
Abstract
Background:
South Asians (SA) constitute a quarter of the global population and are disproportionally affected by both type 2 diabetes (T2D) and heart failure. There remains limited data of the acceptability and efficacy of low-energy meal replacement plans to induce remission of T2D in SA.
Objectives:
The objective of this exploratory secondary analysis of the DIASTOLIC study was to determine if there was a differential uptake, glycometabolic and cardiovascular response to a low-energy meal replacement plan (MRP) between SA and White European (WE) people with T2D.
Methods:
Obese adults with T2D without symptomatic cardiovascular disease were allocated a low-energy (~810 kcal/day) MRP as part of the DIASTOLIC study (NCT02590822). Comprehensive multiparametric cardiovascular magnetic resonance imaging, echocardiography, cardiopulmonary exercise testing and metabolic profiling were undertaken at baseline and 12 weeks. A comparison of change at 12 weeks between groups with baseline adjustment was undertaken.
Results:
Fifteen WE and 12 SAs were allocated the MRP. All WE participants completed the MRP versus 8/12 (66%) SAs. The degree of concentric left ventricular remodelling was similar between ethnicities. Despite similar weight loss and reduction in liver fat percentage, SA had a lower reduction in Homeostatic Model Assessment for Insulin Resistance [−5.7 (95% CI: −7.3, −4.2) versus −8.6 (−9.7, −7.6), p = 0.005] and visceral adiposity compared to WE [−0.43% (−0.61, −0.25) versus −0.80% (−0.91, −0.68), p = 0.002]. Exercise capacity increased in WE with no change observed in SA. There was a trend towards more reverse remodelling in WE compared to SAs.
Conclusions:
Compliance to the MRP was lower in SA versus WE. Overall, those completing the MRP saw improvements in weight, body composition and indices of glycaemic control irrespective of ethnicity. Whilst improvements in VAT and insulin resistance appear to be dampened in SA versus WE, given the small sample, larger studies are required to confirm or challenge this potential ethnic disparity.
Trail registration:
NCT02590822.
Introduction
The continued increase in the incidence of type 2 diabetes (T2D) in parallel with obesity gives emphasis to its importance as a global health priority. 1 Cardiovascular risk factor control reduces the risk of coronary artery disease; however, the risk of heart failure (HF) in people living with T2D remains elevated, particularly at younger ages, even when risk factors are well controlled. 2 South Asians (SA) represent 6.8% of the UK population 3 and almost one quarter of the global population. 4 They have a two to four times higher prevalence of T2D compared to White Europeans (WE) and develop the condition up to a decade earlier, at a lower body mass index (BMI). 5 Further, SA ethnicity, irrespective of diabetes status, is associated with an increased risk of cardiovascular but reduced all-cause mortality compared to their WE counterparts.6,7 SA have a significantly higher prevalence of multi-vessel coronary artery disease 8 corresponding to the higher prevalence of T2D (42% versus 15%) compared to WE. 9 Male and female SAs living in the United Kingdom have higher rates of HF hospitalizations compared to WE (rate ratios 3.8 and 5.2 for males and females, respectively) 10 and develop HF at younger age with a similar comorbidity burden as WE. 8
The Southall and Brent Revisited (SABRE) study showed baseline ethnic differences in cardiac structure and function, with evidence of more significant left ventricular (LV) concentric remodelling and lower longitudinal function amongst SA compared to WE on echocardiography. 11 Furthermore, diabetes and hyperglycaemia have been shown to potentiate the difference between ethnic groups, with SA having a greater reduction in diastolic and systolic function. 12
The landmark Diabetes Remission Clinical Trial (DiRECT) trial provided robust evidence that a low-energy meal replacement plan (MRP) delivered in primary care could induce remission of T2D with diet alone. 13 However, there remain limited data of the acceptability and efficacy of low-energy MRP to induce remission of T2D in SA. 14 The aims of this exploratory secondary analyses of the Diabeted Interventional Assessment of Slimming or Training tO Lessen Inconspicuous Cardiovascular Dysfunction (DIASTOLIC) randomized controlled trial 15 were to compare differences between WE and SA participants in: (i) compliance; (ii) weight loss, glycaemic control and exercise capacity and (iii) cardiovascular reverse remodelling following a 12-week MRP.
