
Abstract
Background:
Hyperkalemia is an electrolyte abnormality that may cause ventricular dysrhythmias and cardiac arrest. The presence of hyperkalemia may necessitate prompt treatment via intravenous insulin and dextrose. One notable complication of this therapy is the development of hypoglycemia. Previous trials have examined the impact of altering the insulin dose administered on hypoglycemia development; no trials to date however, have examined the impact of altering the dextrose dose.
Methods:
This was a multicenter, retrospective, matched cohort study of patients who received intravenous insulin and dextrose for reversal of hyperkalemia. Patients received either 25 g or 50 g of dextrose in addition to 10 units of insulin. Study populations were matched based on preexisting rates of acute kidney injury, end-stage renal disease, and diabetes mellitus. Blood glucose levels were measured at 60 and 240 min following treatment.
Results:
A total of 240 patients were included in the analysis. At 60 min following treatment, 15.8% of patients who received 25 g of dextrose developed hypoglycemia, as opposed to 8.3% of patients who received 50 g of dextrose (p = 0.11). Hyperglycemia was more common in patients who received 50 g of dextrose at 60 min posttreatment; however, this difference did not persist at 240 min. Potassium reduction at 60 min did not differ between groups. In patients with a pretreatment blood glucose <110 mg/dl or without diabetes, rates of hypoglycemia were significantly lower when 50 g of dextrose was administered.
Conclusion:
In the overall patient population, use of 50 g of dextrose instead of 25 g does not reduce hypoglycemia incidence. However, it may be beneficial is select patient populations, such as patients without type 2 diabetes or patients with a baseline blood glucose <110 mg/dl. Administration of 50 g of dextrose did not appear to place patients at significant risk for hyperglycemia however and could be considered during treatment of hyperkalemia.
Introduction
Hyperkalemia, an electrolyte abnormality that occurs frequently in both the emergency department and intensive care unit, is defined as a serum potassium level >5 milliequivalents per milliliter (mEq/ml). 1 While hyperkalemia may result in symptoms such as relatively minor muscle pain and weakness, it may also destabilize the cardiac membrane. 2 This can result in ventricular arrhythmias and cardiac arrest, particularly at potassium levels >6 mEq/ml.1–3 In the event that electrocardiogram abnormalities develop, hyperkalemia must be treated in a prompt and effective manner.
Treatment of hyperkalemia involves targeting multiple processes.2–7 Rapid-acting intravenous (IV) insulin is the most commonly used agent to redistribute potassium via stimulation of the sodium–potassium ATPase pump. It is typically dosed at 10 units and is administered via rapid IV push.2,3 Dextrose is administered IV concomitantly with the previously described insulin to prevent development of hypoglycemia. Additionally, there are data to suggest that IV dextrose may potentially augment redistribution of potassium via stimulation of endogenous insulin secretion.2,3,8
Hypoglycemia is one of the most significant complications of IV insulin administration and it has been associated with both increased inpatient length of stay and mortality.9–11 Several retrospective studies have been conducted which describe the incidence of hypoglycemia development following hyperkalemia treatment with IV insulin, with rates ranging from approximately 8–20%.12–15 A number of risk factors have been reported that place patients at greater risk for hypoglycemia development including renal dysfunction, baseline blood glucose, and lower patient weight.12,14
One strategy to prevent hypoglycemia is to increase the dose of dextrose that is administered concomitantly with insulin. However, no trials have been published to date that exclusively compare the effects of different IV dextrose doses. The objective of this study is to compare the impact of administration of 25 g of IV dextrose versus 50 g of IV dextrose in addition to 10 units of IV insulin on rates of hypoglycemia development.
