
Abstract
The history of intervention trials of periconception folic acid with multivitamin and folic acid supplementation in women has shown a recent breakthrough in the primary prevention of structural birth defects, namely neural-tube defects and some other congenital abnormalities. Recently, some studies have demonstrated the efficacy of this new method in reducing congenital abnormalities with specific origin; for example, in the offspring of diabetic and epileptic mothers, and in pregnancy with high fever. The benefits and drawbacks of four possible uses of periconception folate/folic acid and multivitamin supplementation are discussed: we believe there has been a missed opportunity to implement this preventive approach in medical practice. The four methods are as follows: (i) dietary intake of folate and other vitamins, (ii) periconception folic acid/multivitamin supplementation, (iii) food fortification with folic acid, and (iv) the combination of oral contraceptives with 6S-5-methytetrahydrofolate (‘folate’).
Keywords
Historical background
The occurrence of neural-tube defects (NTDs) depends on maternal socio-economic status (i.e. low risk in the highest social class to an above-average risk in the lowest class) [Elwood et al. 1992]. Thus, Smithells and colleagues hypothesized that undernutrition could be the common factor in the origin of NTDs [Smithells et al. 1976]. As a result, the same group tested the effect of diet supplemented with a multivitamin containing 0.36 mg folic acid in the first intervention trial [Smithells et al. 1980]. Women who had given birth to one or more previous infants with NTDs were supplemented with this multivitamin during the periconception period while controls were recruited among similar women who were already pregnant without vitamin supplementation. The results of Smithells et al.'s study were published separately for the Yorkshire region of the UK [Smithells et al. 1989] and Northern Ireland [Nevin and Seller, 1990], and they reported a 91% and 83% reduction in NTD recurrence for the two areas, respectively.
However, their results were not accepted by some experts due to possible selection bias in their nonrandomized controlled trial (non-RCT). Thus, the Medical Research Council (MRC) in the UK [MRC Vitamin Study Research Group, 1991] organized a multicenter RCT (43% of participants came from Hungary). There were four supplementation groups: folic acid (4 mg), other vitamins, folic acid and other vitamins, and minerals as a control. The results of the MRC Vitamin Study showed that a pharmacological dose of folic acid 4 mg can reduce NTD recurrence by 71% compared with minerals (0.8% versus 4.3%; relative risk [RR] 0.29 with 95% confidence interval [CI] 0.12–0.71). Other vitamins were not associated with a significant reduction of NTD recurrence.
In addition, Tolarova reported a protective effect of a multivitamin plus folic acid (10 mg) together during the periconception period for the recurrence of cleft lip [Tolarova, 1982].
The periconception multivitamin supplementation was incorporated into the Hungarian Periconception Service (HPS) launched in 1984 [Czeizel, 1989]. (We prefer to use the term periconception instead of preconception because prenatal care usually begins in about the 8th to 12th week of pregnancy; thus, the most sensitive and vulnerable early period of foetal development from the third postconception week until the 8th week is omitted from medical health care; therefore, embryos are unprotected.) The HPS is a new faculty within the primary healthcare system which starts 3 months before planned pregnancy and continues for 3 months postconception. HPS includes information counselling, examinations and interventions performed by nurses trained for the HPS. The HPS consists of three steps:
Check up of reproductive health. In fact, it is a preconception screening for risk identification and assessment (e.g. couples with high genetic risk or females with sexually transmitted vaginal infections), and referral of couples or persons at high risk to appropriate secondary care. The 3-month preparation for conception. The preparation for conception is an appropriate period to stop smoking, alcohol drinking, and the use of narcotic and unnecessary drugs with hazard to germ cells and later the foetus. In addition, it is an optimal time to start periconception folic acid or multivitamin supplementation. The better protection of early pregnancy. Females are asked to visit the HPS immediately after the first missed menstrual period to confirm conception by a sensitive pregnancy test and ultrasound scanning. In addition, they are asked to continue the intake of folic acid or multivitamins, etc., and finally are referred to prenatal care clinics with the discharge summary of the HPS.
The HPS worked as a model to test its feasibility in the Department of Human Genetics and Teratology (Head: A.E. Czeizel), National Institute of Public Health, Budapest, between 1984 and 1989. Since 1990, the HPS has become a national network including 33 local centres under the coordination of the above department. There are three criteria for participation in the HPS: (i) no infertility, (ii) not currently pregnant, and (iii) voluntary participation.
A RCT of periconception folic-acid-containing multivitamin supplementation for the reduction of first occurrence of NTDs and cleft lip with or without cleft palate (CL ± CP) was performed in the participants of the HPS in the above department. Half of the participants were supplied with a micronutrient combination (the so-called ‘multivitamin’ containing 12 vitamins including folic acid 0.8 mg, B12 4.0 µg, B6 2.6 mg and B2 1.8 mg, four minerals and three trace elements), while the other half of participants were supplied by a placebo-like trace element combination, i.e. ‘no multivitamin’, randomly. The periconception use of this multivitamin was defined as at least 1 month before conception and at least 2 months after conception.
There were three major questions asked by the Hungarian RCT on the basis of the findings of the three earlier recurrence studies described above: (I)–(II) ‘Does a folic-acid-containing multivitamin reduce the risk of first occurrence of NTDs and CL ± CP?’ About 95% of women who deliver infants with NTD or CL ± CP have no previous NTD or CL ± CP pregnancies; thus, the prevention of their first occurrence would be a real public health success. (III) The pharmacological dose (4 and 10 mg) of folic acid used in previous recurrence trials may have some adverse effects; thus, it was necessary to evaluate the effect of a more physiological dose (1 mg or less) of folic acid. Thus, the efficacy of a multivitamin containing 0.8 mg folic acid was tested.
No NTDs occurred in the 2391 offspring of the multivitamin group, while 6 NTDs were found in the 2471 offspring of the no-multivitamin group (p = 0.01). Thus, the Hungarian RCT demonstrated that a multivitamin containing 0.8 mg folic acid prevented about 90% of the first occurrence of NTDs [Czeizel and Dudás, 1992]. However, there was no reduction in the first occurrence of CL ± CP, because of the 2391 offspring in the multivitamin group, 4 were affected with CL ± CP compared with 3 in the 2471 offspring of the no-multivitamin group.
