
Abstract
Primary hyperparathyroidism (PHPT) is classically associated with both an elevated or ‘inappropriately normal’ parathyroid hormone (PTH) level and raised serum calcium. However, in clinical practice, increasing numbers of patients present with raised PTH but normal serum calcium, renal function and vitamin D; this is known as normocalcaemic PHPT (nPHPT). Studies investigating the clinical presentation of this condition have shown that patients may present with hypertension, nephrolithiasis, impaired glucose tolerance, osteoporosis and fragility fractures. The prevalence of such complications in nPHPT is similar to that in classical hypercalcaemic PHPT (hPHPT). Although the National Institute for Health and Care Excellence (NICE) have developed guidelines for the management of PHPT generally, a consensus is yet to be reached on the optimal management of nPHPT specifically. A review of the literature on parathyroidectomy in the treatment of nPHPT revealed that nPHPT patients were more likely to present with multi-glandular disease and significantly less nPHPT patients had an intra-operative PTH fall of >50% compared with those with hPHPT. These findings demonstrate that patients with nPHPT are more likely to receive bilateral neck explorations and require remedial surgery compared with hPHPT patients. Following surgery, improvements in bone mineral density (BMD) and renal stones are generally observed in those with nPHPT. Where surgery is not possible, medical management with alendronate has been shown to be effective in nPHPT patients. Given the higher incidence of multi-gland disease and greater possibility of remedial surgery in nPHPT, careful consideration of risks and benefits should be made on an individualised basis and surgery should be performed by surgeons experienced in four gland exploration.
Introduction
Primary hyperparathyroidism (PHPT) is an endocrine condition resulting from inappropriate parathyroid hormone (PTH) hypersecretion. 1 Traditionally, the biochemical profile of PHPT is elevated serum calcium (>2.6 mmol/l) with elevated or ‘inappropriately normal’ PTH that may result in multi-system complications, including fractures and nephrolithiasis.2,3 However, an increasingly common biochemical profile is of raised PTH in the context of normal serum calcium (total and ionised), vitamin D and renal function – recognised as normocalcaemic PHPT (nPHPT).1,4,5 This biochemical picture is largely being discovered in patients through osteoporosis screening. Whilst the reported prevalence of nPHPT varies significantly within the literature (0.1–8.9%), 6 a recent retrospective study of 6280 patients by Schini et al. reported a prevalence of 0.18%. 7
Pathophysiology
Several hypotheses have been proposed to explain the pathophysiology of nPHPT. A French study by Maruani et al. of 178 patients (34 normocalcaemic and 144 hypercalcaemic patients) identified less severe PTH hypersecretion in nPHPT patients compared with hypercalcaemic patients. 8 In addition to this, possible PTH target tissue resistance was hypothesised, which contributed to normocalcaemia in spite of the raised PTH. This was demonstrated by lower levels of bone resorption markers, lower plasma 1,25-dihydroxyvitamin D, decreased fasting urine calcium excretion and reduced renal tubular calcium reabsorption. Oestrogen has also been hypothesised as a potential mediator in reduced target tissue response, suggesting that oestrogen deficiency (as observed in menopause) would result in hypercalcaemia.2,8 However, nPHPT is most frequently discovered in postmenopausal women, the validity of this hypothesis has been questioned. 8
An alternative hypothesis proposed by Rao et al. suggests a biphasic process to evolution of PHPT – an initial subclinical stage of normocalcaemia, followed by a clinical stage of hypercalcaemia. 9 This sequential process therefore adds the implication that a proportion of those with nPHPT will progress to hypercalcaemic PHPT (hPHPT).
Natural history
There has been discussion as to whether nPHPT represents early disease prior to progression into overt hPHPT or is a separate entity associated with partial tissue resistance to PTH. Ultimately the evidence in this area is based on relatively small numbers of participants so that firm conclusions cannot be drawn on this issue. The condition tends to be defined by an adjusted calcium in the upper end of the normal reference range with elevated circulating PTH. Care needs to be taken to differentiate from other causes of elevated PTH, particularly associated with low normal adjusted calcium such as vitamin D deficiency, renal impairment, malabsorption and medications including anti-epileptics, loop diuretics and lithium. Šiprová et al. carried out a 6-year study that reported that 19% (n = 36) of 187 normocalcaemic patients became hypercalcaemic – the shift occurring within the first 2 years for 66.7% (n = 24) of patients. 10 This relatively early ‘conversion’ is supported by Silverberg and Bilezikian, with 13.6% of their nPHPT patients developing hypercalcaemia within 12 months. 11 Moreover, a recent study by Schini et al., which investigated the natural history of nPHPT patients over a 5-year period, found that 4 of the 11 identified nPHPT patients remained normocalcaemic 7 ; however, only 2 of these patients continued to exhibit persistently high PTH levels. The remaining seven patients progressed to display intermittent hypercalcaemia over the 5-year period.
