
Abstract
Background:
Proper storage of insulin and accuracy of injection technique are essential for maintaining the effectiveness of insulin and optimizing glycemic control. In resource-poor countries like Ethiopia, poor storage conditions and incorrect injection techniques are prevalent, and hence, less than desired glycemic results are obtained. Interventional studies aimed at addressing these problems in Ethiopia are lacking.
Objectives:
This study aimed to evaluate the effect of an educational intervention on glycemic control, insulin storage behavior, and injection practices among diabetic patients at Debre Tabor Hospital.
Design:
A quasi-experimental pre- and post-intervention study design was employed.
Methods:
The study was conducted at Debre Tabor Hospital from January to June 2024. Baseline data on insulin storage, injection practices, and fasting blood glucose levels were collected using structured questionnaires and clinical records. The intervention was educational conferences with demonstrations and take-home materials on appropriate injection and storage practices. A follow-up after 3 months was carried out to determine changes in glycemic control and practice change. The intervention’s efficacy was determined by analyzing data using STATA version 17 with logistic regression and McNemar’s test.
Results:
There were 330 diabetic patients enrolled with a mean age of 42.87 ± 13.76 years, of which 59.39% had type 1 diabetes. Insulin injection technique improved from 48.68% to 72.46% following the intervention (p = 0.001). Lipohypertrophy occurred in 40.9% of patients, predominantly in the arm. Poor glycemic control at the baseline was significantly associated with variables like age (adjusted odds ratio (AOR) = 2.254), polypharmacy (AOR = 2.321), poor injection angle (AOR = 2.311), and inappropriate storage (AOR = 2.675). After the intervention, only age (AOR = 1.504) and polypharmacy (AOR = 1.976) maintained significance.
Conclusion:
The educational intervention successfully enhanced the insulin injection and storage procedures, thereby achieving improved glycemic control results. However, glycemic outcomes were still adversely affected by enduring factors of age and polypharmacy. This justifies the need for continuous education and individualized interventions to handle both unchangeable patient factors and mutable behaviors.
Plain language summary
Proper insulin storage and injection techniques are crucial for controlling blood sugar in people with diabetes. In Northwest Ethiopia, many patients struggle with incorrect injection practices and unsafe storage due to limited resources and a lack of education. This study assessed the effect of an educational program on insulin handling and blood sugar control among 330 diabetic patients at Debre Tabor Hospital. Participants received training on correct injection methods, site rotation, needle handling, and proper storage. Three months later, injection practices improved significantly, and blood sugar control was better. However, factors like older age and taking multiple medications (polypharmacy) still contributed to poor glycemic control. The study highlights that simple, low-cost educational interventions can improve insulin use and diabetes management, but persistent patient-specific factors require ongoing support and personalized care. These findings emphasize the importance of combining education, regular follow-up, and healthcare access to achieve optimal diabetes outcomes in resource-limited settings
Keywords
Introduction
Diabetes mellitus (DM), a metabolic disorder characterized by elevated blood glucose levels, is a prevalent non-communicable disease. 1 It is a major global health concern, especially in low- and middle-income nations with scarce medical resources. 2 Numerous severe, life-threatening illnesses are more likely to strike people with diabetes, which raises medical expenses, lowers quality of life, and increases mortality. 3 Poor glycemic control is still a common problem among patients on insulin, although insulin therapy is crucial for the management of type I and II diabetes. 4 Insulin injection technique is necessary to enhance glycemic control and reduce the risk of diabetic-related complications.5,6
Insulin misuse and storage are common problems that have a big influence on diabetes care, especially in environments with low resources. According to studies, between 50% and 60% of insulin users worldwide do not use the recommended injection sites, rotate their sites, or reuse their needles.7,8 More than 70% of patients in sub-Saharan Africa, including Ethiopia, lack adequate refrigeration facilities or are ignorant of appropriate preservation procedures, according to surveys.9,10 Since studies have shown that inappropriate insulin handling increases the risk of hyperglycemia and complications in over 40% of afflicted patients, these improper practices contribute to poor glycemic control. 11 Given how common these problems are, it is imperative that resources be allocated and educational initiatives be implemented to enhance insulin storage and usage.
