
Abstract
Aims:
Patients’ adherence to using knee-high offloading treatment is critical to effective healing of diabetes-related foot ulcers (DFUs). Previous studies have found that patients generally have low adherence to using removable knee-high offloading treatments, yet no study has investigated whether their adherence differs during daytime and nighttime. This study aimed to investigate the levels and factors associated with adherence to using knee-high removable cast walker (RCW) treatment during daytime and nighttime weight-bearing activities in people with DFUs.
Methods:
This was a secondary analysis of data collected from a multi-centre cross-sectional study investigating adherence to using knee-high RCWs among 57 participants with DFUs. All participants had multiple socio-demographic, physiological and psychosocial factors collected, before having their adherence to using RCWs during weight-bearing activity monitored over a 1-week period using the dual activity monitor method. Adherence data were categorised into daytime (06:00–18:00) and nighttime (18:00–06:00) periods and calculated separately. Multiple linear regression was used to identify factors associated with daytime and nighttime adherence.
Results:
Mean adherence to using RCW during weight-bearing activities in people with DFUs was higher during daytime compared with nighttime [39.9% (SD = 18.9) versus 20.4% (SD = 16.7), p < 0.001]. Factors independently associated with lower adherence during daytime were being male, longer diabetes duration, not having peripheral artery disease (PAD), and higher perceived RCW heaviness. Factors associated with lower adherence during nighttime were higher mean daytime steps, not having retinopathy and having dyslipidaemia.
Conclusions:
Adherence to using RCWs during weight-bearing activities reduced significantly at nighttime compared with daytime among people with DFUs, and this was associated with different factors. Interventions to improve adherence, in research and clinical practice, should incorporate methods to target daytime or nighttime adherence specifically.
Introduction
Diabetes affects ~530 million people around the world and is expected to affect ~780 million by 2045. 1 Diabetes-related foot ulcers (DFUs) affect around ~20 million people and are the leading cause of global amputations and global diabetes disability burden.2–4 DFUs usually take months to heal and require intensive treatments to try and prevent hospitalisation, amputation and even death.2,5–9
Offloading treatment is essential to heal DFUs6,10 by reducing the high plantar pressure that causes the development of DFUs in the first place. 11 Non-removable knee-high offloading devices, such as total contact cast (TCC), and removable knee-high offloading devices, such as removable cast walkers (RCWs), have been shown to be the most effective offloading treatments at reducing plantar pressure, reducing around 90% of plantar pressure. 12 Thus, guidelines strongly recommend that non-removable knee-high offloading devices should be the first choice of offloading treatment, but if contraindicated or not tolerated, then removable knee-high offloading devices are recommended as the second choice of offloading treatment. 10 These recommendations are based on reviews finding a high quality of evidence that using non-removable knee-high devices results in healing more ulcers than removable knee-high devices or other offloading treatments.13–15 Yet, the only obvious functional difference between non-removable and removable knee-high offloading devices is the ability of patients to remove the device, which can lead to lower adherence to using these removable devices. 16 Furthermore, the use of TCC has been found to be relatively low in routine clinical practice due to barriers related to ease of use, material cost, and patients’ satisfaction, with surveys suggesting <10% of patients receive TCCs, whereas >15% of patients receive RCWs and the rest typically another similar removable offloading device.17–20
Several studies have shown that people with DFUs adhere to using their RCW treatment for around 30–60% of their daily weight-bearing activity or necessary treatment time.16,21,22 Factors found to be associated with low RCW adherence include male gender, longer diabetes duration, absence of peripheral artery disease (PAD), larger DFU size, postural instability and perceived heavier RCWs.16,22 While these studies all used recommended dual activity monitor methods to measure adherence levels, they reported averaged daily adherence levels across weeks,16,21,22 with none investigating whether there were differences in adherence during different parts of the day or night.
