
Abstract
Background:
Endometriosis is an oestrogen-dependent disease that can cause subfertility in women who may require assisted reproductive technology (ART) to achieve their pregnancy goals.
Objectives:
The aim of this study was to compare ART outcomes in women with endometriosis following the long GnRH-agonist controlled ovarian stimulation (COS) protocol with those taking the GnRH-antagonist COS protocol.
Data Sources and Methods:
MEDLINE, Embase and Web of Science were systematically searched in June 2022. Randomized controlled trials (RCTs) and observational studies comparing the long GnRH-agonist COS protocol and the GnRH-antagonist COS protocol in women with all stages/subtypes of endometriosis were included. Data were synthesized into comprehensive tables for systematic review. The Scottish Intercollegiate Guidelines Network (SIGN) checklists were used for the risk of bias assessment of non-randomized studies and randomized studies, and all the included studies were deemed to have acceptable quality.
Main Results:
Eight studies (one RCT and seven observational) with 2695 patients (2761 cycles) were included. Most studies generally reported non-significant differences in clinical pregnancy or live birth rates regardless of the COS protocol used. However, the GnRH-agonist protocol may yield a higher total number of oocytes retrieved, especially mature oocytes. Conversely, the GnRH-antagonist protocol required a shorter COS duration and lower gonadotrophin dose. Adverse outcomes, such as rates of cycle cancellation and miscarriage, were similar between both COS protocols.
Conclusion:
Both the long GnRH-agonist and GnRH-antagonist COS protocols generally yield similar pregnancy outcomes. However, the long GnRH-agonist protocol may be associated with a higher cumulative pregnancy rate due to the higher number of retrieved oocytes available for cryopreservation. The underlying mechanisms of the two COS protocols on the female reproductive tract remain unclear. Clinicians should consider treatment costs, stage/subtype of endometriosis and pregnancy goals of their patients when selecting a GnRH analogue for COS. A well-powered RCT is needed to minimize the risk of bias and compare the risk for ovarian hyperstimulation syndrome.
Registration:
This review was prospectively registered at PROSPERO under Registration No. CRD42022327604.
Keywords
Introduction
Endometriosis is an inflammatory oestrogen-dependent disease characterized by endometrial-like tissue found outside of the uterus. Endometriosis lesions are often located in the peritoneum, ovaries (endometrioma) and uterus, but lesions can also be found in the bowel, urinary tract and vagina. Endometriosis is associated with a wide range of symptoms including visceral syndrome (e.g. pelvic pain, painful urination, dyschezia), dysmenorrhoea and subfertility. Traditionally, endometriosis classification is based on the location of endometrial tissue lesions, and the three most prevalent types are ovarian endometriomas, superficial peritoneal endometriosis or deep endometriosis.1,2 Endometriosis is commonly graded on the revised American Society for Reproductive Medicine (r-ASRM) classification scale. Depending on the extent of lesions, it is classified according to the four stages: minimal (stage I), mild (stage II), moderate (stage III) and severe (stage IV).1,2
Endometriosis lesions can alter the pelvic anatomy, lead to excess inflammation and can negatively impact the reproductive cycle resulting in subfertility in 30–50% of affected women.3,4 In women with endometriosis desiring to become pregnant, around 10–25% require assisted reproductive technology (ART), such as in vitro fertilization (IVF) and intracytoplasmic sperm injection (ICSI). 5 Since the 1980s, the long gonadotrophin-releasing hormone (GnRH) agonist protocol has been the gold standard for controlled ovarian stimulation (COS) to prevent a premature luteinizing hormone (LH) surge and improve ART outcomes. However, this protocol requires an extensive treatment period which is associated with more frequent side effects (such as hot flushes/flashes, bleeding, cyst development and headache) and has a higher risk of ovarian hyperstimulation syndrome (OHSS), which can be life-threatening. 6 The GnRH-antagonist protocol is a promising alternative with a reduced risk of OHSS, shorter treatment time and often requires a reduced gonadotrophin dose as a result of GnRH antagonists being able to rapidly inhibit GnRH receptors within hours of administration. 7 However, previous studies report poorer pregnancy outcomes in infertile couples after the GnRH-antagonist protocol.8,9
Compared to other causes of infertility, little research has focused on patients with endometriosis specifically, and it remains uncertain whether patients with endometriosis respond similarly to the long GnRH-agonist and GnRH-antagonist COS protocols. Furthermore, the fertilization rate is often overlooked, and it has recently been shown that fertilization rate positively correlates with cumulative live birth rate (LBR). 10 In this systematic review, we aim to compare ART outcomes following the long GnRH-agonist COS protocol with the GnRH-antagonist COS protocol specifically for women with endometriosis.
