
Abstract
Purpose:
Lower extremity amputation resulting from diabetic foot ulcer, with neuropathic and/or ischemic etiologies, remains a devastating and costly complication of diabetes mellitus. This study evaluated changes in care delivery of diabetic foot ulcer patients during the COVID-19 pandemic. A longitudinal assessment evaluating the ratio of major lower extremity amputation to minor lower extremity amputations after implementation of novel strategies to combat access restrictions was compared to the pre-COVID-19 era.
Methods:
The ratio of major to minor lower extremity amputation (i.e. the high-to-low ratio) was assessed at two academic institutions, the University of Michigan, and University of Southern California, in a population of patients with diabetes who had direct access to multidisciplinary foot care clinics in the 2 years prior to the pandemic and the first 2 years of the COVID-19 pandemic.
Results:
Patient characteristics and volumes including patients with diabetes and those with a diabetic foot ulcer were similar between eras. In addition, inpatient diabetic foot-related admissions were similar, but were suppressed by government shelter in placed mandates and subsequent COVID-19 variants surges (e.g. delta, omicron). In the control group, the Hi-Lo ratio increased every 6 months by an average of 11.8%. Meanwhile, following STRIDE implementation during the pandemic, the Hi-Lo ratio reduced by (−)11% (p < 0.001) and doubled limb salvage efforts as compared to the baseline era. The reduction of the Hi-Lo ratio was not influenced significant by patient volumes or inpatient admissions for foot infections.
Conclusion:
These findings signify the importance of podiatric care in the at-risk diabetic foot population. Through strategic planning and rapid implementation of at-risk diabetic foot ulcer triage, multidisciplinary teams were able to maintain accessible care during the pandemic which resulted in a reduction of amputations. Furthermore, this manuscript highlights the value of the Hi-Lo ratio as an indicator of institutional limb salvage efforts.
Introduction
Although opponents on the field, the University of Michigan (UM) and the University of Southern California (Keck USC) saw similar challenges for diabetic limb salvage during the pandemic. The rapid explosion of the COVID-19 pandemic required a sudden shift in best care practices for health care providers and institutions requiring new plans of unprecedented complexity. Patients with diabetes mellitus (DM) and diabetic foot ulcer (DFU), who normally required frequent DFU care and debridement during face-to-face visits, were severely impacted by initial government shelter in place order which required social distancing to curb the spread of COVID-19 and preserve personal protective equipment (PPE).1,2 The subsequent reduced access to timely necessary care was hypothesized to be counterproductive to available limb salvage efforts. With the end of the initial government shelter in place orders came a new era in limb salvage informed by innovative practices born out of necessity at the beginning of the pandemic.3–6
Many of these strategies remained in place after shelter in place orders were lifted, including the ‘STRIDE protocol’ at UM 7 and a full service limb-preservation program at Keck USC At Keck USC, the limb-preservation program was implemented in 2018 for all diabetic tissue loss. A team-based approach was utilized from acute care settings to remission centers for evaluation of ulcerations after healing. 8 While initial data from both centers was encouraging,5,7 longitudinal data evaluating the benefits of these new limb salvage strategies was lacking.
It has been previously published that a high-to-low amputation ratio (Hi-Lo) is a practical measurement of limb salvage rates in a given population.9,10 The ratio is defined as the rate of major lower extremity amputation (LEA) divided by the total number of minor LEA. 9 Wrobel et al. described distal foot amputations as minor LEA and below-knee and above-knee amputations as major LEA. Intuitively, as this ratio increases (i.e. is greater than one), where the numerator is equal to or greater than the denominator, then limb salvage efforts are not sufficient. 9 To the contrary, when limb salvage efforts improve, and major LEA are being avoided, the ratio approaches the asymptote of zero and indicates greater limb salvage. 9 This ratio is particularly beneficial because it is a simple unitless measurement of an institution’s limb salvage efforts at any given time and permits further insight into care delivery across the continuum of disease
The longitudinal care of individuals with DFU during the pandemic marked an interesting juxtaposition with pre-pandemic methods of limb salvage. The use of virtual care, telephonic intervention, and rapid outpatient triage changed the approach to diabetic limb salvage. After implementation of various strategies to combat restricted access caused by the worldwide pandemic, we examined the counts and rates of major and minor amputation, in additional to the Hi-Lo ratio, from March 2020 to March 2022. This was compared directly with the immediate 2 years prior, when pandemic strategies where not in place (control) and when all DFU care was provided in a face-to-face setting.