A recent qualitative study reported patients with DFUs stated that they mostly used their RCWs during daytime activities and removed their RCWs during nighttime activities, such as walking inside the home, bathing and sleeping. 23 Similarly, patients with a history of DFUs using custom-made footwear to prevent DFUs were found to have much higher adherence levels to using their footwear outside the home during the daytime than inside the home during nighttime. 24 These findings suggest that there may be important differences in adherence levels and factors associated during daytime and nighttime periods for people with DFU using RCWs. Therefore, this study aimed to investigate the levels and factors associated with adherence to using RCW treatment during daytime and nighttime in people with DFUs.
Methods
Study design and settings
This was a secondary analysis of data collected from a multi-centre cross-sectional study investigating adherence to using knee-high RCWs among people with DFUs. 22 Data were collected from three main referral diabetes centres in Jordan: (1) the National Centre for Diabetes, Endocrinology and Genetics (NCDEG); (2) Jordanian Royal Medical Services (JRMS), and (3) Prince Hamza Hospital (PHH). Ethical approval was obtained from the Office of Research Ethics and Integrity at the Queensland University of Technology (QUT), Australia (Approval No.1900000418) and the Institutional Review Board Ethics Committee at each centre in Jordan: the NCDEG (No. 3266-9), JRMS (No. T/F3/1-12689) and PHH (No. MH/32/2527). The methodology has been described in detail elsewhere 22 and will be summarised below.
Participants and sample size
Eligible participants were adults who had diabetes (type 1 or 2), a plantar DFU and had been treated with a RCW for at least 4 weeks prior to recruitment. 22 Exclusion criteria included those unable to ambulate or with a history of cognitive impairment. 22 A sample of 60 participants was calculated as conservatively needed for the original study, 22 based on the assumptions of (1) including five factors in the final multiple linear regression model as was reported in the only previous similar adherence study, 16 (2) that 10 participants were needed for each included factor to not overfit the model as per statistical texts 25 and (3) allowing for a 5–10% drop-out rate as observed in other similar studies using similar activity monitors. 26
Data collected
Data collected were in the domains of socio-demographic, physiological and psychosocial factors. 22 Socio-demographic factors collected included age, gender, living arrangement, highest educational level, employment and family income. Physiological factors included diabetes type, diabetes duration, HbA1c, dyslipidaemia, end-stage renal failure, heart failure, hypertension, myocardial infarction, osteoarthritis, retinopathy, body mass index (BMI), daily steps (daytime and nighttime), peripheral neuropathy, PAD, foot deformities, previous amputations, DFU size, depth and infection. Psychosocial factors included the Foot Care Confidence Scale (FCCS), Foot Care Outcomes Expectations Scale (FCOES), Patient Interpretation of Neuropathy (PIN) scales, Neuropathy-Specific Quality of Life (NeuroQoL) scales, and Customised Adherence Offloading-Related scales. The definitions for all factors are outlined in detail elsewhere. 22
Outcome measures
The outcome of adherence to using RCWs was measured using a recommended dual activity monitor method. 27 In brief, participants were provided with two activity monitors (Fitbit Flex©) to measure their adherence during weight-bearing activity (steps), with one worn on the wrist and one attached to the offloading device. This method has been validated and used in previous similar studies,16,21,28 and has been recommended by international experts.27,29 The Fitbit Flex activity monitors have shown good criterion-related validity in comparison with observed steps [intra-class correlation coefficient (ICC) = 0.843, 95% confidence interval [CI]: 0.683–0.923), 30 excellent test–retest reliability (ICC = 0.79, 0.87, 95% CI: 0.57–0.90, 0.73–0.94) 31 and only 8% mean absolute random error. 32
Participants were instructed to wear the wrist monitor continuously for a 7-day period and were informed that the wrist and RCW monitors were to measure the number of steps people with DFU perform on average so as to conceal the primary reason for measuring adherence from participants. Otherwise, there were deliberately no other instructions provided to participants or their treating clinicians by the researchers on adherence to wearing the RCW so as to not interfere with participants’ adherence patterns.