Clinical presentation
Historically, patients with PHPT presented with symptoms of hypercalcemia, including constipation, fatigue and polyuria. 12 However, the clinical presentation of nPHPT patients is not as well established.
In their longitudinal cohort study of 37 patients with nPHPT, Lowe et al. revealed that 57% had osteoporosis and 11% experienced previous fractures. 13 Compared with hPHPT patients, studies have shown no significant difference in the incidence of both osteoporosis and fractures between nPHPT and hPHPT patients.14–17 However, a recent comparative prospective study by Gómez-Ramírez et al. found certain bone resorption markers (osteocalcin, P1NP and B-CTX) to be significantly lower in nPHPT patients compared with those with hPHPT, 18 which may be suggestive of reduced skeletal impact in this patient group (see Table 1).
A summary of the studies investigating the clinical presentation of nPHPT.
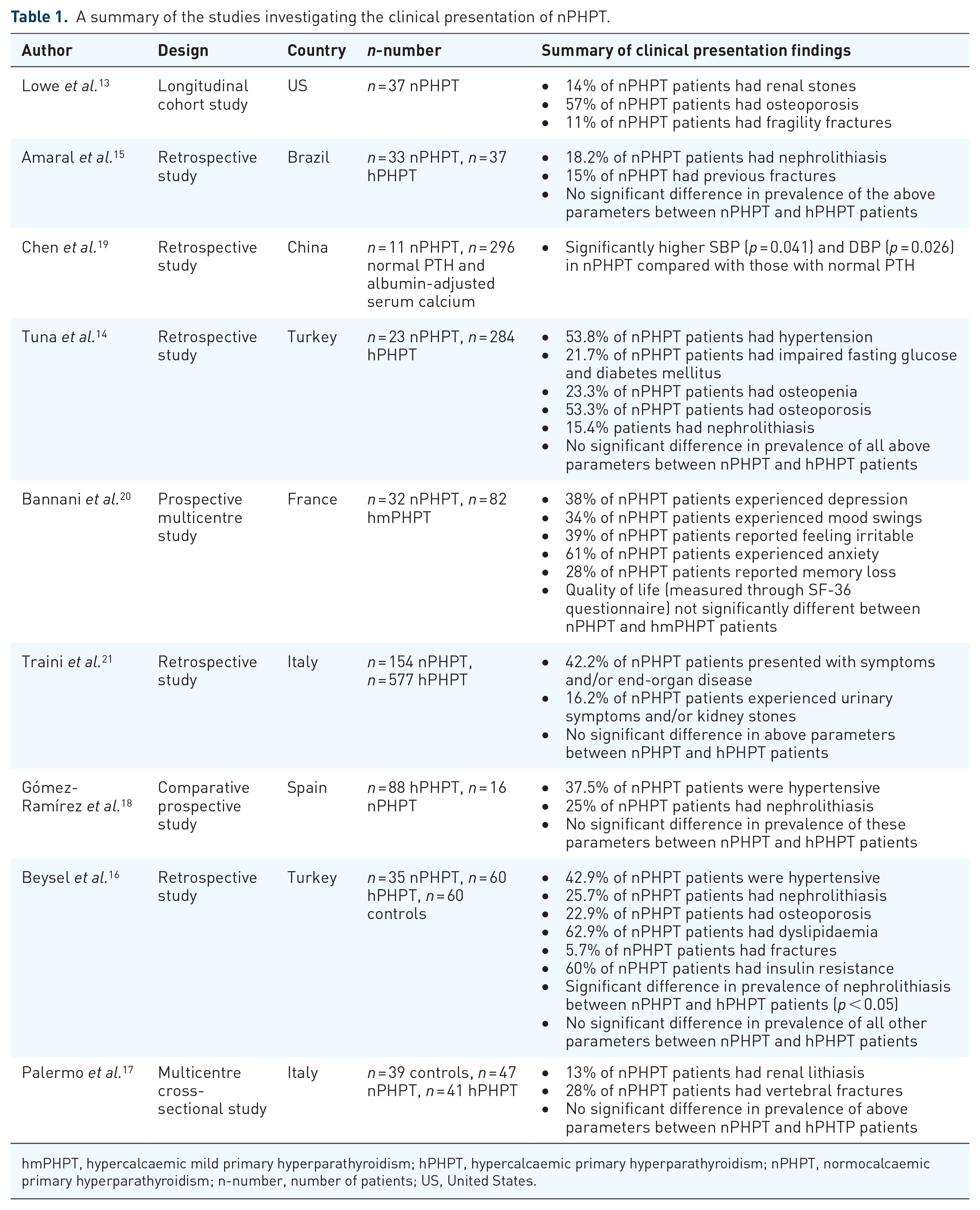
hmPHPT, hypercalcaemic mild primary hyperparathyroidism; hPHPT, hypercalcaemic primary hyperparathyroidism; nPHPT, normocalcaemic primary hyperparathyroidism; n-number, number of patients; US, United States.
Furthermore, Gómez-Ramírez et al. reported comparable incidence of both hypertension and nephrolithiasis in both groups. 18 In the nPHTP patient cohort, 37.5% of patients had hypertension (n = 6) and 25% experienced nephrolithiasis (n = 4). However, the relatively smaller number of patients within the nPHPT cohort (n = 16) may have prevented significant differences in clinical characteristics being uncovered. 18 Other studies have reinforced these findings, with no significant differences reported in the incidence of hypertension or nephrolithiasis between the nPHPT and hPHPT patient groups.14,15,17,21 However, a study by Beysel et al. revealed that whilst the incidence of all other associated co-morbidities was comparable between nPHPT and hPHPT patients, 16 the incidence of nephrolithiasis was significantly lower in those with nPHPT.