Improper insulin administration strategies can affect glycemic control and raise the risk of complications connected to diabetes due to a number of factors. One of the biggest issues is a lack of knowledge and instruction on proper insulin injection techniques, especially in settings with low resources, when medical professionals do not have enough time or resources to counsel patients.12,13 Reusing needles, which is frequently motivated by financial limitations, can result in dull needles that hurt, promote lipohypertrophy, and cause irregular insulin absorption.14,15 Because elderly patients or those with neuropathy may have trouble using the right injection procedures, patient-related characteristics, including age, cognitive impairment, and reduced manual dexterity, are also very important. 16 Due to ignorance or habit, inappropriate site selection and insufficient site rotation are also frequent, which lowers insulin efficacy and raises the risk of lipohypertrophy. 17 In certain groups, cultural attitudes and misconceptions regarding the use of insulin may further impede appropriate administration methods. 18
For diabetic patients, maintaining ideal glycemic control, lowering the risk of complications, and enhancing their quality of life all depend on using the right insulin injection procedures. Studies have shown that insulin users frequently adopt incorrect strategies, which result in less-than-ideal glycemic control and higher medical expenses.12,19 Evidence-based findings from this study could improve diabetes care at Debre Tabor Comprehensive Specialized Hospital (DTCSH) and other similar facilities. The risk of lipohypertrophy, discomfort, and insulin absorption variability, all of which are frequent obstacles to reaching glycemic targets, is decreased with proper insulin delivery.14,20 The results might help medical practitioners emphasize injection technique instruction and training as a critical part of diabetic therapy. By evaluating the effectiveness of real-world interventions on glycemic outcomes, the study’s quasi-interventional design contributes to the body of literature. Given that the majority of current research on insulin administration methods focuses on wealthy nations, this is particularly crucial. 21 The results will fill in information gaps and guide future recommendations for low-resource countries. This study aims to assess the effect of insulin injection techniques intervention on glycemic control among patients with diabetes at DTCSH, Northwest Ethiopia.
Methods
Study setting, period, and design
The study was carried out at the DTCSH, which is situated in the south Gondar Zone of the Amhara Region of Northwest Ethiopia, far from 100 km from Bahirdar and 666 km from Addis Ababa. In the canton area, it serves roughly 3 million people.
A hospital-based one-group pre-post, quasi-experimental study was conducted in two phases from January 2024 to July 2024. A total follow-up period of 7 months was conducted: the first phase consisted of a 4-month intervention period, and the second phase was a 3-month post-intervention study conducted at the ambulatory clinic of DTCSH.
Study participants and sampling technique
The sample size is calculated by using the single population proportion formula with the 95% confidence level. Considering 95% confidence interval (CI) and 5% marginal error, the sample size was calculated as follows:

where
n = sample size, p = prevalence of fair practice, with a median insulin handling practice at Tikur Anbessa, which is 73.4%. 7
z—standard deviation normal value at 95% CI, which is 1.96
d—possible margin of error that can be tolerated, which is 5% (0.05).
A total of 300 sample sizes were calculated with p = 73.4%, a marginal error (d) of 5%, a threshold of significance (α) = 0.05, Zα/2 = 1.96, and q = 1 − p in consideration of prior research of this type. By adding 10% non-response rate, the final total sample size is 330.
A consecutive sampling technique was conducted to collect data.
Inclusion and exclusion criteria
Inclusion criteria
Participants in the study had to be at least 18 years old, either patients or patient caretakers.
Patients had to be taking insulin for a minimum of 3 months and returning to the hospital to replenish their prescriptions.