Methods
Patient populations
The patient populations consisted of women diagnosed with any form of endometriosis undergoing IVF/ICSI with ovarian stimulation using the long GnRH-agonist protocol compared to the GnRH-antagonist protocol.
Core outcome sets
The primary outcomes were related to pregnancy [clinical pregnancy rate (CPR) and LBR]. Secondary outcomes included the number of oocytes retrieved [total and metaphase II (MII)], fertilization rate, COS parameters (treatment duration and gonadotrophin dose) and adverse ART outcomes (miscarriage rate, cycle cancellation rate and OHSS).
Search strategy, eligibility criteria and study selection
A systematic search of the published literature up to 10 June 2022 was undertaken on MEDLINE, Embase and Web of Science databases using the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) guidelines. 11 The following keywords and medical subject headings (MeSH) were queried: endometriosis, endometrioma, infertility, GnRH agonist, GnRH antagonist, in vitro fertilization and ICSI (the full search strategy is detailed in Supplementary Table 1). Database search results were imported into EndNote (X9, Clarivate Analytics) prior to title and abstract screening. The PRISMA flowchart can be found in Figure 1.
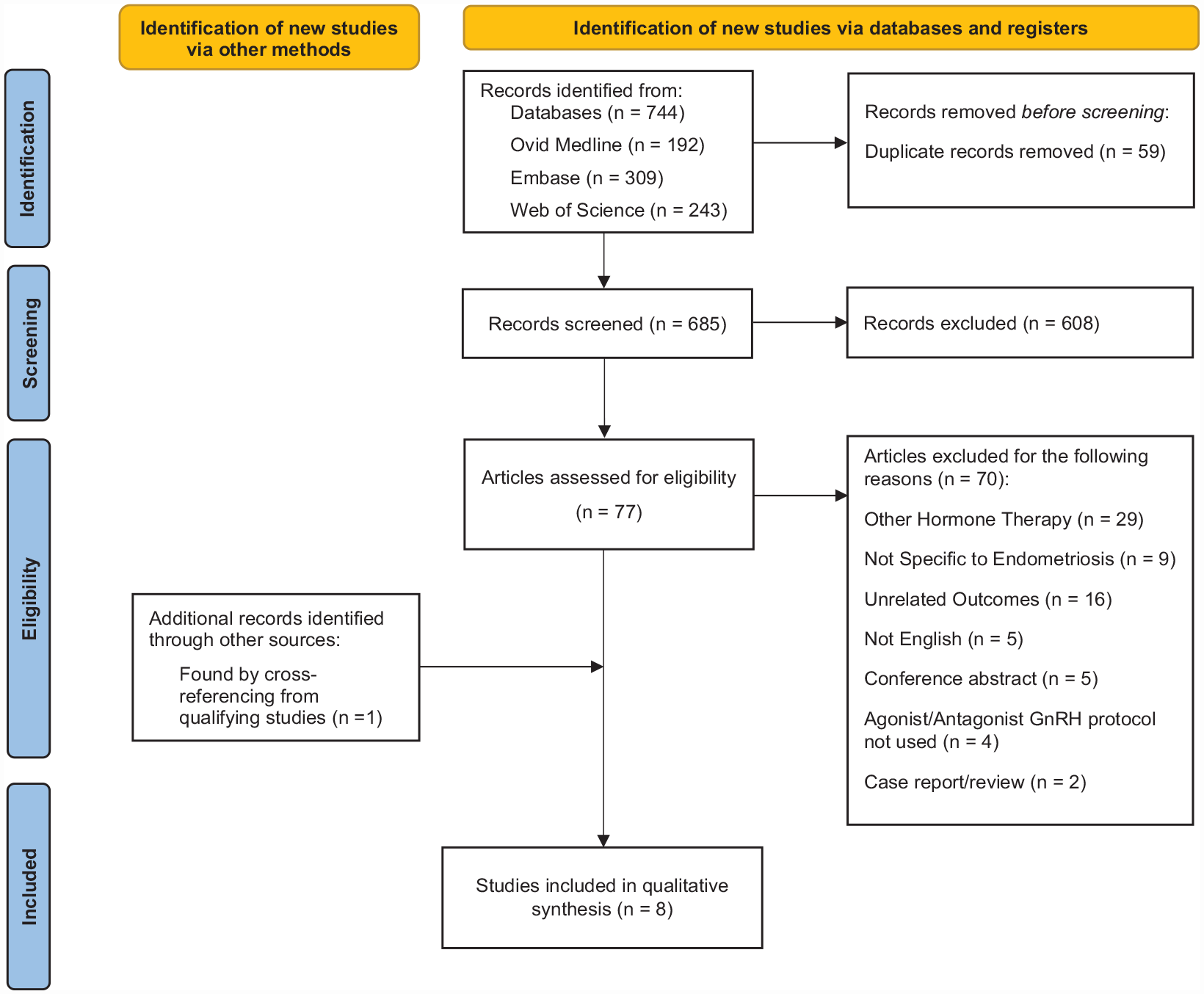
PRISMA flow diagram summarizing the search strategy used to identify qualifying studies.
