
Abstract
The use of antithrombotic medicines in patients who have a history of intracerebral haemorrhage is widely perceived as being contraindicated. However, many patients with intracerebral haemorrhage may suffer from conditions for which antithrombotic medicines are indicated. Such scenarios represent a therapeutic dilemma whereby treating infers an increased risk of recurrent intracerebral haemorrhage, but not treating infers an increase of thrombotic complications. Despite the importance of this dilemma, there is very little guidance for prescribers. This perspective review considered previous systematic reviews that addressed this issue, together with recently published research findings from the Tayside Stroke Cohort. Systematic reviews of experimental and observational studies have concluded that there is a marked lack of data on which to judge the safety of oral anticoagulant agents following intracerebral haemorrhage. In addition, the limited data available regarding the use of antiplatelet medicines following intracerebral haemorrhage provide no evidence that they are harmful, and again further data are required. In the absence of such data, a decision analysis approach has been proposed. This considers the findings of other studies to infer the likely impact of using antithrombotic agents in patients with intracerebral haemorrhage. The success of this approach is contingent on the availability of reliable data that describe the rate of recurrent intracerebral haemorrhage; however, published data on this varies widely. There are a number of factors that conspire against researchers addressing this issue. The current paucity of evidence to guide prescribers faced with this therapeutic dilemma seems likely to remain for some time.
Keywords
Background
The use of antithrombotic medicines in patients who have a history of intracerebral haemorrhage is widely perceived as being contraindicated [Wani et al. 2005]. However, many patients with intracerebral haemorrhage have comorbidities for which antithrombotic medicines are indicated. This may take different forms: for example, a patient being treated with warfarin indicated because of a prosthetic heart valve, subsequently sustaining an intracerebral haemorrhage with an international normalized ratio (INR) within the therapeutic range. Alternatively, a patient with a history of primary intracerebral haemorrhage may suffer a myocardial infarction and thus be indicated for antiplatelet medication. Both scenarios represent a therapeutic dilemma whereby treating infers an increased risk of recurrent intracerebral haemorrhage, but not treating infers an increase of thrombotic complications. Despite this, there is very little guidance for prescribers wishing to know whether it is beneficial to prescribe long-term antithrombotic agents [Scottish Intercollegiate Guidelines Network, 2008; Broderick et al. 2007].
Evidence relating to antithrombotic use following intracerebral haemorrhage
Randomized controlled trials
A systematic review of randomized controlled trials revealed very little data addressing the issue of antithrombotic use following intracerebral haemorrhage [Wardlaw et al. 2004]. Only short-term trials were found including two in which patients with presumed cerebral infarction were ‘mistakenly’ prescribed aspirin with therapy stopped following diagnosis of intracerebral haemorrhage, and one smaller trial in which patients were randomized to receive a short course of heparin following hospitalisation for intracerebral haemorrhage. The authors of this systematic review concluded that the wide confidence intervals ruled out neither modest harm nor moderate benefit.
Observational studies
Antiplatelet medicines
Comparison of observational studies considering antiplatelet (AP) medicine use following ICH [Flynn et al. 2010b].