Exclusion criteria
Patients who did not provide their consent to take part in the research; patients with physical disabilities such as hearing or speaking impairments were not included; and psychiatric comorbidity and serious sickness in a patient.
Study variables
Dependent variable
Glycemic control: (good vs poor), assessed at baseline and after intervention.
Independent variables
Sociodemographic characteristics (age, sex, residence, education, marital status, religion, occupation, alcohol use) and clinical/treatment-related traits (diabetes type, length of insulin therapy, follow-up frequency, glycated hemoglobin (HbA1c), fasting blood sugar, lipid profile, insulin type and dose, oral hypoglycemic use, comorbidities, and polypharmacy) were examples of independent variables. Behavioral factors included self-medication habits, food, exercise, and medication adherence. Overall injection method, injection angle, vial rolling, appropriate insulin loading, and particular injection steps were all evaluated as insulin-related variables. Appropriate insulin storage conditions and storage location were among the storage-related parameters. The number of injection sites, lipohypertrophy, and side effects like discomfort, hemorrhage, and leaking were all considered injection-site factors.
Data collection tools, procedures, and quality control
Following a comprehensive analysis of the body of national and international literature on insulin storage, injection methods, and diabetes self-management habits, the data collection instruments for this study were created.15,19,21–24 The format and content of the questionnaire were informed by WHO/IDF recommendations and evidence from previously validated instruments. We created an extensive, structured, interviewer-administered questionnaire based on this literature that recorded sociodemographic traits, clinical history, insulin use patterns, knowledge and attitudes, and self-reported injection and storage procedures. In addition, a standardized observation checklist was created to objectively evaluate participants’ insulin handling procedures and injection techniques through demonstration. To guarantee accuracy and dependability, clinical measures, such as fasting blood glucose and HbA1c, were obtained using validated laboratory and point-of-care devices.
Data collectors and supervisors received training on interviewing, observation, and measurement techniques, and the tools were translated into Amharic and back-translated to guarantee accuracy. Before data collection, the tools were pretested, and any necessary adjustments were made. Regular monitoring, spot checks, and form verification were carried out by supervisors. Every measurement device underwent routine calibration, and laboratory analyses adhered to internal quality control protocols. To guarantee the final dataset’s completeness, dependability, and validity, data were double-entered, cross-checked for consistency, and disagreements were settled utilizing source documents.
Interventions and outcome measurement
The average blood glucose levels over a given time period are reflected by the biomarker HbA1C, which was used to quantify glycemic control. By objectively evaluating long-term glucose regulation, this approach offers important insights into how well diabetes management techniques work. After receiving thorough training and instructions on insulin administration and storage methods based on American Diabetes Association recommendations.25,26 Three months later, they checked how well they were controlling their blood sugar. The training covered keeping insulin working by storing it at the right temperature and handling it carefully to avoid damage. They also learned how to use injection devices, rotate injection sites, choose the right dose, and pick the best spot to inject. These methods, based on advice, aimed to make patient care better, make things more consistent, and make insulin use more accurate.
Assessment of lipodystrophy: In accordance with Ethiopian clinical standards, lipodystrophy, comprising lipohypertrophy and lipoatrophy, was identified and evaluated by visual inspection and palpation of insulin injection sites (abdomen, arms, and thighs). 27 Number of injections per day: During patient interviews, the frequency of insulin injections was noted and classified as ⩽2 or ⩾3 injections per day. And needle length: Participants’ insulin needle lengths were recorded in patient records and categorized as either short (⩽6 mm) or longer (>6 mm). 28
Data processing and statistical analysis
We put the data into Epi-data version 4.6 software after coding, cleaning, entering, and putting it all together. We used STATA version 17 for all stats stuff. We made sure there was not too much overlap between the things we were looking at and that our model was good before we got started. We used stuff like frequency and percentages to sum up what we found. If we had numbers, we showed the average, how spread out they were, the middle number, or the range between the middle 50%.
