
Abstract

Introduction
Albiglutide is an injectable glucagon-like peptide-1 (GLP-1) receptor agonist, approved by the US Food and Drug Administration (FDA) in 2014 for the treatment of type 2 diabetes mellitus (T2DM) [Prasad-Reddy and Isaacs, 2015]. Administered initially as a 30 mg subcutaneous (SC) once-weekly injection and subsequently as 50 mg SC to achieve glycemic targets, it provides effective glycemic control through an increase in glucose-dependent insulin secretion and a decrease in glucagon levels [Prasad-Reddy and Isaacs, 2015; Gallwitz, 2016; Madsbad, 2015]. In addition to reducing blood glucose, it also promotes weight loss by increasing satiety and delaying gastric emptying [Prasad-Reddy and Isaacs, 2015; Madsbad, 2015]. Owing to its long half-life of about 5 days, it allows the ease of once-a-week administration and improved adherence. [Madsbad, 2015]. Adverse effects reported from its use include upper respiratory tract infections, nausea, and diarrhea [Madsbad, 2015; Trujillo and Nuffer, 2014]. From the pooled data across the eight phase III HARMONY trials, pancreatitis was likely attributed to the use of albiglutide compared with placebo or comparative drugs. There is also an issued warning on the package insert against use in patients with a history of pancreatitis. To our knowledge no case of albiglutide-induced pancreatitis has been reported following FDA approval. We report the first case of a 59-year-old man who was diagnosed with albiglutide-induced pancreatitis and managed successfully at our medical center.
Case presentation
A 59-year-old African-American man presented to the emergency department with severe, 9/10, intermittent, burning, nonradiating epigastric pain of 4 days duration. The pain was aggravated with dietary intake, and associated with nausea but no vomiting. He had a past history of T2DM, hypertension, hepatitis C with sustained virologic response, and benign prostatic hypertrophy. He had been started on 30 mg albiglutide SC weekly 4 weeks prior to admission, and had been taking atorvastatin, amlodipine, glipizide, and metformin for several years. The onset of his epigastric pain was 2 days prior to his fourth dose of albiglutide. The patient had denied alcohol consumption for the last 8 years, had a cholecystectomy 2 years ago, and endorsed an active lifestyle.
On examination, his vital signs were stable and examination showed no icterus, xanthomas, or organomegaly. There was epigastric tenderness with normal bowel sounds. Initial blood tests included lipase 1184 U/L (normal range, 20–200 U/L), amylase 113 U/L, calcium 2.35 mmol/L, bilirubin 6.84 µmol/L, aspartate aminotransferase (AST) 60 U/L, alanine aminotransferase (ALT) 173 U/L, hemoglobin A1C (HbA1C) 11.1%, triglycerides of 0.67/ mmol/L white blood cell count 3970 mm3, hemoglobin 126 g/L (SI), hematocrit 38.4%, and platelets of 285×109/L. Troponins were negative and an electrocardiogram showed normal sinus rhythm with no acute changes. Computed tomography scan of the abdomen revealed no pancreatic findings. An ultrasound of the abdomen showed surgically absent gall bladder and a short segment of common bile duct without stones or ductal dilatation. A diagnosis of pancreatitis based on abdominal pain and elevated lipase was made [Banks et al. 2013], and the patient was started on fluids with oral dietary restriction and pain control.
Alcohol, gallstones, hypertriglyceridemia, hypercalcemia, autoimmune pancreatitis, and smoking were ruled out, and with a Naranjo Adverse Drug Reaction Score of 5, a probable association of albiglutide with pancreatitis was suspected. The Bedside Index of Severity in Acute Pancreatitis (BISAP) score was 0. The albiglutide was discontinued and intolerance was documented in the chart.
The patient was admitted for overnight observation. His blood sugars ranged between 11.1 mmol/L and 17.2 mmol/L and he was treated with glargine insulin during the hospital stay. He reported improvement in pain and tolerated a liquid diet after 1 day.
He was discharged home on glargine insulin, metformin, and glipizide for diabetes control. Laboratory tests showed improvement in lipase to 678 U/L (on day 2) and 112 U/L on his 2-week follow-up visit to the clinic. AST and ALT levels on a follow-up visit were 24 U/L and 33 U/L, respectively. On his 3-month follow-up visit, the patient continued to do well, with HbA1C of 7.0%, improvement in lipid profile, and a lipase level of 71 U/L.
Discussion
Albiglutide is a newer agent in the GLP-1 receptor agonists class that has been shown to be effective in management of T2DM and was well tolerated in clinical trials [Prasad-Reddy and Isaacs, 2015; Gallwitz, 2016; Madsbad, 2015; Trujillo and Nuffer, 2014]. Albiglutide activates protein kinase A through a different mechanism from other GLP-1 receptor agonists. It increases intracellular levels of calcium, subsequently leading to the release of insulin vesicles from pancreatic beta cells. Moreover, this agent is also unique in its ability to resist degradation by dipeptidyl peptidase-4 (DPP-4). Its long half-life of 5 days can be attributed to the fact that the drug resists hydrolysis of the two terminal amino acids by DDP-4 enzyme [Sharma et al. 2016].
