
Abstract
Norepinephrine (NE) is commonly recommended as a first-line vasopressor treatment for the majority of adult patients with acute circulatory failure.1,2 Critically ill patients with circulatory shock may need rescue treatment with high doses of NE, which can be associated with a poor outcome due to excessive vasoconstriction. 3 We describe a patient with mixed cardiogenic and septic shock who developed bilateral digital necrosis while on an extremely high dose of intravenous NE. According to the Naranjo probability scale, 4 a probable relationship between the adverse effect (digital necrosis) and NE therapy in this patient is indicated.
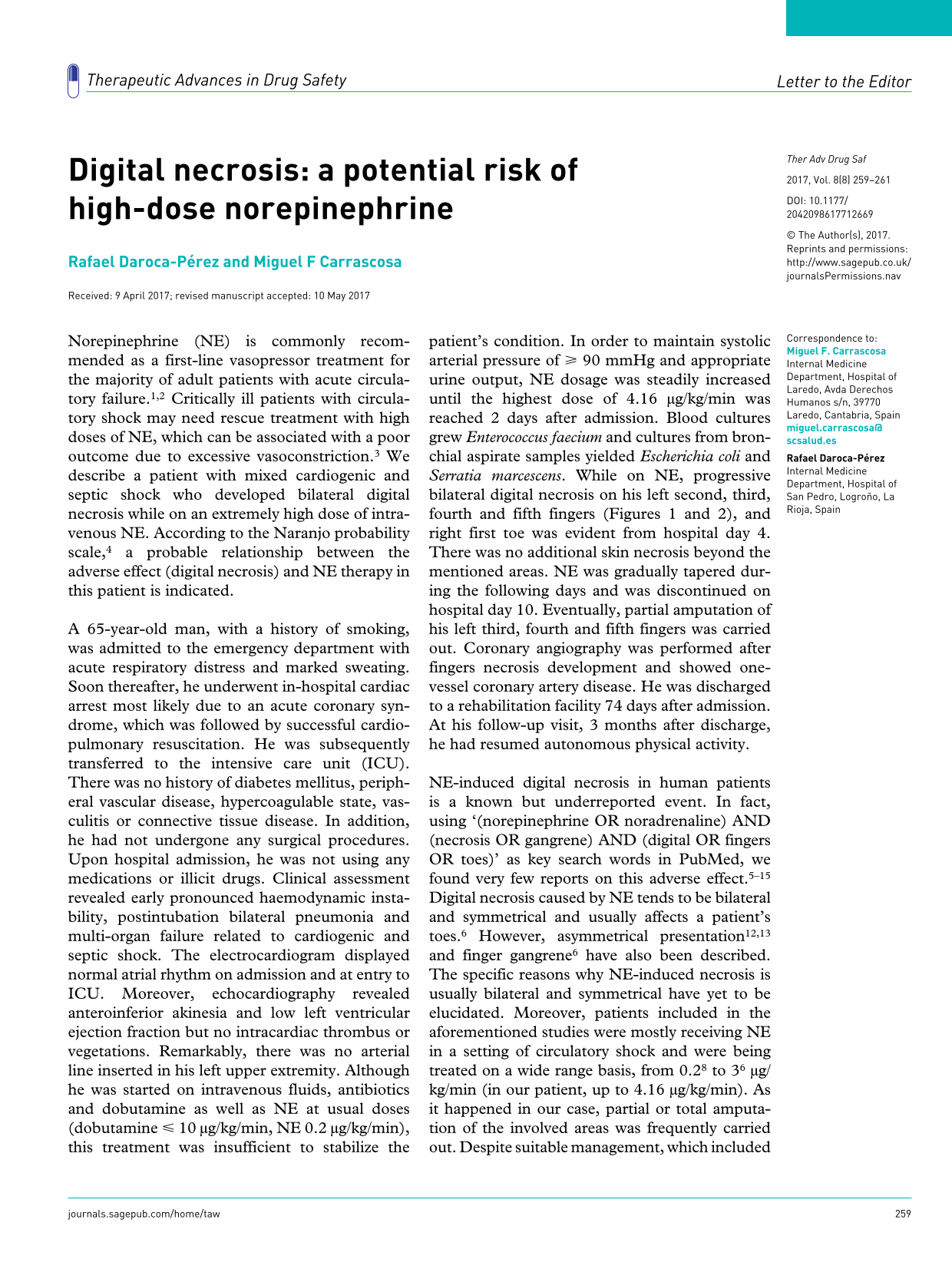
A 65-year-old man, with a history of smoking, was admitted to the emergency department with acute respiratory distress and marked sweating. Soon thereafter, he underwent in-hospital cardiac arrest most likely due to an acute coronary syndrome, which was followed by successful cardiopulmonary resuscitation. He was subsequently transferred to the intensive care unit (ICU). There was no history of diabetes mellitus, peripheral vascular disease, hypercoagulable state, vasculitis or connective tissue disease. In addition, he had not undergone any surgical procedures. Upon hospital admission, he was not using any medications or illicit drugs. Clinical assessment revealed early pronounced haemodynamic instability, postintubation bilateral pneumonia and multi-organ failure related to cardiogenic and septic shock. The electrocardiogram displayed normal atrial rhythm on admission and at entry to ICU. Moreover, echocardiography revealed anteroinferior akinesia and low left ventricular ejection fraction but no intracardiac thrombus or vegetations. Remarkably, there was no arterial line inserted in his left upper extremity. Although he was started on intravenous fluids, antibiotics and dobutamine as well as NE at usual doses (dobutamine ⩽ 10 µg/kg/min, NE 0.2 µg/kg/min), this treatment was insufficient to stabilize the patient’s condition. In order to maintain systolic arterial pressure of ⩾ 90 mmHg and appropriate urine output, NE dosage was steadily increased until the highest dose of 4.16 μg/kg/min was reached 2 days after admission. Blood cultures grew Enterococcus faecium and cultures from bronchial aspirate samples yielded Escherichia coli and Serratia marcescens. While on NE, progressive bilateral digital necrosis on his left second, third, fourth and fifth fingers (Figures 1 and 2), and right first toe was evident from hospital day 4. There was no additional skin necrosis beyond the mentioned areas. NE was gradually tapered during the following days and was discontinued on hospital day 10. Eventually, partial amputation of his left third, fourth and fifth fingers was carried out. Coronary angiography was performed after fingers necrosis development and showed one-vessel coronary artery disease. He was discharged to a rehabilitation facility 74 days after admission. At his follow-up visit, 3 months after discharge, he had resumed autonomous physical activity.