Methods
This was a retrospective, multicenter, matched cohort study conducted at two tertiary care hospitals. It was approved by the Indiana University Institutional Review Board. Both of the centers utilized an order set for hyperkalemia reversal which allowed prescribers to order a treatment regimen including 10 units of IV insulin lispro, either 25 or 50 g of IV dextrose, and blood glucose checks at 60 min following administration of insulin. The order set does not provide guidance to providers with regard to the choice of 25 or 50 g of dextrose and the decision is left to the discretion of the provider. Many patients receive a follow up blood glucose check at 4–6 h following administration of IV insulin, but this is not mandated by the hyperkalemia order set.
Patients were included if they were at least 18 years old and received either 25 or 50 g of dextrose between July 2014 and August 2015 as part of the hyperkalemia treatment order set. Exclusion criteria were administration of an IV insulin lispro dose different than 10 units; failure to administer IV dextrose within 15 min of IV insulin; hyperkalemia development secondary to documented rhabdomyolysis, hemolysis, or tumor lysis syndrome; failure to check a blood glucose level within 120 min of therapy; previous treatment for hyperkalemia during the current admission; concurrent use of an IV insulin infusion; and concurrent use of an dextrose infusion >5% in concentration within the 60 min following administration of IV insulin. After the first blood glucose check at approximately 60 min, patients were able to receive open IV dextrose or subcutaneous insulin as clinically indicated.
Patient groups were matched based on three comorbidities that effect the development of hypoglycemia following hyperkalemia treatment: acute kidney injury (AKI), end-stage renal disease (ESRD), and type 2 diabetes mellitus (DM). AKI was defined as meeting Kidney Disease Improving Global Outcomes criteria for acute kidney injury, ESRD was defined as documented dependence on hemodialysis, and DM was defined as a documented history of type 2 DM by a treating physician in the patient’s past medical history. Subgroup analyses were conducted in patients with or without baseline DM and based on baseline blood glucose levels.
The primary outcome of the study was the percentage of patients who developed hypoglycemia (blood glucose < 70 mg/dl) at 60 min following the administration of IV insulin. Secondary outcomes included the percentage of patients who developed hypoglycemia at 240 min following IV insulin administration, percentage of patients with severe hypoglycemia (blood glucose < 40 mg/dl) at both 60 and 240 min, percentage of patients with hyperglycemia (blood glucose > 180 mg/dl) at 60 and 240 min, and reduction in serum potassium at 60 min, and change in blood glucose levels at 60 min.
A power calculation was conducted which indicated that 240 patients would be necessary to provide 80% power at an alpha of 0.05 to detect a reduction in hypoglycemia percentages from 20% to 7%. For statistical analysis, the primary outcome of the study was analyzed using a Chi-square test. Data did not have parametric distribution and secondary outcomes were analyzed using a Chi-square test, Fisher’s exact test, or Mann–Whitney U test as indicated. All statistical analysis was conducted via IBM SPSS (IBM Corp., Armonk, NY, USA).
Results
A total of 132 patients who received 50 g of dextrose and 286 patients who received 25 g were eligible for study inclusion (Figure 1). First, 120 patients were randomly selected from the group who received 50 g of dextrose to compose one patient group. An equal number of patients who received 25 g of dextrose were then matched to the selected patients who received 50 g of dextrose based on the presence of the previously described baseline comorbidities (AKI, ESRD, and DM). As a result, 240 patients were included for final analysis.