At the conclusion of the 7-day period, the data from the two monitors were returned by participants, time-synchronised and transformed into activity units. 22 An activity unit was defined when the participant’s wrist activity monitor recorded any weight-bearing step activity during a 15-min period (e.g. there were a possible 96 potential activity units in each 24-h day). Participants were deemed to have been adherent to using their RCW during an activity unit if their RCW monitor recorded at least 50% of the steps recorded by the wrist monitor during that same 15-min period. The adherence data were then categorised into daytime and nighttime periods. Daytime was defined as the period from 06:00 to 18:00 h, and nighttime was defined as the remaining period of 18:00–06:00 h the next day. This was based on a previous adherence study 33 and the average sunrise time for the period in which participants were recruited from October 2019 to February 2020 for Amman (Jordan) between 05:46 and 06:46 and the average sunset time between 17:33 and 18:21. 34 Therefore, for each 24-h day, there were a total of 48 (15-min) weight-bearing activity units possible during daytimes, plus 48 activity units possible during nighttimes. The proportion of adherence for each participant was calculated as the recorded adherent weight-bearing activity units divided by the recorded weight-bearing activity units for the participant during the daytime period and nighttime period. 22 The adherence levels for the cohort were calculated as the mean [standard deviation (SD)] of the proportion of adherence for each participant during the daytime and nighttime periods.
Statistical analysis
All data were analysed using SPSS 21.0 for Windows (IBM Corp, Armonk, NY, USA). Descriptive statistics used to display factors included frequencies (proportions), mean (SD) and median [interquartile range (IQR)]. Paired-sample t-tests were used to examine the difference between the mean daytime and nighttime adherence outcomes. Simple linear regression was conducted to test the unadjusted associations between each factor and each outcome measured. All factors with an unadjusted association of p ⩽ 0.1 with an outcome were entered into the multiple linear regression model for that outcome, after excluding any factors with <8 subjects per factor (to reduce type 1 statistical error) 35 or displaying multicollinearity. Multicollinearity was defined as having a statistical significant association (p < 0.05) between any independent factors that were originally associated (p ⩽ 0.1) with the outcome. If multicollinearity was identified, the factor with least statistical significance with adherence, or in cases with similar statistical significance, the factor with least clinical causal plausibility was excluded. A backward stepwise method was used to eliminate non-significant factors that did not result in any significant change in the power of the model. Missing data were handled by excluding cases with missing data as missing data were minimal.
Results
Sixty-one participants were recruited for the original cross-sectional study. Four were excluded due to no adherence data being obtained [monitors fail to record any data (n = 2), refusal to wear the monitors (n = 1) and hospitalised before using the monitors (n = 1)]. Therefore, 57 participants [mean age, 56 years (SD = 10), 79% males, 95% type 2 diabetes] were included in this secondary analysis and their characteristics are displayed in Table 1.
Factors associated with daytime and nighttime adherence to using RCWs.