McNemar’s test was used to compare insulin injection technique practices before and after the intervention. This helped us know if what we did had any effect on sugar control. Also, to find out what things were related to not-so-good sugar control, we did binary logistic regression for both before and after. We used a fancy logistic regression model to include things that seemed like they mattered (p-value less than 0.25) when we looked at them one by one. For both before and after education, we showed adjusted odds ratios (AORs) with a 95% confidence range. If the p-value was less than 0.05 in the fancy model, we said it was a big deal.
Results
Sociodemographic characteristics
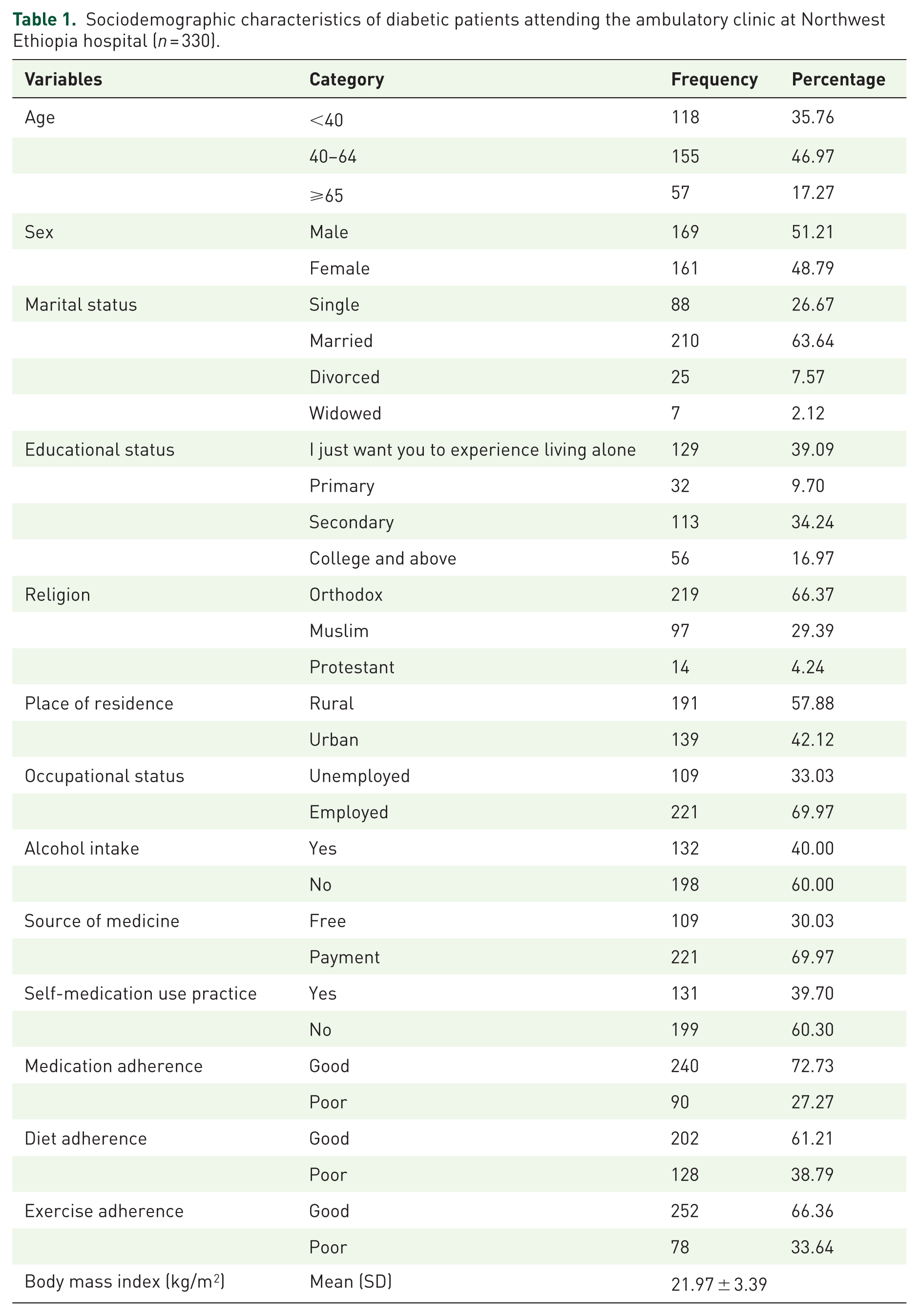
The study included 330 diabetes patients in total. A total of 46.97% of the respondents were between the ages of 40 and 64, and slightly more were men (51.21%). The majority of participants identified as Orthodox Christians (66.37%), were married (63.64%), and resided in rural areas (57.88%).