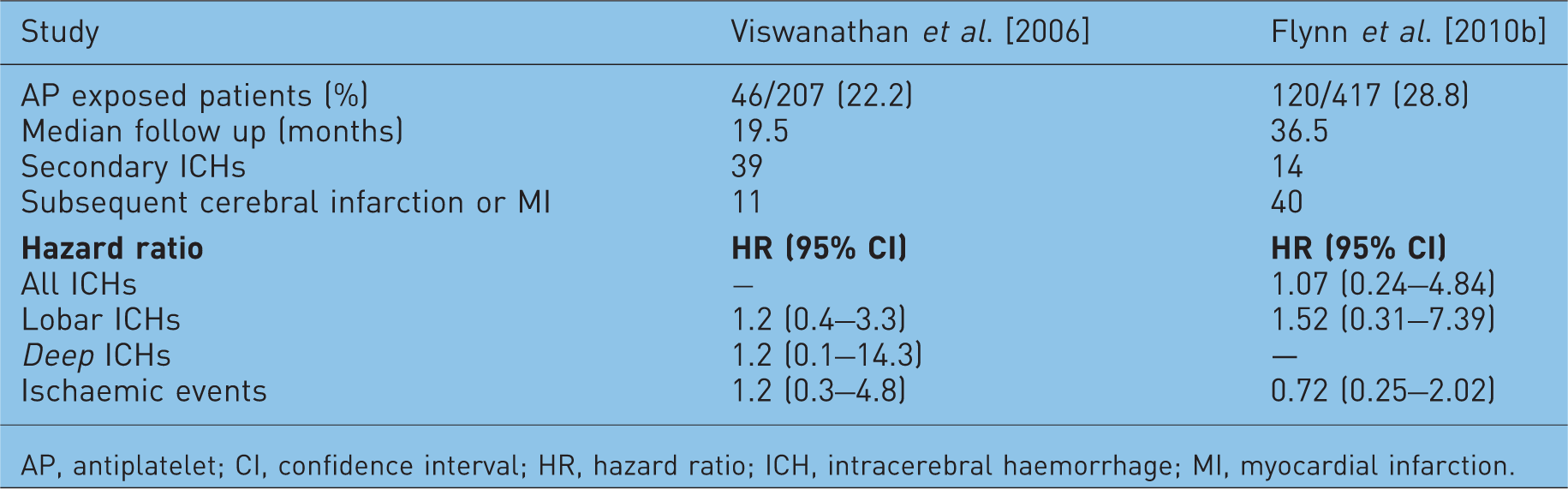
AP, antiplatelet; CI, confidence interval; HR, hazard ratio; ICH, intracerebral haemorrhage; MI, myocardial infarction.
Since the publication of this review, we have conducted our own observational study also addressing this issue [Flynn et al. 2010b]. This study used data from the Tayside Stroke Cohort [Flynn et al. 2010c], a derived cohort of stroke patients with an accurate diagnosis and good case ascertainment [Flynn et al. 2010d] record linked to primary care prescribing data. The data from this study is also shown in Table 1. Although our study and that of Viswanathan and colleagues used different methodologies, the risk estimates for recurrent and secondary events associated with antiplatelet use were similar. However, although these relative risks were similar, the absolute risk of recurrent intracerebral haemorrhage and subsequent ischaemia differed markedly between the two studies, a finding without a clear explanation (see the further comment below). We concluded in our study that there was no conclusive evidence that antiplatelet agents are harmful in patients who had previously experienced an intracerebral haemorrhage, but that further data are required.
Oral anticoagulation
The potential use of oral anticoagulants following intracerebral haemorrhage is a more troubling issue: whilst the need for anticoagulant protection is generally much greater than the need for antiplatelet therapy [Ohira et al. 2006], the risk of haemorrhage is also perceived as being much greater in anticoagulated patients [Wani et al. 2005]. Not treating implies a high risk of potentially fatal thromboembolism, whilst treating implies a high risk of recurrent intracerebral haemorrhage. The observational evidence addressing this issue comes from one epidemiological study and six case series with a total of just 42 patients in studies which followed up for at least 6 months [Flynn et al. 2010a]. Amongst these there were four recurrent intracerebral bleeds and nine thrombocculsive events. We concluded that there was a marked lack of data from both randomized controlled trials and observational studies on which to judge the safety of anticoagulants following intracerebral haemorrhage.
Data taken from the Tayside Stroke Cohort added little to the available numbers for study [Flynn et al. 2010b]. Of 417 initial intracerebral haemorrhage long-term survivors, 15 received subsequent oral anticoagulants during a follow up of 43.2 patient years. There were no recurrent intracerebral haemorrhages (rate 0.0 per 1000 patient years; 95% confidence interval [CI] 0.0–85.4), and one subsequent ischaemic event (rate 23.1 per 1000 person years; 95% CI 0.6–128.9).