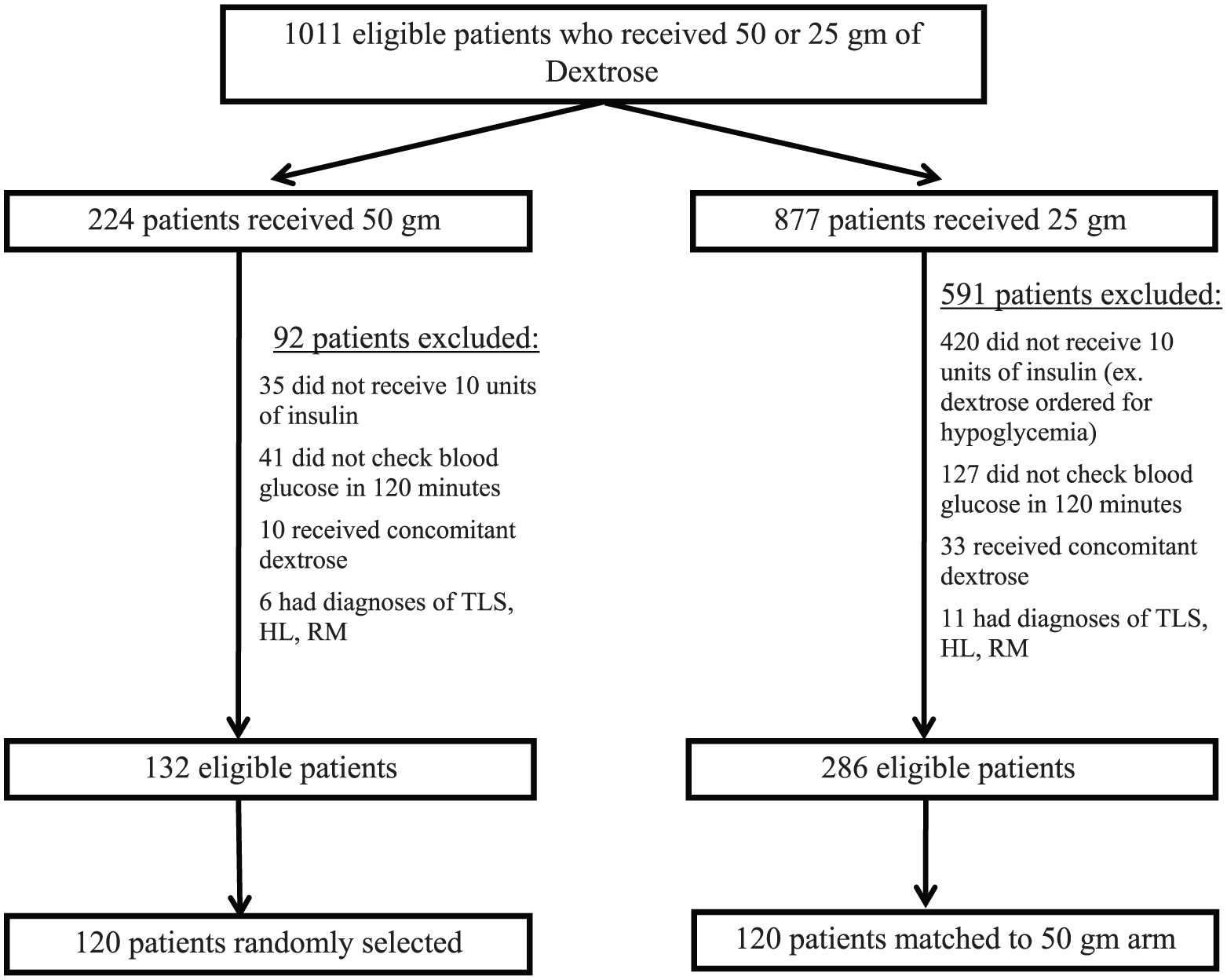
Patient selection.
Baseline patient weight, age, and sex did not differ significantly between groups (Table 1). In each arm, 50.8% of patients had an AKI, 28.3% had baseline ESRD, and 26.7% of patients had baseline DM. Baseline potassium levels were higher in patients who received 25 g of dextrose (6.5 versus 6.3 mEq/l, p = 0.046). Patients who received 25 g of dextrose also had significantly higher baseline blood glucose levels relative to patients who received 50 g of dextrose (126 versus 107 mg/dl, p = 0.008) and were more likely to have a baseline blood glucose level >140 mg/dl (41.7% versus 19.2%, p ⩽ 0.001).
Baseline patient characteristics.