Although studies have revealed no significant difference in the incidence of hypertension between those with hPHPT and nPHPT, one study comparing those with nPHPT (n = 11) with patients with normal albumin-adjusted serum calcium and PTH (n = 296) reported significantly higher systolic blood pressure (SBP) and diastolic blood pressure (DBP) in those with nPHPT. 19 This therefore suggests that it may be the elevated PTH causing cardiac morbidity rather than the high calcium; this positive predictive relationship between serum PTH and elevated blood pressures has been similarly uncovered by Beysel et al. 16
Neuropsychiatric symptoms, including anxiety, depression, and worsening health-related quality of life (HRQoL), can be a prominent manifestation of nPHPT. 22 In their comparative study of nPHPT and hypercalcaemic mild PHPT (hmPHPT), Bannani et al. reported that, of the 32 nPHPT patients in their cohort, 38% suffered from depression, 34% experienced mood swings, 39% reported feeling irritable, 61% experienced anxiety and 28% reported memory loss. 20 In this same study, HRQoL was assessed using the Short Form 36 (SF-36) questionnaire, which enables assessment of both physical and mental health aspects. Preoperatively, the physical component score (PCS) and mental component score (MCS) were both lower, on average, in nPHPT patients compared with hcmPHPT patients – although, the difference for both of these summary scores was not significant (p > 0.05).
Management
Patient work up and assessment with regard to ‘candidates for surgery’
Referral for surgery
At present, for PHPT as a whole, referral for surgery is deemed necessary if patients are symptomatic, if there is end-organ involvement or if serum calcium is greater than 2.85 mmol/l. NICE also recommends to ‘consider’ surgery for those who do not fulfil the above criteria (see Table 2). 23 This appears to be a reasonable starting point for nPHPT patients as those who may stand to benefit from prevention of progression of end organ effects can be referred for surgery. Questions remain, however, on whether surgery is of benefit to reduce risk of a number of non-skeletal and renal outcomes in nPHPT and whether alternative criteria should be developed.
Existing NICE guidance for PHPT surgical referral. 23

NICE, National Institute for Health and Care Excellence; PHPT, primary hyperparathyroidism.