Duplicate studies were removed and two authors (K.K.W.K. and S.O.) independently screened titles and abstracts, and excluded obviously irrelevant studies. Equivocal studies were independently screened by the third author (J.A.T.) until a consensus could be reached. Full manuscripts of studies meeting the selection criteria were retrieved and reviewed by K.K.W.K., S.O. and J.A.T. for the final decision. Studies that used other GnRH-agonist protocols (i.e. ultralong or short) or had patients without endometriosis were excluded. Case reports, conference abstracts with unavailable data and trial protocols were also excluded.
Data synthesis and bias assessment
Data extraction was completed by K.K.W.K. and S.O. All data from randomized controlled trials (RCTs) and observational studies (and their relevant subgroups) comparing the long GnRH-agonist protocol versus the GnRH-antagonist COS protocol for women with endometriosis were included (Supplementary Table 2). Data were synthesized into outcome tables.
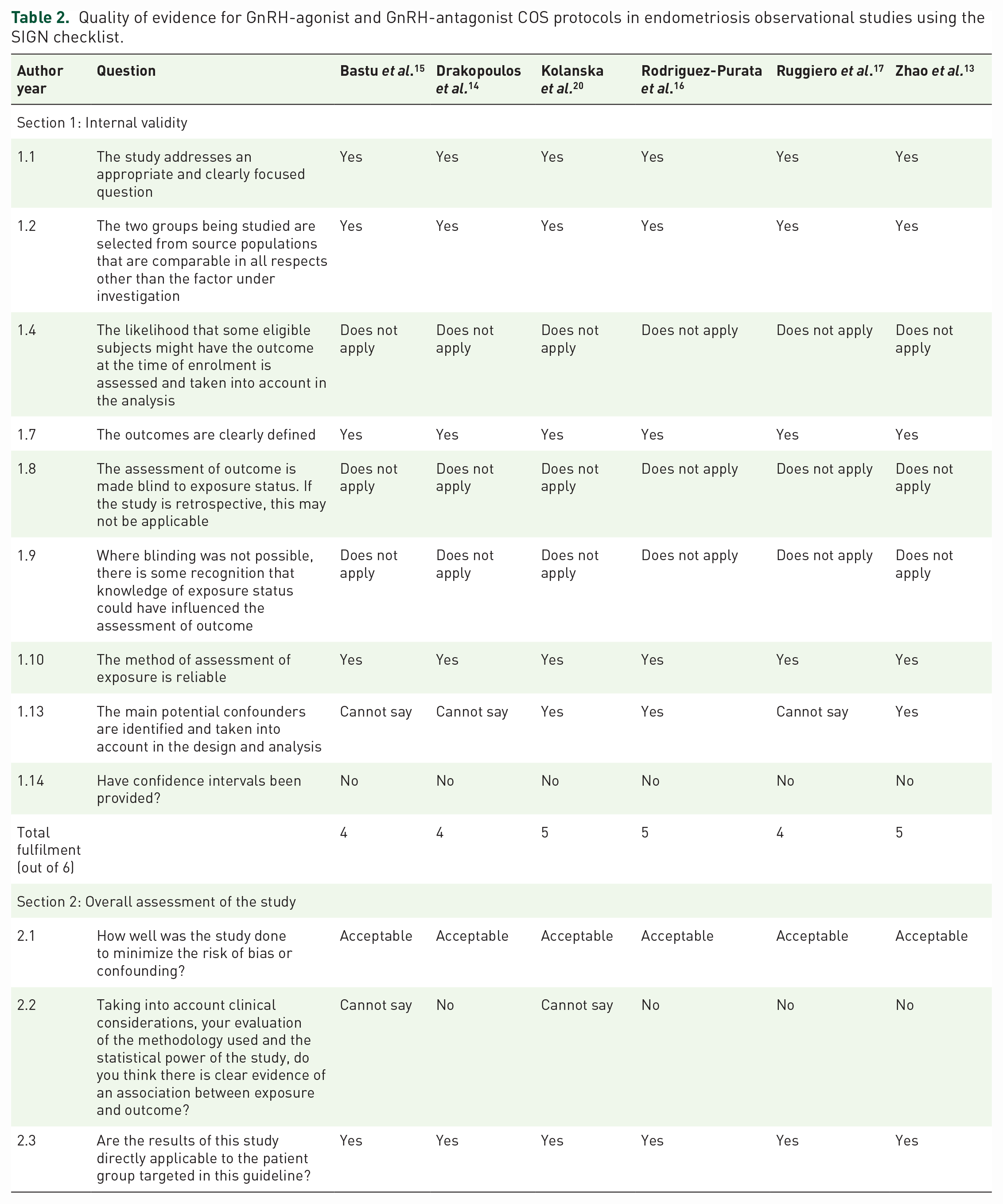
The rigour of study methodology and risk of bias was critically appraised using the relevant Scottish Intercollegiate Guidelines Network (SIGN) criteria for cohort studies and RCTs (description of criteria are available on the SIGN website). 12 For cohort studies, this tool aims to assess the internal validity (selection of subjects, assessment of exposure and outcomes, confounding factors, statistical analysis) and overall study quality. Statements 1.3, 1.5, 1.6, 1.11 and 1.12 of the SIGN cohort study tool were excluded as all the studies were retrospective in nature and outcomes were objective in accordance with the SIGN’s checklist notes. 12 The RCT tool assesses for a focused research question, patient randomization, blinding methods, interventions, attrition bias, analysis methods and overall study quality.