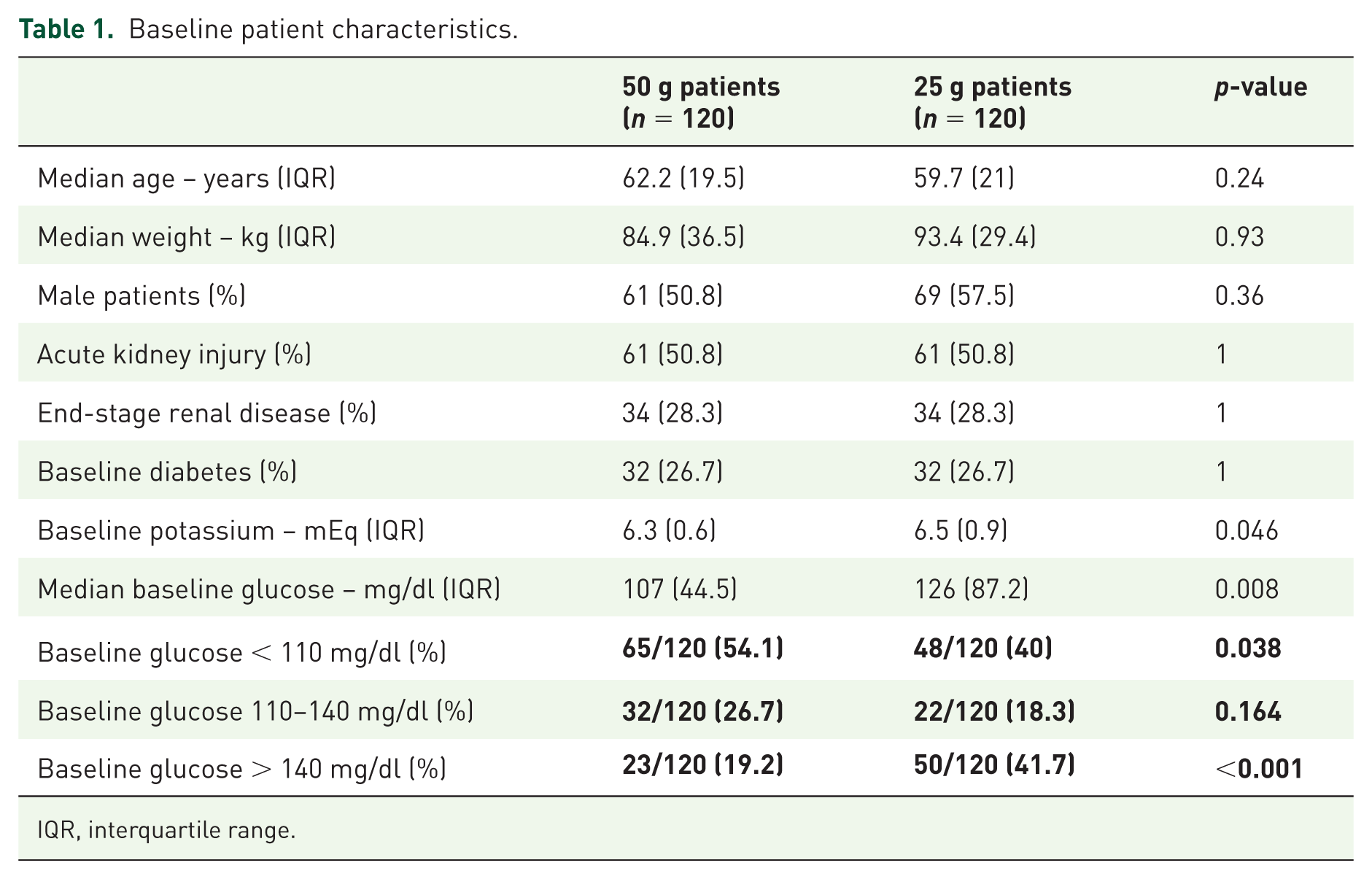
IQR, interquartile range.