Materials and methods
An observational cohort analysis was performed at our institutions of LEA from March 2018 to March 2022 by any provider. The period from March 2018 through February 2020 represented standard operating procedure during non-pandemic times. March 2020 through February 2022 represented standard operating procedure during the COVID-19 pandemic. Each period was assessed in 6-month intervals to account for seasonal variation and to assess impact of local shelter in place mandates (e.g. Michigan Executive Order 2020-21 and California Executive Order N-33-20 2020). All patients who had type 1 or type 2 DM and underwent a non-traumatic LEA from a DFU classified by University of Texas (UT) system, 11 were included. Institutional Review Board approval was received.
Patients with DM were identified by having a diagnosis code (ICD – DM 357.2x, 362.x, 648.0x, 250.xx, or 366.41) on at least two outpatient visits or one emergency department visit or one inpatient stay evaluation and management (E/M) code. 12 We excluded traumatic amputations. 13 We defined major LEA as transtibial or transfemoral (CPT 27880, 27590, and 27882, respectively). Minor amputations were defined as toe, ray resection, transmetatarsal, and midfoot (Chopart’s) amputation (CPT 28820, 28825, 28810, 28805, and 28800, respectively). Similarly, patients with DM with a DFU were identified using a combination of ICD-9/10 coding for DFU with and without a debridement procedure (CPT 97597/8 and 11042-5). We then evaluated the numerators, which described the total number (n) of major amputations. The denominator described the total number (n) of minor amputations for a given period. The numerator was divided by the denominator for a given period to create a Hi-Lo ratio of major LEA to minor LEA. This number was then evaluated for the defined periods.
We utilized two data sources to confirm amputation counts and calculate Hi-Lo ratio: DataDirect 14 and provider billing and Common Procedural Terminology (CPT) coding. DataDirect, software developed by the UM Medical School Office of Research facilitates cohort discovery; it is a self-serve electronic data repository. Following compilation of publicly available data, statistical analysis was performed.
Statistical analysis consisted of the calculation of the Hi-Lo ratio for a given 6-month period. The Hi-Lo amputation ratio was computed for each 6-month period by dividing the major amputation rate by the minor amputation rate. The ratio is reported as a unitless measurement. Secondarily, the Pearson correlation coefficient (r) was used to evaluate the direction and strength of association, if any, between variables. All statistical analysis was completed using SPSS statistical software, version 22 (SPSS Inc., Chicago, IL). Statistical significance was set at the 5% level (p ⩽ 0.05).
Results
Patient population
Patient characteristics between the two eras were similar by age, sex, body mass index, diabetes type (% type 1), and comorbid burden as assessed via Charlson Comorbidity Index (CCI) (p > 0.05). A higher percentage of individuals presented with more ischemic DFU in the control era (25.3%) while more missing data occurred during the pandemic (Table 1). Patient volumes, including those presenting for care of DM and/or DFU, was reduced by the COVID-19 pandemic. The average number of patients seen every 6 months at UM pre-pandemic was 427,268 ± 10,340 and was 377,290 ± 29,900 during the pandemic (p < 0.05). Similarly, the number of patients with diabetes presenting for care at the UM was reduced from 68,987 ± 1,285 to 54,438 ± 5,257 before and after the start of the pandemic, respectively (p < 0.05).
Patient Characteristics during the defined periods.