Materials and methods
This is a post hoc secondary analysis of the DIASTOLIC study; only data from participants allocated to the low-energy MRP were included. The full study protocol and main outcome data have been previously published.15,16 Key inclusion criteria included working aged adults (18–65 years) with established T2D (⩾3 months and <12 years) and obesity (BMI ⩾ 30 kg/m2 or ⩾27 kg/m2 if SA) without signs, symptoms or evidence of prevalent cardiovascular disease. The term ‘glycometabolic’ is used as an umbrella term for glycaemic indices, lipid profile and weight.
Low-energy MRP diet
The MRP comprised an average of ≈810 kcal/day (30% protein, 50% carbohydrate and 20% fat, Cambridge Weight Plan®). Participants discontinued all glucose-lowering and anti-hypertensive therapies following treatment allocation to avoid hypoglycaemia and hypotension, respectively. Both glucose and blood pressure were monitored throughout the study. Participants were advised to maintain their usual daily activities while on the diet and asked not to initiate any new physical activity. The diet was discontinued and a maintenance diet introduced once 50% excess body weight had been lost, or by 12 weeks, whichever came first. Those participants who achieved a loss of <2% body weight at week 1 and <4% at week 3 were considered non-compliant and were excluded from the study.
Assessments
All assessments were performed pre- and post-intervention. Demographics, medical history and anthropometric measures were collected as described previously. 15 A fasting blood sample was obtained to measure glucose and HbA1c, renal function, lipid profile and adipokines.
Magnetic resonance imaging
Comprehensive cardiac magnetic resonance imaging (MRI) scanning was performed on a 1.5T scanner (Siemens Aera, Erlangen, Germany) using a standardized protocol, 15 for the assessment of cardiac chamber volumes, function (including systolic and diastolic strain/strain rates), mass and rest/vasodilator perfusion. Images were analysed offline using CMR42 version 5 (Circle Cardiovascular Imaging, Calgary, AB, Canada) by an experienced observer blinded to all patient details and treatment group.
Transthoracic echocardiography
For echocardiographic diastolic function, images were acquired and reported as per American Society of Echocardiography guidelines 17 by one of two accredited operators using an iE33 system with S5-1 transducer (Philips Medical Systems, Best, The Netherlands) to estimate LV filling pressures (E/e′).
Cardiopulmonary exercise testing and body composition assessment
A symptom-limited incremental cardiopulmonary exercise test (CPET) was performed on a stationary electromagnetically braked cycle ergometer (eBike, General Electric Healthcare, Bedford, UK) with expired gas analysis (Ganshorn PowerCube, General Electric Healthcare, Bedford, UK) to determine peak oxygen consumption (VO2) and maximum workload. Total fat mass, visceral fat and fat-free mass were assessed by a dual-energy X-ray absorptiometry (DEXA) scan (Lunar iDEXA, General Electric Healthcare, Bedford, UK). Volumetric liver fat fraction, referred to as liver fat percentage, was quantified using either HepaFat-Scan® or 2-point MRI DIXON method with the same method used for each time-point per participant. Both utilize proton density fat fraction, which is the preferred non-invasive quantitative imaging biomarker for hepatic stenosis.
Statistical methods
Normality was assessed using histograms, the Shapiro-Wilk test and Q-Q plots. Continuous data are expressed as mean (±SD) for normally distributed data and median (Q1–Q3 interquartile range) for non-normally distributed data. In this per-protocol analysis, baseline and post-intervention data are reported by ethnic group; however, given the large number of comparisons undertaken in secondary outcome measures, only 95% confidence interval (CI) for within group changes from baseline to 12-week is displayed from paired t-test data or the interquartile range where Wilcoxon rank sum was used for non-parametric data. Analysis of covariance (ANCOVA) was conducted to determine if there was a differential response to MRP by ethnicity. All comparisons were adjusted for baseline levels. The estimated mean difference between groups with associated 95% CIs and p values are reported. Statistical analysis was performed using IBM SPSS Statistics for Windows, version 26.0 (IBM Corp., Armonk, NY, USA).
Results
Baseline data
Table 1 details the demographics, anthropometrics, glycometabolic profile, and CPET and body composition (DEXA), at baseline by ethnic group. WE were older than SA but had comparable body weight, glycometabolic measures or circulating adipokines at baseline. On CPET, the maximum workload adjusted for body weight achieved by WE group was significantly higher, and whilst peak VO2 was higher in WE (~1.6 mL/kg/min), it was not statistically different to the SA group. There was no significant difference in body composition by DEXA scan assessment, nor for liver fat percentage between the two ethnic groups at baseline.
