well tolerated: 88.8% of patients achieved a platelet response (platelet count ⩾30 × 103/µl and at least a twofold increase of the baseline count, with concurrent resolution of bleeding symptoms and absence of any rescue intervention during the preceding 8 weeks), with a median time to platelet response of 12 days. Furthermore, during the entire period under examination, a maintained platelet response rate was achieved by 75.2% of patients, while AEs, mainly graded 1–2, were observed in less than 20% of them.
Second, another multicenter study was performed in Italy, in which 124 patients with chronic ITP who had failed several lines of therapy were treated with TPO-RAs, 69 of them with eltrombopag, and were retrospectively analyzed. 30 Eltrombopag was effective in the majority of patients, since the overall response rate was 94.2 %. Response in nonsplenectomized patients was higher than in splenectomized ones. Thrombotic events were documented in 3% of patients and constituted the most consistent AEs.
Lastly, a Turkish group reported their experience with 31 chronic ITP patients who had been refractory to, at least, two previous treatments, in a retrospective study on their response to eltrombopag. 57 The median duration of treatment was 29 weeks. The response (i.e. a platelet count ⩾50 × 103/µl at any time point during the study), was achieved by 83.9% of the cohort, mostly by the second week of treatment. Furthermore, concomitant ITP medications were withdrawn in 9 out of the 11 patients who were taking them. Overall, four patients were forced to discontinue treatment due to thrombotic events. Other AEs were mild and easily managed.
In summary, three experiences with eltrombopag in daily clinical practice in the context of chronic ITP in refractory patients support the notion that this treatment may be effective and well tolerated in the long term. Although not frequent, thrombotic events are AEs whose consequences might be potentially serious. This means that the decision about treatment in patients with thrombosis risk factors should include careful consideration of whether or not the expected benefits outweigh the odds of thromboembolism.
Use of eltrombopag in ITP in special situations
Eltrombopag in newly diagnosed ITP
The studies reported so far have approached the use of eltrombopag mostly in chronic ITP patients. Although the evidence is more limited and involves rather smaller cohorts, the experience with eltrombopag in daily clinical practice with newly diagnosed patients (i.e. patients who were diagnosed with ITP less than 3 months before they started eltrombopag therapy), 1 deserves attention. The Spanish experience has been recently reported. The efficacy and safety of eltrombopag was retrospectively compared between chronic (n = 160), persistent (n = 30) and newly diagnosed (n = 30) ITP patients. 58 The fact that there were no baseline differences among groups regarding most relevant parameters allows us to perform reliable comparisons. There were no statistically significant differences among groups either in terms of platelet response (platelet count ⩾30 × 103/µl and at least a twofold increase of the baseline count, with concurrent resolution of bleeding symptoms and absence of rescue interventions in the preceding 8 weeks) or in terms of complete response (as response, but with platelet count ⩾100 × 103/µl). Interestingly, a trend towards greater efficacy in newly diagnosed ITP could be observed (93.3% of response versus 83.3% and 79.4% in persistent and chronic ITP patients, respectively, and 86.7% of complete responses versus 80.0% and 73.1% in persistent and chronic ITP patients, respectively). On the other hand, there were no noticeable differences regarding AEs among groups.
The experience of two other groups from Mexico and India had previously been documented. In the first one, 12 adult patients with newly diagnosed ITP were administered a single 4-day course of dexamethasone followed by daily eltrombopag during the following 28 days. 59 At 6 months, complete response (platelets ⩾100 × 103/µl) and response (platelets ⩾30 × 103/µl <100 × 103/µl) were achieved by 50% and 25% of patients respectively. Relapse-free survival at 12 months was observed in eight patients. Lastly, a single center study involved 25 newly diagnosed ITP patients who had been refractory to steroid medication and were subsequently treated with eltrombopag. 60 A total of 80% of them showed a response by the end of the first month, the time at which the median platelet counts had shown a net increase of more than ⩾100 × 103/µl. Furthermore, the response was sustained in 76 % of patients at the end of the third month.
Therefore, although larger studies with a longer follow up are undoubtedly needed to assess the efficacy and safety of eltrombopag in newly diagnosed patients, these studies highlight the potential value of this therapy in this particular situation.