Results
Study characteristics
Using a systematic searching approach, 744 titles were identified from database searches. After 59 duplicate titles were removed, 608 titles and abstracts were excluded. Ultimately, eight studies were included for the final analysis with a total of 2695 women and 2761 cycles (study characteristics are summarized in Table 1).13–20 In these studies, 1721 cycles used the long GnRH-agonist protocol and 1040 cycles used the GnRH-antagonist protocol. Six retrospective analyses,13–17,20 one cross-sectional study 18 and one RCT 19 were identified. Each study was undertaken at a single centre, and all inclusion/exclusion criteria were available.
Summary table of characteristics of included endometriosis studies.

♀, female; #, number; ASRM, American Society for Reproductive Medicine Classification; COS, controlled ovarian stimulation; CP, clinical pregnancy; CPR, clinical pregnancy rate; d, days; DOR, diminished ovarian reserve; ET, embryo transfer; FR, fertilization rate; GnRH-a, gonadotrophin-releasing hormone agonist; GnRH-ant, gonadotrophin-releasing hormone antagonist; Hx, history; hMG, human menopausal gonadotrophin; IN, intranasal; ICSI, intracytoplasmic sperm injection; IR, implantation rate; IU, units; IVF, in vitro fertilization; MRI, magnetic resonance imaging; N, number of patients; OCP, oral contraceptive pills; OR, oocytes retrieved; PCOS, polycystic ovarian syndrome; Prev., previous; r-AFS, revised American Fertility Society classification system; RCT, randomised controlled trial; SC, subcutaneous.
For the long GnRH-agonist protocol, four studies administered triptorelin,14,15,18,19 two studies administered leuprorelin16,17 and one study administered decapeptyl 13 daily starting from day 20 to 21 of the previous menstrual cycle. One study 20 did not specify which GnRH agonist was used and started treatment after day 21 of the preceding cycle. Seven studies in the GnRH-antagonist arm administered subcutaneous cetrorelix or ganirelix.13–19 Five of which followed a flexible multiple dosing protocol13,15–17,19 and two of which followed a fixed protocol from day 5 or day 6.14,18 One study also gave patients in the GnRH-antagonist arm an oral contraceptive pill pretreatment taken for 14–24 days in the preceding cycle followed by a 3- to 5-day washout period. 16 One study did not specify the antagonist used and started the protocol after at least 6 weeks of oral contraceptives. 20
Study quality and risk of bias assessment
The completed SIGN assessments for observational studies and the RCT can be found in Tables 2 and 3, respectively. Since the study by Hosseini et al. was a cross-sectional study, a SIGN 12 checklist was not required (as described by SIGN’s study design algorithm). As mentioned earlier, Statements 1.3, 1.5, 1.6, 1.11 and 1.12 were not applicable for retrospective studies. Statements 1.3, 1.8 and 1.9 did not apply since patients did not have the outcome before starting the intervention (1.4) and the primary outcomes of interest (pregnancy and LBRs) were objective and would not be affected by blinding (1.8 and 1.9). All studies had a clearly focused question, had representative patient characteristics and clearly defined outcomes. All studies had overall acceptable quality and were eligible for review. Two observational studies mentioned that the assignment of the GnRH-agonist protocol or the GnRH-antagonist protocol varied between clinicians.15,16 Kolanska et al. 20 were the only observational study to exclusively offer either the GnRH-agonist protocol or the antagonist protocol during specific timelines minimizing selection bias to either protocol. Although Rodriguez-Purata et al. 16 mentioned that poorer responders tended to use the antagonist protocol, a propensity score matching statistical method was used to compare CPRs. This method adjusts for covariates such as disease severity and comorbidities that may affect the probability of patients allocated to a certain treatment. As such, only patients with similar characteristics were compared for this outcome which helped mitigate selection bias. Two studies performed multivariate logistic regression to identify predictive factors affecting pregnancy or birth rates.13,18 The inclusion of a small number of women with polycystic ovary syndrome, tubal infertility or adenomyosis alongside endometriosis also raised concerns for additional confounding factors.14,20 Four of the studies only included women undergoing their first IVF/ICSI cycle, which reduced the risk of confounders from women who require multiple IVF cycles due to poorer ART outcomes.14,15,18,19 Since the primary outcomes of interest were objective, the studies were at lower risk of measurement bias. For the RCT, randomization methods were adequate, although there was a lack of blinding. An adequate sample size for pretest power estimation could not be calculated since there was a lack of studies comparing the long GnRH-agonist versus the GnRH-antagonist protocol prior to this RCT. 19
Quality of evidence for GnRH-agonist and GnRH-antagonist COS protocols in endometriosis observational studies using the SIGN checklist.
