
Abstract
Tiotropium is a long-acting inhaled anticholinergic agent that is widely used in the treatment of chronic obstructive pulmonary disease (COPD). It was initially launched as the tiotropium HandiHaler formulation, but this was followed by a newer version based on a potentially more efficient drug delivery device, known as Respimat. This Respimat formulation is available worldwide but has not yet succeeded in gaining regulatory approval in the USA. In the past few years, the adverse effects profile of tiotropium has come under close scrutiny owing to concerns about the possibility of urinary and cardiovascular adverse effects. These concerns appeared to have been alleviated following the publication of data from the Understanding Potential Long-Term Impacts on Function with Tiotropium (UPLIFT) trial, which was a large trial of 4 years’ duration. This trial did not show any excess myocardial infarction, renal or urinary adverse events with tiotropium compared with placebo. However, the risk of urinary retention has been in the spotlight again following publication of two observational studies reporting a significantly increased risk of urinary retention in men recently started on inhaled anticholinergics, especially when prostatic hyperplasia coexists. More recently, a meta-analysis of mortality data for the tiotropium Respimat formulation raised the possibility of an increased risk of death, including death from cardiovascular causes. It is unclear if the more efficient drug delivery offered by the Respimat device is hitting a different part of the dose-toxicity curve. In the absence of any evidence of superior clinical efficacy with tiotropium Respimat compared with tiotropium HandiHaler, some experts have argued that there is no compelling reason to choose the Respimat formulation given the new uncertainties about its safety profile.
Background
The existing controversy surrounding the safety of the inhaled anticholinergic agents (such as ipratropium bromide and tiotropium bromide) has historical origins that date back almost two decades. The potential threat of urinary retention with inhaled anticholinergics was described by Pras and colleagues in 1991 who recommended that ipratropium should be used cautiously in older men with prostatic hypertrophy [Pras et al. 1991]. Since then, a significantly increased risk of urinary infections has been described in a systematic review of trial data involving tiotropium, with a pooled odds ratio (OR) of 1.6 [95% confidence interval (CI) 1.03–2.6] [Barr et al. 2006]. However, the risk of urinary retention was not fully elucidated, with the meta-analysis showing only a trend towards increased risk of urinary retention (OR 2.6; 95% CI 0.6–12). Subsequently, a pharmaceutical company pooled analysis reported a significant OR of 10.9 (95% CI 1.26–94.9) for urinary retention with tiotropium [Kesten et al. 2006].
In addition to urinary problems that stem predictably from blockade of muscarinic receptors, the possibility of cardiovascular harm has been a constant source of debate following the publication of 5-year follow-up data from the Lung Health Study regarding an increased risk of cardiovascular adverse events with ipratropium [Anthonisen et al. 2002]. The intention-to-treat analysis of this trial showed a statistically significant increase (p = 0.027) in cardiovascular deaths (18 of 1961; 0.92%) with ipratropium compared with the placebo arm (7 of 1962; 0.36%). These findings were refuted by the sponsoring company in a subsequent subgroup analysis in which it was argued that the risk of cardiovascular adverse events stemmed from patients who were not using their ipratropium inhalers [Lanes et al. 2003]. However, this method of post hoc subanalysis based on unvalidated measures of inhaler use would generally be considered to be at a lower level of credibility than the original intention-to-treat analysis.
More recently, the debate surrounding cardiac toxicity was reignited by two independent publications in September 2008 that reported significantly increased risk of cardiovascular events with inhaled anticholinergics. A nested case–control study based on patients with newly diagnosed chronic obstructive pulmonary disease (COPD) included on the Veterans Affairs database reported a significantly elevated OR for all-cause mortality (1.11; 95% CI 1.08–1.15) and cardiovascular death (OR 1.34; 95% CI 1.22–1.47) with ipratropium [Lee et al. 2008]. A systematic review of 17 randomized controlled trials (RCTs), involving either ipratropium or tiotropium, showed that the pooled rate of major adverse cardiovascular events [myocardial infaction (MI), stroke, cardiovascular death] was significantly increased in patients treated with anticholinergic inhalers compared with controls [Singh et al. 2008]. Shortly after this review, however, the results of the large, long-term Understanding Potential Long-Term Impacts on Function with Tiotropium (UPLIFT) study were made available, showing no conclusive evidence of increased cardiovascular harm or mortality from tiotropium [Tashkin et al. 2008]. Publication of the findings from UPLIFT appeared to have assuaged any concerns regarding harm from tiotropium, with some experts stating that the data had proved reassuring [Mcivor, 2010].
