
Abstract
Background:
Pituitary apoplexy (PA) is a neuroendocrine emergency characterized by acute hemorrhage or infarction of a pituitary adenoma. While its initial presentation and management are well documented, data on recurrent PA remain scarce.
Objectives:
To determine the prevalence, clinical characteristics, and predictors of recurrent PA in a national cohort, and to contextualize findings through a structured review of the literature.
Design:
Multicenter retrospective cohort study complemented by a structured literature review.
Methods:
We analyzed 274 patients from the Spanish Pituitary Apoplexy Registry (2010–2023) with complete follow-up. Recurrent PA was defined as a new acute episode with radiological evidence of hemorrhage or infarction within a previously affected lesion. Clinical, radiological, and treatment-related variables were compared between recurrent and non-recurrent cases. A complementary literature review identified published reports of recurrence.
Results:
Recurrent PA occurred in 9 patients (3.3%), including 6 of 214 with nonfunctioning adenomas (2.8%) and 3 of 60 with functioning adenomas (5.0%). Compared with nonrecurrent cases, patients with recurrence had significantly larger tumors (median 35 vs 25 mm; p = 0.006), higher rates of cavernous sinus invasion (77.9% vs 37.3%; p = 0.006), and more frequent prior cabergoline therapy (33.3% vs 6.3%; p = 0.020). Median time to recurrence was 18 months (range, 2–108). The literature review identified 11 studies reporting recurrence rates of 2.6%–16.7%, with more consistent estimates (4%–9.6%) in larger series (n ⩾ 50). All recurrent cases showed a favorable clinical course and recovery.
Conclusion:
Recurrent PA is uncommon, affecting approximately 3% of patients with a prior apoplexy episode. Given the low frequency of recurrence, the associated factors identified should be interpreted cautiously and considered primarily hypothesis-generating. The second episode was not more severe than the initial event, and the long-term prognosis was favorable.
Trial registration:
Not applicable.
Plain language summary
Pituitary apoplexy is a sudden bleeding or infarction within a pituitary tumor that can cause headache, visual loss, and hormonal imbalance. Most patients experience this event only once in their lifetime, but in rare cases, it may happen again, this condition is called recurrent pituitary apoplexy. In this study, we analyzed nearly 300 patients from the Spanish Pituitary Apoplexy Registry, one of the largest series worldwide. Only 3% of patients had a second episode, and these recurrences were generally not more severe than the first. Recurrence was slightly more common in patients with larger or invasive tumors and in those previously treated with dopamine agonists, such as cabergoline. Overall, the study shows that recurrent pituitary apoplexy is very uncommon and that patients can be reassured about their favorable long-term prognosis. Continued follow-up is recommended, especially for those with residual or invasive tumors, but no specific additional monitoring is usually required.
Introduction
Pituitary apoplexy (PA) is an uncommon but potentially life-threatening clinical syndrome characterized by the acute onset of severe headache, visual impairment, ophthalmoplegia, and sometimes altered consciousness because of hemorrhage or infarction of a pituitary adenoma.1,2 Although PA has been the focus of several large case series and is recognized as a neuroendocrine emergency, data on recurrent apoplexy are extremely scarce.
Most available studies describe the clinical presentation of a single episode of PA,3,4 its management,5–7 and its short- and long-term outcomes,4,8 or tumor recurrence.9,10 In contrast, repeat apoplectic episodes have been reported only in isolated case reports and a limited number of small series. Early work by Maccagnan et al. 11 described two recurrent events within a prospective cohort of 12 patients, 1 among 7 managed conservatively and 1 among 5 who underwent surgery, both within 6 months of the first episode. Randeva et al. 12 later reported one rebleeding 2 years after initial decompressive surgery for apoplexy, in a cohort of 35 cases. More recently, Hosmann et al. 13 identified recurrent hemorrhage in 5.3% of surgically treated patients and highlighted cavernous sinus invasion and subtotal resection as major risk factors. Other contemporary reports, including the largest surgical series, have also described recurrences, but with discrepant results (2 of 50 patients, 4%) 14 and (11 of 115, 9.6%). 15 In aggregate, the existing literature for surgical cases suggests that recurrence rates range from 2% to 11%.