The unexpected finding of the Hungarian RCT was a significant reduction in the total rate of major congenital abnormalities (CAs): 20.6 per 1000 informative offspring (live and still births, and elective termination of pregnancy after prenatal diagnosis of malformed foetuses) in the multivitamin and 40.6 per 1000 in the no-multivitamin group (RR 0.53; 95% CI 0.35–0.70). The detailed analysis of final data set, based on the personal medical examination in all children, indicated a significant reduction in urinary tract CAs (2 versus 9 children; RR 0.21; 95% CI 0.05–0.95) and cardiovascular CAs (10 versus 20; RR 0.42; 95% CI 0.19–0.98) in live-born babies in the multivitamin group compared with the no-multivitamin group [Czeizel, 1998, 1996, 1993]. There was also some but not significant reduction in the rate of congenital limb deficiencies (1 versus 5; RR 0.19; 95% CI 0.03–1.18) and pyloric stenosis (2 versus 8; RR 0.24; 95% CI 0.05-1.14) in the multivitamin group.
For ethical reasons, the Hungarian RCT could not be continued, thus a cohort controlled trial (CCT) was designed to collect more data regarding the potential preventive effect of this multivitamin for other CAs beyond NTDs [Czeizel et al. 2004]. All participants in the different centres of the HPS were supplied with the multivitamin containing 0.8 mg folic acid that had been used in the RCT, while women in the unsupplemented cohort were recruited at the 14th week of pregnancy without vitamin use from the regional prenatal care clinics of different HPS centres and they were matched to each pregnant woman of the supplemented cohort. The protective effect of this multivitamin for the reduction of NTD was confirmed in these 3056 ‘pairs’ (1 versus 9; odds ratio [OR] 0.11; 95% CI 0.01–0.91).
The rate of cardiovascular CAs was again significantly reduced (31 versus 50, OR 0.60; 95% CI 0.38-0.96) in the multivitamin supplemented cohort, explained mainly by the lower occurrence of ventricular septal defect (5 versus 19; OR 0.26; 95% CI 0.09–0.72) compared with the unsupplemented cohort. The CAs of the urinary tract did not show significant difference between supplemented and unsupplemented cohort (14 versus 19; OR 0.71; 95% CI 0.33–1.50), although stenosis of the pelvicureteric junction (2 versus 13; OR 0.19; 95% CI 0.04–0.86) was reduced within the obstructive CAs of the urinary tract. The rate of limb deficiencies and pyloric stenosis showed again a decreasing trend in the supplemented cohort, but there was no reduction in CL ± CP (2 versus 3).
However, a 30% reduction was found in the birth prevalence of cases with CL ± CP (OR 0.72; 95% CI 0.55–0.92) in another study based on the Hungarian Case–Control Surveillance of Congenital Abnormalities (HCCSCA) [Czeizel et al. 1999] after the use of high dose (in general 6 mg) of folic acid alone; thus, a dose-dependent preventive effect of folic acid for CL ± CP cannot be excluded.
The main topic of this review is the primary prevention of NTDs by folic acid though the partial prevention of cardiovascular CAs is more important from a clinical aspect because the birth prevalence of cardiovascular CA is 3.6-fold higher (10.2 per 1000) than the incidence of NTDs (2.8 per 1000) in Hungary and, at present, cardiovascular CAs are the major factor in CA-related infant mortality [Czeizel, 2008, 2011].
Later, the results of only one intervention trial were reported, which found that folic acid 0.4 mg was effective at preventing the first occurrence of NTDs in a Chinese–US study [Berry et al. 1999]. There was a 79% reduction in the risk of NTDs in areas with high rates of NTDs (with a population incidence of 6.5 per 1000 live births), while this reduction was 41% in areas with low NTD rates (with the population incidence of 0.8 per 1000 live births).
Many observational studies of folic-acid-containing multivitamins and folic acid have also been published, and a meta-analysis of the available data confirmed the prevention of NTDs and some other CAs [Goh et al. 2006]. However, the results of intervention trials have a higher quality (in general one compound is used, the dose and duration of treatment are known based on prospective medically recorded data, and the endpoint, e.g. NTDs, and other CAs were checked individually); therefore, only data from intervention trials on this subject have been summarized in this review.
Thus, the results of both intervention trials and observational studies have shown the primary prevention of NTDs by folic acid (both low dose, 0.4 mg, and high dose, 4.0 mg) or folic acid-containing multivitamins (containing 0.4–0.8 mg of folic acid). In addition, a reduction of some CAs, mainly cardiovascular CAs, has been found after folic-acid-containing multivitamin supplementation [Czeizel, 2009].
These studies have evaluated NTDs and other CAs in general populations without any specified origin. Obviously, CAs may be caused by special causes such as diabetes mellitus (DM) or epilepsy-related drugs; thus, in the next step of research the possible prevention of CAs with different specified origins, by folic acid alone or folic-acid-containing multivitamins, was studied.
Primary prevention of congenital abnormalities with specified origin
These studies were based on the large population-based HCCSCA 1980–1996 including 22,843 cases with different CAs and 38,151 matched controls without any CAs [Czeizel et al. 2001].
Folic acid use in the prevention of diabetic embryopathy
Maternal DM during pregnancy is associated with a higher risk of CAs in offspring [Moore, 2004]. The spectrum of DM-related ‘embryopathy’ includes both isolated CAs [Nielsen et al. 2005; Becerra et al. 1990; Molsted-Pederson et al. 1964] such as NTDs (mainly spina bifida) [Milunsky et al. 1982], cardiovascular CAs particularly transposition of great vessels, double outlet right ventricle, and common truncus [Loffredo et al. 2001; Ferencz et al. 1990], kidney CAs (renal a/dysgenesis), obstructive CAs of the urinary tract, congenital limb deficiency (mainly a/dysplasia of femoral head), CAs of the spines (mainly sacral agenesis) [Sheffield et al. 2002; Martinez-Frias et al. 1998; Rusnak and Driscoll, 1965] and a specific multiple CA, the so-called caudal dysplasia sequence comprising sacrolumbal vertebral defects with secondary dislocation of the hip and clubfoot, imperforate anus and renal agenesis [Passarge and Lenz, 1966; Kucera et al. 1965].