However, the safety profile of tiotropium has recently come under scrutiny yet again with the publication of two articles in 2011 suggesting an increased risk of death in tiotropium users [Gershon et al. 2011; Singh et al. 2011]. Given the continuing uncertainty about possible links to serious adverse events such as urinary retention, MI and death, we aimed to review and critically appraise data on the risks of tiotropium in patients with COPD. In particular, the heterogeneity between studies needs to be explored from a methodological perspective so that the reasons for conflicting findings can be discussed. For this purpose, we have looked at the bibliographical collection of studies previously identified from two systematic reviews. We also carried out an updated search of PubMed based on the terms (ipratropium or tiotropium) and (chronic and obstructive) AND ((Clinical Trial[ptyp])) and signed up to receive a monthly automated electronic notification of any new articles including these terms.
Cardiovascular events or death with tiotropium
The risk of cardiovascular events and/or death has been evaluated through a number of different study designs, ranging from meta-analyses of RCTs through to retrospective case–control studies. A brief summary of the key studies and their findings can be found in Tables 1 and 2.
Characteristics and results of pooled analyses of randomized controlled trials evaluating mortality and cardiovascular events with tiotropium.
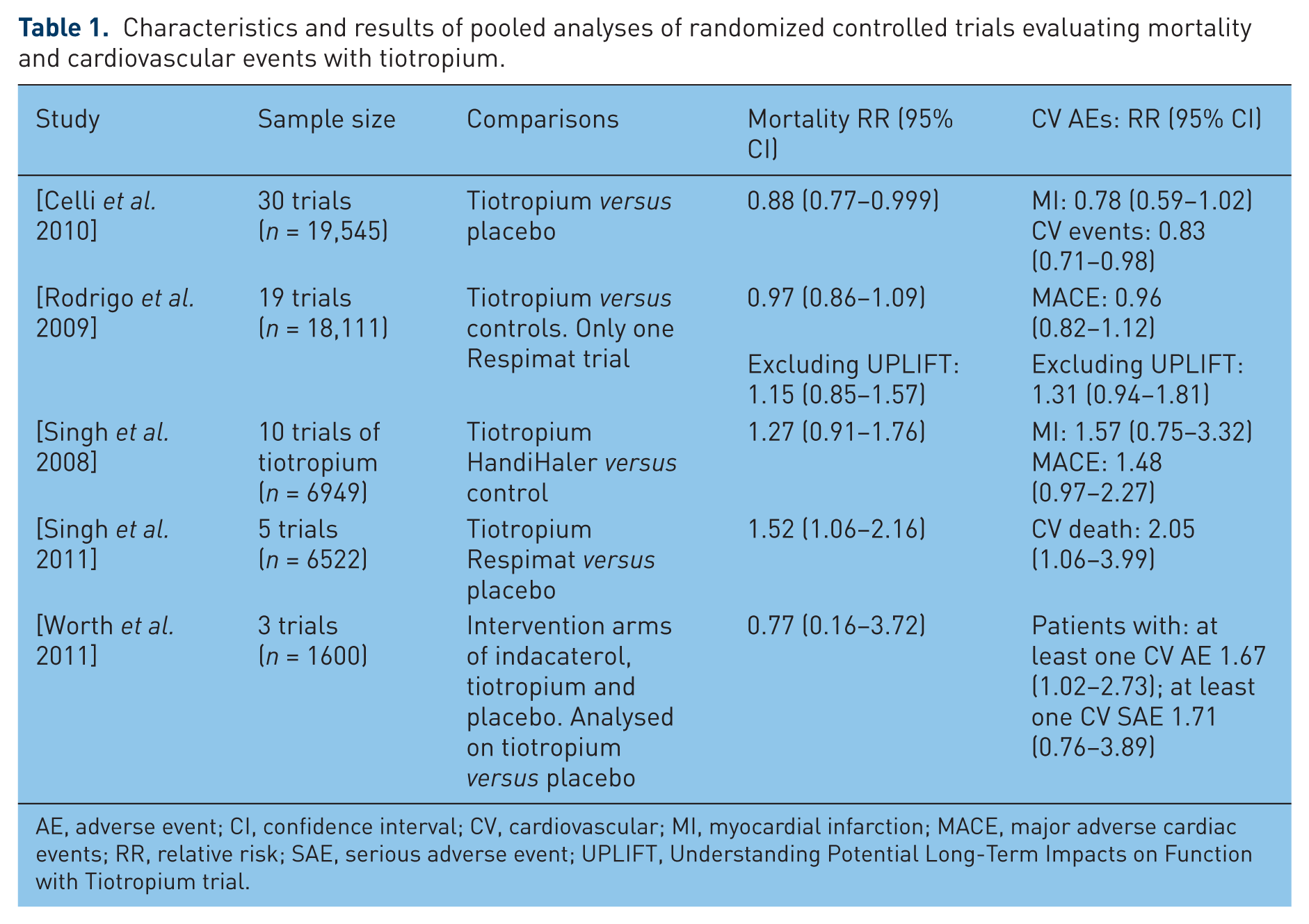
AE, adverse event; CI, confidence interval; CV, cardiovascular; MI, myocardial infarction; MACE, major adverse cardiac events; RR, relative risk; SAE, serious adverse event; UPLIFT, Understanding Potential Long-Term Impacts on Function with Tiotropium trial.
Observational studies of mortality, cardiovascular events, or acute urinary retention associated with inhaled anticholinergics.
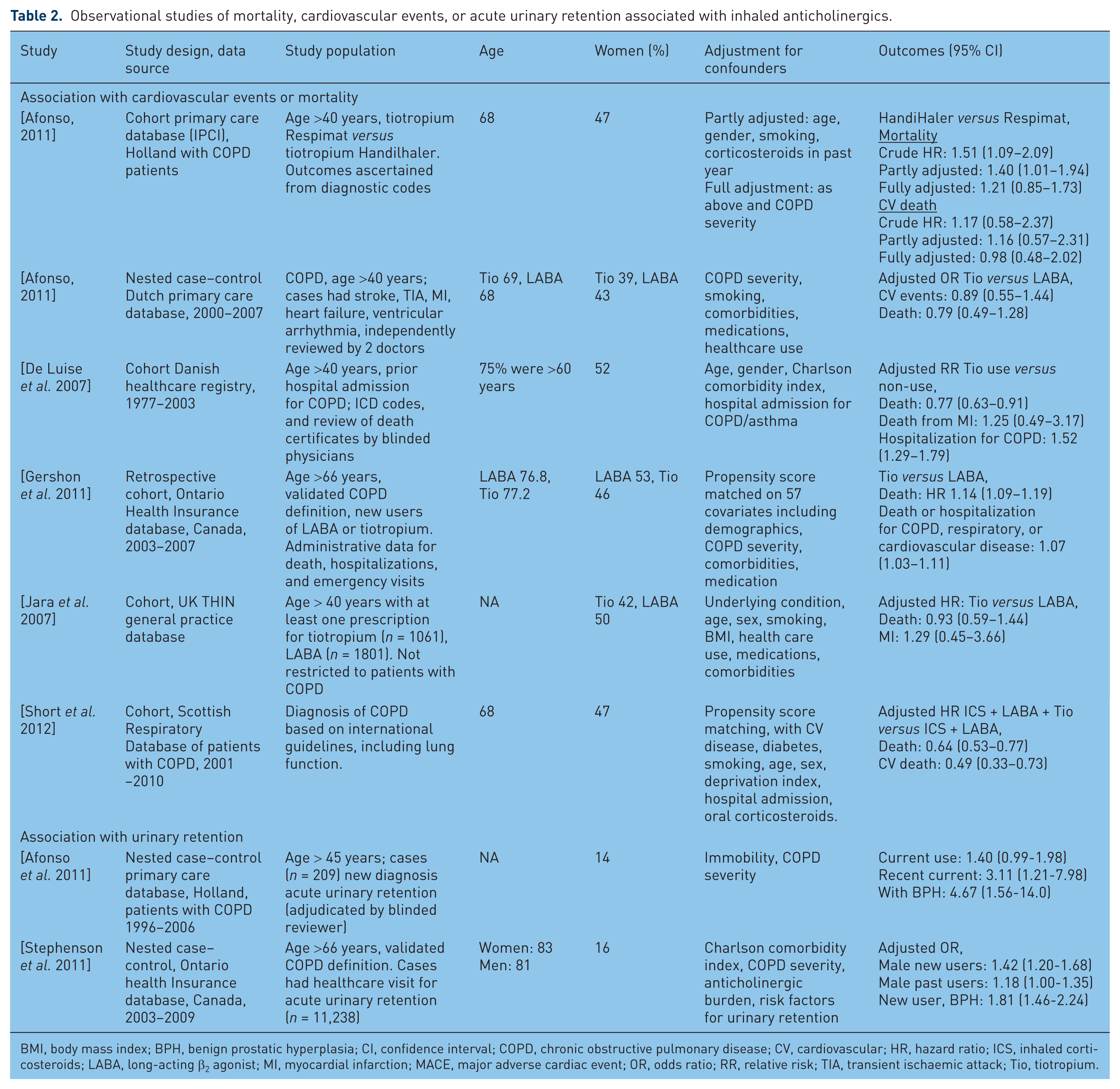