Baseline characteristics for n = 27 randomized participants grouped by ethnicity.

WE: n = 15 and SA: n = 9.
WE: n = 14, SA: n = 8.
AD, aortic distensibility; BNP, brain natriuretic peptide; DBP, diastolic blood pressure; DEXA, dual-energy X-ray absorptiometry; EDVi, end diastolic volume index; EF, ejection fraction; GLS, global longitudinal strain; HbA1c, haemoglobin A1c/glycated haemoglobin; HOMA-IR, homeostatic model assessment of insulin resistance; LV, left ventricle; MPR, myocardial perfusion reserve; MRI, magnetic resonance imaging; RER, respiratory exchange ratio; SBP, systolic blood pressure; PEDSR, peak early diastolic strain rate.
Cardiac functional assessment by MRI and echocardiography at baseline are also detailed in Table 1. The WE group had significantly higher LV end diastolic volumes when indexed for Body Surface Index (BSA). Absolute LV mass and LV mass indexed to BSA was also higher in the WE group, but LV mass:volume ratio, a global measure of concentric remodelling, was not statistically different between the two groups nor was myocardial perfusion reserve (MPR). Finally, echocardiographic measures of structure and diastolic function showed no significant differences between the groups.
Adherence to the MRP
A flow chart of the participant journey for those enrolled included in this analysis is provided in Figure 1. The single Black-Caribbean participant was excluded from analysis given the single person group, thus permitting a focus on the SA versus WE ethnic comparison. Twenty-seven participants commencing the MRP were included in this analysis comprising 15 WE and 12 SAs. All WE completed the MRP compared to 8 (67%) SA. Of the four non-completers, none reached week 4 of the intervention. Two males were withdrawn by the study team because they could not comply with the diet (one after week 1 and the other after week 3), whereas the two females withdrew themselves from the study for non-compliance (one after the baseline visit and another after visit 3) citing family pressures and inability to adhere to the diet due to lifestyle and family commitments. Supplemental Table 1 details the baseline demographics between the four SAs who did not complete and the eight who completed. The non-completers tended to be younger, had shorter duration of diabetes, and were less obese with less insulin resistance.