Localisation studies
Prior to surgery, ultrasonography and radionuclide scanning are utilised in an attempt to localise a parathyroid adenoma. However, studies have shown that imaging in nPHPT is less successful compared with hPHPT; this poses an additional challenge from a surgical perspective. 18 In their case series of 616 patients, Trinh et al. reported a significantly higher incidence of multi-glandular disease (p = 0.002) in nPHPT patients, with 12% of nPHPT patients having multi-glandular disease compared with 4% of hPHPT patients. 24 Moreover, Gómez-Ramírez et al. reported that parathyroid adenomas of nPHPT patients weighed on average 656 mg less than hPHPT patients (p = 0.058). 18 These findings of a greater incidence of multi-glandular disease and smaller adenomas in nPHPT are supported extensively within the literature.21,24–26 The combination of these two factors contributes to a lower sensitivity upon ultrasonography and technetium (Tc)-sestamibi scintigraphy amongst nPHPT patients. 18
Parathyroidectomy and biochemical ‘cure’
Trinh et al., in their study of 616 patients (nPHPT = 119, hPHPT = 497), investigated the role of intraoperative PTH monitoring in the management of nPHPT. 24 A significantly lower percentage of nPHPT (97%) patients demonstrated a >50% fall in their IOPTH levels compared with those with hPHPT (99%). The drop of >50% was 82.9% predictive of a long-term biochemical cure in nPHPT patients, which was not significantly different from the predictive value for hPHPT patients (p = 0.90). Trinh et al. concluded that a stricter threshold should be used during parathyroidectomy, such that if a >50% fall in IOPTH does not occur within a 10-min period or if there is small abnormal glandular disease, bilateral exploration should be initiated. 24
Alvarez-Allende et al. have similarly explored the role of parathyroidectomy in nPHPT. 27 All patients included in their retrospective analysis were required to have a minimum of one successful localisation scan prior to surgery. Of the 50 patients analysed, 26 (52%) underwent surgery based on a prediction of a postoperative fall in PTH level of >50%. Postoperatively, all patients demonstrated a fall in their PTH levels ⩾50% and 67% of patients exhibited a fall >75%.
A study from Sho and colleagues, with a follow-up period of 23.1 months, found a lower curative rate to parathyroidectomy, with 46.5% of nPHPT patients continuing to exhibit a persistently high PTH following surgery. In this study, a relationship between pre-operative PTH levels >100 pg/ml and post-operative PTH persistent elevation was uncovered 28 ; this raised the question as to whether more severe PHPT is less likely to be biochemically cured following parathyroidectomy. Interestingly, this study included a relatively large proportion of patients with multi-glandular disease (54%) so it is possible that this accounts for the higher rates of persistently raised circulating PTH. Estimates of rates of persistent PTH elevation in nPHPT post-surgery range between 10.0% and 46.5% between studies outlined in Table 3; however, the studies are heterogenous in nature and are variable in terms of inclusion of biochemical follow-up data. Further follow-up data would help us to refine our criteria for surgical cure. It is interesting to note that in the Sho et al. study, clinical improvements were only seen in in those with biochemical normalisation of PTH, 28 with a 5.6% improvement in bone mineral density (BMD) in this group versus no improvement in those with persistently elevated PTH.
A summary of the studies on the efficacy of parathyroidectomy in nPHPT.

BMD, bone mineral density; CIMT, carotid intima media thickness; hmPHPT, hypercalcaemic mild primary hyperparathyroidism; HOMA-IR, homeostasis model assessment-insulin resistance index; hPHPT, hypercalcaemic primary hyperparathyroidism; IOPTH, intraoperative parathyroid hormone; nPHPT, normocalcaemic primary hyperparathyroidism; n-number, number of patients; PTH, parathyroid hormone; PWV, pulse wave velocity; sCD40L, soluble CD40 ligand; SF-36, Short Form 36; US, United States.
A multi-institutional, retrospective study of 7634 patients by Pandian et al. showed comparable rates of ‘clinical concern for persistent hyperparathyroidism’ (p = 0.09) between nPHPT and hPHPT patients. 31 However, the authors of the study acknowledged that this data was not recorded for 25% of study participants and this may have prevented possible differences being identified.