A decision analysis approach
In the absence of sufficient experimental or observational studies, a decision analysis approach in relation to anticoagulation was published by Eckman and colleagues [Eckman et al. 2003]. This has been widely cited and apparently influential in the formulation of practice guidelines [Scottish Intercollegiate Guidelines Network, 2008; Broderick et al. 2007] and expert opinions [Aguilar et al. 2007] on the use of warfarin following intracerebral haemorrhage. This approach used existing data to infer the likely impact of reintroducing warfarin to a patient with atrial fibrillation who has suffered an intracerebral haemorrhage. The study used a Markov state transition model to analyse decision trees and carry out sensitivity analyses. By considering the balance between the competing risks and the likely outcomes of implementing different treatment strategies, this represented a rational approach to the question ‘Can a patient be anticoagulated after intracerebral haemorrhage?’. The aim is to arrive at the optimum decision by considering the possible contingencies arising when different decisions are made. This is the ‘benefits versus risks’ approach that is advocated in some guidelines.
The decision model considered a hypothetical 69-year-old man with newly diagnosed atrial fibrillation and history of intracerebral haemorrhage. The patient’s risks of thrombotic and haemorrhagic outcomes were considered both ‘on’ and ‘off’ warfarin. A range of likely outcomes were considered (for example, the patient suffers long-term morbidity post-intracerebral haemorrhage, patient suffers short-term morbidity post-intracerebral haemorrhage, patients dies following embolus, symptoms resolve, etc.), with the decision-tree structure considering 28 states of health (see Eckman et al. [2003] for more details). Much of the required data came from existing published systematic reviews and meta-analyses; however, many data were also extrapolated from previous studies, taken from the authors’ own prospective cohort of 435 consecutive intracerebral haemorrhage patients, or were assumed. To test the impact of assumptions made, a detailed sensitivity analysis of all of the factors was conducted by the authors. These revealed whether the findings of the study held true for a range of values and also gave ‘threshold’ values at which the decision of whether to treat would be altered. Separate consideration was given to intracerebral haemorrhages whose origins were ‘lobar’ (frontal, parietal, temporal or occipital) or ‘deep’ hemispheric (thalamus or basal ganglia) brain regions as these together account for over 80% of all haemorrhagic strokes. The authors concluded for both lobar and deep intracerebral haemorrhages, withholding anticoagulation therapy improved quality-adjusted life expectancy. However, in the case of a deep intracerebral haemorrhage the balance could be tipped in favour of treatment where there was higher risk of thromboembolic stroke. Of particular interest are the range of sensitivities that were tested for recurrent bleeding for both deep and lobar haemorrhages, from 0 to 0.2 events per year (0 to 200 per 1000 patient years), and threshold rebleeding rate below which anticoagulation would be considered beneficial of 0.014 per year (14 per 1000 patient years). Clearly estimates of recurrent event rates taken from the literature and the nature of other assumptions can have a profound impact on the outcome and validity of the decision analysis methodology. Some specific concerns are discussed below.
Rates of recurrent haemorrhage
Rates of recurrent intracerebral haemorrhage (ICH) taken from a variety of difference sources.