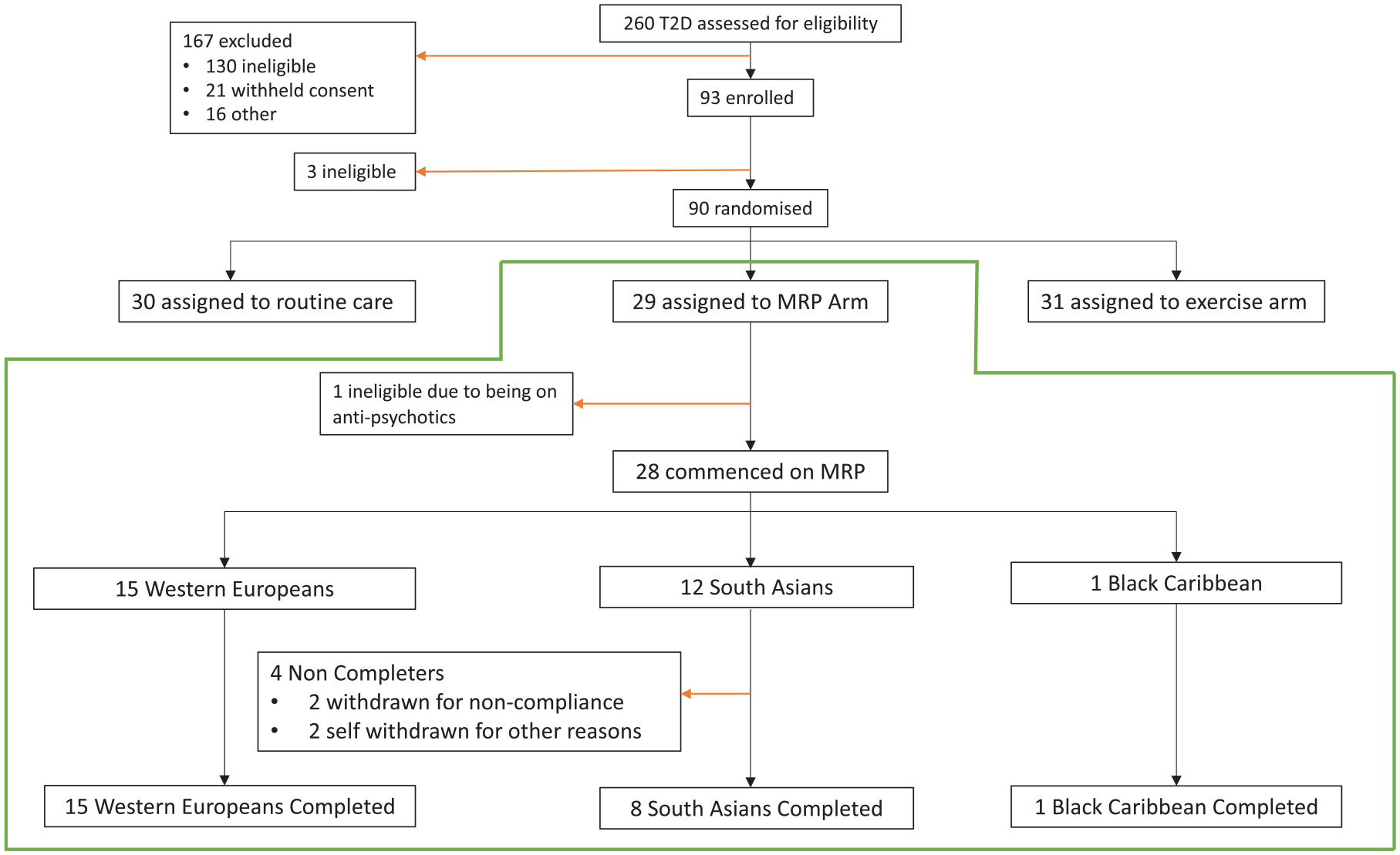
Flow chart of participant recruitment and completion, Consolidated Standards of Reporting Trials (CONSORT) Diagram.
Responses to MRP by ethnicity
The effects on anthropometric, glycometabolic response, cardiorespiratory fitness and body composition measures at 12-week MRP are presented Table 2 and key measures in Figure 2.
Summary of key anthropometric, gylcometabolic and exercise response to 12-week MRP grouped by ethnicity.

Normoglycaemic defined as HbA1c < 6.5% at week 12.
Measures achieving statistical significance indicated in bold.
Estimated mean difference in change from 12 weeks between SA and WE.
p value for change from baseline to 12 weeks between ethnic groups with adjustment for baseline values.
Fishers exact unadjusted comparison. Normally distributed data expressed as mean (SD), non-normal data as median (interquartile range).
ANCOVA, Analysis of Covariance; CPET, cardiopulmonary exercise testing; DBP, diastolic blood pressure; GFR, glomerular filtration rate; HbA1c, haemoglobin A1c/glycated haemoglobin; HOMA-IR, homeostatic model assessment of insulin resistance; MRI, magnetic resonance imaging; MRP, meal replacement plan; SA, South Asians; SBP, systolic blood pressure; VAT, visceral adiposity; WE, White European.

Box plots detailing the change in the key outcome measures of weight, HbA1c, HOMA-IR and LV mass:volume ratio. (a) Change in weight from baseline to week 12 grouped by ethnicity. (b) Change in HbA1c from baseline to week 12 grouped by ethnicity. (c) Change in HOMA-IR from baseline to week 12 grouped by ethnicity. (d) Change in LV mass:volume ratio from baseline to week 12 grouped by ethnicity.
Change in anthropometrics and haemodynamics
Following the MRP the reduction in weight observed in both groups was not statistically different [mean difference in change between SA and WE (2.5 kg (−1.2, 6.2), p = 0.172)]. Moreover, the proportion achieving ⩾ 10% and 15% weight loss at 12 weeks in both groups was comparable [⩾10% and <15 kg loss WE versus SA (9 (60%) versus 4 (50%), p = 0.269), ⩾15% kg loss WE versus SA (5 (33%) versus 2 (25%), p = 0.999)]. There was no significant difference between the groups for change in systolic and diastolic blood pressure or heart rate.