Eltrombopag discontinuation
Discontinuation of eltrombopag is thought to lead to a decrease in platelet counts to baseline levels within 2 weeks (i.e. thrombocytopenia might reoccur), which would prompt bleeding events, especially in the presence of anticoagulant or anti-aggregant agents. 51 For this reason, it is recommended that platelet counts be monitored on a weekly basis for 4 weeks after discontinuation, and it is advisable to restart ITP treatment according to the current treatment guidelines. 19 Furthermore, cessation of anticoagulant or antiplatelet therapy, reversal of anticoagulation, or platelet support, should at least be considered. 51 Nevertheless, in recent years there has been increasing evidence that a sustained platelet response, once eltrombopag has been discontinued, may be achieved. There are three studies that have reported data that support such notion. On the one hand, a recent study of 39 patients with ITP treated with TPO-RAs (eltrombopag was used in 11 of them), demonstrated that, after treatment discontinuation, 7 of them (18%) reached a sustained response, defined as the first assessed platelet count ⩾30 × 103/µl available at more than 4 weeks after discontinuation. 61 Notably, this response was achieved in the absence of concomitant or rescue therapies. Among these patients, 71% of them had previously reached a durable response, which was defined as a response (platelet count ⩾30 × 103/µl and at least a twofold increase as compared with the baseline count) or complete response (platelet count ⩾100 × 103/µl with no bleeding) persisting for at least 4 weeks during the treatment period. On the other hand, another study found that, among 49 adult ITP patients who had achieved complete remission (platelet count >100 × 103/µl) with eltrombopag and subsequently discontinued therapy, 26 showed a sustained response without additional medication during a follow-up period ranging between 6 and 25 months (median time: 9 months). 62 Overall, 15% of them had been diagnosed with ITP less than 1 year previously. Unfortunately, no predictive factors of sustained response other than complete remission could be identified. Finally, a French study showed that, among 14 adult ITP patients who discontinued treatment with a TPO-RAs after having achieved a complete response, eight had a sustained response during a follow-up period ranging between 5 and 27 months (median time: 13.5 months). 63 Eltrombopag was used in six of these patients (in three of them there was a switch with another TPO-RA in the course of the treatment period). In addition, no predictive factors for sustained response were identified.
These encouraging results prompted the design of larger studies aimed to ascertain if patients who have been on eltrombopag treatment, especially those who have achieved a complete response, are able to maintain platelet counts high enough to prevent spontaneous bleedings. Duration of sustained response, as well as markers to predict the type of patients who will reach this goal, are important gaps that should also be filled. A clinical trial (STOP-AGO, ClinicalTrials.gov identifier: NCT03119974) is currently ongoing to assess the rate of sustained response after discontinuation of TPO-RA (eltrombopag or romiplostim) therapy in ITP patients.
In conclusion, it must be said that partial eltrombopag discontinuation is strongly recommended when the platelet count increases to ⩾400 × 109/l. In such cases, eltrombopag should be withheld until the platelet count falls to below 150 × 109/l. Then, therapy can be restarted at a lower dose.62,64
Switching from one TPO-RA to another
As anticipated, there is also another TPO-RA which is being widely used, namely romiplostim. Both TPO-RAs are thought to induce signaling that leads to platelet production (i.e. their clinical effect is essentially similar). Indeed, a sustained platelet response has also been observed upon treatment with romiplostim, in studies covering longer periods of time than those used in eltrombopag trials. 65 However, while eltrombopag is a small molecular weight compound for daily oral administration, romiplostim is a recombinant polypeptide which is administered subcutaneously, preferentially on a weekly basis. 66 A matter of controversy in the use of TPO-RAs in ITP is the utility of their sequential use (i.e. switching from one agonist to another due to AEs or after non-achievement of a response with the first one). A large number of case reports broaching this topic have been published. However, few papers cover a series of patients. On the one hand, there is a study presenting a cohort of 51 adult ITP patients who were retrospectively evaluated after switching from romiplostim to eltrombopag. 67 The first agonist had been used during a period whose median duration was 12 months. The reason for switching was mainly lack of efficacy (49% of patients), although other cases were due to side effects, patient preference or platelet count fluctuation. The response rate to eltrombopag was 80%. Furthermore, a complete response could be seen in 67% of cases. Efficacy with eltrombopag was maintained after switching in all patients in the patient preference, platelet count fluctuation and side-effect groups, which means that failures were seen among the patients who had not previously responded to romiplostim. No major safety concerns were detected. A second study identified the fact that the desired platelet count had not been achieved or the lack of response to prior therapy as the main causes of switching from romiplostim to eltrombopag or vice versa, and roughly confirmed that switching from one TPO-RA to another may be beneficial when the response to the agonist used first has failed. 68 Both studies demonstrated that switching due to an AE can solve the AE while maintaining efficacy and also that switching due to undesirable platelet count fluctuations can resolve the problem in a substantial proportion of cases. There is also a retrospective evaluation of switching from eltrombopag to romiplostim or vice versa that further substantiates the usefulness of such practice. In this case, the authors found a tendency towards a better response after switching from eltrombopag to romiplostim. 69
Therefore, although confirmatory studies are still needed, switching from one TPO-RA to another may be beneficial when nonresponse, or AEs, have prevented success with the former.
Conclusion
In summary, eltrombopag is being increasingly used as second line of therapy for ITP patients, instead of other treatments or more aggressive procedures like splenectomy. Results from clinical trials and, importantly, day-to-day clinical practice, suggest that this drug is effective, well tolerated and safe to restore platelet counts at levels high enough to prevent bleeding events. Nevertheless, there are still some aspects of this therapy that deserve particular attention (i.e. relevance of the associated thrombotic risk), and further investigation as well as achievement and duration of sustained response after discontinuation. Therefore, patients treated with this therapy should be carefully selected and caution must be taken until we have better knowledge of the behavior of this drug.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The authors declare that there is no conflict of interest.