In terms of education and occupation, 69.97% were employed, and 43.94% had finished secondary school. The majority (69.97%) paid for their prescription drugs out of pocket, 39.7% self-medicated, and 40% reported drinking alcohol. A total of 72.73% of participants had good medication adherence, followed by exercise adherence (66.36%) and diet adherence (61.21%). Sixty-eight percent had a normal BMI (Table 1).
Sociodemographic characteristics of diabetic patients attending the ambulatory clinic at Northwest Ethiopia hospital (n = 330).
Clinical characteristics and laboratory parameters
Of the 330 diabetic patients included, 59.39% had type 1 diabetes. The mean duration of insulin therapy was 6.12 ± 3.11 years, with 54.85% on insulin for more than 5 years. A majority (73.33%) had ⩾4 follow-up visits per year, and the mean HbA1c and fasting blood glucose levels were 7.15% ± 2.03% and 134.18 ± 13.00 mg/dL, respectively. Most patients (74.85%) received ⩽50 IU of insulin daily, primarily using a combination of neutral protamine Hagedorn insulin and regular insulin (67.27%). Comorbidities and polypharmacy were reported in 71.21% and 22.42% of patients, respectively (Table 2).
Clinical and laboratory characteristics of patients with DM at Northwest Ethiopia Hospital (n = 330).

DM, diabetes mellitus; FBS, fasting blood sugar; GbA1C, glycated hemoglobin; HDL, high-density lipoprotein; LDL, low-density lipoprotein; NPH, neutral protamine Hagedorn insulin; RI, regular insulin; SD, standard deviation; TC, total cholesterol; TG, triglyceride.
Insulin injection technique among study participants
According to McNemar’s test, the results of the study showed that insulin injection procedures significantly improved after the intervention, with overall performance rising from 48.68% to 72.46% (p = 0.001). Important procedural actions, including site rotation, rolling the vial, evaluating clarity, and using the right injection angle, showed a significant improvement (p < 0.001). Checking expiration dates and using cotton wool with spirit were two practices that did not significantly alter the results (p > 0.05). Overall, the intervention successfully improved the majority of critical abilities related to insulin administration (Table 3).
Insulin injection technique among study participants before and after the intervention at Northwest Ethiopia Hospital, McNemar’s test (n = 330).

Insulin storage conditions
The different insulin storage settings that participants employed are displayed in the bar chart. The most commonly reported method of storing insulin was in sand (38.48%), followed by refrigeration (31.82%). Less frequently, boxes (7.58%) and dark rooms (22.1%) were utilized for storage (Figure 1).

Insulin storage conditions practice among study participants at Northwest Ethiopia Hospital (n = 330).
Insulin injection site complication
Lipohypertrophy affected about 40.9% of participants, most of whom had a single location, usually the arm. About 27.58% of respondents said they have injected into lipohypertrophic areas, primarily out of habit, convenience, or less pain. Various factors, such as technique, volume, or reusing needles, contributed to 40% of reported injection site pain cases. By contrast, bleeding/bruising (5.76%) and leaking (17.27%) were less frequent and primarily happened infrequently (Table 4).