Three main types of DM are differentiated such as type 1 (DM-1) (previously also known as juvenile-onset DM or insulin-dependent DM [IDDM]); type 2 (previously also known as adult-onset DM or non-insulin-dependent DM [NIDDM]); and gestational DM. The study of Bánhidy and colleagues [Bánhidy et al. 2010a] was focused on pregnant women with DM-1 in the HCCSCA, and a 1.5-fold higher risk of CAs was found in the offspring of these pregnant women. However, the risk of CAs in the offspring of pregnant women with overt DM (frequently without the specification of DM type) prior to conception was fourfold to eightfold higher in the previous studies [Moore, 2004]. Thus, the study by Bánhidy and colleagues may reflect the recent progress in the specific medical care of diabetic pregnant women.
The objective of another study was to check whether the recently introduced periconception folic acid supplementation in Hungary may have contributed to the reduction of CAs in the offspring of pregnant women with DM-1 [Bánhidy et al. 2010b] because folic acid diminished diabetes-induced embryotoxicity in rats [Gareskog et al. 2006].
Of 22,843 cases with CAs, 79 (0.35%) had mothers with DM-1, while of 38,151 control newborns without CAs, 88 (0.23%) had mothers with DM-1 during the study pregnancy. In the next step, these pregnant women were differentiated with or without folic acid supplementation, because the objective of the study was to compare the incidence of different CAs in these two subgroups in order to estimate the possible protective effect of folic acid for these CAs. Of 79 diabetic case mothers, 40 (50.6%) had folic acid supplementation during the study pregnancy compared with 54 (61.4%) in 88 diabetic control mothers (OR 0.65; 95% CI 0.33–1.25). The average daily dose of folic acid was 3.3 mg.
Estimation of risk for different congenital abnormalities (CAs) in the offspring of pregnant women with type 1 diabetes mellitus (DM-1), with or without folic acid supplementation, by comparison of prevalence of DM-1 in the mothers of cases with CAs and in the mothers of controls without any CAs.
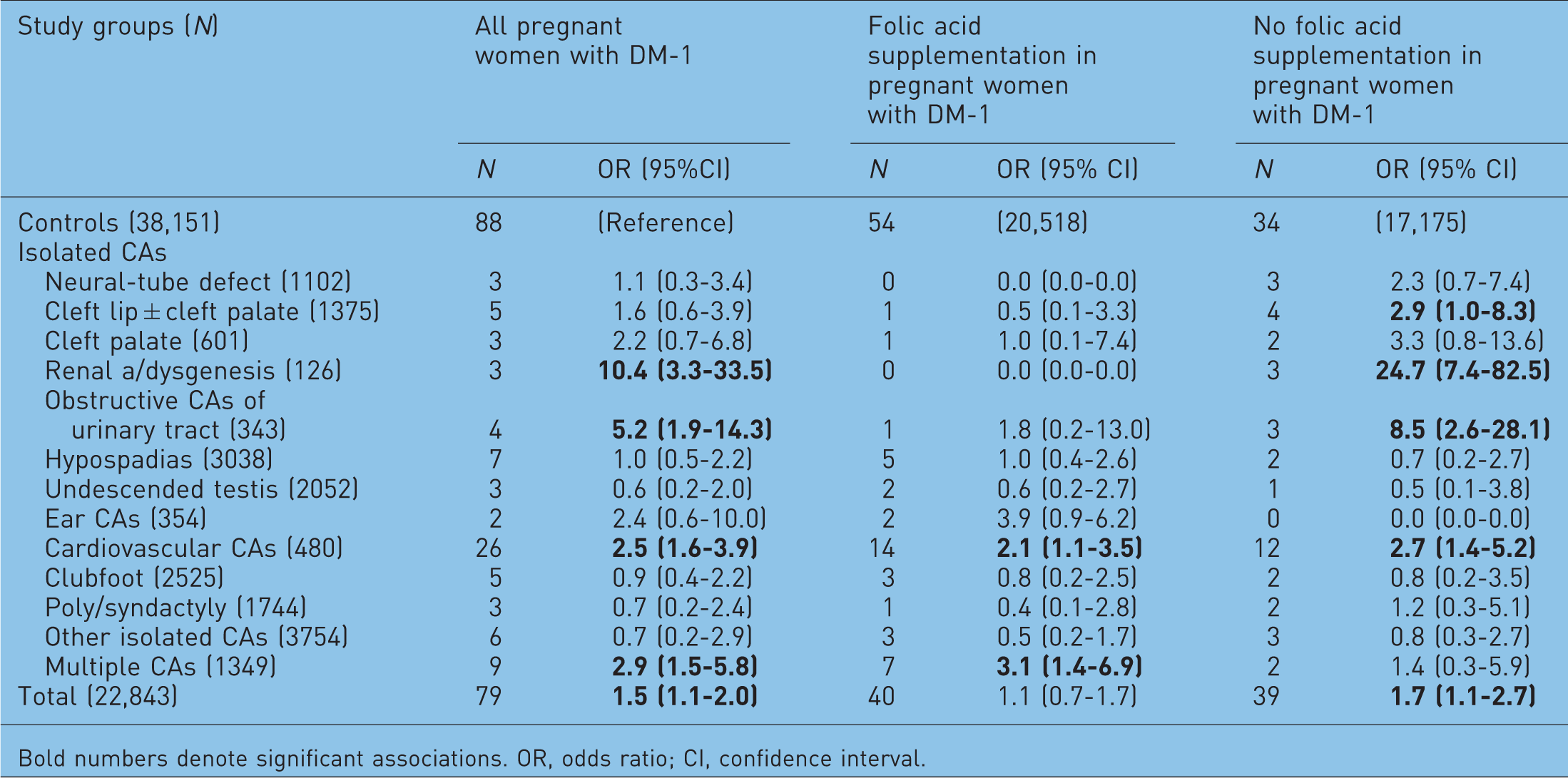
Bold numbers denote significant associations. OR, odds ratio; CI, confidence interval.
However, there was no higher risk of total CAs in the offspring of diabetic pregnant women with folic acid supplementation. NTDs and renal a/dysgenesis did not occur in these cases, and there was no higher risk of obstructive CAs of the urinary tract. However, the risk of cardiovascular CAs and multiple CAs has remained higher in the subgroup of diabetic pregnant women with folic acid supplementation.