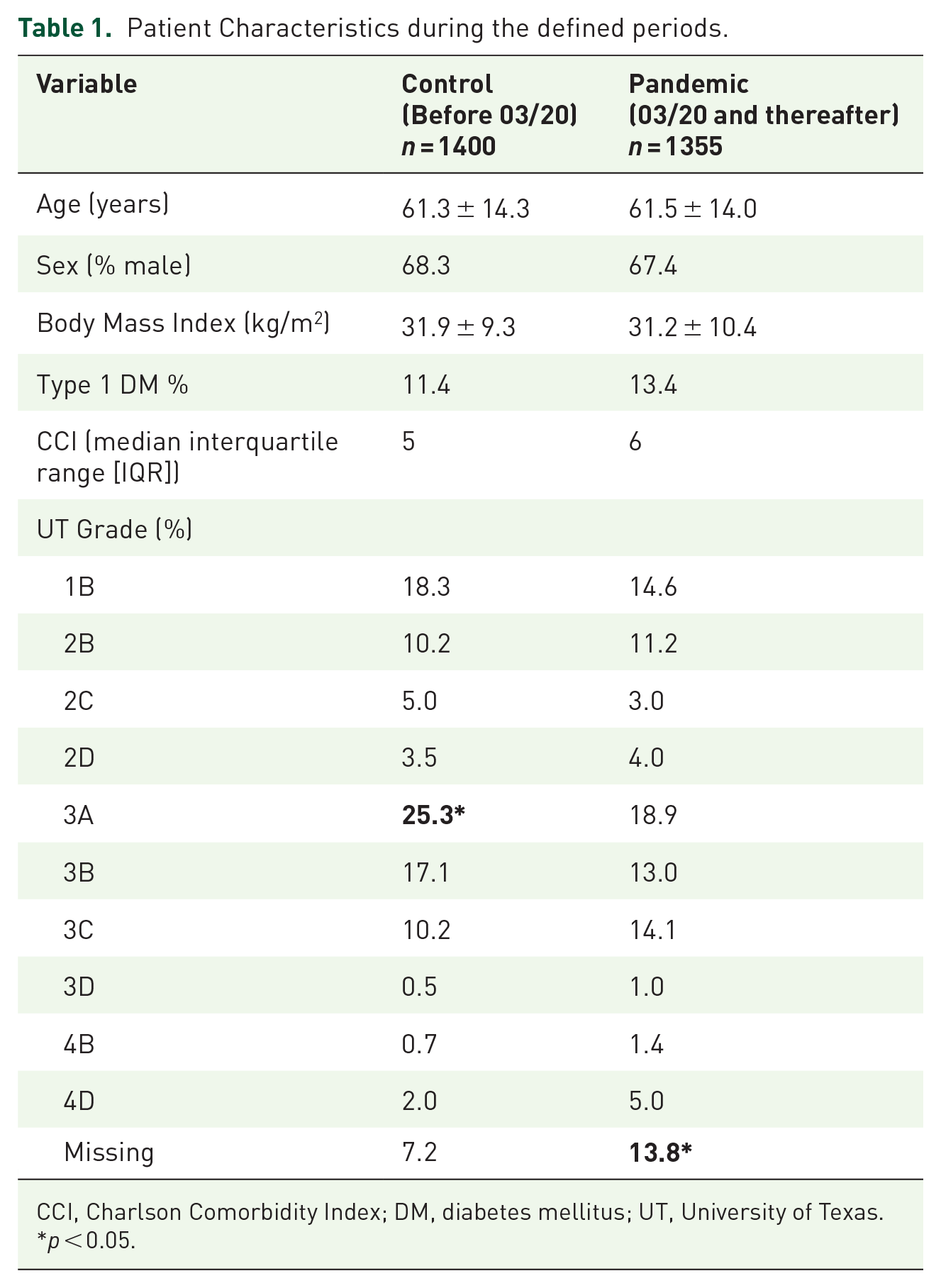
CCI, Charlson Comorbidity Index; DM, diabetes mellitus; UT, University of Texas.
p < 0.05.