Changes in glycometabolic profile, body composition and exercise capacity
The proportion achieving normoglycaemia (HbA1c < 6.5%) at 12 weeks was comparable between groups [11 (73%) versus 5 (63%), p = 0.657, for WE and SA, respectively] with no difference in HbA1c response (mean difference in change between SA and WE [0.2% (95% CI: −0.4, 0.8), p = 0.428]. Both groups showed a decrease in fasting insulin and homeostatic model assessment of insulin resistance (HOMA-IR) with a greater reduction observed in the WE compared to the SA group [fasting insulin; −16.3 min/L (IQR: −19.8, −3.3) versus −13.1 (−27.2, −0.1), p = 0.002 and HOMA-IR; −7.4 (−9.9, −3.3) versus −4.3 (−8.5, −0.3), p = 0.005 for WE and SA, respectively]. There was no significant difference in the change between the groups for liver fat percentage or for total fat mass and lean mass which decreased and increased respectively as a percentage of body weight. However, the reduction in % visceral adipose tissue (VAT) in the WE group was greater and almost double that of the SA group [−0.80% (95% CI: −1.0, −0.62) versus −0.37(−0.56, −0.18) for WE and SA, respectively (p = 0.002)].
There was no change in absolute peak workload for either group, but workload/kg increased comparably between the groups following MRP. In the WE group, peak VO2 increased by 2.8 mL/kg/min with a negligible increase observed in SA with the between group not reaching statistical significance.
Change in cardiovascular structure and function in response to MRP
Changes in cardiac MRI and echocardiography in response to the MRP, stratified by ethnic group, are shown in Table 3. LV ejection fraction showed a decrease in both groups post-MRP, but remained within normal limits, and there was no change in global longitudinal strain or peak early diastolic strain rate following the MRP. However, LV mass:volume ratio decreased in the WE but not the SA group and GLS decreased in the SA group but not the WE. There was no change in MPR; however, aortic distensibility increased in WE and to a lesser degree in the SA group with no significant difference in mean change between groups. Both groups saw no change in non-invasive estimate of LV filling pressure (E/e′).
Change in cardiovascular structure and function in response to MRP grouped by ethnicity.

Data are expressed as mean ± SD or median (Q1–Q3), change is expressed as mean (95% CI).
Estimated mean difference in change from 12 weeks between SA and WE.
p value for change from baseline to 12 weeks between ethnic groups with adjustment for baseline values.
AD, aortic distensibility; GLS, global longitudinal strain; EDV, end diastolic volume; EF, ejection fraction; LV, left ventricle; LVM, left ventricular mass; Max LAV, maximum left atrial volume; MBF, myocardial blood flow; MPR, myocardial perfusion reserve; MRI, magnetic resonance imaging; PEDSR, peak early diastolic strain rate.
Discussion
In this secondary analysis of the DIASTOLIC study, we sought to determine if there is a differential response by ethnicity (WE versus SA) to those allocated the 12-week low-energy MRP. We have undertaken a detailed characterization beyond weight loss and glycaemic control that includes multimodal assessment of cardiovascular structure and function, body composition and exercise capacity via CPET. In this study, most participants achieved normoglycaemia (HbA1c < 6.5%) by 12 weeks, thus adding important novel findings in response to the call for ‘active observation of individuals experiencing a remission’ by the international diabetes remission panel. 18 Moreover, it adds much needed interventional data for those of SA origin who remain significantly underrepresented in clinical research studies despite comprising a quarter of the global population. 4 Whilst the results should be considered exploratory, given the small sample size and within group comparisons, in the SA group, we have demonstrated poorer compliance, less reduction in VAT and lesser improvement in insulin resistance compared to their WE counterparts despite comparable weight loss and reduction in liver fat percentage.
MRP compliance in SA
The seminal DiRECT trial has demonstrated the efficacy of a low-energy MRP to induce remission of T2D in a primary care setting 19 and NHS England has rolled out pilot programmes across the country (https://www.england.nhs.uk/diabetes/treatment-care/low-calorie-diets/). However, there is under representation of SA in most studies. A pilot, proof of concept has recently been published, which has shown that SA living in the United Kingdom can lose weight in response to a low-energy MRP and induce remission of T2D. 14 However, this small study (total n = 25) randomized SA participants to immediate (n = 13) or delayed MRP (n = 12), and there was no comparison with WE subjects. Due to the impact of the COVID-19 pandemic the study, had limited phenotyping (no cardiac MRI or assessment of exercise capacity) with some missing data.