On the other hand, the risk for total CA rate was significantly higher in the offspring of diabetic pregnant women without folic acid supplementation because there was no reduction in the rate of renal a/dysgenesis, obstructive CAs of urinary tract, CL ± CP and cardiovascular CAs.
Thus, folic acid seems to be protective for DM-1-related CAs, but the number of cases and controls was very limited in the study. In addition, only one third of these pregnant women with DM-1 started to use folic acid before conception, the onset of this supplementation was after the first visit in the prenatal care clinic between 7 and 10 gestational weeks in most pregnant women. The above beneficial effect therefore may be an indirect association with the higher socioeconomic status and better medical care of diabetic pregnant women. Nevertheless, it is worth checking the possible preventive effect of folic acid for DM-related CAs in other larger observational studies or intervention trials because folic acid may be a promising contributor to the further progress in the medical care of diabetic pregnant women to reduce the risk of adverse birth outcomes.
Folic acid use in epileptic pregnant women
Epilepsy is one of the most frequently studied maternal diseases during pregnancy because most epilepsies had an early onset therefore epilepsy occurs in 0.3–0.6% of pregnant women and their treatment with antiepileptic drugs (AEDs) is associated with the higher rate of CA syndromes (e.g. foetal hydantoin/dilantin/phenytoin and foetal valproate syndrome/effect), isolated CAs, and functional disturbances (e.g. mental retardation) in their children [Czeizel and Bánhidy, 2010]. The plasma level of AEDs needs to be controlled due to its decline during pregnancy: these examinations showed a decline in plasma folate level as well. Special preconception and antenatal care are very important for prospective epileptic pregnant women.
Estimation of the association between maternal epilepsy treated with antiepileptic drugs (AEDs) during pregnancy and different congenital abnormalities (CAs) on the basis of comparison of cases with different CAs and all matched controls without any CA.
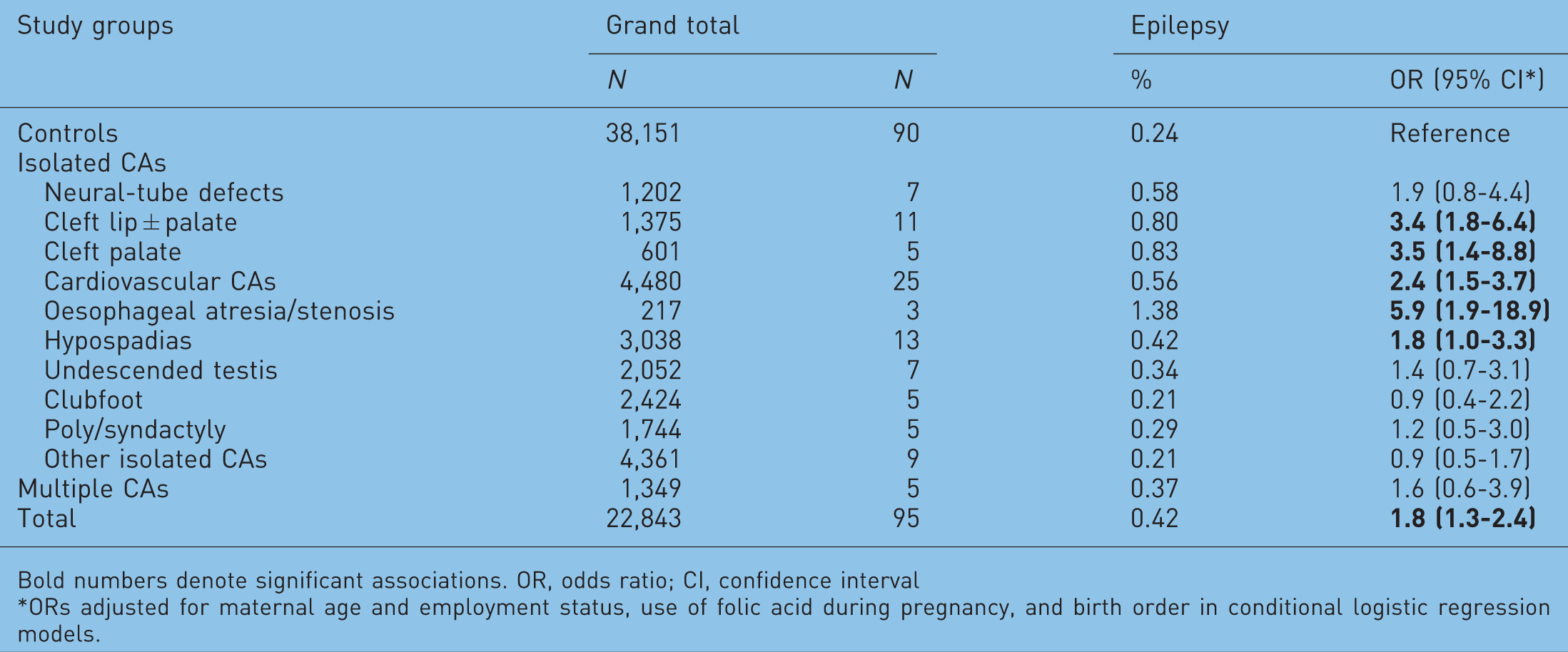
Bold numbers denote significant associations. OR, odds ratio; CI, confidence interval
ORs adjusted for maternal age and employment status, use of folic acid during pregnancy, and birth order in conditional logistic regression models.
Risk estimation of different congenital abnormalities (CAs) in epileptic pregnant women treated with antiepileptic drugs (AEDs), without or with folic acid supplementation [Kjaer et al. 2008].