Despite these observations, the frequency in large series, in conservatively managed patients, and the clinical spectrum of recurrent PA remain poorly understood. The rarity of the condition and the lack of systematic follow-up in most cohorts limit firm conclusions. Importantly, recurrent PA may represent a distinct clinical entity. Its recognition has direct implications for surgical decision-making, postoperative surveillance, and counseling of patients regarding long-term risks.
To address this knowledge gap, we analyzed the national Spanish Pituitary Apoplexy Registry, which included 301 patients, of whom 274 met the inclusion criteria and had complete follow-up data. In this study, we describe the clinical features and outcomes of patients with recurrent PA, compare them with those without recurrence, and place our findings within the context of a structured review of the literature.
Patients and methods
Study design and population
This is a retrospective analysis of patients included in the Spanish Pituitary Apoplexy Registry, which collects nationwide data from tertiary centers on clinically and radiologically confirmed cases of PA. As of 2025, the registry comprises 301 patients diagnosed between 2010 and 2023. The database includes detailed information on demographic, clinical, biochemical, and radiological presentation, as well as therapeutic approach. 8 A total of 18 medical centers across Spain participated in the registry. A final version of the protocol was approved as a multicenter observational study by the ethics committee of the coordinating center, the Vall d’Hebron University Hospital (No. PR(AG)577-2021). The study followed the STROBE statement 16 and was conducted according to the mandates of the Declaration of Helsinki and good clinical practices. The patients’ confidential information was protected according to the Spanish national data protection law. For retrospective cases, the ethics committee waived the requirement for individual informed consent because of the use of anonymized data, whereas written informed consent was obtained from all patients with active follow-up.
From the 301 patients with clinically and radiologically confirmed PA included in our national registry, 8 data on recurrence were available for 274 patients, while 27 cases were excluded due to missing follow-up information (Figure 1).
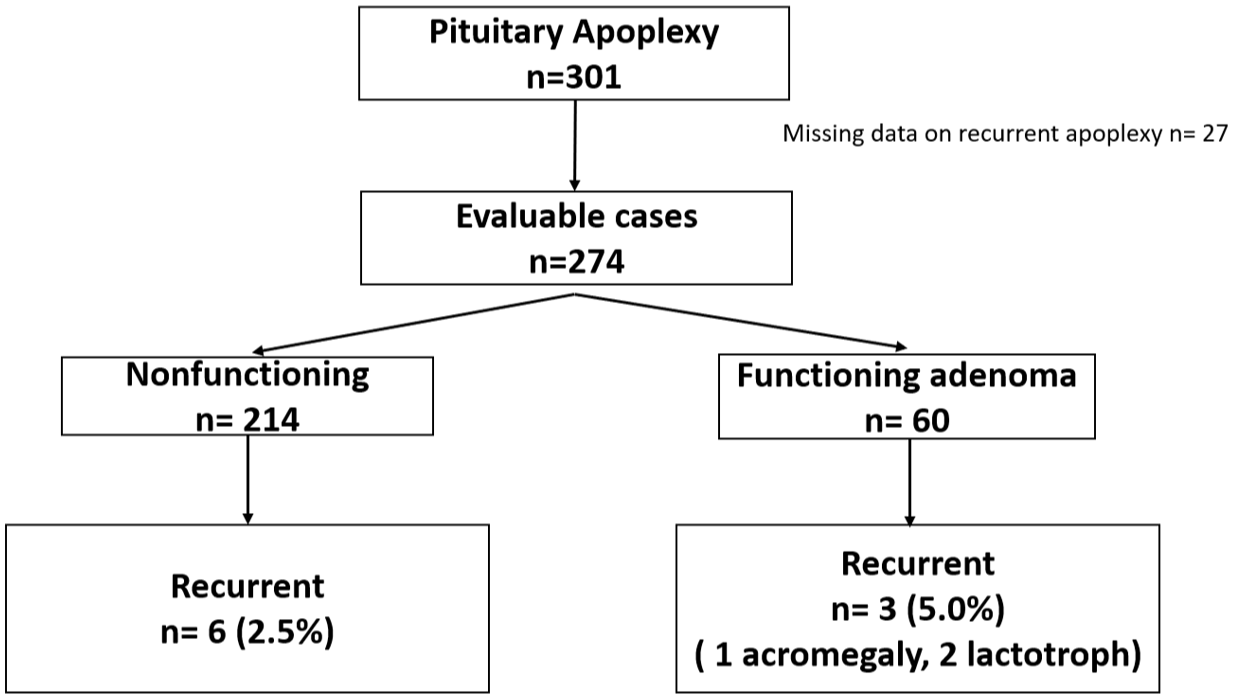
Distribution of recurrent pituitary apoplexy cases according to tumor functionality. Flowchart showing the number of patients included in the Spanish Pituitary Apoplexy Registry (n = 301). Data on recurrence were available in 274 patients. Recurrent apoplexy occurred in nine patients (3.3%): six with nonfunctioning adenomas (2.5%) and three with functioning adenomas (5.0%; one with acromegaly and two with prolactinomas).