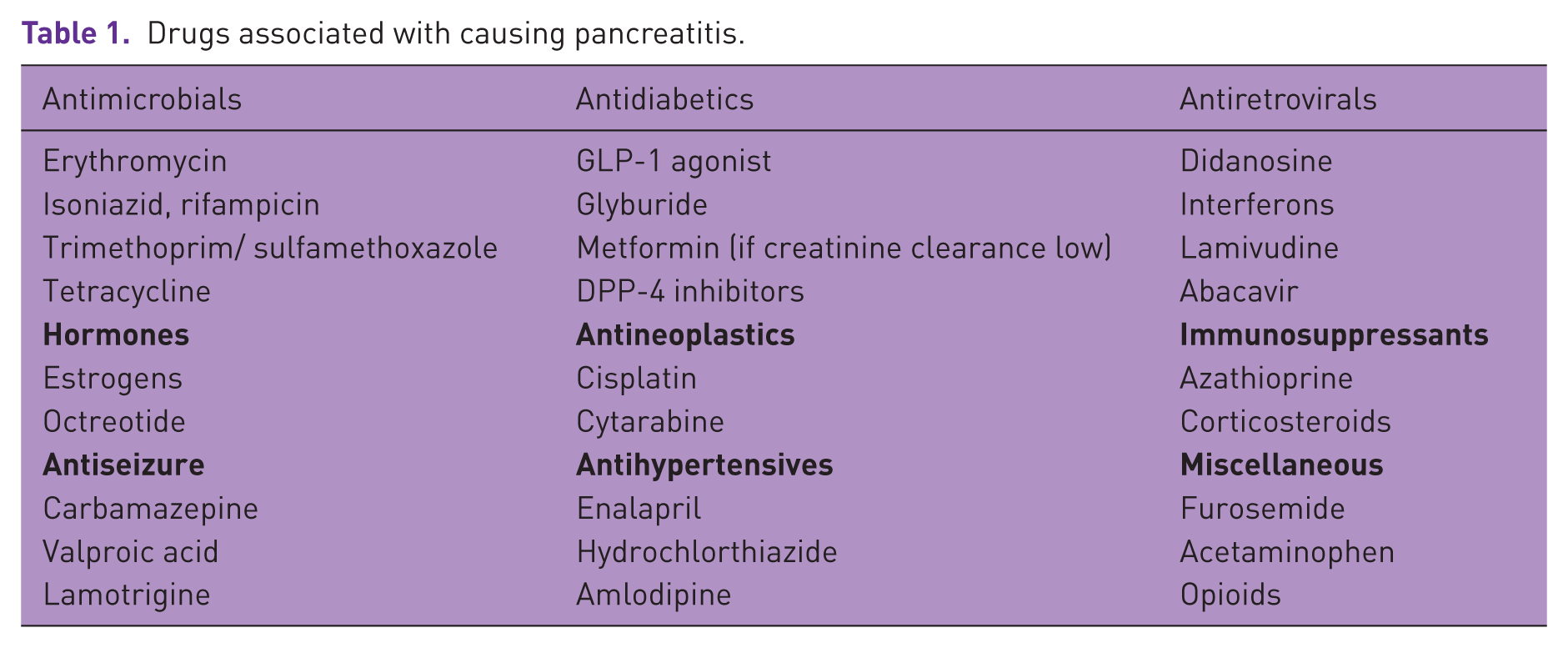
Cases of pancreatitis have been reported with GLP-1 receptor agonists, but more commonly with liraglutide and exenatide [Anderson and Trujillo, 2010; Montilla et al. 2014] (Table 1). Interestingly, randomized control trials and meta-analysis have shown no increased risk of acute pancreatitis with incretin-based therapies but have reported increased lipase levels in patients on incretin therapy [Smits et al. 2015; Filippatos et al. 2014; Giorda et al. 2014; Thomsen et al. 2015]. Isolated case reports of acute pancreatitis linked to certain GLP-1 receptor agonists have been increasingly reported despite the fact that no causal relationship has been established by controlled, randomized double-blinded clinical trials. Across all eight HARMONY trials that established the safety and efficacy of albiglutide, the incidence of albiglutide-induced pancreatitis was 0.3% [Blair and Keating, 2015]. While the risk in the trials was based on 12 weeks of therapy, our case reveals the possibility of developing pancreatitis with incretin therapy use as early as 4 weeks. To our knowledge, this is the first case of albiglutide-induced pancreatitis reported since approval of the drug by the FDA.
Drugs associated with causing pancreatitis.
Drug-induced pancreatitis remains a diagnosis of exclusion as diagnoses including idiopathic acute pancreatitis must be taken into account prior to inappropriate discontinuation of an agent [Tenner, 2014]. In our case, idiopathic acute pancreatitis cannot be ruled out since an extensive evaluation including an endoscopic retrograde cholangiopancreatography, endoscopic ultrasound, or magnetic resonance cholangiopancreatography was not deemed crucial, considering that the patient improved with conservative treatment. Such extensive, invasive procedures could possibly discover microlithiasis, sphincter of Oddi dysfunction, or pancreas divisum, all of which would explain an initial diagnosis of idiopathic acute pancreatitis [Tenner, 2014]. However, the fact that the patient developed severe epigastric tenderness along with blood laboratory results to support pancreatitis 4 weeks after the initiation of a new agent and improvement in symptoms after its cessation, strongly hints to the possibility of albiglutide-induced pancreatitis. Moreover, we can sufficiently rule out alternative diagnoses including alcohol, hypertriglyceridemia, and gallstones as the cause of his pancreatitis based on a thorough history, laboratory values, and imaging results.
Conclusion
Though shown to be effective and well tolerated in the management of T2DM, albiglutide can possibly be associated with acute pancreatitis as highlighted by our case. The symptoms can occur within the first few weeks of therapy and hence providers must be aware and counsel patients of this potential side effect as the use of albiglutide increases in the community. Pancreatitis is itself common in diabetics, but when related to anti-diabetic medications like albiglutide, the agent should be discontinued; intolerance documented and alternative therapies be considered for glycemic control. Asymptomatic elevations in lipase are reported with these drugs, and should not be a reason for discontinuation of the medication.
Footnotes
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Conflict of interest statement
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.