Although fewer patients with diabetes were being managed at UM during the pandemic, the average number of patient visits for patients with diabetes was not significantly different than prior to the pandemic (p > 0.10). In addition, the rate and counts of patients with diabetes, who also had a new DFU, did not change. Pre-pandemic new DFU occurrences ranged from 336 ± 9.4 in control group, while new DFU occurrences during the pandemic were approximately 296 ± 70.7 every 6 months (p > 0.10).
Inpatient volumes
Admissions at the institutions directly related to DFU and/or diabetic foot infections to fully account for contributions to the Hi-Lo ratio. As shown in Table 2, approximately 58.3 ± 10.7 diabetic foot–related admissions occurred monthly in the control cohort while 56.5 ± 12.1 admissions for foot infection occurred monthly during the pandemic era (p > 0.10). At the most restrictive period of shelter in place orders (March–August 2020), admissions for foot infections did not vary versus the control (51.2 ± 16.5 vs 53.3 ± 6.1; p = 0.79). In the immediately following 6 months (September 2020–February 2021), there was a significant increase in foot infection admissions as compared to the pre-pandemic era (61.8 ± 9 vs 50.2 ± 4.6, p < 0.05). As hospital operations continued to normalize (March 2021–August 2021), foot infection admissions again mirrored the control era (58.5 ± 11.8 vs 62.2 ± 11.6, p = 0.61). In the final 6 months of comparison (September 2021–February 2022), a significant suppression of foot infection admissions was demonstrated versus the control era (54.3 ± 5.2 vs 67.7 ± 8.6; p < 0.05).
Diabetic Foot–Related Admissions by month during control and pandemic periods (2018–2022).

At Keck USC, there was a significant decline in the number of DFU-related admissions. Increases in transfers from our aortic center and transplant teams were noted. Patients with diabetic foot infections were directed to other facilities and locations with emergency rooms. Numbers normalized to pre-pandemic levels after the shelter orders were lifted in at the end of 2021 and showed a decline with the omicron variant.
Foot infection admissions during the control era were not associated with DM patient encounters (r = 0.87; p > 0.05), counts of DFU patients (r = 0.81; p > 0.05), but were strongly associated with overall hospital admissions (r = 0.95; p < 0.05). During the pandemic, foot infection admissions were not associated with overall hospital admissions (r = 0.17, p > 0.05) but were moderately and inversely associated with COVID-19 hospitalizations (r = –0.66; p < 0.001).
Hi-Lo ratio
The Hi-Lo ratio, following implementation of the STRIDE protocol at UM and maintenance of the limb salvage program at Keck USC, did not change significantly versus the control era. This included the longitudinal performance of major and minor amputations, regardless of amputation level (Figure 1). However, the rate of change of the Hi-Lo ratio was significantly different after implementation of the STRIDE protocol.