Quality of evidence for GnRH-agonist and GnRH-antagonist COS protocols in endometriosis RCTs using the SIGN checklist.

ART outcomes
Clinical pregnancy rate
CPR was reported by all eight studies and was calculated by CPR per embryo transfer (ET) in three studies13,17,18 or CPR per patient/cycle in four studies,14–16,19 (see Table 4). Kolanska et al. 20 were the only study to report both CPR per cycle with ET and CPR per patient and analysed fresh/frozen ETs separately. Most studies found no significant difference in CPR13–20 between the long GnRH-agonist and GnRH-antagonist protocols except for two subgroup analyses.18,20 For advanced endometriosis, Hosseini et al. 18 reported a significantly higher pregnancy rate with the GnRH agonist when anti-Müllerian hormone (AMH) levels were between 1.1 and 2.7 ng/ml (p = 0.04). Kolanska et al. 20 found significantly higher CPR per started cycle with the GnRH agonist when analysing fresh ETs from women with all forms of endometriosis combined (p = 0.02) but no significant difference for CPR per cycle with ET only or freeze–thaw cycles. No difference (p > 0.05) was found when analysing deep or ovarian endometriosis in isolation regardless of fresh or freeze–thaw cycles. 20 Multivariate logistic regression analysis was performed by two studies which identified maternal age (p = 0.006) and number of embryos (p = 0.03) as main factors that may predict pregnancy rate.13,18
CPR outcome data for GnRH-agonist and GnRH-antagonist COS protocols in women with endometriosis.

AMH, anti-Müllerian hormone; CPR, clinical pregnancy rate; DE, deep endometriosis; ET, embryo transfer; Hx, history; NS, not statistically significant.
All values shown as percentage (absolute number).
Live birth rate
LBR was included in three studies13,14,20 (see Table 5). The LBR was calculated as either births per ET cycles13,20 or births per started cycle regardless of the number of embryos transferred.14,20 Two studies found no significant difference in LBR between protocols.13,14 Kolanska et al. performed subgroup analyses by endometriosis subtype and fresh/freeze–thaw embryos and found no significant difference between protocols in LBR for patients with DE or endometriomas in isolation regardless of ET methods. However, the LBR per started cycle (regardless of whether embryos were transferred) was significantly higher (p = 0.02) in the long GnRH-agonist group. 20 Zhao et al. 13 were the only study to perform regression analysis and found maternal age to be the strongest predictive factor for women with diminished ovarian reserve (DOR) following ovarian cystectomy.
LBR outcome data for GnRH-agonist and GnRH-antagonist COS protocols in women with endometriosis.

All values shown as percentage (absolute number).
CPR, clinical pregnancy rate; DE, deep endometriosis; ET, embryo transfer; LBR, live birth rate; NS, not statistically significant.
Number of oocytes retrieved
Six studies assessed the total number of oocytes retrieved13,14,16–19 (see Table 6). Two studies included women with resected endometrioma and found no difference in the number of oocytes retrieved between COS protocols.13,19 However, in women with active endometriomas, Pabuccu et al. reported a higher number of oocytes (p = 0.002) retrieved using the GnRH-agonist protocol. The number of oocytes retrieved from patients with stage I–II endometriosis was reported by two studies, and both found no significant difference between protocols.14,19 Three studies included women with stage III–IV endometriosis and two found no significant difference.14,17 In a subgroup analysis of advanced endometriosis grouped by AMH levels, women with AMH levels between 1.1 and 2.7 ng/ml did not differ in the number of oocytes retrieved between the two COS protocols. However, in women with AMH less than 1.1 ng/ml, the long GnRH-agonist protocol yielded more oocytes, while in women with AMH greater than 2.7 ng/ml, the GnRH-antagonist protocol led to an increased number of oocytes retrieved. 18 Rodriguez-Purata et al. 16 included all stages of endometriosis and found a significantly higher number of oocytes retrieved using the long GnRH-agonist protocol (p = 0.001). However, the propensity score was not applied to this outcome.