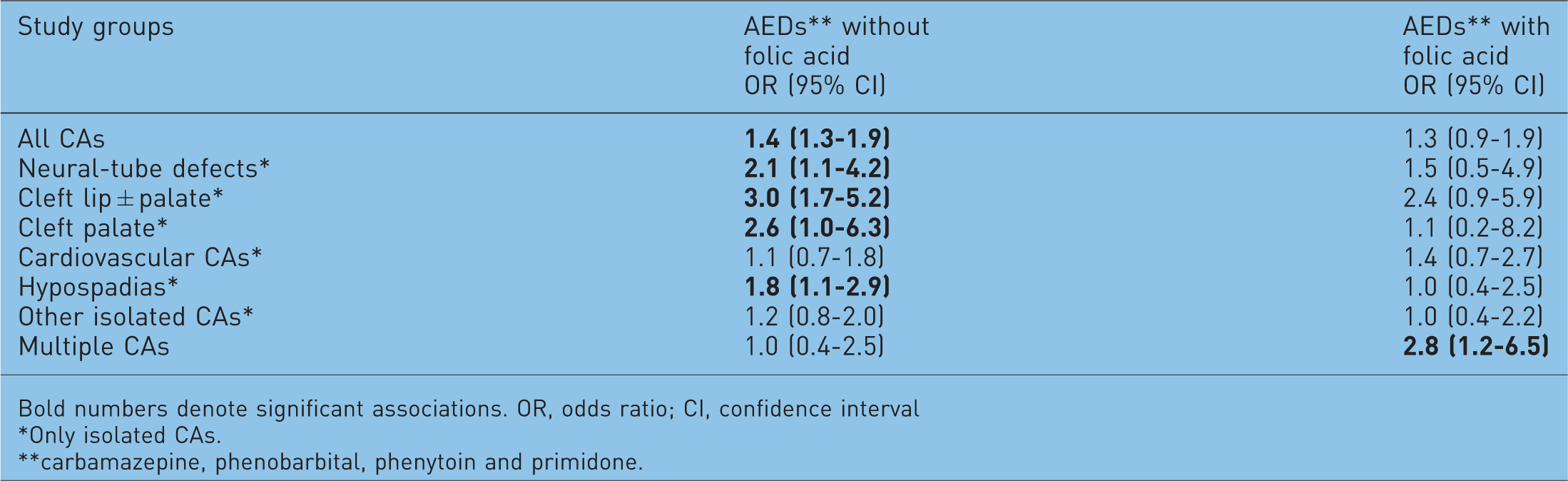
Bold numbers denote significant associations. OR, odds ratio; CI, confidence interval
Only isolated CAs.
carbamazepine, phenobarbital, phenytoin and primidone.
The aim of our recent analysis was to check the use of folic acid and folic-acid-containing multivitamins in the medical care of epileptic pregnant women in the data set of the HCCSCA, 1980–1996 [Bánhidy et al. 2010c]. All epileptic pregnant women with or without AEDs were recorded by obstetricians in the prenatal maternity logbook on the basis of their medical documents.
Frequency of folic acid and folic acid-containing multivitamin use by case and control mothers with epilepsy and without epilepsy as reference.

In conclusion, epileptic pregnant women, particularly epileptic case mothers used folic acid less frequently and at lower doses. Thus, the possible folic acid preventive effect for the teratogenic potential of some AEDs was utilized rarely. The explanation may be the previous contraindication of folic acid in epileptic pregnant women because the very high doses of folic acid acted as a convulsant in experimental animals [Erős et al. 1988]. However, Dansky and colleagues [Dansky et al. 1987] were not able to detect any change in the seizure rate of epileptic pregnant women using folic acid of 0.1–1.0 mg. In addition, there was no higher risk of seizure in epileptic pregnant women who participated in the Hungarian RCT and CCT trials of periconception folic acid (0.8 mg) containing multivitamin supplementation in Hungary [Erős et al. 1988]. On the other hand, the use of carbamazepine, phenytoin, primidone, and valproate reduces the folate level in plasma with increasing levels of AEDs [Wyllie, 2001] and there is evidence that folate deficiency is a well-known cause of NTDs and some other CAs.
Thus, our opinion is that the incorporation of folic acid would be beneficial for the care of pregnant women with epilepsy to reduce the teratogenic potential of some AEDs.
Reduction of the teratogenic potential of high fever by folic acid
The higher risk of some specific congenital abnormalities in the offspring of pregnant women with high-fever-related maternal diseases during the second and/or third gestational month, in addition the modification of these risks according to parallel folic acid use or without folic acid.

OR, odds ratio; CI, confidence interval. Bold numbers show significant associations.
Hyperthermia-induced CAs were detected first in animal investigations, but human evidence for the teratogenicity of high fever is now continuing to accumulate [Czeizel et al. 2007a]. The high-fever-related CA spectrum includes both isolated CAs such as NTDs, microcephaly, congenital cataract, microphthalmia, facial CAs such as micrognathia and midfacial hypoplasia, cleft palate, CL ± CP, anotia/microtia, cardiovascular CAs, limb deficiencies, neurogenic contractures, micropenis, and multiple CAs [Czeizel et al. 2007b]. Thus, a high-fever-related multiple CA syndrome (including two or more CAs) was delineated [Czeizel et al. 2008] on the basis of combination of NTDs, orofacial clefts, microcephaly, microphthalmia, anotia/microtia, arthrogryposis/neurogenic contracture, and indeterminate sex.
Thus, there is no doubt that temperature over 40°C has a teratogenic effect; however, the teratogenic effect threshold is very likely to be at 38.5°C, and one or more days seem to be the critical duration of hyperthermia. The timing of high fever during pregnancy is extremely important because its teratogenic risk depends on the critical period of specific CAs [Czeizel, 2008]. The most important experience is that high-fever-related CAs are preventable by specific (e.g. influenza vaccination) and general (antipyretic drugs) medical interventions. In addition, folic-acid-containing multivitamins and folic acid can also reduce the high-fever-related CA risk as the findings of Botto and colleagues showed [Botto et al. 2002, 2001]. Shaw and colleagues reported a 7.4-fold increased risk for NTDs in mothers with high fever who did not take folic-acid-containing multivitamins [Shaw et al. 1998]. The HCCSCA data [Czeizel atal. 2007a] also showed that folic acid/multivitamin supplementation can reduce and/or protect against the teratogenic effects of high fever in NTDs, CL ± CP and cleft palate (Table 5), but not all CAs. For example, periconception multivitamin/folic acid supplementation cannot reduce the high-fever-related risk of multiple CAs.
Our hope is that this historical review and the results of recent studies have shown that periconception multivitamin/folic acid supplementation may provide a breakthrough in the primary prevention of NTDs and some other CAs. However, the beneficial effect of this important new primary preventive method has not been routinely implemented in the medical practice.