BMI, body mass index; BPH, benign prostatic hyperplasia; CI, confidence interval; COPD, chronic obstructive pulmonary disease; CV, cardiovascular; HR, hazard ratio; ICS, inhaled corticosteroids; LABA, long-acting β2 agonist; MI, myocardial infarction; MACE, major adverse cardiac event; OR, odds ratio; RR, relative risk; TIA, transient ischaemic attack; Tio, tiotropium.
Analysis of randomized controlled trials
The RCTs analysed are summarized in Table 1. An increased risk of cardiovascular events was described in a systematic review and meta-analysis of 17 RCTs involving inhaled anticholinergic drugs (ipratropium or tiotropium) [Singh et al. 2008]. Trials of tiotropium in this analysis were generally of shorter duration, ranging from 6 to 48 weeks, except for one study of 104 weeks. While attempts were made to include data from unpublished trial reports and journal manuscripts, the lack of clear or complete reporting of cardiovascular events meant that it was not possible to analyse all potentially relevant studies. Following the subsequent correction of a minor data entry error in one trial and removal of a duplicate publication, the updated meta-analysis showed a relative risk (RR) of 1.60 (95% CI 1.22–2.10) for major adverse cardiac events with inhaled anticholinergics.
This meta-analysis aimed primarily at evaluating inhaled anticholinergics as a class; it did not set out to evaluate tiotropium specifically [Singh et al. 2008]. However, subgroup data on tiotropium are available from the Forest plots, and it is possible to look at data on cardiovascular events and death relating specifically to trials involving tiotropium HandiHaler* (Boehringer Ingelheim, Ingelheim, Germany) (rather than ipratropium or tiotropium Respimat* (Boehringer Ingelheim, Ingelheim, Germany)). The results of this specific analysis are shown in Table 1, and show elevated, but nonstatistically significant point estimates for the outcomes of death, MI or major adverse cardiac events.