In the DIASTOLIC study, we harnessed the multi-ethnic population base in Leicester with just under half of participants being of SA heritage. This was specifically encouraged by patient and public involvement events and community engagement within the Leicester boroughs that have high SA populations. The adherence to the MRP was worse in the SA as compared to the WE participants for which all completed the MRP. The percentage dropout observed in our study is higher than that reported for both the ‘South Asian diabetes remission randomized trial for proof-of-concept and feasibility (STANDby)’ study and DiRECT trial at 16% 14 and 22%, 19 respectively, for those who commenced the MRP. The four non-compliant SA participants in our study were evenly split by sex, with females withdrawing themselves after failing to comply and the males being withdrawn by the study team for non-compliance observed at clinical review assessments. The SA females cited lack of support and understanding from the family with an expectation to continue cooking family meals and perform household chores. These served as a deterrent to compliance despite an interest in pursuing the MRP. Both male participants were deemed non-compliant by the study team, physician and dietician with one having failed to achieve the 2% reduction in body weight at week 1 and the other failing to achieve 3% weight loss at week 4. These results are suggestive of sex differences to dropout; however, interpretation must be taken with caution given the small numbers. Future studies would benefit from a formal qualitative analysis of non-compliant/withdrawals to explore potential ethnic and sex differences and challenges to adherence and compliance to MRP.
Anthropometrics, cardiometabolic markers and body composition
The two groups were well-matched at baseline. Overall, for completers, there was a very good response to the MRP with similar average weight loss, normalization of glycaemic status and reduction in systolic blood pressure. Moreover, this study has shown that the MRP is an effective weight loss tool within the SA population cohort that adhered to the intervention, in line with recent findings. 14 Further, a Dutch study by Van Schinkel and colleagues looked at a short-term caloric restriction as a metabolic stress to study cardiac flexibility. They studied 12 middle-aged overweight and insulin resistant SA and 12 matched WE. Myocardial triglyceride levels were increased in both ethnicities following the intervention with no significant difference between groups. However, ectopic fat stores, specifically paracardial fat volume, demonstrated a differential response, with fewer favourable changes in SA. 20 This is in line with our observations of an almost two-fold reduction in percentage VAT mass in WE versus SA, again despite similar overall weight loss, and comparable baseline values. This may be related to the difference in the differential metabolic response in SA. 21 A previous study utilizing a two-step hyperinsulinaemic-euglycaemic clamp before and after an 8-day very low calorie diet (VLCD) has shown that SA display a different metabolic adaptation to VLCD than WE. SA had a lower insulin clearance rate but a lower glucose disposal rate. Insulin clearance is a fundamental component of insulin metabolism acting to reduce the availability of insulin with lower insulin clearance associated with insulin resistance and metabolic dysfunction. 22 This study aligns with the reduced improvement in insulin and HOMA-IR we observed in the SA group versus WE group, for the same reduction in body weight. This could be, in part, attributed to the lower reduction in VAT observed in SA and reflected by residual adipokine dysregulation in SA. WE saw a more marked increase in adiponectin and reduction in leptin compared to the SA group, albeit non-significant. However, given that there was no significant difference in the reduction in liver fat between the two groups and comparable reduction in HbA1c, a less variable measure of glycaemic control, this finding could indeed be a type II error and occurred due to chance and required confirmation or challenging in larger studies. Further, it is plausible that the higher fasting insulin and subsequent HOMA-IR observed in SA are resultant from a failure to fast for the study appointment future studies could confirm fasting status with ketone assessment and/or provide standardized meal the night before fasting with telephone contact to support adherence to the standardize meal and overnight fasting.
Exercise capacity
Absolute and weight-adjusted maximum workload was higher in the WE group at baseline; however, the observed increase for weight-adjusted maximum workload was comparable between ethnic groups. Relative peak VO2 was also higher in WE at baseline which increased following MRP in WE and only negligibly in SA; however, the difference did not meet statistical significance. Peak VO2 is a key measure of fitness and exercise capacity and considered the gold standard measure of prognosis in HF. 23 The data suggest that MRP may not provide equivalent effects to cardiorespiratory fitness across the ethnicities.