Insulin injection site complications among patients with diabetes at Northwest Ethiopia hospital (n = 330).

Factors of glycemic control
At baseline, older age was significantly associated with poor glycemic control (AOR: 2.254; 95% CI: 1.260–5.349), as was polypharmacy (AOR: 2.321; 95% CI: 1.171–4.215), incorrect injection angle (AOR: 2.311; 95% CI: 1.421–5.341), and improper insulin storage (AOR: 2.675; 95% CI: 1.297–5.582). Incorrect injection techniques (AOR: 2.471; 95% CI: 1.654–4.428) and injection-related complications (AOR: 2.665; 95% CI: 1.296–5.481) were also significantly associated with poor baseline control. Following the intervention, age (AOR: 1.504; 95% CI: 1.076–3.012) and polypharmacy (AOR: 1.976; 95% CI: 1.146–4.626) remained significant predictors of suboptimal glycemic control. However, previously significant factors such as injection angle, technique, and storage conditions lost statistical significance post-intervention. Medication adherence and self-medication practices showed no significant association with glycemic control at either time point. Overall, the intervention appeared to mitigate the impact of several technical and behavioral factors on glycemic outcomes (Table 5).
Factors affecting glycemic control before and after the intervention among study participants at Northwest Ethiopia Hospital.

Bold value represents statistical significance (p ⩽ 0.05).
AOR, adjusted odds ratio; CI, confidence interval; COR, crude odds ratio.
Discussion
This study looked at how insulin injection and storage affect blood sugar control in people with diabetes. The research showed that things like incorrect injection angles, bad storage, the age of the insulin, taking many medicines, and wrong procedures were related to poor blood sugar control at the start. When people learned better ways to manage these things, their blood sugar levels got better. But even after the teaching, things like age and the number of medicines they took still had an influence.
This study, aligning with global research, found that education led to better insulin injection techniques. This included improvements in reading vials, checking clarity, mixing, loading air, handling syringes, and using the right injection angles. These results support those who stress that safe and efficient diabetes management depends on using the right insulin preparation and injection methods.26,29 We stress the need for safe and efficient diabetes care through appropriate insulin preparation and injection practices. Like Ji et al. 30 and De Coninck et al., 31 the study discovered that properly pinching the skin and rotating injection sites greatly enhanced insulin absorption and decreased the likelihood of lipohypertrophy. Checking expiration dates and sterilizing cotton wool with spirit, however, showed little benefit32,33 both noted this difficulty, arguing that patients frequently undervalue the significance of infection control procedures. Evidence from Powers et al. 34 and Funnell et al. 35 showing structured diabetes self-management education improves patient competency, lowers medication mistakes, and improves glucose control is highly supported by the improvement in overall injection performance. To maintain appropriate insulin handling and administration behaviors and, eventually, improve patient outcomes in diabetes management, it is imperative that patients get ongoing education, as this body of data shows.
According to insulin storage condition, 38.48% of participants store insulin in sand, a conventional method used in environments with few resources. Although 31.82% of participants stored their insulin in a refrigerator, in line with WHO guidelines of 2°C–8°C for preserving its strength, its real influence on insulin stability needs investigation. 36 About 22.12% of insulin is kept in dark rooms, which may provide some light protection but little control over temperature. 37 According to Jacob, 38 just 7.58% use box storage, indicating limited availability or confidence in this approach. These findings highlight the urgent need for targeted educational initiatives to support safe and efficient insulin storage, particularly in settings with limited resources.39,40
This study identified key factors associated with glycemic control among insulin-dependent diabetic patients both before and after an educational intervention. Age was significantly associated with poor glycemic control at both baseline and post-intervention. This finding bring into line with studies by Kirkman et al. 41 and Alramadan et al., 42 which found that older adults often struggle with issues like insulin resistance, cognitive decline, and reduced self-care, all of which can make diabetes harder to manage. Similar results were reported in Ethiopia by Getie et al., 43 who emphasized that older patients often have longer disease durations, increasing their risk for poor glycemic outcomes. Even if the intervention did help with blood sugar, age still mattered. This means older people might need specific help beyond just general advice.