Shortly after this meta-analysis was published, data from the UPLIFT trial were made available [Tashkin et al. 2008] and this led to a number of newer pooled analyses incorporating mortality and cardiovascular events from UPLIFT. The first of these was a company-sponsored analysis of 30 placebo-controlled trials which reported a significant reduction in overall mortality and cardiovascular events, and a nonsignificant trend towards reduction in MI [Celli et al. 2009]. The strength of this study is that the authors were able to access company data that may not have been available in trial reports elsewhere. However, the data analysis cannot be replicated by independent researchers as some of the trial data are not publicly available, and the manuscript does not give the number of events per intervention arm in each individual trial. The absence of separate relative risk estimates from each study according to randomized groups is another limitation as it prevents readers from evaluating variation between trials or patient heterogeneity. Moreover, the key benefit of randomized comparisons between the specific trial arms was lost when the authors chose to generate pooled estimates by adding up all the patient events in the tiotropium arms from many different studies to compare against the overall placebo arms. This gives potentially less weight to smaller studies, and allows larger studies to dominate. It was not possible to tell from this type of analysis what weight each study contributed to the pooled risk (although it seems that the large UPLIFT study [Tashkin et al. 2008] would have contributed to >80% of the patient follow up), nor if any heterogeneity was present. Finally, interpretation of the validity of the results was hindered by the apparent absence of any explicit assessment of trial quality and risk of bias.