Possible mechanisms of NTD and CA prevention by folic acid/multivitamins
The natural monoglutamate folate was discovered by Lucy Wills 80 years ago [Wills, 1931] and sherecommended using the term vitamin 11 as a ‘twin’ of vitamin B12. Later, the polyglutamate form of this vitamin, as folic acid, was produced [Hoffbrand, 2001]. Thus, we prefer to use the term vitamin 11 including natural monoglutamate folate and synthetic polyglutamate folic acid.
Humans cannot produce folate: the major dietary sources of folates are fresh and frozen green leafy vegetables, citrus fruits and juices, liver, wheat bread and legumes, such as beans. Thus, our requirement for this water-soluble vitamin is supplied partly by dietary intakes of folates and partly by the use of synthetic folic acid; thus, to estimate the necessary dose we have to add these two forms of this vitamin.
After dietary intake of monoglutamate folates and intentional supply of synthetic polyglutamate folic acid, the two forms of this vitamin are absorbed in the cells of the upper small intestine. Folic acid can be absorbed directly while folate is changed into the monoglutamate form by a conjugase enzyme. These monoglutamates are then converted into dihydrofolate and then into tetrahydrofolate (THF) by reductase enzymes. THF is the parent compound of all biologically active forms of this vitamin. THF is converted to 5,10-methylene-THF and 5-methylene-THF (5-MTHF) before transfer into the hepatic portal vein and the liver and onwards to the systematic blood circulation and all body tissues.
The plasma folate level to which cells of the foetus are exposed reflects the maternal intake of folate/folic acid in previous days and it decreases relatively quickly after discontinuation of folate/folic acid from the diet. In contrast, red blood cell folate level changes slowly within the 120-day life of erythrocytes and therefore shows a more constant characteristic level. However, the cells of the foetus are exposed to circulating plasma folate.
In recent years, a nature-identical folate of 5-MTHF, 6S-5-MTHF, has been synthesized as a calcium salt and it was marketed as Metafolin® [Wright et al. 2010]. Thus, 6S-5-MTHF is a synthetic product but equal to its natural form, thus the term folate is correct.
A polymorphism of genes with an important role in folate metabolism is associated with an increased risk of NTDs, i.e. mutations of the methyleneterahydrofolate-reductase (MTHFR) gene (C677T). About 10–12% of the European population are homozygous (TT) for this polymorphism and it is associated with an approximately 70% reduction in MTHFR enzyme activity. This lower enzyme activity reduces the production of 5-MTHF and increases plasma homocysteine levels, which causes a delay in the closure of neural-tube, i.e. NTD. If the mother is homozygous for this mutation, the risk of NTD is twofold, if both the mother and foetus are homozygous, the risk of NTD increased sixfold to sevenfold. About 40% of the European population (45% of the Hungarian people) is heterozygous (CT) which is associated with a slight increase in the risk of NTDs.
However, beyond folate/folic acid, vitamins B12, B2 and B6 are also important as cofactors in homosyteine–folate metabolism, and are thus involved in the origin of hyperhomocysteinemia [Czeizel, 2011]. The methyl group of 5-methyl-THF is used by methionine-synthase to recycle homocysteine back to methionine, and methionine-synthase is a vitamin B12 dependent enzyme. Vitamin B12 is important for DNA and RNA biosynthesis as well. These functions may explain why vitamin B12 deficiency is an independent factor in the origin of NTDs.
The conversion of homocysteine to cystathione by cystathione-synthase requires pyridoxine, i.e. vitamin B6 dependent enzyme. A disturbance in the above processes results in decreased homocysteine remethylation causing hyperhomocysteinemia and the shortage of methionine; therefore, cells are not able to methylate important compounds such as proteins, lipids and myelin.
MTHFR is a key factor in the neutralization of homocysteine and it is a vitamin B2 (riboflavin) dependent enzyme. The function of thermolabile MTHFR is impaired due to lack of riboflavin.
These factors explain that multivitamins containing folic acid, vitamin B12, vitamin B6 and vitamin B2 are more effective in the prevention of NTDs (about 90%) [Czeizel et al. 2004; Czeizel and Dudas, 1992; Smithells et al. 1989] than folic acid alone (about 70%) [Berry et al. 1999; MRC Vitamin Study Research Group, 1991]. In addition, we have evidence for the preventive effect of these multivitamins in cardiovascular CAs, CAs of the urinary tract and limb deficiencies [Goh et al. 2006; Czeizel, 1996], but we are not aware of evidence for the similar preventive effect of folic acid alone [Czeizel, 2008].
Practical application of folate/folic acid in the primary prevention of NTDs and some other CAs
There are four main ways to use folate/folic acid in the primary prevention of NTDs (and some other CAs) for women of childbearing age who are capable of becoming pregnant.
1. Consumption of a folate-rich and other vitamin-rich diet
The preconception period is an appropriate time to change dietary habits and to improve the lifestyle of prospective parents, particularly mothers due to their good compliance as they want to do their best to have a healthy baby. Thus, it is an important task to advise all women to start a folate-rich and other vitamin-rich diet from the preconception time onwards.
McPartin and colleagues suggested that the optimal daily intake of folate/folic acid in the preconception and postconception period is about 0.66 mg per day [McPartlin et al. 1993]. Thus, the recommended intake of folate/folic acid advised to a woman of childbearing age, who is sexually active, is 0.70 mg daily [Food Safety Authority of Ireland, 2006].
The average daily intake of folate is about 0.18–0.20 mg/day in Hungarian pregnant women [Czeizel and Susánszky, 1994] and this consumption is not significantly higher in other countries [UK Department of Health, 2000]. Thus, it is difficult to imagine an about 3.5-fold increase in folate intake every day in anticipation of conception through food alone, because it would require the consumption of 500 g raw spinach, 900 g boiled spinach or 900 g raw broccoli [Bower and Wald, 1995], i.e. about 15 servings of broccoli in each day. However, an extreme increase in the consumption of extra folate from natural food is relatively ineffective at increasing folate status [Cuskelly et al. 1996], and some part of dietary folate is lost through cooking and processing.
In conclusion, a diet rich in vitamins, particularly folate, is important in the prevention of NTDs and some other CAs, but cannot alone completely neutralize the genetic predisposition for these CAs.