Impact on BMD
Existing evidence suggests that parathyroidectomy yields similar improvements in BMD in both nPHPT and hPHPT patients. In their longitudinal cohort study of 60 PHPT patients (39 nPHPT), Koumakis et al. highlighted the beneficial impact of parathyroidectomy on BMD in nPHPT patients with osteoporosis (see Table 3). 29 This patient group exhibited significant improvements in hip (+1.9 ± 5.7%) and spine (+2.3 ± 5.0%) BMD. Although these improvements were less than those observed in hPHPT patients, the difference observed between the two groups was not significant (p > 0.1). Traini et al. similarly found a beneficial impact of surgery on BMD, with 41.7% of nPHPT patients showing improved BMD and 50% exhibiting stabilisation of BMD at a 72.9 (±46.8) month follow up post-parathyroidectomy. 21 However, it is important to consider that only 12 of the 39 patients who had diminishing BMD before parathyroidectomy were examined post-surgery, which reduces the representativeness of the findings. A recent single-centre study by Sho et al. of 71 nPHPT patients, revealed that BMD improvements following parathyroidectomy may be related to normalisation of PTH. 28 This was demonstrated by mean BMD improving by 5.6% (p < 0.01) amongst patients with normalised PTH post-parathyroidectomy, whereas BMD failed to improve significantly amongst patients with a persistently high PTH post-parathyroidectomy (p < 0.47).
Impact on renal outcomes
Traini et al. also reported improvements in renal outcomes following parathyroidectomy in nPHPT patients. 21 Whilst the findings are somewhat limited by only 38.5% of patients who had nephrolithiasis prior to surgery undergoing kidney ultrasound scans following parathyroidectomy, resolution of nephrolithiasis was observed in 40% of patients; yet, 60% of patients were found to have asymptomatic microlithiasis. Based on this, Traini et al. concluded that a follow-up kidney ultrasound (US) scan should be performed post-parathyroidectomy for all nPHPT patients initially presenting with nephrolithiasis. 21
Impact on cardiovascular outcomes
nPHPT appears to be associated with similar features of arterial stiffness as those seen in hPHPT; however, data on the effect of parathyroidectomy in this setting are limited. 32 A prospective study by Cansu et al. investigated the impact of parathyroidectomy on atherosclerotic parameters in asymptomatic PHPT patients. 30 Carotid intima media thickness (CIMT), pulse wave velocity (PWV) and soluble CD40 ligand (sCD40L) levels, measured both prior to and 6-months following parathyroidectomy, were not significantly different in nPHPT patients. However, in patients with hPHPT, a significant decrease in CIMT and PWV levels was found, suggestive of improved cardiovascular outcomes in this patient group. Conversely, a retrospective study by Beysel found that parathyroidectomy yielded similar cardiovascular benefits in both nPHPT and hPHPT patients. 16 Cardiovascular parameters including serum total cholesterol, systolic and diastolic blood pressures and the homeostasis model assessment-insulin resistance index (HOMA-IR) were significantly lower following parathyroidectomy (p < 0.05) in both nPHPT and hPHPT patients. Furthermore, the Framingham cardiovascular risk score was also found to have significantly decreased in both nPHPT (p = 0.001) and hPHPT (p = 0.005) patients. 16
Impact on quality of life
Patients with nPHPT commonly report a deterioration in their quality of life. 19 Therefore, it is important to consider whether parathyroidectomy can improve the quality of life of these patients. A prospective multicentre study by Bannani et al. compared quality of life improvements following parathyroidectomy in nPHPT patients and hypercalcaemic mild PHPT (hmPHPT) patients. 20 Following parathyroidectomy, the physical component summary score from the SF-36 questionnaire was shown to significantly improve in both nPHPT (p = 0.040) and hmPHPT (p = 0.016) patients. However, the mental component summary score failed to improve significantly following parathyroidectomy in nPHPT patients, improving only in hmPHPT patients (p = 0.043). The effect of parathyroidectomy on 25 non-specific symptoms was also investigated in this study. At 3 months post-surgery, three non-specific symptoms (thirst, mood swings and anxiety) were found to have improved in nPHPT patients. However, extended follow up of these patients at 1 year post-surgery (likely to give an indication of long-term benefits), revealed significant improvements in only two symptoms (thirst and fatigue). This improvement in non-specific symptoms was less in nPHPT patients compared with the hmPHPT patient group, who showed significant improvement in nine non-specific symptoms 1-year post-surgery.