A subsequent meta-analysis of 19 tiotropium trials (18 HandiHaler and 1 Respimat) by Rodrigo and colleagues overcomes most of the limitations in the previous study by Celli and colleagues by providing risk estimates from each trial according to treatment assignment, plus some reporting of quality assessment [Rodrigo et al. 2009]. Additionally, the authors performed a sensitivity analysis based on the exclusion of the UPLIFT trial (which had been dominating the pooled estimate with weighting of around 80%). Overall the results showed no significant harmful or beneficial effect of tiotropium on mortality or major adverse cardiovascular events. However, it is worth noting that for both outcomes, reversal of direction of effect was seen [e.g. risk of major adverse cardiovascular events (MACEs) changed from 0.96 (0.82–1.12) to 1.31 (0.94–1.81) following exclusion of UPLIFT]. The authors state that trial quality (adequate or unclear allocation concealment) did not appear to be an important influence on the estimates of cardiovascular harm. Hence, any divergence between the results of UPLIFT and other trials cannot be solely explained by the argument that the datasets were of different quality (and had a different risk of bias), when a variety of other effect modifiers might also be present.
The most recent published meta-analysis of tiotropium was directed specifically at mortality with the Respimat formulation, a device that potentially provides greater ease of use and enhanced drug delivery [Singh et al. 2011]. This meta-analysis relied on data submitted by the pharmaceutical company to the US Food and Drug Administration (FDA), thus reducing the extent of missing data, an important limitation that has otherwise affected two of the preceding meta-analyses. In five randomized, placebo-controlled trials, tiotropium administered via Respimat was associated with a significant risk of mortality at the licensed dose of 5 µg daily, and some indication of a possible dose–response effect with a higher risk from trial doses of 10 µg daily. Details of cardiovascular deaths (as adjudicated by the FDA reviewer) and company-reported cardiovascular fatalities also showed a significantly increased risk of cardiovascular mortality in the meta-analysis. Limitations of this meta-analysis were the lack of details on nonfatal events such as MI or stroke, and the inability to identify patient risk factors. However, based on the sponsor’s post hoc subgroup analysis, Table 74 in the FDA documents reported that patients with cardiac rhythm disorders at baseline had an elevated risk for cardiac death (RR 8.61; 95% CI 1.10–67.2) in the Respimat trials [FDA, 2009].
Finally, indirect evidence from a pooled analysis of data from the indacaterol development programme also provides some insight into possible cardiovascular harm from tiotropium, with a RR of 1.67 (95% CI 1.02–2.73) for patients to have at least one cardiovascular adverse event with tiotropium compared with those on placebo. This pooled analysis has the same limitations as those of the analysis by Celli and colleagues, with lack of study level data or risk estimates prior to pooling [Worth et al. 2011].