Definition of recurrent PA
Recurrent PA was defined as a new acute clinical episode compatible with PA (sudden headache and/or visual or neurological deterioration) associated with radiological evidence of hemorrhage or infarction in a previously affected pituitary lesion or remnant. Patients with progressive tumor necrosis or postoperative hemorrhage within the first 30 days after surgery were not classified as recurrent PA.
Data collection and variables
Demographic information, clinical features, radiological findings, disease course, and management approach were retrieved from patients’ medical records. Magnetic resonance imaging (MRI) data were reviewed locally to characterize each tumor, assessing parameters such as maximal diameter, parasellar extension, optic chiasm compression, and Knosp grade, together with available biochemical and histopathological results.
Statistical analysis
Continuous variables are expressed as median and (interquartile range: Q1–Q3). Categorical variables are presented as frequencies and percentages. Comparisons between recurrent and nonrecurrent cases use Student’s t or Mann–Whitney U tests for continuous variables and χ2 or Fisher’s exact tests for categorical data. A p value <0.05 was considered statistically significant.
Because this was a retrospective analysis of a national registry, the sample size was determined by the total number of patients diagnosed with PA during the study period. Therefore, no a priori sample size calculation or power analysis was performed, as the registry includes all eligible cases with available follow-up data.
Literature review
A complementary literature review was conducted to identify all studies reporting recurrent PA. The search was performed in the PubMed and Web of Science databases using the terms “pituitary apoplexy” [Title] AND “recurrence” [All Fields], restricted to English-language publications between January 1995 and September 2025.
The search links accessed on September 30, 2025, were as follows:
Web of Science:
After merging both databases and removing duplicates, all titles and abstracts were screened. Only studies that explicitly reported recurrent or multiple apoplexy episodes in the same patient were included. Additional manual searching of the largest published PA series and their reference lists was also performed to ensure completeness.
All studies describing recurrent, multiple, or relapsing episodes of PA were considered eligible, including case reports, small series, and observational cohorts. The extracted information included study design, number of patients, recurrence rate, time, and clinical characteristics. Given the heterogeneity of study designs and the predominance of case reports and small series, data were summarized qualitatively, and no quantitative meta-analysis was performed.
Results
Among the 274 evaluable patients, 214 (78.1%) had non-functioning pituitary adenomas and 60 (21.9%) were functioning adenomas, including prolactinomas, somatotroph, and corticotroph adenomas.
Recurrent PA during follow-up was identified in 9 patients (3.3%): 6 of 214 with nonfunctioning adenomas (2.8%) and 3 of 60 with functioning adenomas (5.0%), of whom 1 with acromegaly and 2 with prolactinomas (Figure 1).
Table 1 summarizes the baseline demographic, radiological, and clinical characteristics according to the occurrence of recurrence. Male sex predominated in both groups, with no significant difference in distribution between recurrent and non-recurrent cases (88.9% vs 64.5%, p = 0.173). Median age at the first apoplexy was also comparable between groups (54.4 (50.3–64.9) vs 59.6 (46.2–69.2) years; p = 0.672).
Comparison of patients with and without recurrent pituitary apoplexy.