2. Periconception folic acid supplementation
Good evidence is available to advise all women capable of becoming pregnant to have periconception (i.e. 2–3 months before and until 4 months after conception) folic acid or folic-acid-containing multivitamin supplementation to reduce the occurrence of NTDs and some other major CAs.
Periconception use of folic acid or multivitamins it would be a simple and useful approach; however, about 50% of pregnancies are unplanned in the United States, Hungary and many other industrialized countries. If women have unplanned pregnancies and are not using a supplement routinely, they cannot take advantage of this new primary preventive method during the preconception period.
There are two public health tasks to help prospective pregnant women in order to increase their use of folic acid or multivitamins during the preconception period. The first is a strong and widespread educational campaign to suggest the start of the use of folic acid or multivitamins immediately after the discontinuation of oral contraceptive pills or other contraceptive methods when couples decide to have a baby. However, unfortunately these campaigns have had only a limited success in all countries [Neville and de Walle, 2010; Busby et al. 2005; Botto et al. 2005].
The second important task is to establish a network of preconception or periconception care within primary healthcare [Healthy People USA, 2000]. As we mentioned previously, the HPS was launched in 1984 [Czeizel et al. 1998] and the Hungarian RCT and CCT (presented previously) were based on the HPS. Our Hungarian experience has shown that periconception care is feasible and economical, in addition to providing an appropriate opportunity for nutritional interventions [Czeizel et al. 2005].
Another problem is connected with the dose of folic acid. Based upon the Hungarian RCT and some observational studies, the CDC in 1992 recommended that ‘all women of childbearing age who are capable of becoming pregnant should consume 0.4 mg of folic acid per day for the purpose of reducing their risk of having a pregnancy affected with spina bifida or other NTD’ [CDC, 1992] and this recommendation was subsequently followed by several countries. However, at that time the recommended 0.4 mg folic acid per day was not based on scientific evidence, it was only later that the efficacy of 0.4 mg folic acid for the prevention of first occurrence of NTD was shown [Berry et al. 1999].
Daly and colleagues reported that the minimum effective dose of folic acid is 0.2 mg, this was previously the optimal daily intake of folate/folic acid in the preconception and postconception period to prevent NTDs [Daly et al. 1997]. They also reported that the lowest risk of having a child with NTDs was related to a red blood cell folate concentration of 906 nmol/l or more [Daly et al. 1993]. However, in clinical practice it would require 8–12 weeks to reach this concentration after the intake of previously recommended 0.4 mg folic acid supplementation, while the use of 0.8 mg folic acid resulted in necessary red blood cell folate concentration at 4.2 ± 3.5 weeks [Brämswig et al. 2009].
Thus, we recommend 1.0 mg of folate/folic acid daily for all preconception and pregnant women, by consumption of 0.2–0.3 mg folate through diet, and by supplementation of 0.7–0.8 mg folic acid [Czeizel and Bánhidy, 2011; US Preventive Service Task Force, 2009].
3. Food fortification
Food fortification seems to be the most practical means of supplementation with folic acid and other vitamins for women with unplanned pregnancies. This public health initiative is comparable to the prevention of goiter by the addition of iodine to salt.
In February 1996, the US Department of Health and Human Services ordered food fortification with folic acid of all cereal grain products at a level of 0.14 mg/100 g beginning January 1998 [US Department of Health and Human Services, 1996]. This adds only about 0.1 mg folic acid to the average daily diet of women of reproductive age; nevertheless, there was a 26% reduction in the total (birth + foetal) prevalence of NTDs [Williams et al. 2002; Honein et al. 2001]. The estimated benefit–cost ratio of US folic acid fortification is 40:1 [Grosse et al. 2005]; thus, the estimated economic benefit is US$312–425 million annually. Canada also introduced a mandatory flour fortification with folic acid (0.15 mg/100 g white flour) in September 1998 and a 42% reduction was found in the total prevalence of NTDs [De Wals et al. 2007], and a 6% reduction in the birth prevalence of cardiovascular CAs [Ionescu-Ittu et al. 2009]. Later, many others countries introduced mandatory flour fortification, and as far as we know, at present this public health project is ongoing in 57 countries. However, mandatory flour or other food fortifications are not available in European countries.
Mandatory flour fortification would be especially important for the large proportion of women with lower levels of education and income who, in general, have difficulties buying more expensive foods rich in folate and other vitamins and who have more frequently unplanned pregnancies.
Our major concern regarding food fortification is the low dose of folic acid used and the lack of vitamin B12 [Scott, 1999]. On the one hand, there is a well-known dose–effect relation in the preventive effect of folic acid for NTDs, which explains why some experts recommended the use of 5 mg folic acid [Koren and Goh, 2007; Wald et al. 2001]. In our opinion 0.8 mg is a good compromise. On the other hand, vitamin B12 is an independent risk factor in the origin of NTDs [Kirke et al. 1993], and the combination of folic acid and vitamin B12 can prevent the so-called ‘masking effect’ of folic acid in patients with pernicious anemia [Oakley, 1997]. This possible masking effect was the previous major concern regarding the use of folic acid, mainly higher doses, in the general population, particularly in some older people [Lindenbaum et al. 1988]. However, experiences of flour fortification with folic acid have shown that the incidence of megaloblastic anemia is reduced significantly without a higher manifestation of this masking effect.
Nevertheless, opinion on food fortification is polarized. Results of some studies have shown that folate deficiency is a precancerous state, but recent data have suggested the possible carcinogenic effect of high doses of folic acid as well. Thus, there may be a U-shaped risk of cancer connected with the doses of folic acid [Fenech, 2001]. Owing to this, some experts did not recommend the introduction of flour fortification by folic acid because it may be associated with risk in older people with precancerous lesions, e.g. in the colon [Osterhues et al. 2009]. The opposite opinion is based on the good experience of flour fortification in USA and Canada; thus, Oakley declared that inertia on folic acid fortification is a public health malpractice [Oakley, 2003].
4. Combination of oral contraceptives and folate
Periconception folic acid or folic-acid-containing multivitamin supplementation is a breakthrough in the primary prevention of NTDs and some other CAs. However, the use of this method depends on planned conception, and the proportion of females who prepare their conception is between only 30–75% in different countries. As was mentioned previously, educational campaigns have not been very successful in any country.