Number of oocytes retrieved for GnRH-agonist and GnRH-antagonist COS protocols in women with endometriosis.

#, number; AMH, anti-Müllerian hormone; Hx, history; IQR, interquartile range; NS, not statistically significant.
All number of oocytes retrieved shown as mean ± standard deviation unless * [mean (IQR)].
Four studies included the number of MII oocytes retrieved15–17,19 (see Table 6). Pabuccu et al. were the only study to analyse patients with stage I–II endometriosis and found no difference between the two protocols. In severe stages of endometriosis, Ruggiero et al. 17 reported a significantly higher number of MII oocytes retrieved when the GnRH-antagonist protocol was used. Two studies included patients with active/resected endometrioma and found a significantly higher number of MII oocytes retrieved when GnRH-agonist COS was used (p = 0.0001–0.01).15,19 Rodriguez-Purata et al. 16 did not apply the propensity score matching for this outcome but also found a significantly higher number of MII oocyte yield using the GnRH-agonist protocol.
Fertilization rate
Fertilization rate (FR) was reported by four studies13,15,17,19 (see Table 7). Pabuccu et al. 19 were the only study to compare FR in women with stage I–II endometriosis and found no difference between COS protocols. Also, no significant difference was found in women with severe endometriosis. 17 Two observational studies of women with endometrioma resection13,15 reported no significant difference in FR although the RCT found a significantly higher FR when the long GnRH-agonist was used in resected endometrioma (p = 0.001) but not in active endometrioma. 19
Fertilization rate outcome data for GnRH-agonist and GnRH-antagonist COS protocols in women with endometriosis.

Hx, history; NS, not statistically significant.
All values shown as mean ± standard deviation.
COS parameters
COS duration
Among the seven studies that reported COS duration13–17,19,20 (see Table 8), only one found a significant difference in the COS duration 14 with the agonist protocol having a longer duration compared to the antagonist protocol (p = 0.001). Drakopoulos et al. 14 found a significant difference between the GnRH-agonist and GnRH-antagonist duration in women with stage III–IV endometriosis (p < 0.001) but no difference in women with stage I–II endometriosis.
Summary of COS parameters for GnRH-agonist and GnRH-antagonist COS protocols in women with endometriosis.

COS, controlled ovarian stimulation; Hx, history; IQR, interquartile range; SD, standard deviation.
Gonadotrophin dose
In the majority of the papers reviewed, there were no significant differences in the total gonadotrophin dose (IU) required for COS treatment between the two protocols (see Table 8). Drakopoulos et al. 14 reported that both women with stage I–II and stage III–IV endometriosis required a greater gonadotrophin dose when using the long GnRH-agonist protocol (p < 0.001) as opposed to the GnRH-antagonist protocol. Ruggerio et al. 17 also found that the gonadotrophin dose between the two protocols was greater in the agonist arm (p = 0.05) when observing women with stage III–IV endometriosis. Whereas two studies that only included women with resected endometriomas found no difference in gonadotrophin dose between the protocols.13,15
Pabuccu et al. 19 reported the amount of gonadotrophin used by the number of recombinant follicle-stimulating hormone (FSH) ampoules and no significant differences were observed in women with stage I–II endometriosis, resected endometriomas or active endometriomas.
Adverse ART cycle outcomes
The risk of developing OHSS was not explicitly reported as an outcome in any of the studies. The miscarriage rate was reported by three studies but there was no significant difference between the outcomes of the GnRH-agonist or antagonist protocols17,19,20 (see Table 9). Pabuccu et al. observed no significant difference between the two protocols in the miscarriage rate in women with stage I–II endometriosis, resected endometrioma or active endometrioma. Interestingly, this study included the total number of cycle cancellations due to the risk of developing OHSS or insufficient ovarian response but did not specify how the cancellations were distributed between the two protocols nor were p-values specified. 19 Three papers measured the cycle cancellation rate in patients taking these two protocols and found that cycles were cancelled due to a variety of reasons, including insufficient ovarian response, risk of ovarian hyperstimulation, elevated progesterone levels and a low number of oocytes or embryos.17,18,20 Of these three studies, all found that the cancellation rate did not differ significantly between the two protocols.
Summary of adverse ART outcome data for GnRH-agonist and GnRH-antagonist COS protocols in women with endometriosis.

All values shown as percentage (absolute number).
AMH, anti-Müllerian hormone; CCR, cycle cancellation rate; DE, deep endometriosis; ET, embryo transfer; Hx, history; MR, miscarriage rate; NS, not statistically significant.