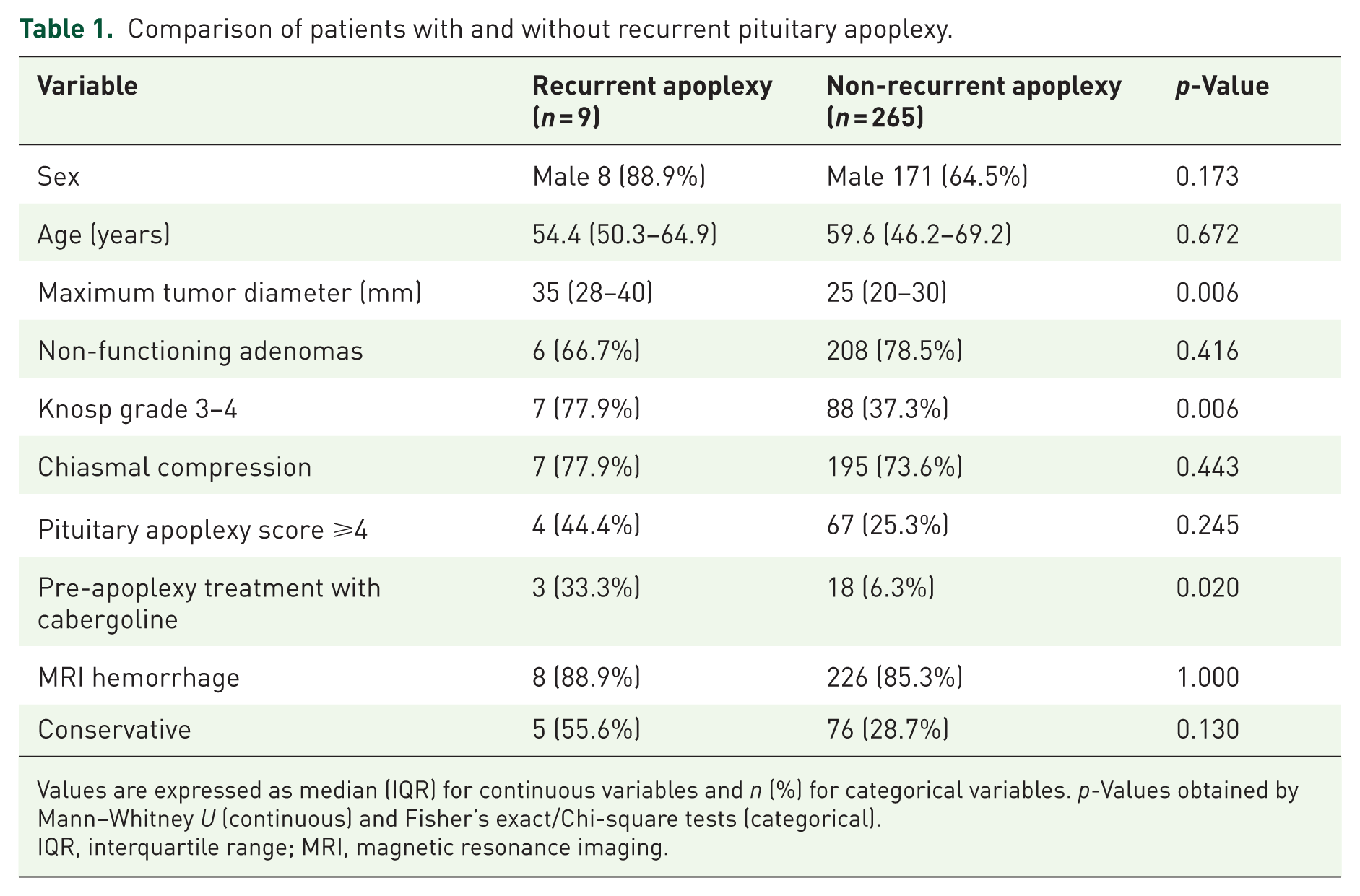
Values are expressed as median (IQR) for continuous variables and n (%) for categorical variables. p-Values obtained by Mann–Whitney U (continuous) and Fisher’s exact/Chi-square tests (categorical).
IQR, interquartile range; MRI, magnetic resonance imaging.