Cardiac functional assessment by MRI and echocardiography
LV mass:volume ratio, a measure of concentric remodelling, is an important morphological alteration observed in T2D, with asymptomatic LV hypertrophy (increased LV mass:volume ratio) a recognized characteristic of stage B HF, 24 and associated with incident HF in T2D. 25 SA and WE had comparable degree of concentric remodelling at baseline; following the 12-week MRP, there was greater reduction in LV mass:volume ratio in WE, but not the SA group although the between group difference did not reach statistical remodelling. However, the data may suggest that reverse concentric remodelling following weight loss may be blunted in SA with T2D, but this observation needs confirmed in a larger population.
The MESA study assessed MPR across their ethnic groups with cardiac MRI; 26 however, this did not include SA, and to date, there have been no published data assessing the difference in MPR assessed by cardiac MRI between SA and WE at a cross-sectional level or post-intervention. 27 This is the first study to our knowledge investigating MPR with an ethnic comparison. The statistical comparisons are limited by the wide standard deviations for MPR and limited sample size but may point to more severe microvascular dysfunction in the SA at baseline with a trend to improvement in this group following the MPR.
There was no significant difference in the change in peak early diastolic strain rate between the ethnic groups; however, both groups demonstrate a trend to worsening strain rate. This is in keeping with previous literature on low-calorie diet interventions, which indicate a worsening in diastolic function postulated to be resultant of a flux of circulating free fatty acids and subsequent increased myocardial triglyceride accumulation following a MRP. 28 However, this was a lower calorific deficit than our study (471 kcal/day), and participants were assessing an acute response at 3 days. Systolic function also reduced in both groups, but, as there is an element of obesity related hypercontractility that has been previously reported, 29 this likely reflects normalization of function following weight loss.
Strengths and limitations
This is an important subgroup analysis of an ethnic population disproportionally affected by T2D and progression to HF. The selection process within our study is robust as the participants were allocated into the MRP arm through a computerized randomization process, and stratified by sex and glucose-lowering therapy. Another strength in the current study is the assessment of cardiac structure and function using comprehensive multiparametric CMR, the gold standard, instead of the more operator dependent echocardiogram with limited reproducibility. We have been limited by a small sample size, and therefore, the results surrounding compliance may not be truly representative and should be considered with caution. Furthermore, this current secondary analysis was not specifically powered to detect ethnic difference in response to MRP but provides important hypothesis generating and exploratory insights to potential differential response to low-calorie-diet-induced weight loss.
Future research
Larger studies with longer follow-up periods are required to assess if our findings translate to the larger population and determine if compliance is systematically lower in people of SA origin. The larger studies should match participants according to age, sex and body composition. Rates of T2D remission will also be an important factor to consider in further ethnicity comparison studies. This will then inform tailored preventative strategies in SA including the effects of newer treatments that affect glycometabolic status like glucagon-like peptide 1 (GLP-1) agonists and sodium-glucose co-transporter-2 inhibitors (SGLT2i).
The effect of ethnicity across different lifestyle interventions, including a supervised exercise programme, should be considered, including using supervised exercise as an added intervention measure to assess if it can augment the improvements seen in the SA group. Metabolomic studies to look at whether metabolic biomarkers are attenuating the improvement in the cardiometabolic profile improvement in SA are also an arena for further research.
Conclusions
In this exploratory secondary analysis of the DIASTOLIC study, we report reduction in body weight, improvements in cardiometabolic risk, liver fat and visceral adiposity across both SA and WE ethnic groups. The signal of a less favourable acceptance and differential ethnic response in VAT and insulin resistance to MRP in SA requires validation in a larger study.
Supplemental Material
sj-docx-1-tae-10.1177_20420188231193231 – Supplemental material for Response to a low-energy meal replacement plan on glycometabolic profile and reverse cardiac remodelling in type 2 diabetes: a comparison between South Asians and White Europeans
Supplemental material, sj-docx-1-tae-10.1177_20420188231193231 for Response to a low-energy meal replacement plan on glycometabolic profile and reverse cardiac remodelling in type 2 diabetes: a comparison between South Asians and White Europeans by Lavanya Athithan, Gaurav S. Gulsin, Joseph Henson, Loai Althagafi, Emma Redman, Stavroula Argyridou, Kelly S. Parke, Jian Yeo, Thomas Yates, Kamlesh Khunti, Melanie J. Davies, Gerry P. McCann and Emer M. Brady in Therapeutic Advances in Endocrinology and Metabolism
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.