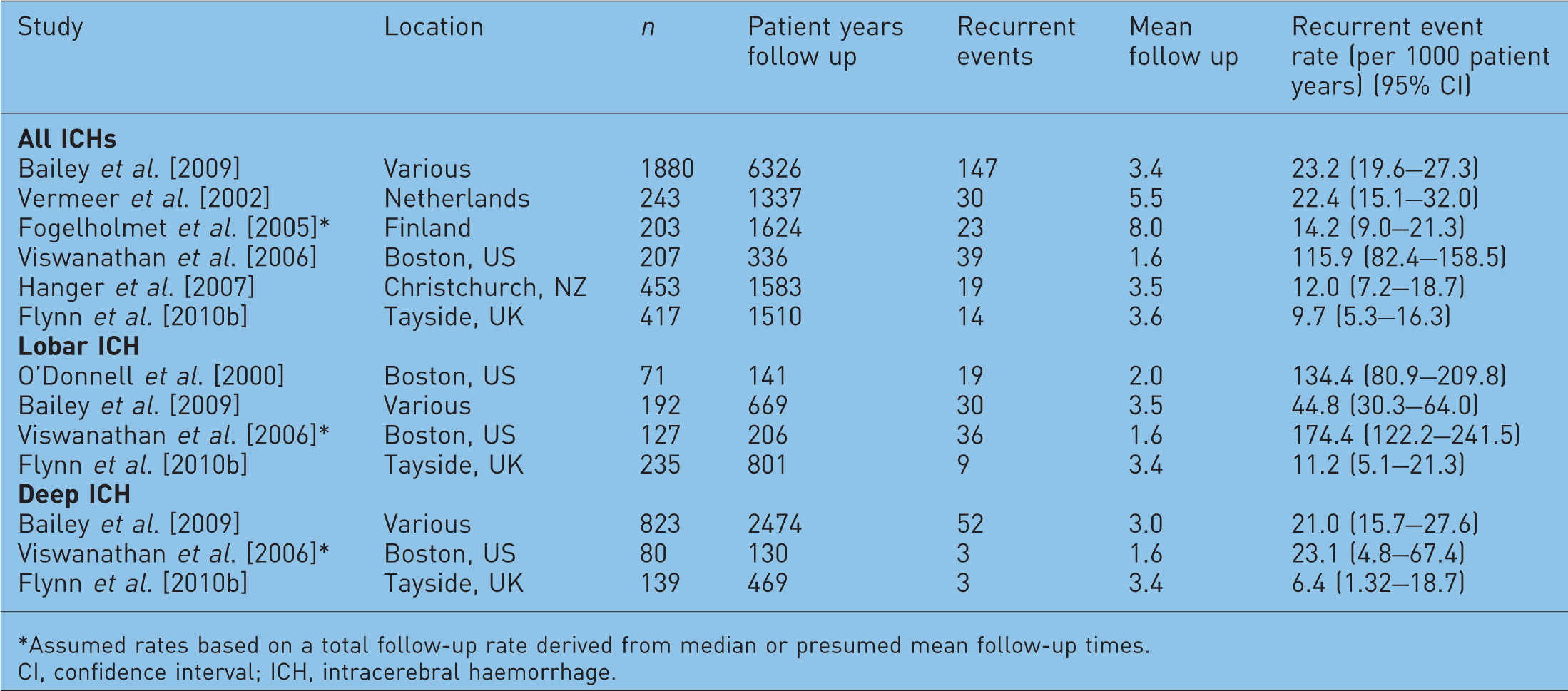
Assumed rates based on a total follow-up rate derived from median or presumed mean follow-up times.
CI, confidence interval; ICH, intracerebral haemorrhage.
The factors underlying the wide variation in recurrent events rates observed between different populations are not clear. This variation may be attributed to case ascertainment bias with our cohort of patients being defined by hospital admissions or deaths, and therefore comprising cases of symptomatic intracerebral haemorrhage, whilst other studies may have employed proactive follow-up imaging likely to detect asymptomatic bleeds [Wani et al. 2005]. As has previously been pointed out, the research group responsible for both the paper by Eckman and colleagues and the antiplatelet use following intracerebral haemorrhage study by Viswanathan and colleagues [Viswanathan et al. 2006] are based at the same tertiary referral centre, which has a special research interest in cerebral amyloid angiopathy [Alberts, 2006]. This condition increases risk of recurrent haemorrhage, and it could be that their study cohort is overrepresented by such patients. Differences may also be due to the different background population, with ours being a truly population-based study, whilst others have been based in secondary care referral centres. Alternatively there may be an actual difference in the underlying rates of recurrent intracerebral haemorrhage in different populations and different localities: it is well established that there is a substantial variation in the rate of first intracerebral haemorrhage amongst different ethnic groups, with higher incidences and mortality amongst non-White ethnic groups [Rosamond et al. 2007], and intracerebral haemorrhages accounting for a higher proportion of all strokes in Asian populations [Sacco et al. 1994].