In contrast, patients who developed recurrence had larger tumors (median maximum diameter 35 (28–40) vs 25 (20–30) mm; p = 0.006) and a higher frequency of cavernous sinus invasion (Knosp grade 3–4 in 77.9% vs 37.3%; p = 0.006). The use of dopamine agonists was significantly associated with PA recurrence (33.3% vs 6.3%; p = 0.020).
No other significant differences were observed in tumor functionality, presence of chiasmal compression, Pituitary Apoplexy Score ⩾4, or MRI findings of hemorrhage or necrosis (all p > 0.05). Although conservative management was more frequent among patients with recurrent PA (55.6% vs 28.7% in non-recurrent cases), this difference did not reach statistical significance.
In our cohort, the median interval between the first and second PA episode was 18 months (range 2–108 months). Similarly, no significant differences were found in the prevalence of metabolic comorbidities, including diabetes mellitus, hypertension, or dyslipidemia, between the two groups.
All patients with recurrent PA had a favorable clinical course, with recovery comparable to that observed after the first event, and no deaths or permanent disabling sequelae were recorded.
Literature review
A structured literature review was performed to contextualize the recurrence rates observed in our national registry. The initial search identified 37 records in PubMed and 38 records in Web of Science (Figure 2). After merging both sources and removing duplicates, 49 unique records remained. Titles and abstracts were screened to exclude studies that did not report recurrent PA (e.g., single cases without recurrent apoplexy,17–21 a PA-like event, 22 tumor regrowth instead of a second hemorrhagic/ischemic apoplexy,10,23–25 pediatric series of apoplexy without PA recurrence, 26 or narrative reviews9,27 and guidelines 5 without individual recurrent cases). Full-text review yielded 11 studies that explicitly documented at least 1 case of clinically relevant recurrent PA; these were included in the qualitative synthesis (Table 2). Most publications consisted of isolated case reports or small case series, and only a few evaluated PA recurrence rates within larger cohorts of PA. Reported PA recurrence rates ranged from 2.6% to 16.7% across published series. Interestingly, the highest recurrence rates were observed in studies including fewer than 20 patients, such as those by Maccagnan et al. 11 and Açikgöz et al. 28
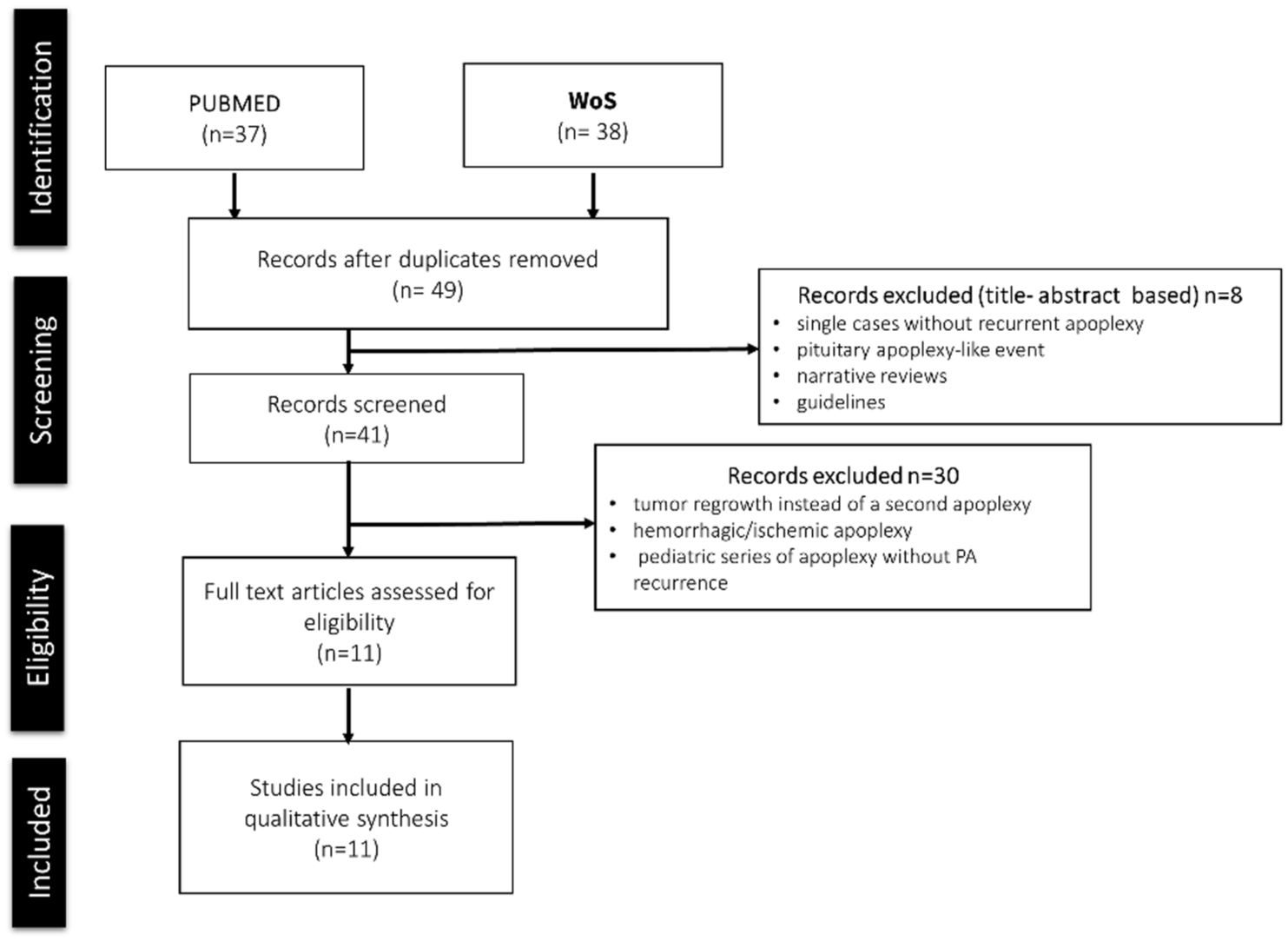
PRISMA-style flow diagram of the literature search and study selection process. PRISMA-style flow diagram illustrating the identification, screening, eligibility, and inclusion of studies reporting recurrent pituitary apoplexy. Due to the rarity of the condition and heterogeneity of study designs, a qualitative synthesis was performed.