Poor glycemic control was significantly predicted by polypharmacy at baseline (AOR = 2.321) and after the intervention (AOR = 1.976). This result is consistent with earlier research showing that polypharmacy impairs glycemic control by raising the likelihood of medication mistakes, negative drug interactions, and poor adherence.44,45 The fact that polypharmacy continues to be a barrier despite the educational intervention emphasizes how crucial it is to regularly examine medications, optimize them, and deprescribing when necessary. 46 Similarly, although comorbidities were significantly linked to poor glycemic control in crude analyses, this relationship was no longer significant after adjustment. This is in line with findings from Demoz et al., 47 who found that comprehensive multidisciplinary care and structured patient education can lessen the detrimental effects of comorbidities on diabetes.
At baseline, poor blood sugar control showed a strong from the use of wrong insulin injection methods, such as not mixing the insulin, using incorrect angles, and poor technique in general (AORs ranged from 1.786 to 2.675). These results are supported by Klonoff et al. 19 and Kalra et al., 48 who stressed that ineffective insulin administration impairs insulin efficacy and absorption. Following the program, most indicators were no longer important, suggesting it fixed issues with technique. Yet, poor storage still had an impact on blood sugar control by 1.6 times, matching studies by Beran et al. 49 and Bogale et al., 50 which found that storage issues, particularly in rural or resource-constrained environments, continue to reduce the effectiveness of insulin.
Results for other variables, like medication adherence and self-medication, were not entirely consistent. Self-medication was strongly related to poor blood sugar control in initial analysis, but this link disappeared after adjustments, an observation that mirrors research by Kassahun et al., 51 showing patients often try unproven treatments that hurt blood sugar management. Also, while global studies52,53 see medication adherence as vital for managing diabetes, our adjusted results did not show it as a key predictor. This could be a result of more technique and polypharmacy influence in this cohort, or measurement limitations. Furthermore, there was inconsistent evidence linking glycemic outcomes to characteristics like sex, residence, insulin dosage, and duration, which is consistent with conflicting findings from studies like Mogre et al. 54 Overall, the results support the idea that although education can help people change habits like how they inject, handling age-related issues, polypharmacy, and insulin storage is still essential for long-term glycemic control.
Overall, our results highlight the crucial importance of patient education in improving glycemic control and self-management behaviors, consistent with previous research on educational interventions in diabetes care. Recent studies indicate that structured educational programs enhance patient knowledge, treatment adherence, and self-care practices.23,55–57 Our findings underscore the value of integrating comprehensive educational strategies into routine diabetes management, as these studies demonstrate that personalized instruction, consistent reinforcement, and interactive approaches can significantly improve clinical outcomes.
There may be underlying socioeconomic inequities in the study environment that contribute to the observed inadequate glycemic control in our study. Maintaining ideal glycemic control is frequently difficult for Ethiopian patients with low incomes, little knowledge, and limited access to diabetes education and monitoring services.58,59 Furthermore, adherence to antidiabetic therapy may be hampered by the high cost of prescription drugs and transportation obstacles to medical facilities.60,61 In comparison to research carried out in higher-income or urban communities, these socioeconomic limitations and inadequate healthcare infrastructure may account for the comparatively moderate benefits seen after the intervention. 62 Socioeconomic and health system-level interventions must therefore be integrated with pharmacologic therapy to improve diabetes outcomes in such settings.