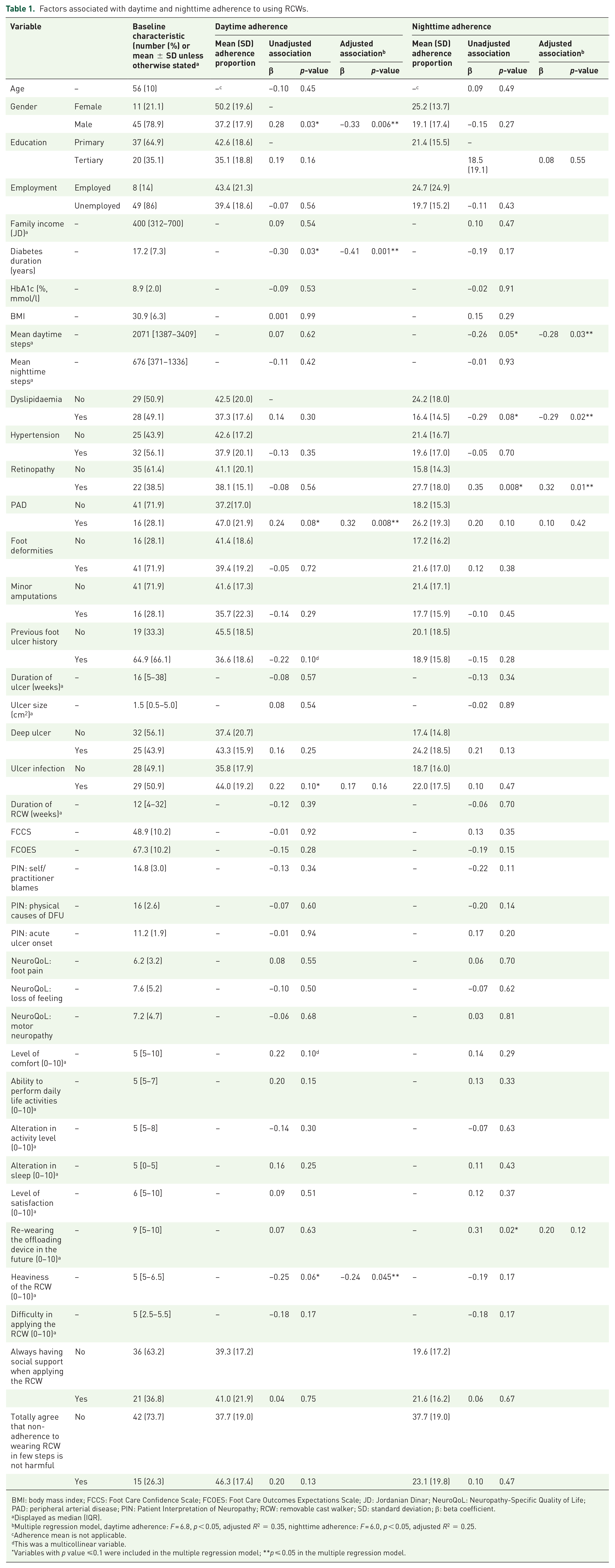
BMI: body mass index; FCCS: Foot Care Confidence Scale; FCOES: Foot Care Outcomes Expectations Scale; JD: Jordanian Dinar; NeuroQoL: Neuropathy-Specific Quality of Life; PAD: peripheral arterial disease; PIN: Patient Interpretation of Neuropathy; RCW: removable cast walker; SD: standard deviation; β: beta coefficient.
Displayed as median (IQR).
Multiple regression model, daytime adherence: F = 6.8, p < 0.05, adjusted R2 = 0.35, nighttime adherence: F = 6.0, p < 0.05, adjusted R2 = 0.25.
Adherence mean is not applicable.
This was a multicollinear variable.
Variables with p value ⩽0.1 were included in the multiple regression model; **p ⩽ 0.05 in the multiple regression model.
Of the daytime period, from a possible 48 (15-min) activity units, there was a daily mean of 25.2 (SD = 9.2) weight-bearing activity units, and of those, a daily mean of 9.8 (SD = 6.2) was recorded as adherent units. Of the nighttime period, from a possible 48 (15-min) activity units, there was a daily mean of 13.3 (SD = 5.5) weight-bearing activity units, and of those, a daily mean of 2.6 (SD 2.5) was recorded as adherent units.
The mean participant adherence level during the daytime period was 39.9% (SD = 16.5) and significantly higher than during the nighttime period [39.9% (SD = 16.5) versus 20.4% (SD = 16.7), p < 0.001].
Table 1 displays the unadjusted and the adjusted factors associated with both the daytime and nighttime adherence levels. After adjustment, the factors that were independently associated with lower daytime adherence were male gender, longer diabetes duration, not having PAD and perceived heavier RCW (all p < 0.05). The factors that were independently associated with lower nighttime adherence were higher mean daytime steps, not having retinopathy and having dyslipidaemia (all p < 0.05).