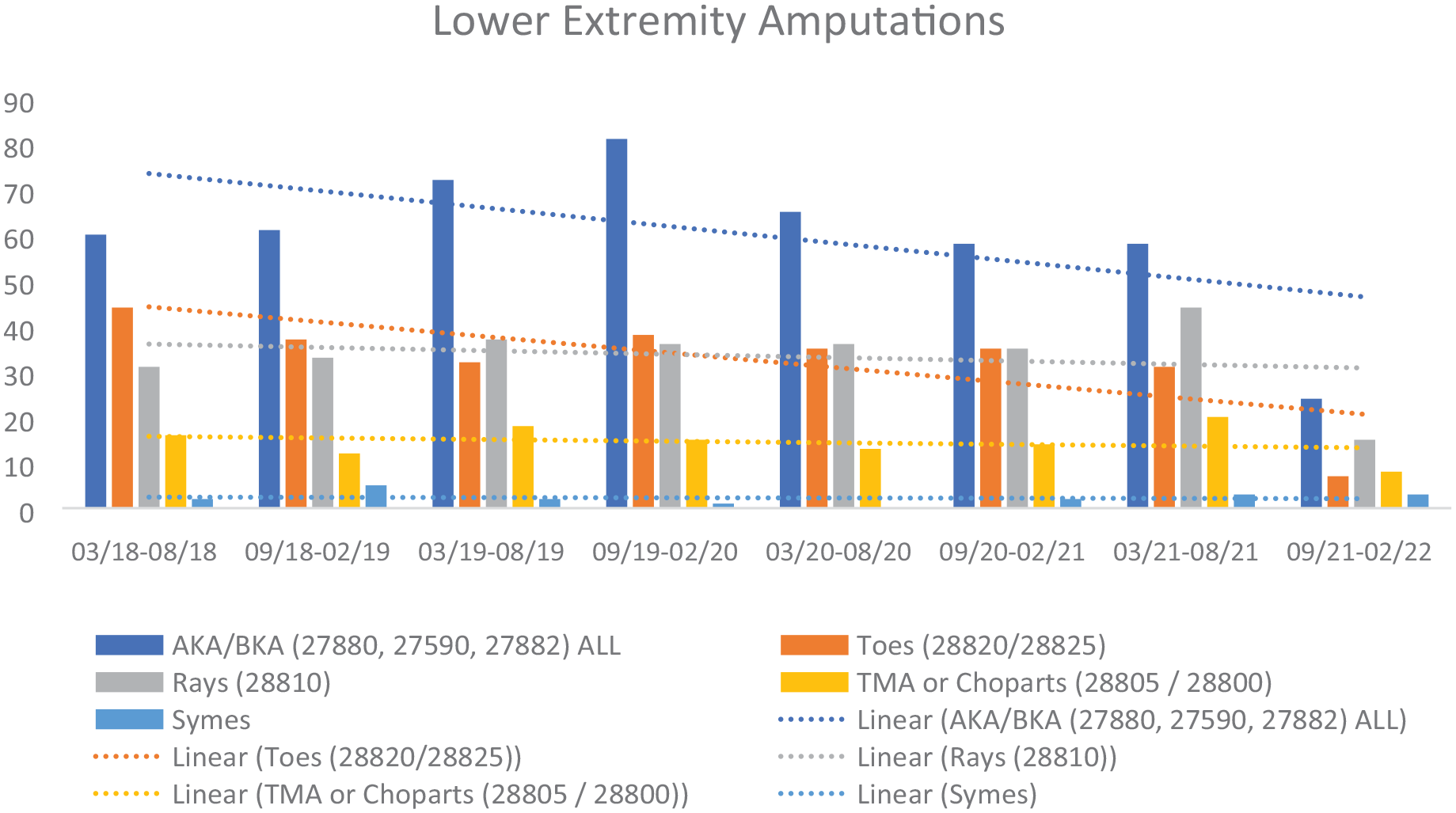
Lower extremity amputations before and during the COVID-19 pandemic.
In the control group, the Hi-Lo ratio increased every 6 months by an average of 11.8%. Meanwhile, following STRIDE implementation at UM, the Hi-Lo ratio reduced by (–)11% (p < 0.001), and doubled the rate of limb salvage at UM versus control.
At Keck USC, the Hi-Lo ratio showed a significant improvement after the implementation of the limb salvage program indicated a rate of 0.20. We were able to maintain this throughout this period until the last year (2021), where a sharp increase in the number of proximal amputations occurred between June 2021 and December 2021; a resultant Hi-Lo ratio of 0.67 (Table 3). Specifically, it was noted lower extremity vascular procedures were delayed because of the shelter in place orders in California.
Hi-Lo ratio at two institutions during the defined periods.