Limitation and strength
This study’s strength lies in its capacity to address important, though sometimes overlooked, aspects of diabetes care, like insulin storage and injection techniques, especially in resource-limited places such as Ethiopia. It is possible to assess the immediate effects of a straightforward, inexpensive educational intervention on glycemic control by using a pre- and post-intervention approach. Nevertheless, the study has many drawbacks, such as the absence of a control group and randomization, which could restrict causal inference and increase selection bias. The study was conducted in a single hospital with specific local practices, including types of insulin used, injection devices, needle lengths, and storage methods such as storing insulin in sand. Also, the short follow-up period 7 months might not show the intervention’s long-term outcomes. Relying on self-reporting could also create bias and the Hawthorne effect. These factors limit the generalizability of the findings to other regions or populations.
Conclusion
This study identified several factors significantly associated with poor glycemic control among insulin-dependent diabetic patients both at baseline and after intervention. With significant AORs before and after the intervention, age and polypharmacy were consistently associated with poor glycemic control. Improper injection techniques, such as not rolling the vial, incorrect injection angle, and improper storage, were strongly linked to poor glycemic outcomes at baseline. However, their impact decreased after the intervention, demonstrating the efficacy of the educational program. In addition, poor glycemic control was associated with comorbidities and injection-related complications, especially at baseline. Adjusted models revealed no significant correlation with medication adherence. However, some intrinsic factors like age and polypharmacy continued to be persistent barriers, despite the fact that the overall insulin technique improved glycemic outcomes after the intervention. This emphasizes the necessity of ongoing education and tailored interventions that address both modifiable and non-modifiable issues. Glycemic control in Ethiopia is greatly impacted by socioeconomic factors such as income, healthcare access, and education. Better diabetes outcomes depend on addressing these disparities through accessible care, patient education, and frequent follow-up.
Therefore, these results should be interpreted cautiously due to the short follow-up and local context, which includes insulin kinds, devices, needle lengths, and storage habits. This underscores the need for further education and longer-term investigations in varied communities.
Supplemental Material
sj-docx-1-tae-10.1177_20420188261417096 – Supplemental material for Impacts of insulin storage and injection techniques intervention on glycemic control among patients with diabetes in northwest Ethiopia: a quasi-experimental study
Supplemental material, sj-docx-1-tae-10.1177_20420188261417096 for Impacts of insulin storage and injection techniques intervention on glycemic control among patients with diabetes in northwest Ethiopia: a quasi-experimental study by Samuel Berihun Dagnew, Woretaw Sisay Zewdu, Samuel Agegnew Wondm, Tilaye Arega Moges, Fisseha Nigussie Dagnew, Sisay Sitotaw Anberbr, Getachew Yitayew Tarekegn, Tigabu Eskeziya Zerihun, Desalegn Addis Mussie, Abel Temeche Kassaw, Azimeraw Siraw Azenega, Teferi Bihonegn Melese, Getu Berihun Dagnaw, Mitikie Wondmagegn Mebrat, Tirsit Ketsela Zeleke and Taklo Simeneh Yazie in Therapeutic Advances in Endocrinology and Metabolism
Supplemental Material
sj-docx-2-tae-10.1177_20420188261417096 – Supplemental material for Impacts of insulin storage and injection techniques intervention on glycemic control among patients with diabetes in northwest Ethiopia: a quasi-experimental study
Supplemental material, sj-docx-2-tae-10.1177_20420188261417096 for Impacts of insulin storage and injection techniques intervention on glycemic control among patients with diabetes in northwest Ethiopia: a quasi-experimental study by Samuel Berihun Dagnew, Woretaw Sisay Zewdu, Samuel Agegnew Wondm, Tilaye Arega Moges, Fisseha Nigussie Dagnew, Sisay Sitotaw Anberbr, Getachew Yitayew Tarekegn, Tigabu Eskeziya Zerihun, Desalegn Addis Mussie, Abel Temeche Kassaw, Azimeraw Siraw Azenega, Teferi Bihonegn Melese, Getu Berihun Dagnaw, Mitikie Wondmagegn Mebrat, Tirsit Ketsela Zeleke and Taklo Simeneh Yazie in Therapeutic Advances in Endocrinology and Metabolism
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.