Finally, other clinical factors may be involved. Blood pressure is the principal modifiable risk factor for intracerebral haemorrhage and blood pressure management varies between localities and across time [Joint National Committee on Prevention, Detection, Evaluation and Treatment of High Blood Pressure, and National High Blood Pressure Eradication Program Coordinating Committee, 1997; Colhoun et al. 1998]. This could have an impact on rates of recurrence in populations with different levels or management of hypertension.
Other issues with the decision analysis approach
Other concerns regarding the decision analysis approach have been raised [Stollberger and Finsterer, 2003]. Secondary causes of intracerebral haemorrhage are not accounted for, such as vascular malformations, vasculitis, amyloid angiopathy, haemorrhages secondary to cerebral infarctions and traumas. Where such secondary causes have been identified and rectified, it would be quite rational to assume that the underlying problem no longer exists and that treatment with either oral anticoagulants or antiplatelet medicines could be started with impunity. It was also assumed that the site of the index event was predictive of the site of subsequent event. This also has been questioned [Stollberger and Finsterer, 2003], with one study of 243 patients finding that the site of initial event was not predictive of recurrence [Vermeer et al. 2002]. Further data are required to address this issue, particularly in view of the fact that differences in recurrence rate seem to be much greater between geographic regions than between brain regions (see Table 2). Similarly, little consideration was given in the decision analysis to the effect of other risk factors for thromboembolism. Factors such as hypertension, diabetes, hypercholesterolaemia and history of stroke or transient ischaemic attack could significantly impact on secondary events of this nature [Stollberger and Finsterer, 2003]. The decision-tree analysis made no account of these assuming a fixed rate of thromboembolism of 4.5% per year; however, in practice this could vary from 1.0% to 8.9% depending on the presence and management of these risk factors [Stollberger and Finsterer, 2003]. The results of the sensitivity analysis suggested that this could be an important consideration with treatment being preferred where the annual risk was above 7%. The analysis therefore fails to take into account the extent to which effective management of these additional risk factors impacts on thromboembolism. Given that hypertension is a risk factor for both intracerebral haemorrhage and cerebral infarction, it is hard to judge exactly how this would affect the risk–benefit balance. As can be seen in Table 1, for patients in Tayside, following an initial intracerebral haemorrhage there is a greater risk of cerebral infarction and myocardial infarction than recurrent intracranial haemorrhage.
In general, these criticisms are based around the fact that intracerebral haemorrhage is a multifactorial disease which is, through necessity, represented in simplistic terms in the analysis used. However, because of these criticisms and the uncertainty relating to the rates or recurrent intracerebral haemorrhage, the conclusions of the decision-tree analysis by Eckman and colleagues are questionable. This, however, does not invalidate the approach used. As has been stated above, the approach used by Eckman and colleagues is intuitive and represents a rationalisation of the process that is undertaken when physicians follow the much offered, but not precisely defined, advice of balancing the ‘risks’ against the ‘benefits’ of treatment [Broderick et al. 2007].
It is clear from the literature that there is a heterogeneity of expert opinion as to how such dilemmas should be addressed [Aguilar et al. 2007; Estol and Kase, 2003]. The underlying issue is that there is a marked paucity of randomized and observational data addressing the safety of antithrombotic medication following intracerebral haemorrhage and that there are issues with the intuitive inferred decision analysis approach.