Discussion
In this secondary analysis, we investigated adherence levels to using RCWs during weight-bearing activities in people with DFUs during daytime and nighttime periods. We found significantly lower adherence levels during nighttime (~20%) than during daytime (~40%). Also, the factors associated with nighttime and daytime adherence were different. We found male gender, longer diabetes duration, not having PAD and perceived heavier RCW devices were independently associated with lower daytime adherence, whereas higher mean daytime steps, not having retinopathy and having dyslipidaemia were independently associated with lower nighttime adherence. Thus, there were differences in the levels and factors associated with RCW adherence depending on the time of day, and this suggests different methods to improve adherence should be targeted towards daytime or nighttime adherence in future.
Previous studies in people with diabetes-related foot disease have also shown differences in treatment adherence during different times of the day. For example, qualitative studies have found people with DFU prefer to use their removable knee-high offloading devices during the daytime and not use them during nighttime activities.23,36 Furthermore, a quantitative study on people at risk of DFU found adherence to using custom-made footwear was higher during daytime than nighttime periods. 24 One possible explanation for lower adherence during nighttime may be that people with DFU sub-consciously use their RCW as they use their everyday footwear, that is, they use them when outside the home during the daytime and remove them for activities traditionally performed inside the home during the nighttime. This may be partly explained by incorrect considerations by patients that their feet are protected from harm when inside the home, and that footwear or devices that are used outside the home are too dirty to use inside the home. 24 However, we can only infer this from the time periods we measured, as we did not specifically measure indoor and outdoor adherence. We, therefore, suggest future studies also take the locations of use (e.g. outside versus inside the home) into account when investigating adherence, and clinicians ensure they educate their patients that total adherence means using their RCW treatment for activities both outside of the home (typically during the daytime) and inside of the home (typically during the nighttime). Furthermore, we suggest adherence inside the home may also be improved and explored by designing RCWs for indoor activities or even providing RCW covers for inside the home, as has recently occurred with the development of indoor therapeutic footwear to prevent future DFU. 37
Although we found higher adherence levels to wearing RCWs during the daytime, daytime non-adherence still presents a major challenge to unoffloaded (or ‘unprotected’) activity considering the significantly higher weight-bearing activity recorded during the daytime in comparison with nighttime. This means while patients may have higher adherence during the daytime, they also have higher rates of activity during the daytime, and thus a higher total load of unprotected steps during the daytime which likely results in more overall repetitive plantar tissue stress on the DFU during the daytime than during the nighttime. 27 Thus, clinicians should consider both the different levels of weight-bearing activity along with adherence during the daytime and nighttime.
The factors we found associated with lower daytime adherence were, perhaps unsurprisingly, similar to the factors we originally found associated with overall adherence, as the majority of overall weight-bearing activity was performed during the daytime. Factors associated with lower adherence during daytime included male gender, longer diabetes duration, not having PAD and perceived heavier RCW. 22 As per our original study, 22 we hypothesise that this may be because males tend to perform fewer self-care activities than females, such as adhering to treatment, 38 and people with longer diabetes duration are likely to have to adhere to more self-care activities due to a more complex burden of diabetes, PAD may be indicative of more severe plantar DFU cases (and pain) that is likely to result in more benefit when adhering to RCW treatments, and heavier RCWs are likely to be more challenging to use. 22
Interestingly, however, we found different factors associated with lower nighttime adherence to using RCW, including higher mean daytime steps, having dyslipidaemia and not having retinopathy. First, the reasons for higher daytime steps associated with lower nighttime adherence may be similar to our earlier hypothesis that patients are somewhat ‘culturally accustomed’ to using their RCW as they do their everyday footwear. This may be even more likely in patients who are more active during the day, with RCWs that are much heavier than footwear. We, therefore, hypothesise that this may explain why active people are more likely to remove their RCW when they return from their outside activity and subsequently have lower nighttime adherence.21,23,36,39 Second, people with dyslipidaemia have been found to have lower adherence to their medications and dietary recommendations,40,41 and this might reflect their low adherence to wearing RCWs or perhaps this may be a chance finding in our cohort. Finally, our finding that people without retinopathy were associated with lower RCW adherence at nighttime may be that retinopathy is often also associated with more severe DFU cases 42 which can result in higher adherence, 24 or an alternative explanation could be that people with retinopathy require more support to apply their RCW and thus may prefer not to remove their RCWs at nighttime if that support is not available, resulting in higher adherence.