Thus, we have to do our best to find alternative approaches. Our view is that the optimal option would be to establish a national network of preconception clinics; however, the wider use of this new healthcare infrastructure needs a long time to implement.
Combining the oral contraceptive pill with folate is another option [Holzgreve, 2010]. Recently, the US FDA (Food and Drug Administration) has approved a new medicinal product comprising a contraceptive (drospirenone and ethinylestradiol) and folate (levomefolate calcium).
Four advantages can be expected from the use of combination of oral contraceptive pill with folate, as follows:
Overall between 30% and 50% of women between the ages of 15 and 49 take oral contraceptives in most Western European countries [Szarevsky, 2010]. Information on the beneficial effects of folic acid or folic-acid-containing multivitamins could be provided on the packet of this medicinal product. Thus, our hope is that the user of this kind of contraception will better understand that starting to take folic acid or multivitamins immediately after the discontinuation of oral contraceptive pills is necessary when couples decide to have a baby. A well-known fact is that the compliance of pill use is not perfect. For example, in one study only 42% of oral contraceptive users remembered to take their pill every day [Oakley et al. 1991]. Thus, inadvertent ‘accidental’ conception may occur in about 2% of women who use contraceptive pills; the parallel use of folate is therefore important for the prevention of foetal NTDs and some other CAs. Studies showed that 42% of women who discontinued pill use had no consultation with their healthcare provider [Rosenberg and Waugh, 1998]. In addition, about 60% of young females who used oral contraceptives and stopped in order to have their first pregnancy, had no connection with gynaecologists in Hungary [Czeizel et al. 1998]. Thus, they have a low chance to use folic acid/multivitamin. The European Active Surveillance Study (EURAS) evaluated 2000 women who stopped taking oral contraceptives in order to become pregnant [Cronin et al. 2009]: 31% were pregnant in the first month after the discontinuation of these pills, and 46% after 3 months. In another study, conception occurred within 2 months after the cessation of oral contraceptives use in 30–40% of all pregnancies and within 4 months in 50–60% [Dunson et al. 2004]. Thus, an important benefit for women who conceived soon after stopping combined contraceptive plus folate is that they have a higher blood folate level initially; but this declines with time. Also, plasma folate levels decrease faster than red cell folate levels following discontinuation [Baker et al. 2009], and it is the former that cells of the foetus are exposed to. This ‘post-use effect’ may be useful in general and in special maternal diseases such as in diabetic mothers and in epileptic women with AED treatment to reduce the teratogenic potential of these pathological conditions. At present, the use of 6S-5-MTHF seems to be better than folic acid from four aspects:
The polymorphism of MTHFR gene (C677T) is associated with an increased risk of NTDs. However, in contrast to folic acid, the plasma response of 6S-5-MTHF is not affected in women carrying the common TT variant of MTHFR genes [Prinz-Langenohl et al. 2009]. The previous major concern regarding the use of folic acid, mainly higher doses, was its possible masking effect in patients with pernicious anaemia; however, supplementation with 6S-5-MTHF cannot ‘mask’ the clinical signs and symptoms of anemia and therefore a B12 deficiency is more likely to be diagnosed and treated. 6S-5-MTHF may be associated with a reduced interaction with antifolate drugs that inhibit dihydrofolate reductase [Pietrzik et al. 2010]. 6S-5-MTHF and folic acid showed comparable physiological activity, bioavailability and absorption [Pietrzik et al. 2010]. Thus, the equimolar dose of 6S-5-MTHF appears to be at least as effective as folic acid in increasing maternal red blood cell folate concentration in women of childbearing age [Pietrzik et al. 2007; Lamers et al. 2006].
However, it is necessary to stress that human data of controlled epidemiological studies regarding the preventive effect of Metafolin® for NTD and other CAs are not available. At present, we can mention only the expected benefits of oral contraceptive and folate combination and it is difficult to estimate the possible unexpected risks. Thus, further data based on scientific evidence are needed to draw final conclusions regarding this new medicinal product for the primary prevention of NTDs and some other CAs.
Final conclusions
Before the 1960s, nearly all victims of NTDs had fatal outcomes. In the 1960s, physicians introduced very early complex surgical and medical management, and the lives of victims were saved in the majority of spina bifida cases. (Of course, anencephaly is lethal.) In the 1970s, the selective criteria of surgical intervention were introduced to reduce the production of multiple handicapped children.
In the 1980s, prenatal screening based on maternal serum alpha-fetoprotein (MS-AFP) and/or ultrasonography was introduced. In the low-risk populations, the detection rate (i.e. sensitivity) of MS-AFP testing for open spina bifida varies from 72% and 91% and the specificity from 96.2% to 98.7% [Canadian Task Force on the Periodic Health Examination, 1994]. This prenatal screening resulted in a significant drop in the birth of NTD foetuses (previously it was called ‘secondary prevention’, i.e. the prevention of the birth of babies with NTDs, but recently the representatives of the WHO and European Union’s expert groups have rejected the term prevention for this special form of euthanasia). This approach increased the number of pregnancy terminations and was associated with some psychological and somatic complications of pregnant women.
Finally, since the 1990s, we have had a chance to reduce the incidence of NTDs due to the intentional modification (supplementation) of the diet in the periconceptional period of the life. Now, periconceptional folic acid or folic-acid-containing multivitamin supplementation as a primary preventive method of NTDs offers an appropriate alternative with the same efficacy of the elective abortion of NTD foetuses.
Obviously, the primary prevention of NTDs and some other CAs is much better than the termination of pregnancy after the prenatal diagnosis of foetal defects from moral, medical (comparing the risk of pregnancy termination and folic acid/multivitamin supplementations), and financial (periconceptional folic acid/multivitamin supplementation is much cheaper than the combined method of prenatal diagnosis, mainly followed by pregnancy termination) aspects. Nevertheless, the reduced proportion of NTD births is explained in two thirds by elective abortion and only one third by folic acid/multivitamin supplementation.
Thus, we have to change medical practice and to widen the use of folic acid/multivitamin supplementation because the proper preparation for conception is the earliest and most effective method for the prevention of NTDs and some other CAs.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The authors declare no conflict of interest in the preparation of this article.