We then evaluated the associations between patient volumes and the Hi-Lo ratio. The association between patient volume changes and changes in Hi-Lo ratio was weak for (1) the general population (r = 0.12; p = 0.793), (2) patients with diabetes (r = 0.16; p = 0.735), and (3) patients with new DFU (r = 0.16, p = 0.221). In addition, the variation of foot infection admissions did not correlate with Hi-Lo ratio changes (r = 0.48, p = 0.23). Thus, there was no increase in amputation count(s) or rate of (any level) amputation in patients with DM during the pandemic (p > 0.10).
Discussion
The pandemic was a difficult period for individuals with DM and DFU. We hypothesized that restricted access would result in worsened outcomes. Initial data during government shelter in place orders demonstrated a reduction of elective procedures, emergency care, and non-essential services, including limb salvage efforts.3,5,7,15 UM saw an approximate 11.7% and 21.1% average reduction in total patient encounters and encounters for patients with diabetes, respectively, versus the control era (p < 0.05). In fact, there was no increase in the amount of new DFU or the proportionality of DFU patients during this period as well (both p > 0.05). This was like reported data from other academic centers nationally and internationally.3,5,7,15
We demonstrated the effect COVID-19 had on inpatient hospitalizations for patients with diabetic foot-related admission. Trends throughout each 2-year period were similar in terms of patient-, wound characteristics (Table 1), and average number of diabetic foot–related admissions (Table 2), but there were differences in the 6-month eras when hospital activity was affected by government shelter in place orders and the number of daily hospitalized COVID-19 patients. The former was demonstrated to cause a (relative) spike in foot infections once orders were lifted or relaxed. Meanwhile, the latter moderately suppressed (r = –0.65, p < 0.001) inpatient admissions of foot infection.
Institutional data on the average Hi-Lo ratio in each era demonstrated a similar rate of limb salvage (0.76 vs 0.69; p > 0.05). First, in the 2 years prior to the pandemic, there was a decreased rate of limb salvage (i.e. more amputations) that was disparate with previously longitudinal data observed in a previous retrospective study.10,16 In stark contrast, once the pandemic began, triage was altered to place greater strategic emphasis on the identification of and targeted care of individuals with the highest risk feet. This resulted in an
Because of institutional strategic change in the delivery of healthcare for individuals with DFU, the rate of Hi-Lo change reduced by 11% on average compared to the control era. The reduction in patient volumes, both overall and for patients with diabetes, did not account for the significant reduction in the rate of change of the Hi-Lo ratio (increased limb salvage). In addition, the rate of change of the Hi-Lo ratio fell during each 6-month period assessed, indicating longitudinal progress despite the pandemic. It underscores the high utility of the Hi-Lo ratio to inform an institution about the effectiveness of their limb salvage program(s). Also, it has dual function to serve as a research tool to evaluate inter-institutional practices as we demonstrate.
This study is not without limitations. First, definitive conclusions about limb salvage efforts cannot be drawn until the COVID-19 historical era ends. Second, we did not account for rates of additional limb salvage interventions (e.g. lower extremity revascularization) in this study. Based on strict inclusion diagnoses for this study and use of UT wound grading, we demonstrated similar patient- and wound characteristics in both eras. Third, the pandemic era resulted in a greater percentage of missing data as it pertains to classification of wounds. This was deemed not critical as the Hi-Lo ratio is an inclusive measure of all limb salvage efforts and accounts for variation in performance of system-based intervention strategies. Thus, the Hi-Lo ratio accurately represented the amputation counts and rates during the defined periods as planned. Future studies should assess these newly adopted limb salvage strategies to determine which are the most effective at preventing limb loss.
In conclusion, the outbreak of the COVID-19 pandemic strained medical facilities, providers, and patients alike. In DFU care, novel strategies were developed, implemented, and executed to maintain high levels of access for those at risk of limb loss. The longitudinal changes in the Hi-Lo ratio emphasized this approach and demonstrated the effectiveness of limb salvage efforts during the pandemic. These strategies have continued to be successful despite successive COVID-19 variant surges.