Regarding the primary outcome of the study, 8.3% of patients who received 50 g of dextrose developed hypoglycemia at 60 min following administration compared with 15.8% of patients who received 25 g of dextrose, as depicted in Figure 2 (p = 0.11). At 60 min following administration of insulin, blood glucose increased by a mean of 65.1 ± 97.9 mg/dl in patients receiving 50 g of dextrose compared with a mean of 7.5 ± 51.7 mg/d in patients receiving 25 g of dextrose (p ⩽ 0.01). At 240 min following administration of insulin, only 5% of patients who received 50 g of dextrose were hypoglycemic compared with 4.2% of patients who received 25 g of dextrose (p = 1.00). Severe hypoglycemia occurrence was rare and rates of hypoglycemia did not differ significantly between the groups at either time point.
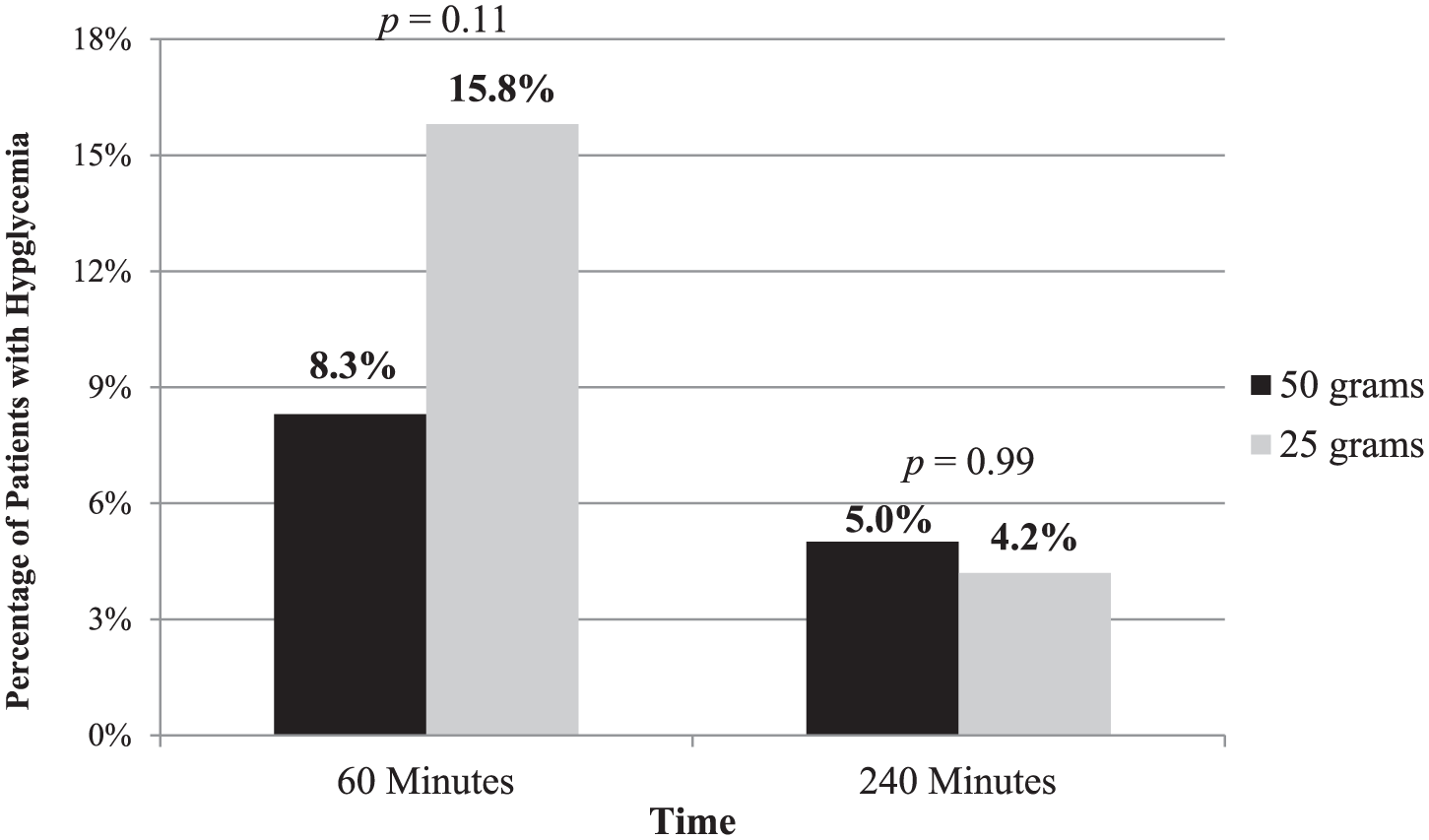
Hypoglycemia outcomes.