Observational studies
Observational studies are summarized in Table 2. There are six observational studies with conflicting findings on death and/or cardiovascular events with tiotropium. All the studies relied on electronic records of drug exposure (e.g. prescription claims), while most of the outcome verification was through diagnostic codes, administrative healthcare data and death certificates. Hence, misclassification of exposure or outcome is a possibility in these datasets. Compared with long-acting β2 agonists (LABAs), tiotropium was associated with increased mortality in a propensity score matched new user study from Ontario, Canada [Gershon et al. 2011]. However, two company-sponsored studies from databases in Denmark [De Luise et al. 2007] and the UK [Jara et al. 2007] did not find any evidence for increased mortality with tiotropium, with the Danish study actually showing a significant association with reduced mortality (and a counter-intuitive significant increase in hospitalizations due to COPD) for tiotropium. These studies reported a nonsignificant elevated point estimate for MI with tiotropium [De Luise et al. 2007; Jara et al. 2007]. In contrast, a retrospective cohort study in Scotland reported significantly reduced cardiovascular death and overall mortality in users of tiotropium [Short et al. 2012]. An unpublished nested case–control study within the Dutch primary care databases found no significant association with tiotropium use relative to LABAs [Afonso, 2011]. Intriguingly, the same investigators also conducted a cohort study of mortality with tiotropium Respimat use compared with tiotropium HandiHaler and found a potential association with Respimat, albeit nonsignificant in a fully adjusted model [Afonso, 2011].
Risk of acute urinary retention
The possibility of urinary retention with inhaled anticholinergics has recently been evaluated in two observational studies of nested case–control design (Table 2) [Afonso et al. 2011; Stephenson et al. 2011]. The results of these studies are consistent in demonstrating that the likelihood of acute urinary retention is most prominent in patients who have recently started on inhaled anticholinergics. Afonso and colleagues studied patients with COPD in the Dutch primary care database who had a new diagnosis of acute urinary retention and found a significant association in recent (within the past 2 weeks) users of inhaled anticholinergics, with tiotropium and ipratropium showing a similar degree of risk [Afonso et al. 2011]. In a study from the Ontario database, Stephenson and colleagues found that new users of inhaled anticholinergics were significantly more likely to have had healthcare interventions for acute urinary retention, with ipratropium and tiotropium showing similar risks [Stephenson et al. 2011]. Both studies reported that men with benign prostatic hyperplasia were a particularly high risk group.
Interpreting heterogeneous data on harms
The heterogeneous evidence on cardiovascular harm and mortality with tiotropium still remains a source of debate [Cazzola et al. 2010; Singhet al. 2010]. The first point of contention stems from the discrepant findings between meta-analyses of smaller trials and the findings of a large RCT. This, in itself, is not a new phenomenon, with previous empirical research showing that discrepant findings can occur in up to 35% of cases when a meta-analysis is compared with a large trial [Lelorier et al. 1997]. However, balanced appraisal of the situation can be hampered by the natural instinct to seek clear-cut ‘black or white’ dichotomized interpretation of the contrasting data (e.g. ‘safe or unsafe’, ‘right or wrong’) when it would be more appropriate to evaluate the entire dataset surrounding this complex arena. Horwitz and colleagues. have pointed out that it is not unusual to find conflicting results between trials of the same intervention, and instead of simply attributing discrepancies to ‘poor trial quality’ or ‘inadequate sample size’, researchers need to look at heterogeneity of participants and variations in trial protocols [Horwitz et al. 1996].
From a purely methodological perspective, the principal advantage of the ‘large’ trial is the ability to generate more precise estimates. If all other quality components (e.g. randomization, allocation concealment, double blinding, adequate follow up and outcome ascertainment) are equal, the smaller trials should be at no greater risk of bias than the large trial. When carried out in the same populations and appropriately pooled, trials with smaller sample sizes ought to generate similar point estimates of risk to larger ones, albeit possibly within wider confidence intervals.
Differences in entry criteria (e.g. exclusion of those with a history of cardiovascular disease), trial populations and follow up are potential factors behind the variation in risk estimates amongst trials. The finding of lower risk in a long-term trial may stem from ‘depletion of susceptibles’ whereby those patients with susceptibility to drug-related adverse events would potentially have dropped out earlier on, with only the healthier patients remaining in the intervention arm [Hammad et al. 2011]. This may explain the discrepant findings between the long-term UPLIFT study (no significant increase in renal or urinary adverse events) [Tashkin et al. 2008] compared with the earlier company pooled analysis from short-term trials showing a significant risk of urinary retention (OR 10.9; 95% CI 1.26–94.9) [Kesten et al. 2006]. In view of the evidence from two pharmacoepidemiological studies that urinary retention is most likely to occur shortly after initiation of therapy [Afonso et al. 2011; Stephenson et al. 2011], such urinary adverse events may have contributed to early withdrawal of susceptible patients from the UPLIFT study.