Challenges when researching intracerebral haemorrhage
There are a number of factors that conspire against researchers addressing this particular issue. In our cohort a large number (52.4%) of the 979 patients with radiologically confirmed intracerebral haemorrhage did not survive to discharge [Flynn et al. 2010c]. Of the 417 patients who did survive to discharge, 5.9% were deceased within 3 months and a further 8.4% within 6 months. A smaller proportion of patients are either prematurely censored or suffer events which would bring about the completion of their follow up within a short period of time (5.5% within 3 months, 8.6% within 6 months). Such an attrition rate reduces the opportunity for patient exposure to antiplatelet medicines. This is even more true of the less widely used anticoagulant drug, warfarin. Patients with cogent indications for warfarin therapy will likely have been receiving it prior to the index event. These patients, already anticoagulated on admission, will have a high rate of short-term (predischarge) mortality [Sjalander et al. 2003], further depleting the pool of potential study subjects. The resulting cohort is then unlikely to be exposed to the medicines of interest because physicians are often reluctant to prescribe antiplatelet medication and warfarin to those patients that do survive [Aguilar et al. 2007]. The net result is that the number of surviving intracerebral haemorrhage patients exposed to antiplatelet medication is small and the number receiving anticoagulation is even smaller. To fully address this area of outstanding uncertainty using observational data, multiple data are required from multiple sources in multiple regions using different methodologies. Clearly the gold standard approach would be a well-designed randomized study, however obtaining ethical approval for such a study is likely to be challenging, especially without clear evidence of safety from observational studies. If this is forthcoming, the scarcity of suitable subjects combined with the practical challenges of consenting and following up such patients means it will be a long time before this question is adequately addressed in a randomized study, if ever. Approaches that balance the benefits and risk of therapy may need to be developed further.
Further development in the understanding of the pathophysiology of cerebral haemorrhage is also required to inform decision making. For example, there has been recent interest in the ability to detect cerebral microbleeds with associated efforts to determine their clinical implications. The concern is that the use of antithrombotic agents could be predictive of cerebral microbleeds, and that this in turn could increase risk of overt cerebral haemorrhage (with or without the presence of antithrombotics). Currently, there is a lack of consistent evidence as to whether the presence of cerebral microbleeds does predispose individuals to intracerebral haemorrhage [Cordonnier, 2011]. Some studies have found that lobar microbleeds are associated with subsequent intracerebral haemorrhage whilst others have found a greater risk of subsequent cerebral infarction [Thijs et al. 2010]. Further well-designed studies are required to address this issue. A previous reviewer concluded that observed associations between antithrombotic drugs and the presence of microbleeds are likely to be confounded, and that there is currently no evidence to contraindicate the use of antithombotics in patient with microbleeds [Cordonnier, 2011].
Conclusions
Until there is better evidence to guide prescribers, should patients with a history of intracerebral haemorrhage be given antithrombotic medicines? Not if they have unaddressed risk factors, for example uncontrolled hypertension. Not if they have anything other than an absolutely cogent indication for antiplatelet treatment (for example, a history of myocardial infarction) or anticoagulation (for example, the presence of a prosthetic heart valve). However, what is the advice in respect of a patient with such indications for whom other risk factors have been controlled? Our opinion, based on the limited information available at this time and on the knowledge gained whilst researching this issue, is that it would not be unreasonable to introduce such agents following recovery from the initial haemorrhage. In the meantime, the current paucity of evidence to guide those faced with this therapeutic dilemma seems likely to continue for some time. Prescribers will have to continue to balance the ‘benefits’ of treatment against the ‘risks’.
Footnotes
Funding
Robert Flynn’s fellowship was funded by Chief Scientist Office, Scottish Executive Health Department (fellowship grant number CZF/1/41).
Conflict of interest statement
The authors declare no conflict of interest in preparing this article.