Published series reporting recurrent PA.

PA, pituitary apoplexy.
The largest contemporary cohorts were those by Hosmann et al. 13 (76 patients; 5.3% recurrence) and Siu et al. 15 (115 patients; 9.6% recurrence). Both studies identified remnant tumor and cavernous sinus invasion as a key anatomical feature associated to rebleeding. Figure 3 summarizes recurrence rates reported across published series alongside the recurrence rate observed in our national registry, illustrating the wide variability in smaller case series and the more consistent rates observed in larger cohorts.

Recurrence rates of PA reported in published clinical series compared with the national Spanish Registry. Reported recurrence rates of PA in published series and in the Spanish Registry (2025). Values are expressed as the percentage of recurrence relative to the total number of described cases. Recurrence rates were higher in older studies with small case series while larger cohorts show more consistent recurrence rates between 3% and 10%.
Individual reports illustrated recurrence in more specific clinical contexts, such as pregnancy, 30 phenotypic transformation of adenomas, 31 or functioning tumors such as Cushing’s disease and acromegaly. 32
Across all reports, recurrent apoplexy was generally associated with macroadenomas, invasive growth, or previous medical or surgical treatment. No prospective study has yet systematically compared patients with and without recurrence.
The median time to recurrence among studies reporting this information ranged between approximately 4 and 5 years, although individual cases have described a second apoplexy occurring as early as 2 months 11 or as late as 13 years after the initial episode 31 : These findings highlights the need for continued long-term follow-up in all patients with pituitary macroadenomas, as is standard practice, while underlining that particular attention should be paid to those managed conservatively or with residual or invasive tumors, who may remain at higher risk of re-apoplexy.
Discussion
This multicenter study represents the largest real-world dataset evaluating recurrent PA to date. Within a national cohort of 274 well-characterized patients, the frequency of recurrence was 3.1%, which lies at the lower end of previously reported rates ranging from 2.6% to 16.7%. By combining population-based data with a structured literature review, our study provides an updated and comprehensive overview of recurrence risk and its potential determinants.