Medical management
As an alternative to surgery, medical management can be utilised in some cases of nPHPT. Surgery may not be suitable for all patients – patients may decline surgery or alternatively be deemed unfit for surgery due to associated frailty or comorbidities. 23 Medical management entails management of the complications of nPHPT such as osteoporosis, rather than the treating the underlying pathological cause of inappropriate PTH hypersecretion. As a result, medical management does not offer curative potential for nPHPT patients.
Limited investigation has been conducted on the impact of alendronate on BMD in a normocalcaemic cohort. One prospective open label randomised trial of 30 nPHPT postmenopausal women revealed improved BMD following alendronate administration. This trial involved comparison of two groups of 15 nPHPT women, with one group receiving oral alendronate in addition to cholecalciferol and the other group only cholecalciferol. Following 1 year of treatment, the alendronate group exhibited significant improvements in lumbar, femoral neck and hip BMD (p = 0.001) – a finding not observed in the control group. 33
Cinacalcet is commonly used in the management of hPHPT. NICE guidance suggests cinacalcet should be considered in symptomatic patients with calcium levels ⩾2.85 mmol/l as well as asymptomatic patients where calcium levels are ⩾3.0 mmol/l. 23 With regards to the possible use of cinacalcet in nPHPT patients, one prospective randomised pilot study consisting of 10 PHPT patients (4 hPHPT and 6 nPHPT), demonstrated a significant decrease in the number and diameter of renal stones in both patient groups following provision of cinacalcet over a 10-month period. 34 However, given the small sample size of this study, larger studies are needed to understand the true impacts of cinacalcet amongst nPHPT patients.
Does surgical referral differ for nPHPT patients?
A key question remains as to whether nPHPT should be considered a different entity to hPHPT, or if they can be managed using a single approach. Whilst studies have reported that nPHPT presents differently to hPHPT, such as with a higher incidence of multi-glandular disease,21,24–26 studies have also shown that a proportion of normocalcaemic patients will progress to hypercalcaemia.7,10,11 In line with this, a standardised approach to managing PHPT irrespective of serum calcium appears appropriate and the aforementioned NICE guidance for PHPT surgical referral remains applicable for nPHPT. However, it is important that discussions regarding surgery are individualised and patient expectations are comprehensively explored. This involves counselling the patient to ensure adequate understanding of both the positive (a reduction in end-organ effects) and adverse (risk of surgical complications) outcomes that may occur following surgery.
For clinicians, it is also important to avoid routinely screening PTH levels unless there is evidence to suggest measurement would be appropriate. This includes evidence of calcium homeostasis disturbance, renal dysfunction and occasionally if there is vitamin D deficiency.
Limitations of the current literature
Many of the studies investigating the role of surgery in the treatment of nPHPT consist of a relatively small cohort of patients. This is compounded by comparative studies in the field generally having a significantly larger number of hPHPT patients relative to nPHPT patients. Future studies should aim to analyse larger nPHPT cohorts, with comparative studies providing equal representation to nPHPT and hPHPT patients. Moreover, there is a need for large consortia based prospective registries of those managed both surgically and medically, with an extended follow up period of more than 10 years. This would enable the true natural history and adverse events of treatment to be observed, providing much needed clarity to clinicians.
Conclusion
Successful surgery for nPHPT can yield significant benefits, including improvements in BMD and renal stone risk. However, there is evidence that suggests the magnitude of these improvements may be less in nPHPT patients compared with hPHPT patients. nPHPT can be more challenging to treat due to lower rates of pre-operative localisation, more patients requiring bilateral exploration and smaller but pathological multi-glandular disease. It provides further fuel to the adage that the most important factor is to localise a surgeon fluent in the disease and operative practice. Nonetheless, parathyroidectomy should be considered in patients with nPHPT, but it is important to assess and counsel patients individually to ensure appropriate expectations, even from technically successful parathyroidectomy.
Footnotes
Author contributions
NA, SK, NG and ZHS were all involved in drafting , re-drafting and editing the manuscript.
ZHS and NG were involved in supervising the NA.
NA and ZHS designed search strategy and performed literature searches.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.