At 60 min following dextrose administration, 52.5% of patients who received the 50 g dose experienced hyperglycemia compared with 26.7% of patients who received 25 g (p = 0.001). Overall, 77.5% (186/240) of patients had a blood glucose level collected 240 min after administration of insulin. Only 10.8% of patients who received 50 g of dextrose compared with 14.2% of patients who received 25 g (p = 0.56) remained hyperglycemic at this time point.
Serum potassium reduction was similar between patient groups. Patients who received 50 g of dextrose had a median serum potassium reduction in 1.1 mEq/ml at 60 min following administration compared with 1 mEq/ml in patients who received 25 g of dextrose (p = 0.76).
A subgroup analysis in patients without baseline DM was conducted. In this analysis, 7.9% (7/88) of patients who received 50 g of dextrose were hypoglycemic at 60 min, compared with 19.3% (17/88) of patients who received 25 g of dextrose (p = 0.046). Hyperglycemia outcomes were similar to that of the overall patient population.
Patients with diabetes were also examined. A relatively small number of these patients developed hypoglycemia at 60 min; 9.4% (3/32) of patients who received 50 g of dextrose became hypoglycemic compared with 6.2% (2/32) of patients receiving 25 g. Hyperglycemia was present at 60 min in 53.1% (17/32) of patients who received 50 g of dextrose relative to 40.6% (13/32) of patient who received 25 g (p = 0.45). Notably, the number of patients who were hyperglycemic decreased dramatically at the 240 min time point; only 18.8% (6/32) of patients receiving 50 g of dextrose still had hyperglycemia compared with 31.2% (10/32) of patients who received 25 g of dextrose (p = 0.39).
Hypoglycemia risk at 60 min following administration of either 50 g or 25 g of dextrose was assessed by baseline blood glucose. There was no difference in the rates of hypoglycemia at 60 min in patients with a baseline blood glucose >140 mg/dl (4.3% versus 2%, p = 1.00) or patients with a baseline glucose 110–140 mg/dl (6.3% versus 4.5%, p = 1.00). Among patients with a baseline blood glucose <110 mg/dl hypoglycemia developed in 10.8 % (7/65) of patients who received 50 g of dextrose compared with 35.4% (17/48) of patients who received 25 g of dextrose (p = 0.002).
Discussion
In this study, no statistically significant difference was noted in hypoglycemia occurrence at 60 min following administration of 10 units of IV insulin lispro in addition to 50 g of IV dextrose as compared with 25 g. While administration of 50 g of dextrose did yield more hyperglycemia at 60 min in patients compared with a 25 gram dose, this finding was not prolonged and hyperglycemia rates at 240 min between patient groups did not differ.
This is the largest study conducted to date describing the development of hypoglycemia following hyperkalemia treatment with IV insulin. To the authors’ knowledge, it is also the first study to compare the impact of altering doses of dextrose on hypoglycemia development when given with a fixed dose of insulin.