Discussion
Main findings
Most studies found comparable clinical pregnancy and live birth rates between the long GnRH-agonist and GnRH-antagonist ovarian stimulation protocols. This is similar to that of women in the general IVF population and poor ovarian responders.21–23 In addition, fertilization rates were similar although the long GnRH-agonist protocol might be beneficial for some women with specific endometriosis subtypes and those with low ovarian reserve.
When comparing COS parameters, the GnRH-agonist protocol generally required greater gonadotrophin dose and longer treatment duration although this did not always reach significance. Adverse ART outcomes such as cycle cancellation rate and miscarriage rate were similar between the two protocols. The direct risk of developing OHSS could not be assessed because data regarding OHSS were not reported in these studies.
Interpreting pregnancy and LBRs
How pregnancy and LBRs are reported in studies is important to consider when discussing ART outcomes with patients. Since the number of embryos retrieved could be a predictive factor for pregnancy rate, 24 excluding the patients who do not have a sufficient ovarian response by calculating the CPR per ET cycles13,17,18 would result in higher CPR as demonstrated by Kolanska et al. 20 Future studies may consider reporting both CPR per cycle initiation and CPR per ET cycle as it provides better comparability between studies and more accuracy when discussing the chance of pregnancy at each stage of ART. Two multivariate regression analyses13,18 also identified the number of embryos and maternal age as predictive factors for IVF success which has been previously reported. 25
Biological exploration
The precise mechanism by which GnRH analogues affect extra-pituitary reproductive tissues remains a topic of ongoing debate. Although most studies found no significant difference in CPR/LBR,13,15–20 Kolanska et al. 20 were the only study to analyse both fresh and freeze–thaw cycles and found that the long GnRH-agonist protocol led to a significantly higher pregnancy rate in patients with endometriosis regardless of subtype. The authors suggested that this difference may be explained by the action of GnRH antagonists on the endometrium rather than ovaries which is in line with previous studies. In 2006, Ruan et al. using an IVF mice model compared GnRH-agonist versus GnRH-antagonist COS protocols and found that the expression of two uterine receptivity biomarkers (integrin β3 and leukaemia-inhibitory factor) during the implantation window was significantly lower in the GnRH-antagonist group. This correlated with a significantly lower implantation rate. 26 A later case-control study in 2008 evaluated another receptivity marker, homeobox A10 (HOXA10) expression, from human endometrial biopsies and found decreased stromal and glandular cell HOXA10 expression in the GnRH-antagonist group. 27 Although laboratory studies have found that the GnRH-antagonist protocol can reduce endometrial receptivity, in the clinic, pregnancy and birth rates in endometriosis patients are similar between both protocols13–20 and this is in agreement with meta-analyses that include poor and normal ovarian responders who have other causes of infertility.9,21,22,28
Laboratory studies have also found that the GnRH-antagonist protocol may lead to a poorer follicular microenvironment (higher nitric oxide concentration, increased superoxide dismutase expression and decreased insulin growth factor 1 and 2)29,30 which could impact oocyte yield. However, this is not necessarily reflected in human studies. Trials in women from other IVF populations comparing long GnRH-agonist protocols with GnRH-antagonist protocols report mixed findings on total and mature oocyte yield. In the general IVF population, the long GnRH-agonist may yield a higher number of oocytes, CPR and LBR.9,13 Meanwhile, in women with polycystic ovary syndrome who have a poor ovarian response, meta-analyses have shown that there is no significant difference in the total number of oocytes and mature oocytes retrieved.9,22 Our review found heterogeneous results among endometriosis patients similar to the results from meta-analyses on other infertile IVF populations. This demonstrates the variable effects of GnRH analogues on the ovaries.
While the well-known benefit of the GnRH-antagonist protocol is a reduced dosage of exogenous gonadotrophins required for ovarian stimulation, this may do more harm than good, especially in patients with a history of ovarian endometriomas. A comparative study by Al-Azemi et al. 31 found that the presence of endometriomas significantly diminished ovarian reserve. Moreover, the surgical techniques during endometrioma cystectomy could damage the surrounding healthy ovarian tissue and vasculature increasing gonadotrophin resistance and negatively impact ovarian reserve. 32 Hence, women with endometriomas usually require higher doses of recombinant FSH during ovarian stimulation due to a poorer ovarian response. Since the GnRH-agonist protocols are associated with higher gonadotrophin doses and longer COS duration, this may be advantageous for women with ongoing or resected endometriomas15,19 or with diminished ovarian reserve.