The results and interpretation of this study should be read cognisant of several limitations. First, there is a possibility that this secondary analysis may have been underpowered. However, the sample size calculations of our original study were based on sound sample size calculations, 22 and we also ensured that we excluded any factors with small numbers of events to account for this secondary analysis. Thus, we recommend studies with a larger sample size are undertaken to confirm our findings. Second, the cross-sectional design used in this study is not suitable to determine causality. Third, the 1-week period in which we measured adherence may not be representative of the adherence levels throughout the DFU healing period in which people use RCW treatment, although we only included people who had been prescribed RCW for at least 4 weeks. 43 Fourth, there is a possibility that participants did not wear the wrist activity monitors during some activities; 29 however, they were reminded daily to use their wrist monitor. Fifth, the activity monitors we used are valid and reliable to measure weight-bearing step activity; 44 however, these monitors do not measure standing weight-bearing activity and standing has been associated with DFU healing. 43 Sixth, although we measured adherence during daytimes and nighttimes and we inferred these to be more likely of outdoor and indoor activities, respectively, we did not measure if and when participants were inside or outside their home environment. Finally, this was a secondary analysis of data from an original cross-sectional study, and thus we have performed multiple statistical tests that increase the likelihood of type 1 statistical error. Thus, new and larger studies are required to confirm and externally validate our findings.
As this study has found different adherence levels during daytime and nighttime periods, and different factors that influence those levels, we suggest that when clinicians ask specifically their patients to self-report their RCW adherence, they do so by asking specifically for their RCW adherence during daytime and nighttime separately. If adherence differs, with likely lower adherence during nighttime, clinicians should consider using different interventions to improve adherence levels, depending on whether daytime or nighttime adherence is low. Furthermore, we recommend researchers consider developing novel interventions or specific strategies aimed at enhancing nighttime adherence to RCWs. These may consist of technological innovations, such as developing more nighttime indoor-friendly RCWs as has recently occurred for indoor custom-made footwear to prevent DFU, 37 or smart RCW offloading treatment that provides self-monitoring of adherence to enhance patients’ awareness of their non-adherence, and the times at which their non-adherence is highest. 45 Or these may consist of education and communication interventions. We deliberately did not interfere with the instructions provided by treating clinicians on the use of RCW in this study so as to better observe participants’ natural adherence patterns. Future research should investigate how education currently takes place, whether this affects adherence rates and whether different educational strategies on enhancing self-care activities, such as via motivational interviewing to discuss strategies to encourage patients to use their offloading devices more during nighttime activities, 46 may improve adherence. 47
Conclusion
We found that patients with plantar DFUs have different levels of adherence to wearing RCWs during daytime or nighttime weight-bearing activities, and different factors are associated with these levels. Adherence to using RCW treatment is low during the daytime and significantly lower at nighttime. This indicates that clinicians prescribing RCWs for patients with plantar DFUs need to be aware that already low adherence levels are even lower during nighttime activities. We suggest further efforts are needed to ensure that patients use their RCW treatment for all weight-bearing activities, including importantly at nighttime, to effectively promote DFU healing.
Footnotes
Acknowledgements
AA acknowledges the Australian government research training programme stipend (International) and QUT tuition fee sponsorship as this study has been undertaken in partial fulfilment of a Doctor of Philosophy. PAL also acknowledges support by an Australian National Health and Medical Research Council Early Career Fellowship (#1143435). The authors would like to especially acknowledge Ms Lee Jones (Statistician, QUT) for statistical advice.