Appearance of the left hand and fingers.

Necrosis of all fingers except thumb while the patient was on a very high dose of intravenous norepinephrine.
NE-induced digital necrosis in human patients is a known but underreported event. In fact, using ‘(norepinephrine OR noradrenaline) AND (necrosis OR gangrene) AND (digital OR fingers OR toes)’ as key search words in PubMed, we found very few reports on this adverse effect.5–15 Digital necrosis caused by NE tends to be bilateral and symmetrical and usually affects a patient’s toes. 6 However, asymmetrical presentation12,13 and finger gangrene 6 have also been described. The specific reasons why NE-induced necrosis is usually bilateral and symmetrical have yet to be elucidated. Moreover, patients included in the aforementioned studies were mostly receiving NE in a setting of circulatory shock and were being treated on a wide range basis, from 0.28 to 36 μg/kg/min (in our patient, up to 4.16 μg/kg/min). As it happened in our case, partial or total amputation of the involved areas was frequently carried out. Despite suitable management, which included eventual surgical intervention, the mortality rate remained high.
Pre-existing peripheral vascular disease, concomitant use of other vasopressors (dopamine especially), and prolonged hypotension can increase the risk of NE-induced digital necrosis. In our patient, however, there was no history of peripheral vasculopathy, dopamine was not administered and systolic blood pressure remained at ⩾ 90 mmHg almost constantly throughout his hospital stay; there were only limited and short periods of low blood pressure while he was in the ICU. Since the vasospastic effects of NE may be more intense in the digital vascular beds, low blood pressure could certainly have contributed to his digital gangrene. Of note, it is also true that NE is usually prescribed in critical clinical settings where hypotension and compromised peripheral circulation are relevant and that necrosis is quite uncommon in such circumstances, providing NE is administered at low doses. In addition, the patient did not undergo cardiac catheterization before developing necrosis and endocarditis, disseminated intravascular coagulation and purpura fulminans (which involves extensive, multicentric skin necrosis) were not present. Finally, to our knowledge, E.faecium bacteremia has not been associated with digital necrosis.
Although it is not closely tied to the present case, it is interesting to remember the existing controversy of whether unintentional digital administration of epinephrine in the first-aid treatment of anaphylaxis can cause cutaneous necrosis. In this regard, although consequences of accidental autoinjection might be serious, whether local, exceptionally leading to finger amputation, or systemic,16,17 these events usually have a favourable outcome within 2–24 h of injection, with or without treatment.16,17
An approach that includes early appropriate fluid resuscitation, suitable antibiotic therapy, blood transfusion when needed and cautious use of inotropes with scant vasopressor effect (e.g. dobutamine), could help to keep patients away from very high doses of NE in a context of circulatory shock. Although a maximum tolerable dose of NE has not been established, it is known that high dosing increases the risk of extreme vasoconstriction, tissue hypoperfusion and necrosis. Thus, the current existing recommendations suggest that doses > 1.23–22 μg/kg/min should ideally be avoided and that NE therapy should be withdrawn as early as possible to minimize the risk of necrosis, especially in the presence of any coldness and discoloration in the extremities. 7
Footnotes
Acknowledgements
The involvement of each author in the elaboration of the manuscript was as follows. RDP: care for the patient; substantial contribution to study conception and design; acquisition of data; analysis and interpretation of data; critical revision of the manuscript for important intellectual content; administrative, technical or material support; final approval of the version to be published; agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. MFC: substantial contribution to study conception and design; acquisition of data; analysis and interpretation of data; drafting of the manuscript; critical revision of the manuscript for important intellectual content; administrative, technical or material support; study supervision; final approval of the version to be published; agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors
Conflict of interest statement
The authors declare no conflicts of interest in preparing this article.
Disclosures
The authors confirm that the patient’s written and verbal informed consent were obtained for this case study.
The authors state that the management/leadership teams of their hospital (Dirección Gerencia y Dirección Médica of the Hospital of Laredo) considered that there were no obstacles or restraints to reporting this case.