Fertilization rate as a marker for ART success
Fertilization rate is defined as the number of 2 pronuclear (2PN) oocytes that contain genetic information from both sperm and egg divided by the number of inseminated oocytes. Interestingly, fertilization rate has not been included in prior analyses comparing these two COS protocols. However, it can be a valuable parameter for women considering embryo cryopreservation since it can be a marker for cumulative pregnancy rate.10,33 Furthermore, higher fertilization rates can be an independent predictor for implantation rates. This is relevant when deciding the number of embryos to transfer, which is often problematic for IVF/ICSI providers.34,35 Although the fertilization rates of the two protocols were generally no different, this may be due to the selection of higher quality (mature) oocytes for fertilization. Therefore, the higher number of mature oocytes available for fertilization with the long GnRH-agonist protocol in conjunction with having a similar fertilization rate results in an increased cumulative pregnancy rate.
Selecting a GnRH analogue for ovarian stimulation
ART is an expensive treatment and the cost should be considered especially when ART is not subsidized or covered by insurance. A recent cost-effectiveness analysis comparing GnRH-agonist and GnRH-antagonist COS in the general IVF population by Jing et al. found that the GnRH-antagonist protocol is economically advantageous per fresh embryo cycles due to the shorter treatment duration, lower gonadotrophin dose required and lower incidence of OHSS. However, the cumulative ongoing pregnancy rate in both fresh and frozen embryo cycles is higher with the GnRH-agonist protocol due to the higher number of oocytes retrieved. 36 Furthermore, the significantly shorter treatment duration with the GnRH-antagonist protocol would require fewer injections and lead to reduced treatment cost. Although most studies in our review found no significant differences in pregnancy or birth outcomes between the two protocols, the long GnRH-agonist protocol may still be favoured especially in patients with a history of ovarian endometriomas or diminished ovarian reserve. Thus, a patient-tailored approach should be sought, incorporating the patient’s disease characteristics and reproductive goals as a priority. As mentioned, the risk of developing OHSS could not be assessed due to the lack of available evidence and should be explored in future studies.
Strengths and limitations
To our knowledge, this is the first systematic review comparing ART outcomes following COS using the long GnRH-agonist protocol versus the GnRH-antagonist protocol specifically for women with endometriosis in accordance with PRISMA guidelines. Two authors (K.K.W.K. and S.O.) screened all the titles and completed bias/study quality assessment increasing the strength of our methodology. Several databases were searched without date restrictions minimizing the risk of selection bias. Authors were also sought for additional data and were provided by Drakopoulos et al. 14
The single RCT and relatively small number of studies were the main limitations for this review. In addition, the small study numbers and heterogeneity of endometriosis stages/subtypes in each study did not allow for meta-analysis as one must consider the varying structural changes to the female reproductive anatomy. Due to the nature of observational studies, selection of endometriosis patients to either the GnRH-agonist or GnRH-antagonist protocol may be influenced by the clinician’s preferences. Fertility centres have also gained more experience with the GnRH-antagonist protocol throughout the years and an updated RCT would be preferred to minimize selection bias.
Conclusion
This systematic review compared the long GnRH-agonist and GnRH-antagonist ovarian stimulation protocols and found similar CPRs and LBRs. However, the cumulative pregnancy rate may favour the long GnRH-agonist protocol due to the higher number of retrieved oocytes available for subsequent embryo cryopreservation. Women with ovarian endometriomas or poor ovarian reserve may benefit from the GnRH-agonist protocol due to greater gonadotrophin exposure resulting in an improved ovarian response. The GnRH-antagonist protocol is a sensible option for women with endometriosis, who want to lower the costs and duration of treatment. The risk of developing OHSS in endometriosis patients specifically could not be assessed and this outcome should be reported as a priority in future studies. A larger, well-powered RCT analysing patients according to endometriosis stage/subtype is needed. Ultimately, this review’s findings could help clinicians make an evidence-based decision when choosing a GnRH-analogue ovarian stimulation protocol while balancing treatment costs, stage/subtype of endometriosis and pregnancy goals of their patients.
Supplemental Material
sj-docx-1-tae-10.1177_20420188231173325 – Supplemental material for Comparing ART outcomes in women with endometriosis after GnRH agonist versus GnRH antagonist ovarian stimulation: a systematic review
Supplemental material, sj-docx-1-tae-10.1177_20420188231173325 for Comparing ART outcomes in women with endometriosis after GnRH agonist versus GnRH antagonist ovarian stimulation: a systematic review by Kevin K.W. Kuan, Sean Omoseni and Javier A. Tello in Therapeutic Advances in Endocrinology and Metabolism
Supplemental Material
sj-docx-2-tae-10.1177_20420188231173325 – Supplemental material for Comparing ART outcomes in women with endometriosis after GnRH agonist versus GnRH antagonist ovarian stimulation: a systematic review
Supplemental material, sj-docx-2-tae-10.1177_20420188231173325 for Comparing ART outcomes in women with endometriosis after GnRH agonist versus GnRH antagonist ovarian stimulation: a systematic review by Kevin K.W. Kuan, Sean Omoseni and Javier A. Tello in Therapeutic Advances in Endocrinology and Metabolism
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.