As with urinary retention, ‘depletion of susceptibles’ may potentially be pertinent to the analysis of cardiovascular data. There may be a reduced likelihood of detecting an association between the drug and MI in long-term trials if patients who experience drug-related angina and palpitations (and who may subsequently go on to develop MI) are withdrawn early from the study [Hammad et al. 2011]. The incidence rate of angina as a serious adverse event was 0.51 per 100 patient-years with tiotropium compared with 0.36 per 100 patient-years with placebo in the UPLIFT study, giving a RR of 1.44 (95% CI 0.91–2.26) [Tashkin et al. 2008]. In the meta-analysis by Rodrigo and colleagues, reversal of direction of effect for major adverse cardiac events was seen when UPLIFT was excluded in the sensitivity analysis [Rodrigo et al. 2009]. The FDA also described an excess risk of stroke with tiotropium in a pooled analysis of 29 trials [FDA, 2008] but this was not subsequently confirmed in UPLIFT [Tashkin et al. 2008]. Hence, there is a need to explore a wide variety of methodological factors and differences in patient populations between long-term and short-term trials that can subsequently cause heterogeneity in estimates of harm.
The underlying pharmacological principles also merit discussion. The significant association with acute urinary retention is an indication of systemic absorption of tiotropium. It is possible that tiotropium Respimat, with its more efficient delivery, has reached the tipping point and led to drug concentrations that are up on the slippery vertically oriented slope of the sigmoid dose–response curve for toxicity. In contrast, tiotropium HandiHaler may be delivering levels closer to the lower horizontal sloping end of the curve, thus potentially giving rise to adverse effects in a less consistent manner, and perhaps affecting only certain susceptible people. Older patients with multiple comorbidities (including cardiac conditions, and renal impairment with decreased clearance of tiotropium) may be more sensitive to toxicity from a small increase in tiotropium delivery via the Respimat device. A number of experts have expressed their opinion that there is no rationale for continued use of the Respimat device given the absence of evidence for superior efficacy [Ram et al. 2011] and the signal of increased mortality compared with the HandiHaler formulation [Cates, 2011; Ram, 2011].
Conclusions
Recent evidence indicates a plausible association between initiation of tiotropium and acute urinary retention. True to the predictions made 20 years ago, the risk seems most apparent in men with benign prostatic hyperplasia. Hence, it would be sensible (when possible) to consider alternatives to tiotropium in susceptible patients, or to warn patients about the risk and to be alert for any symptoms that emerge soon after starting on inhaled anticholinergics.
The situation with cardiovascular and mortality data is more complex and cannot be simply summarized with any certainty in absolute terms. When faced with conflicting, divergent data from different centres in the same trial, Horwitz and colleagues posed the question ‘Can treatment that is helpful on average be harmful to some patients?’ [Horwitz et al. 1996] and we believe that this may well apply to the current position with tiotropium. Instead of persisting with the heated debate and attempting to arrive at value judgements of ‘definitely safe’ or ‘definitely unsafe’, it would be far more helpful to think about dose-related gradations of risk that are in line with the continuum of a sigmoid curve, and to identify dose-relatedness and susceptibility factors (e.g. nature of underlying cardiac disorder or renal impairment with potentially reduced clearance of tiotropium) so that any potential risks can be minimized. In particular, it would be prudent to avoid use of tiotropium in patients with a history of palpitations or documented cardiac rhythm abnormalities, as well as those known to have angina or previous acute coronary syndrome. Finally, the pharmacokinetics of tiotropium through the Respimat device should be studied in much larger trials, in comparison to tiotropium through the HandiHaler device and also to placebo with rigorous electrocardiographic monitoring.
Footnotes
SS is supported by NCRR (grant number 1KL2RR025006-03), a component of the NIH, and NIH Roadmap for Medical Research. The article’s contents are solely the responsibility of the authors and do not necessarily represent the official view of NCRR or NIH. The design and conduct of the study; collection, management, analysis, and interpretation of the data; and preparation, review, or approval of the manuscript was independent of any sources of funding.
The authors declare no conflict of interest in preparing this manuscript.