Previous publications on recurrent PA have been limited mainly to isolated case reports and small series, preventing generalizable conclusions. The increased percentage of recurrence rate in smaller series may suggest a potential selection or publication bias, whereby smaller or atypical series may overrepresent recurrent or more complex cases. As summarized in Table 2 and Figure 3, larger studies such as those by Siu et al. 15 Pangal et al., 14 and Hosmann et al. 13 were surgical series. They identified recurrence in approximately 4%–9% of patients, predominantly in the presence of cavernous sinus invasion or residual tumor after subtotal resection. Maccagnan et al., 11 found recurrence of PA developed in one patient conservatively managed 2 months after he had fully recovered from the first episode. These findings raised the possibility that conservative management might not fully prevent early re-apoplex. While in our series, there was a trend toward a higher proportion of conservatively managed patients in the recurrent apoplexy group (55.6% vs 29% in non-recurrent cases); this difference did not reach statistical significance.
Regarding the median interval between the first and second apoplexy in our study was 18 months (range 2–108 months). In previously published series, the median time to recurrence ranged between approximately 4 and 5 years, although individual case reports have described a second apoplexy occurring as early as 2 months 11 and as late as 13 years after the initial event. 31 These findings emphasize that long-term surveillance remains warranted.
In our series, recurrence was associated with larger tumor diameter, cavernous sinus invasion, and prior medical therapy with cabergoline, supporting the concept that residual or invasive macroadenomas remain at risk of repeated vascular events. The association with prior dopamine agonist treatment, both in prolactinomas or in non-functioning adenomas, raises the hypothesis that drug-induced intratumoral ischemia or fibrosis may predispose to subsequent hemorrhage, although causality cannot be established. Conversely, the absence of differences in Pituitary Apoplexy Score, hemorrhage type, or chiasmal compression suggests that recurrence may be more dependent on tumor biology than on the severity of the first episode.
Importantly, due to the low number of recurrent events, all associations observed should be considered exploratory. The observational nature of the study and limited event count do not allow causal inference or reliable adjustment for confounders. Therefore, these findings should not be interpreted as independent or causal risk factors, but as descriptive associations that may assist in clinical risk contextualization. Recognition of recurrent PA risk is relevant for follow-up strategies. While patients with large or invasive macroadenomas already require long-term imaging surveillance, awareness that re-apoplexy can occur (even if infrequently) may help refine clinical vigilance, particularly in those managed conservatively or with residual or cavernous sinus–invasive disease. With regard to cabergoline therapy, individualized risk–benefit assessment is warranted when initiating or continuing treatment, especially in non-functioning adenomas. Importantly, the rarity of recurrence supports a generally favorable long-term prognosis. Consistent with this, evidence from a large series by Iglesias et al., 34 including 142 surgically treated non-functioning adenomas (22 of whom received cabergoline for remnant control) reported no cases of PA during follow-up. Nevertheless, attentive monitoring remains advisable in higher-risk subgroups.
Limitations
As this is a registry-based study, no formal sample size calculation could be performed. The number of patients was determined by all consecutive cases diagnosed during the study period. Although this limits the ability to estimate statistical power for specific subgroup analyses, the large sample size and national multicenter design enhance the robustness and generalizability of the findings.
Conclusion
Recurrent PA is uncommon, occurring in approximately 3% of patients with confirmed apoplexy. Our analysis of 274 patients from a national registry, complemented by a structured literature review, identifies 3 key risk factors: larger tumor diameter (⩾35 mm), cavernous sinus invasion (Knosp grade 3–4), and prior treatment with cabergoline. However, given the overall low recurrence rate, these features should be interpreted as possible associations rather than definitive predictors of recurrence. Importantly, the second episodes were not more severe than the initial events, and most patients achieved favorable long-term outcomes. The association between dopamine agonist therapy and recurrence, observed in both prolactinomas and nonfunctioning adenomas, requires further investigation.
Footnotes
Acknowledgements
We thank all participating centers of the Spanish Pituitary Apoplexy Registry for their contribution to patient recruitment and data collection.
Author’s note
Betina Biagetti: On behalf of the Neuroendocrinology Task Force of the Spanish Society of Endocrinology.