Although the primary outcome did not reach statistical significance, a large reduction in hypoglycemia at 60 min in patients who received 50 g of dextrose as opposed to 25 g was observed. When both patients with a baseline blood glucose <110 mg/dl and patients without baseline DM were analyzed, the difference in hypoglycemia occurrence achieved a statistically significant value in favor of patients receiving 50 g of dextrose. Furthermore, administration of 50 g of dextrose did not place patients at a greater risk for prolonged hyperglycemia relative to 25 g, even in patients with baseline DM. Treatment of hyperkalemia may be indicated during a medical emergency when little is known regarding the patient’s past medical history. Data from this trial suggest that empiric administration of 50 g of dextrose instead of 25 g may be preferred given the potential to prevent a hypoglycemic event without putting a patient at increased risk for prolonged hyperglycemia.
Another strategy to reduce hypoglycemia development is to administer lower doses of insulin. Overall, two studies have been conducted to compare altering the dose of insulin in hyperkalemia therapy and the subsequent effects on development of hypoglycemia. Pierce and colleagues did not find a protective effect on hypoglycemia development in patients when 5 units of insulin were administered as opposed to 10 units in addition to 25 g of dextrose. 15 On the other hand, Wheeler and colleagues did demonstrate a statistical reduction in hypoglycemia development when a weight-based insulin dosing protocol of 0.1 units/kg was used relative to a standard 10 units in addition to 50 g of dextrose. 13 A concern with use of a lower insulin dose is a corresponding reduction in stimulation of sodium–potassium ATPase and inferior potassium redistribution. The study by Wheeler and colleagues only reported the lowest serum potassium value in the 12 h following administration of insulin; in this time frame, therapy with a loop diuretic, potassium exchange resin, or renal replacement therapy may have been initiated, all of which would contribute to lower serum potassium levels. 13 Additionally, the protocol described by Wheeler and colleagues may be difficult to utilize in an emergency situation when patient weight is unknown. This study illustrates a treatment regimen which is relatively simple, rapidly reduces serum potassium concentrations, and yields low rates of hypoglycemia.
Baseline blood glucose levels have also been shown to affect the development of hypoglycemia. In this analysis, baseline blood glucose levels were statistically higher in the group of patients that received 25 g of dextrose, which may have had a protective effect against hypoglycemia development in these patients. Furthermore, in patients with a baseline blood glucose <110 mg/dl, a dextrose dose of 50 g was found to have a protective effect on occurrence of hypoglycemia at 60 min relative to a dextrose dose of 25 g. Although this patient population saw more favorable outcomes with administration of dextrose at a dose of 50 g, rates of severe hypoglycemia at 60 min and hypoglycemia at 240 were not different between treatment groups.
This study is not without other limitations. The differences in baseline blood glucose between treatment groups indicate that there was likely a selection bias in dextrose dose among treating providers. Both hospitals in this study are in the same health system and the results of this study may not be generalizable to other practice sites. While previous studies examining hyperkalemia therapy used regular human insulin, this study used insulin lispro.5,12–15 Although pharmacokinetic parameters for the two types of insulin do not significantly differ when the product is given IV, the impact of insulin lispro use is uncertain. There was no standardization regarding measuring a blood glucose-using point of care test or laboratory evaluation; the accuracy of these two mechanisms may differ. Finally, while IV intake was monitored for all study patients, enteral administration of glucose was not standardized. It is possible that administration of enteral glucose impacted hypoglycemia development.
Conclusions
In this study, use of 50 g of IV dextrose as opposed to 25 g demonstrated a limited protective benefit regarding hypoglycemia development. Certain patient populations, such as patients without diabetes or patients with a pretreatment blood glucose <110 mg/dl, achieved greater benefit from use of 50 g of dextrose. Additionally, administration of the higher dose of dextrose did not place patients at risk for prolonged hyperglycemia. Prospective analysis is warranted at this time to determine whether altering the dose of dextrose alone is the optimal way to prevent hypoglycemia development following treatment of hyperkalemia.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The authors declare that there is no conflict of interest.